Psych · Professional — complaint management and regulation
Complaint management and professional regulation
Also known as Patient complaints · Fitness to practise · Medical board notification · AHPRA notification · Open disclosure · Medicolegal complaints · Professional regulation · Defensive medicine · Second victim · Healthcare complaints
Exam-exhaustive fellowship reference on healthcare complaints versus claims versus regulatory notifications, why patients complain, complaint taxonomies, recurrent-complaint risk, open disclosure, local resolution, fitness-to-practise principles, second-victim harm and defensive medicine, psychiatrist-specific complaint drivers, and support/remediation pathways. FRANZCP-primary, globally tagged. Principles only — no invented statute numbers.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Fellowship exams test complaint management because psychiatrists will lead local resolution, write formal responses, supervise trainees named in service complaints, sit on clinical governance, and personally face regulatory risk. The candidate must separate complaint, claim, incident report, and regulator notification, then act safely for patients, fairly for staff, and lawfully under local process — without inventing section numbers.[1][10]
| Construct | What it is | Exam discriminator |
|---|---|---|
| Complaint | Dissatisfaction about care/service | May be oral or written; often seeks explanation/apology |
| Clinical incident report | Internal safety report | Learning system; not always known to patient |
| Civil claim / suit | Legal action for compensation | Higher threshold; lawyers and limitation periods |
| Regulator notification / FTP | Public-protection process about practitioner | Fitness, conduct, performance, health pathways |
| Open disclosure | Honest communication after harm | Ethical/systems practice; coordinate with indemnity |
Fitness to practise (or equivalent local language) is a public-protection construct: whether the practitioner can practise safely and ethically. It is not synonymous with “a patient was unhappy.” Impairment, professional misconduct, and performance concerns are related but non-identical regulatory ideas — thresholds and names are jurisdiction-specific.[1][13]
Classification — pathways and taxonomies
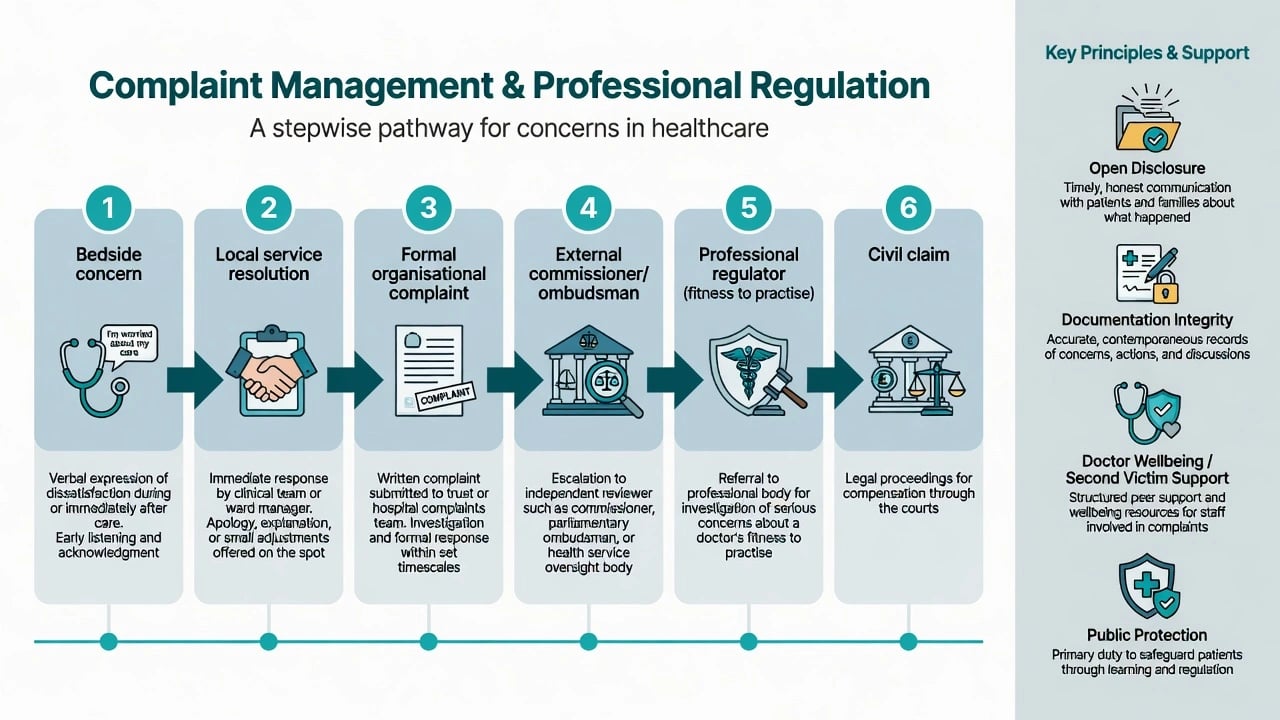
Resolution ladder (principle-level), moving from informal repair toward public-protection and civil tracks as risk and dissatisfaction escalate:[4][6][8]
- Bedside acknowledgment — listen, clarify, fix what is fixable now.
- Local service resolution — senior clinician meeting, apology for experience/harm as appropriate, written response, service change.
- Formal organisational pathway — independent review, complaints officer, root-cause when harm occurred.
- External commissioner / ombudsman / health complaints entity — jurisdiction-specific.
- Professional regulator — notification, investigation, possible conditions, suspension, or cancellation.
- Civil claim / criminal process — separate tracks when compensation or criminal thresholds apply.[4][6][8]
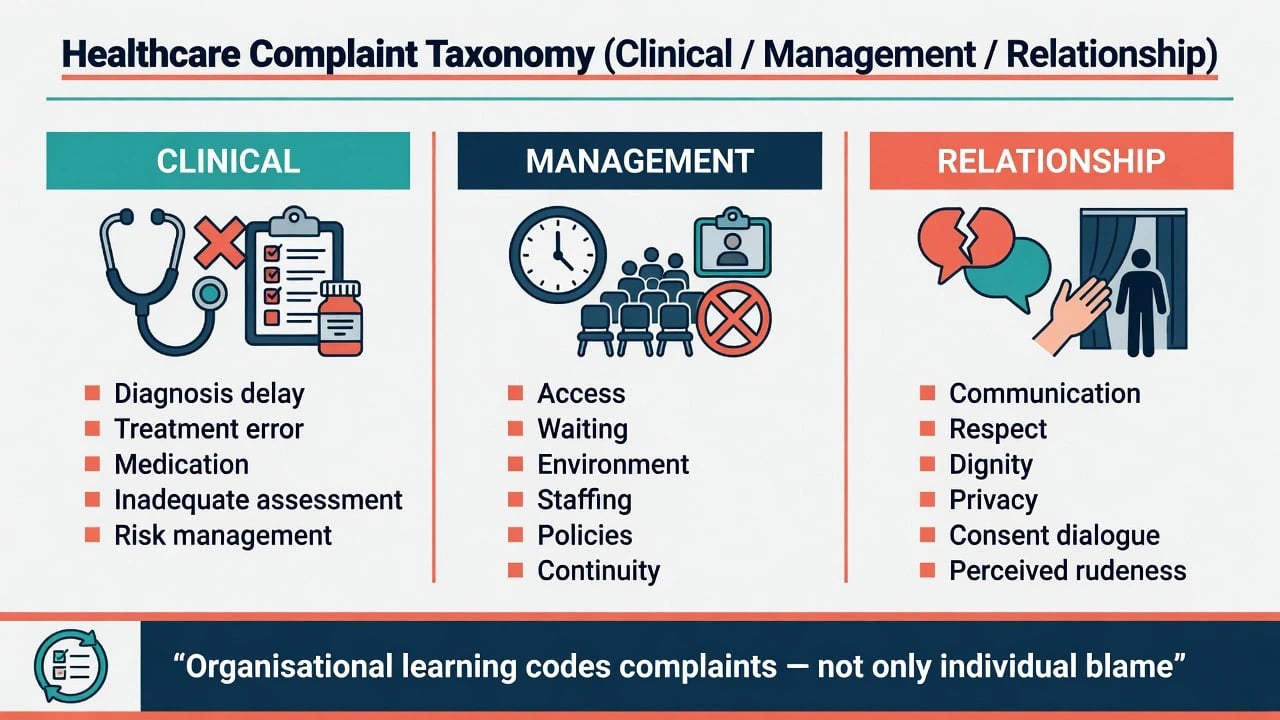
Systematic review of patient complaints supports a reliable clinical / management / relationship taxonomy; the Healthcare Complaints Analysis Tool (HCAT) operationalises coding for service monitoring and learning.[4][5]
- Assessment quality
- Diagnosis delay
- Treatment/medication error
- Risk management failures
- Safety incidents
- Access and waiting
- Environment/staffing
- Policies and continuity
- System bottlenecks
- Often not one doctor's fault alone
- Communication tone
- Respect and dignity
- Privacy
- Consent dialogue
- Perceived rudeness or dismissiveness
Epidemiology and risk
Formal complaints are far more common than malpractice judgments. Australian national complaint data show that a small minority of doctors account for a disproportionate share of recurrent complaints — prior complaint history is a powerful risk signal.[1] The PRONE score uses routinely collected administrative variables (including prior complaints and practice factors) to estimate future formal complaint risk — useful for targeting support and remediation, not for shaming.[2]
Australian work comparing regulated practitioners found mental health practitioners have distinctive complaint profiles relative to many physical health peers, with important signals in professional behaviour and clinical care domains relevant to psychiatry exams.[13]
Medicolegal involvement is common enough that Australian doctors frequently report exposure and perceived practice change after medicolegal concern (more defensive documentation, altered patient selection, increased caution).[10][11]
In the UK, a large cross-sectional survey of doctors found complaints procedures associated with substantial psychological morbidity, defensive practice, and reduced clinical confidence — the process itself is an occupational health event.[3]
Mechanisms — why complaints arise and escalate
Classic litigation research shows patients and relatives who sue often seek accountability, explanation, apology, and prevention of recurrence — not only money. The same motives animate many non-litigious complaints.[6] Patients and physicians differ in expectations about disclosure after error: patients generally want honest explanation; physicians fear litigation and may under-disclose — a mismatch that fuels mistrust.[7]
Malpractice claims also show imperfect overlap between claims, errors, and compensation — exam pearl: a claim is not proof of negligence; absence of a claim is not proof of safety.[8]
Second-victim literature: clinicians involved in adverse events commonly experience shame, guilt, anxiety, sleep disturbance, and professional doubt; organisational support matters.[12] Complaint procedures amplify shame and defensive medicine when handled as pure punishment without learning supports.[3][9][14]
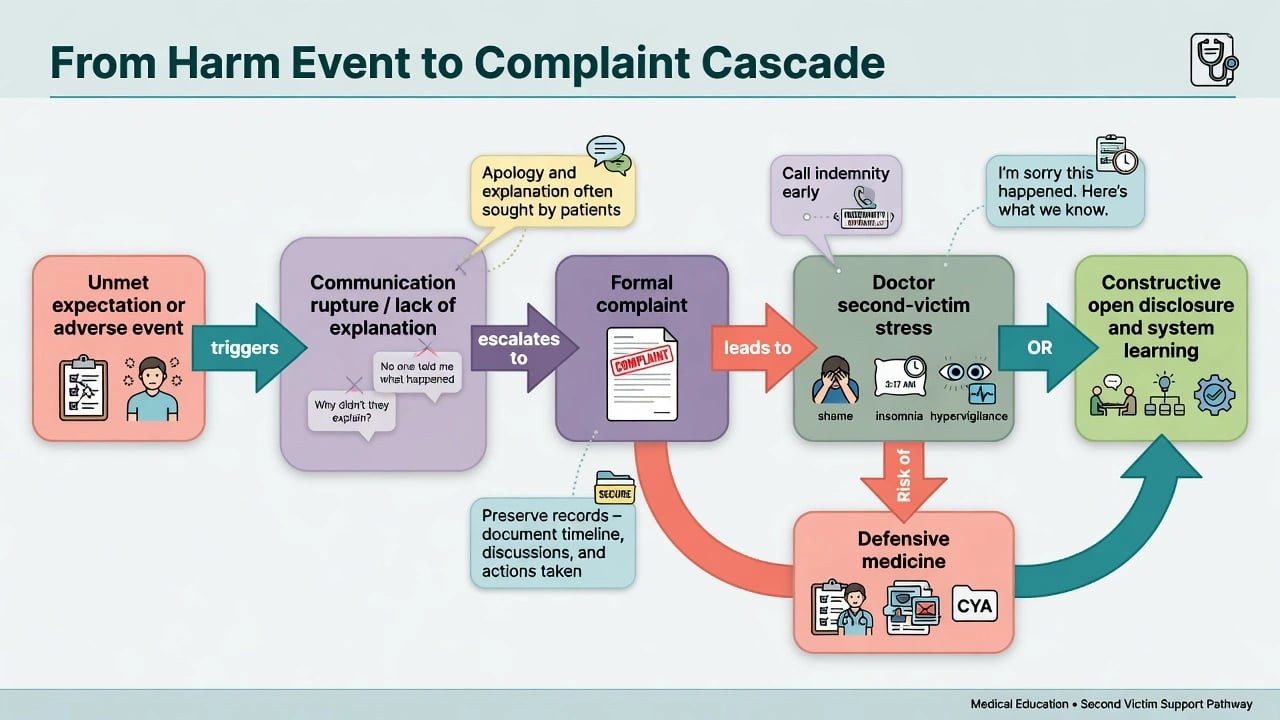
Mechanistic layers for viva synthesise complaint drivers with second-victim and defensive-practice cascades:[3][4][6][12]
- Expectation gap — outcome, access, or manner of care below what patient/family expected.[6]
- Communication rupture — no explanation, defensive tone, perceived disrespect.[4][7]
- Systems latent failures — understaffing, poor handover, access delays coded as management domain.[4][5]
- Formalisation — when informal repair fails, letters and regulators appear.[1]
- Second-victim cascade — shame to isolation to morbidity to defensive practice or crisis.[3][12]
Clinical presentations (exam stems)
Classic stems: family angry after unexpected death or post-discharge suicide; patient alleges rude, dismissive psychiatrist; formal letter after involuntary detention or seclusion; regulator notification about prescribing or boundaries; trainee named in ward complaint; serial complainant across services; cluster of relationship complaints about one clinician; doctor with insomnia and suicidal thoughts after receiving a board letter; allegation of sexual misconduct requiring immediate protective action.[3][13][14]
Doctor under complaint may present with hypervigilance, defensive over-documentation, avoidance of high-risk patients, cynicism, increased substance use, sick leave, or acute psychiatric crisis.[3][9][12]
Differential — what kind of problem is this?
| Pattern | Favours | Action emphasis |
|---|---|---|
| Single relationship rupture, good notes, no harm | Communication repair | Local meeting, coaching |
| Clear clinical error with harm | Quality/safety event | Open disclosure + incident review |
| Recurrent formal complaints re same doctor | Pattern risk (Bismark/PRONE) | Remediation, monitoring, governance |
| Sexual boundary allegation | Misconduct / possible crime | Protect; escalate; no collusion |
| Acute intoxication / cognitive failure at work | Impairment | Remove from duties; public protection |
| Pure access/waiting anger | Management domain | Service-level response |
Never use “vexatious” as a first reflex. Even difficult complainants may surface real safety issues. Assess merit, risk, and process fairness separately from personality of the complainant.[4][14]
Assessment
Triage first, narrative second. Assessment structures safety, evidence preservation, open disclosure, and second-victim support before drafting defensive text.[3][6][7][12]
RESPOND
Assess complainant goals (Vincent framework adapted): explanation, accountability, prevention, apology, sometimes compensation.[6] Assess the named doctor’s mental state and fitness for remaining duties — complaint processes associate with marked distress.[3][14]
Investigations and fact-finding
- Secure the clinical record; never alter after notice of complaint.[9][14]
- Timeline reconstruction from notes, orders, risk assessments, consent, and MSE when psychiatry-relevant.[13]
- Code complaint content (clinical/management/relationship) for learning using HCAT-type approaches at organisational level.[4][5]
- Serious harm: parallel clinical governance / root-cause principles; separate learning from individual discipline where culture allows.[5]
- Regulator, employer, and civil processes have different purposes — seek medical defence / indemnity advice early; do not freestyle legal strategy in exam stems.[8][10]
Immediate management (safety resuscitation)
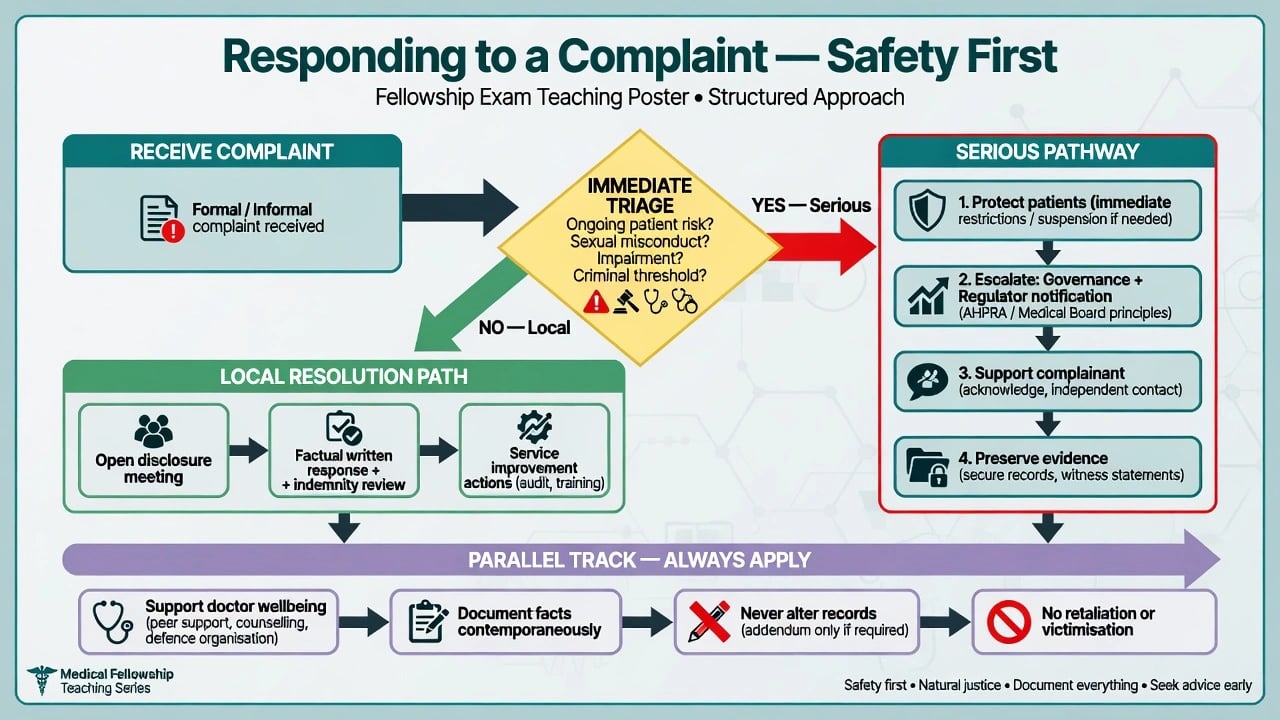
Immediate actions prioritise patient safety, open disclosure of known facts, indemnity notification, and protection of the clinician under process without record alteration or retaliation:[3][7][9][12][14]
- Ensure ongoing safe care for the patient (and other patients if a pattern or impairment is suspected).
- If therapeutic rupture is severe, arrange alternative clinician without abandoning care.
- Notify indemnity / medical defence and clinical governance as local policy requires.
- Begin open disclosure of known facts with empathy; avoid speculation and blame games.[7]
- If the doctor is acutely unsafe (severe crisis, intoxication, gross misconduct): remove from duties, arrange cover, escalate public-protection pathways as required — principles only.[3][12]
- Do not contact the complainant to pressure withdrawal; do not retaliate; do not alter notes.[9][14]
Definitive management — resolution, remediation, regulation
Local resolution and open disclosure
When proportionate and safe, early local resolution is first-line: facilitated meeting, apology for the experience and for preventable harm where appropriate, clear explanation, and tangible service improvements. Patients often want honesty more than silence.[6][7] Written responses should be factual, non-defensive, reviewed with senior/indemnity input, and free of personal attack.
Organisational learning
Use structured complaint coding (HCAT concepts) so management-domain problems are not misread as purely individual incompetence, and so relationship-domain patterns trigger communication coaching before regulator heat rises.[4][5]
Recurrent complaint risk
Bismark and colleagues’ Australian work shows concentrated risk in a minority of practitioners; Spittal’s PRONE work formalises prediction from administrative data. Fellowship response: early remediation, supervision, communication skills, health assessment if indicated, and fair monitoring — not waiting for career-ending events.[1][2]
Regulatory engagement
Cooperate truthfully with investigations. Outcomes may include no further action, caution/education, conditions/undertakings, suspension, or cancellation of registration — names and thresholds are local. Remediation plans, supervised practice, and health pathways are common intermediate tools. Do not invent AHPRA form codes or GMC rule numbers in answers.[1][13]
Doctor health under process
Bourne’s UK survey and second-victim reviews require active support: peer support, GP/doctor-health services, time-limited duty adjustment if concentration is unsafe, and direct suicide enquiry when distress is high.[3][12][14] Defensive medicine after medicolegal threat is common; organisations should counter with just culture and skills support, not only exhortations to “be resilient.”[9][11]
Special populations and psychiatry-specific scenarios
Mental health practitioners. Complaint content and rates differ from many physical-health peers; expect scrutiny of communication, professional behaviour, and clinical risk decisions (including involuntary care interfaces).[13]
Post-discharge suicide / unexpected death. Family grief plus expectation of prevention; open disclosure, compassionate review, and careful risk documentation review; support staff second victims.[6][12]
Involuntary treatment, seclusion, restraint. High relationship and rights sensitivity; document legal criteria used (jurisdiction-specific), least restrictive rationale, and communication with family where lawful — relationship-domain complaints cluster around perceived disrespect in coercive care contexts.[4][13]
Boundary / sexual allegations. Immediate protection of patients; escalate; no dual investigation by the alleged perpetrator’s friends; see boundary-violation topic for depth.[13]
Trainees. Supervisor owns system contributions; protect educational fairness; do not leave junior as sole named scapegoat for team failures.[3][14]
IMGs and rural doctors. Communication style and dual-role density raise complaint risk; mentoring and cultural communication coaching are preventive infrastructure.[1][11]
Complications and pitfalls
Classic fails: silence after harm; altered notes; retaliatory behaviour; inventing statute numbers; dismissing all complaints as personality of the patient; pure resilience talk while ignoring recurrent complaint patterns; abandoning the doctor under investigation so suicide risk is missed; and equating every complaint with proven negligence or every claim with error.[1][3][8][9]
Prognosis and disposition
Most local complaints resolve without career-ending sanction when handled early, openly, and with learning. Recurrent formal complaint patterns predict further risk and need structured remediation.[1][2] Psychological recovery may lag legal closure; second-victim support improves recovery trajectories.[12] Disposition options: continue with support; temporary restriction; remediation and supervised return; rare permanent exit from practice after serious findings.
Evidence, guidelines, and regional differences
Landmark anchors: Bismark recurrent complaints; Spittal PRONE; Reader taxonomy and Gillespie HCAT; Bourne impact survey; Vincent why-people-sue; Gallagher disclosure attitudes; Studdert claims/errors/compensation; Cunningham shame and defensive medicine; Nash medicolegal exposure and practice change; Seys second-victim review; Veness mental health practitioner complaint risk; Jain qualitative GP complaint experience.[1][2][3][4][5][6][7][8][9][10][11][12][13][14]
[3] [7] [13]Exam pearls
Hero overview figure (embedded above)
Primary overview is Figure 1 (pathway). Use Figures 2–4 for taxonomy, cascade, and response algorithm in revision. Together they encode escalation pathways, complaint domains, second-victim cascades, and safety-first response algorithms drawn from complaint science and disclosure evidence.[1][4][6][12]
References
- [1]Bismark MM, Spittal MJ, Gurrin LC, Ward M, Studdert DM Identification of doctors at risk of recurrent complaints: a national study of healthcare complaints in Australia BMJ Qual Saf, 2013.PMID 23576774
- [2]Spittal MJ, Bismark MM, Studdert DM The PRONE score: an algorithm for predicting doctors' risks of formal patient complaints using routinely collected administrative data BMJ Qual Saf, 2015.PMID 25855664
- [3]Bourne T, Wynants L, Peters M, et al. The impact of complaints procedures on the welfare, health and clinical practise of 7926 doctors in the UK: a cross-sectional survey BMJ Open, 2015.PMID 25592686
- [4]Reader TW, Gillespie A, Roberts J Patient complaints in healthcare systems: a systematic review and coding taxonomy BMJ Qual Saf, 2014.PMID 24876289
- [5]Gillespie A, Reader TW The Healthcare Complaints Analysis Tool: development and reliability testing of a method for service monitoring and organisational learning BMJ Qual Saf, 2016.PMID 26740496
- [6]Vincent C, Young M, Phillips A Why do people sue doctors? A study of patients and relatives taking legal action Lancet, 1994.PMID 7911925
- [7]Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W Patients' and physicians' attitudes regarding the disclosure of medical errors JAMA, 2003.PMID 12597752
- [8]Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation N Engl J Med, 2006.PMID 16687715
- [9]Cunningham W, Wilson H Complaints, shame and defensive medicine BMJ Qual Saf, 2011.PMID 21441601
- [10]Nash LM, Kelly PJ, Daly MG, Walter G, van Ekert EH Australian doctors' involvement in medicolegal matters: a cross-sectional self-report study Med J Aust, 2009.PMID 19835537
- [11]Nash LM, Walton MM, Daly MG, Kelly PJ, Walter G Perceived practice change in Australian doctors as a result of medicolegal concerns Med J Aust, 2010.PMID 21077813
- [12]Seys D, Wu AW, Van Gerven E, et al. Health care professionals as second victims after adverse events: a systematic review Eval Health Prof, 2013.PMID 22976126
- [13]Veness BG, Tibble H, Grenyer BF, Morris JM, Spittal MJ, et al. Complaint risk among mental health practitioners compared with physical health practitioners: a retrospective cohort study of complaints to health regulators in Australia BMJ Open, 2019.PMID 31874871
- [14]Jain A, Ogden J General practitioners' experiences of patients' complaints: qualitative study BMJ, 1999.PMID 10364121