Psych · Professional — cultural formulation and Indigenous mental health
Cultural formulation and Indigenous mental health
Also known as Cultural Formulation Interview · DSM-5 CFI · Outline for Cultural Formulation · Cultural safety · Social and emotional wellbeing · SEWB · Explanatory models · Aboriginal and Torres Strait Islander mental health · Indigenous mental health · Working with interpreters
Exam-exhaustive fellowship reference on DSM-5 cultural formulation (OCF and CFI), Kleinman explanatory models, Aboriginal and Torres Strait Islander social and emotional wellbeing, Māori and Pacific awareness, racism and social determinants, working with interpreters, and culturally safe practice. Respectful, non-stereotyping. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Culture is dynamic, plural, and lived — language, kinship, Country, spirituality, migration history, gender, sexuality, class, and disability can all shape identity in one person. Race, ethnicity, and culture are not interchangeable labels. Examiners reward candidates who refuse essentialism ("all Indigenous people believe X") while still naming structural determinants such as racism and colonisation.[1][15][16]
Cultural formulation turns those realities into usable clinical data: how this person understands their problem, what helps and harms, and how the clinical encounter itself is culturally shaped. It is not a second diagnosis of "culture". It is part of a complete psychiatric formulation.[3][7]
| Construct | Core meaning | Exam trap |
|---|---|---|
| Cultural competence | Knowledge/skills/attitudes for cross-cultural work | Implies a finish line; can become checklist competence |
| Cultural humility | Lifelong self-critique of power and bias | Not passive — still requires skills and action |
| Cultural safety | Care free of racism/assault as defined by the recipient | Not self-certified by the clinician |
| Cultural formulation | Structured integration of cultural data into diagnosis/plan | Not stereotyping or folklore collection |
Classification — OCF and CFI
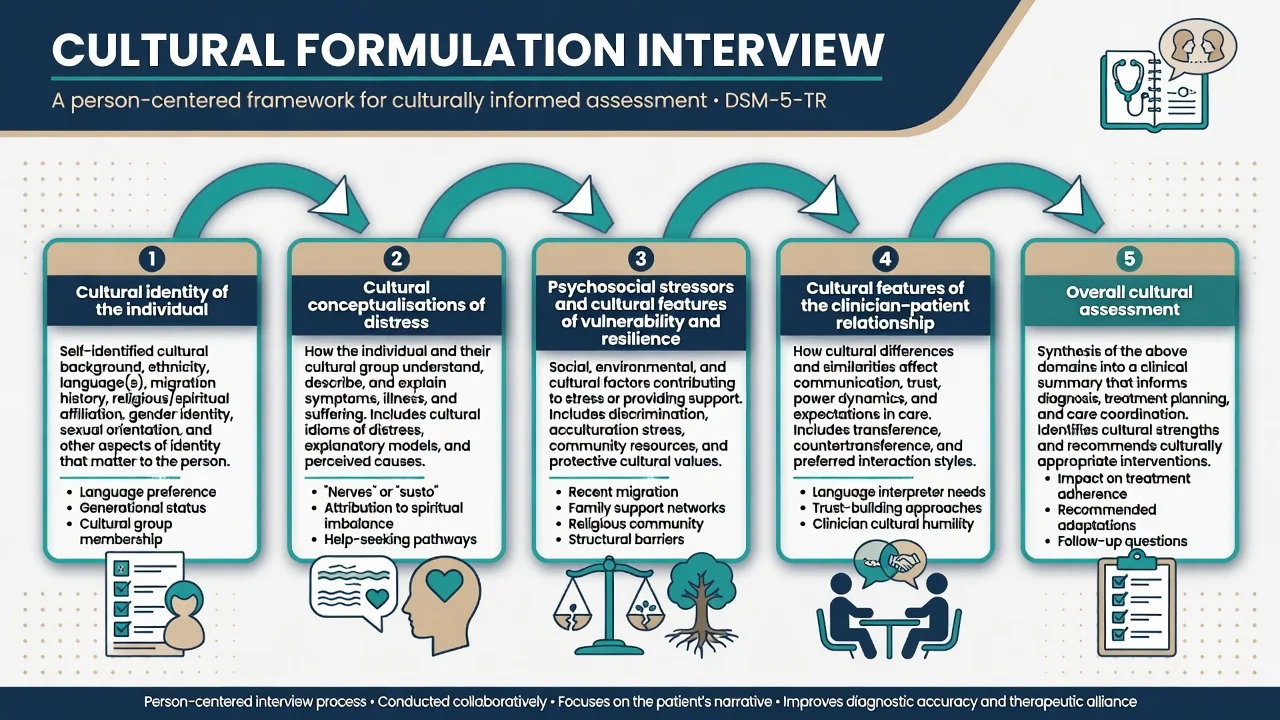
Outline for Cultural Formulation (OCF)
DSM-5 retains the Outline for Cultural Formulation domains clinicians should synthesise:[3][5]
- Cultural identity of the individual
- Cultural conceptualisations of distress
- Psychosocial stressors and cultural features of vulnerability and resilience
- Cultural features of the clinician–patient relationship
- Overall cultural assessment for diagnosis and care
Cultural Formulation Interview (CFI)
The core CFI is a short, person-centred interview (commonly described as 16 items) designed for routine use. Supplementary modules and an informant version extend depth when needed. International field-trial work found the CFI feasible, acceptable, and clinically useful across sites, and qualitative work shows it can change medical communication and the felt quality of the relationship when clinicians actually ask.[2][4][8][23]
Epidemiology, inequity, and protective factors
Inequities in psychological distress, suicide, incarceration interfaces, and service access for Aboriginal and Torres Strait Islander peoples are real and must be framed by colonisation, racism, intergenerational trauma, and social determinants — not by cultural deficit models.[9][15][24]
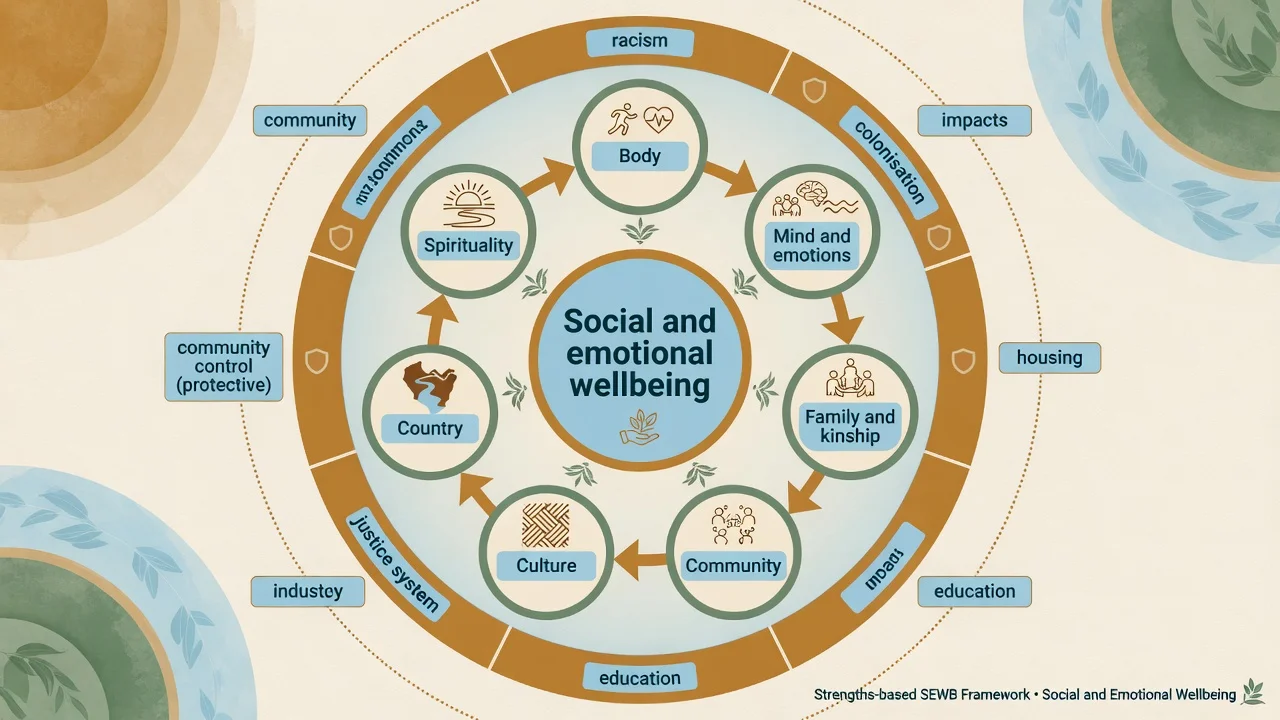
Modifiable psychosocial factors associate with distress, depression, anxiety, and self-rated health in Aboriginal and Torres Strait Islander populations; service design should target these alongside clinical care.[24] SEWB programs for young people that centre culture, community control, and relational practice show promising principles in scoping reviews.[10] Housing, community control, and cultural determinants of resilience matter clinically, not only sociologically.[11][12]
In Aotearoa New Zealand, Māori inequities and the value of culturally informed pathways after self-harm are exam-relevant (e.g. Te Ira Tangata trial of culturally informed care versus treatment as usual).[19][20]
Within-group diversity is large: urban/remote, age, gender and sexuality diversity, disability, Stolen Generations impacts, multilingual households, and multi-heritage identities. Do not collapse this into one script.[9]
Mechanisms — how culture and power shape illness
Kleinman and colleagues taught that disease (biomedical disorder) and illness (lived experience and meaning) are not the same. Explanatory models shape help-seeking, adherence, alliance, and what counts as recovery.[1]
Racism, xenophobia, and discrimination act through structural, interpersonal, and internalised pathways to health outcomes — candidates should name racism as a clinical determinant, not a political optional extra.[15][16] Cultural-ecosocial models integrate meaning, social position, and neurobiology without reducing culture to a biomarker curiosity.[21]
Misdiagnosis arises when idioms of distress are forced into the wrong DSM category (category fallacy risk); language barriers are mistaken for thought disorder; spiritual experiences are automatically psychotic — or psychosis is dismissed as "cultural"; and trauma and grief (including historical) are ignored in favour of a thin major-depression label.[1][16][21]
Clinical presentation
Culture shapes what is said, how it is said, who should be present, and whether services are trusted. Presentations relevant to FRANZCP CASC/viva include delayed help-seeking after racism or past institutional harm (child protection, justice, Stolen Generations legacies); family-centred or community-centred decision-making that mainstream clinics misread as "lack of autonomy"; somatic idioms, spiritual explanations, or shame that mask depression, PTSD, or psychosis; and apparent "poor engagement" that is actually inaccessible, unsafe, or mono-cultural care.[8][9][11]
Spiritual and cultural experiences vs psychosis is a classic discriminator station. Assess distress, dysfunction, cultural consensus (what trusted community members say), onset/course, MSE formal thought disorder, risk, and organic/substance differentials. Use cultural consultation with consent — do not invent ceremonial rules.[1][16]
Differential and discriminators
- Person-specific narrative
- Informs diagnosis and plan
- CFI/OCF structured
- Updates as identity shifts
- Group checklist applied blindly
- Ignores within-group diversity
- Harms alliance
- Exam fail
- Language barrier (interpreter)
- Organic/substance illness
- Acute risk
- Trauma needing specific care
| Problem | Discriminators |
|---|---|
| Normative cultural experience | Shared meaning, low distress/dysfunction relative to community norms, no progressive disorganisation |
| Psychopathology | Distress, disability, risk, MSE signs, course inconsistent with cultural norms |
| Language barrier | Improves with professional interpreter; thought form clearer in preferred language |
| Trauma/grief | Historical and recent trauma narrative; SEWB disruption; not only low mood criteria |
| Capable refusal / mistrust | Explains reasons; may be historically grounded; not automatically delusion |
Bedside assessment — CFI and explanatory models
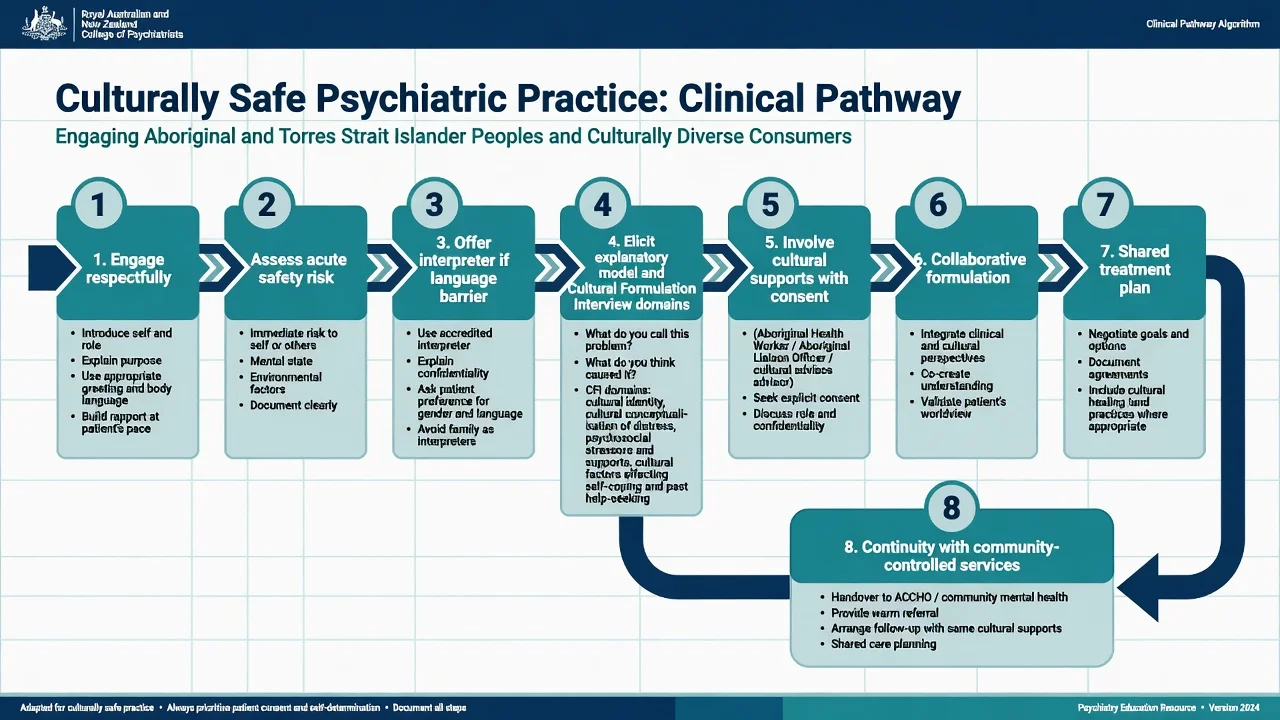
Practical sequence
- Secure acute safety (suicide, violence, medical) with culturally respectful engagement.
- Optimise communication: preferred language, professional interpreter, quiet space, adequate time.
- Introduce purpose: "I want to understand what this means for you and what helps."
- Work through CFI domains with open questions; avoid leading ethnic stereotypes.
- Elicit an explanatory model (Kleinman-style questions).
- Explore stressors, racism, housing, justice, and protective culture/kinship/Country connections.
- Reflect on the relationship — power, trust, gender match, institutional fears.
- Invite consent for cultural supports (Aboriginal Health Worker/Liaison, ACCHO, Māori health worker, family/whānau as the person defines).
- Integrate into formulation, diagnosis differentials, and collaborative plan; document specifically.[2][6][7][8]
Explanatory model questions (high-yield)

Classic probes: What do you call this problem? What do you think caused it? Why did it start when it did? How does it work / what does it do to you? How serious is it? What treatment should you receive, and who should help?[1]
The CFI also surfaces social stressors, supports, and determinants that standard checklists miss if the clinician never asks.[6] Family/informant cultural assessment can add value with consent and careful privacy management.[23]
CULTURE
Investigations and tools
There is no blood test for culture. Standard organic work-up remains indicated by clinical features (delirium, first-episode psychosis, metabolic monitoring for psychotropics, etc.). Cognitive screens and symptom scales need caution when translation/validation is poor — interpret scores in context.[17][21]
Document cultural data in the formulation and care plan, not only as ethnicity demographics. The CFI itself is the primary structured tool; implementation and training literature supports building it into routine care and case formulation.[5][7]
Acute / emergency management
Acute risk takes priority. Culturally safe crisis care still means clear, non-humiliating communication; professional interpreter early if needed; preferred supports present with consent; least restrictive options; avoiding children as interpreters; liaison with Aboriginal/Māori health workers and community-controlled services when available; and recognition that restraint, seclusion, and police involvement can re-traumatise — document necessity and alternatives tried.[14][17][19]
Mental health law criteria remain jurisdiction-specific. Do not invent section numbers. Principles of least restriction and human rights still apply across systems.[16]
Definitive management — culturally safe practice
Integrate formulation into treatment
CFI findings should change something concrete: differential weighting, therapy model, family involvement, spiritual supports, medication discussion style, service location (ACCHO dual care), or who co-facilitates sessions.[7][8]
Medication and therapy
- Shared decision-making: map the person's explanatory model of "tablets", injections, and talking therapies.
- Avoid under-treatment driven by stereotype ("they won't take meds") and over-coercion driven by racism.
- Culturally adapted psychological therapies and Indigenous-led counselling pathways can improve engagement; dual care with mainstream psychiatry is often appropriate for severe illness.[10][11][22]
- Trauma-informed, strengths-based SEWB practice sits alongside evidence-based treatment of diagnosable disorders — both/and, not either/or.[9][11]
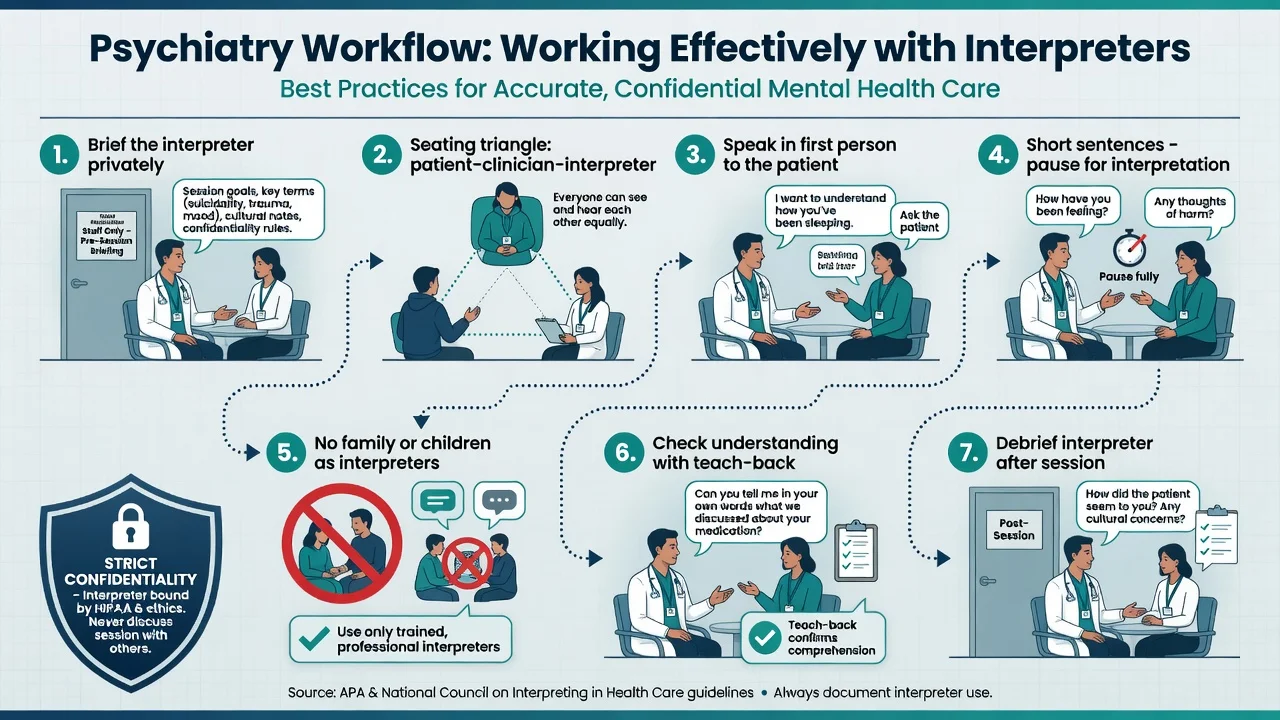
Working with interpreters
Language barriers reduce quality and service use; professional interpreter use is part of equity, not a luxury.[17][18]
| Step | Action |
|---|---|
| Brief | Goals, sensitive topics, key terms, seating |
| Seat | Triangle so all see each other |
| Speak | To the patient, first person, short chunks |
| Avoid | Children/family as interpreters when professional available |
| Check | Teach-back of understanding |
| Debrief | Interpreter after session; note confidentiality |
| Document | Language, interpreter name/service, limitations |
Cultural safety (not self-certification)
Cultural safety, rooted in Aotearoa nursing leadership, centres the recipient's experience of care free from racism and assault; contemporary refinements stress power-sharing, institutional accountability, and clear distinctions from "competency" checklists.[13][14] Psychiatry training and practice must also confront structural racism and violence in systems of care.[16]
Specific scenarios
Aboriginal and Torres Strait Islander peoples (ANZ primary)
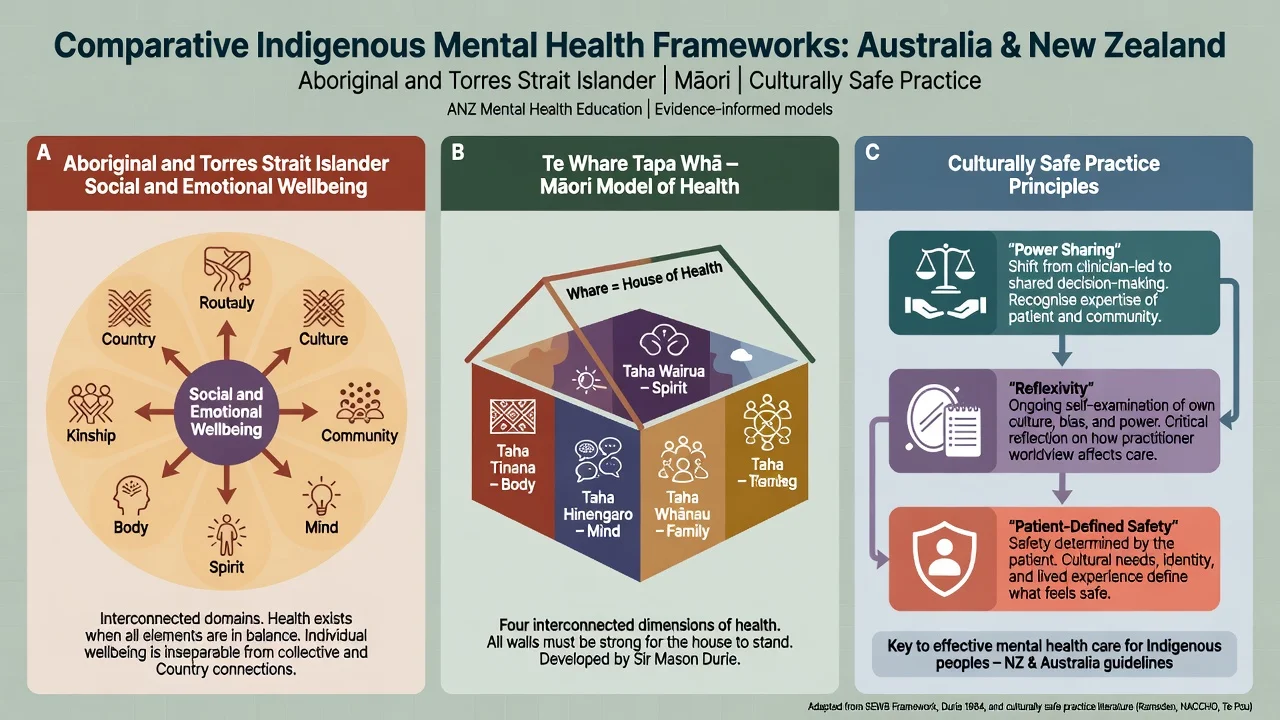
Use SEWB language where it fits the person's preference; partner with Aboriginal Community Controlled Health Organisations (ACCHOs), Aboriginal Mental Health Workers, and local protocols. Connection to Country, culture, kinship, and community control are protective clinical factors, not soft extras.[9][10][12] Acknowledge Stolen Generations and ongoing systemic racism without forcing disclosure.[11][15]
Māori and Pacific awareness
Te Whare Tapa Whā (Durie) is a widely taught Māori health model: taha tinana (body), taha hinengaro (mind), taha whānau (family), taha wairua (spirit). It is a framework for balanced care — not a claim that all Māori share identical beliefs. Culturally informed interventions after self-harm have been trialled for Māori presenting to hospital.[19][20] Pacific peoples are diverse across nations; family-centred models and language access matter. Avoid treating "Pacific" as one culture.
Refugee, migrant, and interpreter-dependent care
Prioritise professional interpreters, trauma-informed pacing, and CFI domains on migration, legal status stress, and transnational family supports. Language proficiency strongly shapes service use.[17][18]
Forensic, perinatal, youth, older adults
Over-representation in justice systems must not become clinical stereotype. Perinatal care needs cultural formulation around parenting supports and historical child-removal fears. Youth identity work includes cultural strength and intersectional minority stress. Older adults may hold Elder roles and different disclosure norms — assess capacity with language supports (see capacity topic).[9][16]
Complications and pitfalls
| Pitfall | Safer practice |
|---|---|
| Stereotype checklist | CFI person-narrative |
| Child as interpreter | Professional interpreter |
| Pathologise culture | Cultural consultation + MSE + risk |
| Miss organic disease | Same medical vigilance for all |
| Token tick-box | Power-sharing, continuity, anti-racism |
| English fluency equals safety | Still elicit identity and explanatory model |
| Ignore racism | Name and address as determinant |
| Invent lore/sections | State principles; use local protocols |
Prognosis and disposition
Engagement and outcomes improve when care is continuous, relational, and linked to community-controlled or culturally informed services, while still delivering evidence-based treatment for severe mental illness.[10][19][20] Disposition planning should include housing, legal advocacy, family/whānau as defined by the person, ACCHO/Māori health pathways, and clear crisis contacts — ethnicity alone never sets follow-up intensity; risk and need do.[12][24]
Special populations
- Intersectionality: Aboriginal and Torres Strait Islander LGBTQIA+ people (including Sistergirl/Brotherboy identities where relevant) face layered stigma — do not force disclosure; create safety.[9]
- Remote care: telehealth helps access but does not replace cultural safety or local workers.[14]
- Intellectual disability: use supported communication and trusted cultural supports; avoid equating disability with incapacity for all decisions.[9]
- Training: cultural competence in psychotherapy is an evolving professional skill set requiring supervision and humility, not one workshop.[22]
Evidence, guidelines, and regional notes
Landmark anchors for exams include Kleinman illness explanatory models; the DSM-5 CFI international field trial on feasibility, acceptability, and utility; implementation, relationship, and formulation literature (Aggarwal, Lam, Lewis-Fernández, Kirmayer); Aboriginal and Torres Strait Islander SEWB scholarship and program principles; cultural safety origins and refined definitions from Aotearoa; racism–health pathways and anti-racism in psychiatry training; interpreter quality evidence; and Māori culturally informed self-harm pathway trial work with Indigenous futures framing (Durie).[1][2][3][5][7][8][9][10][11][13][14][15][16][17][19][20]
FRANZCP candidates are expected to centre Aboriginal and Torres Strait Islander SEWB, cultural safety, ACCHO partnership, and Aotearoa Māori models (e.g. Te Whare Tapa Whā) without stereotyping. Know that College and national policy documents exist; apply local protocols and community-controlled pathways. Do not invent legislative section numbers.[9][14][20]
Exam pearls
Self-test: CASC openers
Safe openers: "How would you like me to understand what you are going through?" / "What does this problem mean in your life and for your family?" / "Is there anyone you would like involved in your care, and how?" / "Would an interpreter help us do this properly?" Avoid: "In your culture, people believe…" as a leading stereotype.[2][8]
References
- [1]Kleinman A, Eisenberg L, Good B Culture, illness, and care: clinical lessons from anthropologic and cross-cultural research Ann Intern Med, 1978.PMID 626456
- [2]Lewis-Fernández R, Aggarwal NK, Lam PC, et al. Feasibility, acceptability and clinical utility of the Cultural Formulation Interview: mixed-methods results from the DSM-5 international field trial Br J Psychiatry, 2017.PMID 28104738
- [3]Lewis-Fernández R, Aggarwal NK, Kirmayer LJ The Cultural Formulation Interview: Progress to date and future directions Transcult Psychiatry, 2020.PMID 32838656
- [4]Aggarwal NK, Desilva R, Nicasio AV, et al. Does the Cultural Formulation Interview for the fifth revision of the diagnostic and statistical manual of mental disorders (DSM-5) affect medical communication? A qualitative exploratory study among patients and clinicians Ethn Health, 2015.PMID 25372242
- [5]Lam PC, Lewis-Fernández R, Aggarwal NK The Cultural Formulation Interview: Building the Case for Cultural Competence in Clinical Care Psychiatr Serv, 2023.PMID 36722093
- [6]Aggarwal NK, Chen D, Lewis-Fernández R Eliciting social stressors, supports, and determinants of health through the DSM-5 cultural formulation interview Front Psychiatry, 2023.PMID 37056400
- [7]Aggarwal NK The Cultural Formulation Interview in Case Formulations: A State-of-the-Science Review Behav Ther, 2024.PMID 39443057
- [8]Krishan Aggarwal N, Chen D, Lewis-Fernández R If You Don't Ask, They Don't Tell: The Cultural Formulation Interview and Patient Perceptions of the Clinical Relationship Am J Psychother, 2022.PMID 35430870
- [9]Dudgeon P, Agung-Igusti R, Derry K, Gibson C Australian aboriginal and Torres Strait Islander social and emotional well-being Am Psychol, 2025.PMID 41379665
- [10]Gupta H, Tari-Keresztes N, Stephens D, et al. A scoping review about social and emotional wellbeing programs and services targeting Aboriginal and Torres Strait Islander young people in Australia: understanding the principles guiding promising practice BMC Public Health, 2020.PMID 33121463
- [11]Gee G, Hulbert C, Kennedy H, Paradies Y Cultural determinants and resilience and recovery factors associated with trauma among Aboriginal help-seeking clients from an Aboriginal community-controlled counselling service BMC Psychiatry, 2023.PMID 36899333
- [12]Brown A, Haregu T, Gee G, et al. Social and emotional wellbeing of Aboriginal and Torres Strait Islander peoples in Aboriginal controlled social housing BMC Public Health, 2023.PMID 37803360
- [13]Papps E, Ramsden I Cultural safety in nursing: the New Zealand experience Int J Qual Health Care, 1996.PMID 9117203
- [14]Curtis E, Loring B, Jones R, et al. Refining the definitions of cultural safety, cultural competency and Indigenous health: lessons from Aotearoa New Zealand Int J Equity Health, 2025.PMID 40346663
- [15]Selvarajah S, Corona Maioli S, Deivanayagam TA, et al. Racism, xenophobia, and discrimination: mapping pathways to health outcomes Lancet, 2022.PMID 36502849
- [16]Jarvis GE, Andermann L, Ayonrinde OA, et al. Taking Action on Racism and Structural Violence in Psychiatric Training and Clinical Practice Can J Psychiatry, 2023.PMID 37198904
- [17]Bauer AM, Alegría M Impact of patient language proficiency and interpreter service use on the quality of psychiatric care: a systematic review Psychiatr Serv, 2010.PMID 20675834
- [18]Bauer AM, Chen CN, Alegría M English language proficiency and mental health service use among Latino and Asian Americans with mental disorders Med Care, 2010.PMID 21063226
- [19]Hatcher S, Coupe N, Wikiriwhi K, et al. Te Ira Tangata: a Zelen randomised controlled trial of a culturally informed treatment compared to treatment as usual in Māori who present to hospital after self-harm Soc Psychiatry Psychiatr Epidemiol, 2016.PMID 26956679
- [20]Durie M Indigenous mental health 2035: future takers, future makers and transformational potential Australas Psychiatry, 2011.PMID 21878027
- [21]Gómez-Carrillo A, Kirmayer LJ, Aggarwal NK, et al. Integrating neuroscience in psychiatry: a cultural-ecosocial systemic approach Lancet Psychiatry, 2023.PMID 36828009
- [22]Kirmayer LJ Cultural competence in psychotherapy World Psychiatry, 2025.PMID 40948046
- [23]Hinton L, Aggarwal N, Iosif AM, et al. Perspectives of family members participating in cultural assessment of psychiatric disorders: findings from the DSM-5 International Field Trial Int Rev Psychiatry, 2015.PMID 25738941
- [24]Thapa S, Allan J, Giri S, et al. Modifiable psychosocial factors associated with psychological distress, depression, anxiety and self-rated health among Aboriginal and Torres Strait Islander populations Epidemiol Psychiatr Sci, 2026.PMID 41913468