Psych · Professional — psychological therapies
DBT and third-wave therapies
Also known as Dialectical behaviour therapy · Dialectical behavior therapy · DBT skills training · Acceptance and commitment therapy · ACT · Mindfulness-based cognitive therapy · MBCT · Third-wave CBT · Third wave behavioural therapies
Exam-exhaustive fellowship reference on dialectical behaviour therapy (modes, modules, stages, biosocial theory, skills groups, consultation team) and third-wave therapies (ACT, MBCT), with evidence for borderline personality disorder and self-harm, comparators (MBT, GPM, schema, STEPPS), and stepped-care referral. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
1 MCQ with explanations
Target exams
Red flags
Fellowship exams test whether you can structure DBT, map biosocial theory to skills, choose ACT vs MBCT vs DBT, and avoid fidelity myths (everything mindfulness is not DBT; DBT is not always uniquely superior to good structured care).[4][6][11][16]
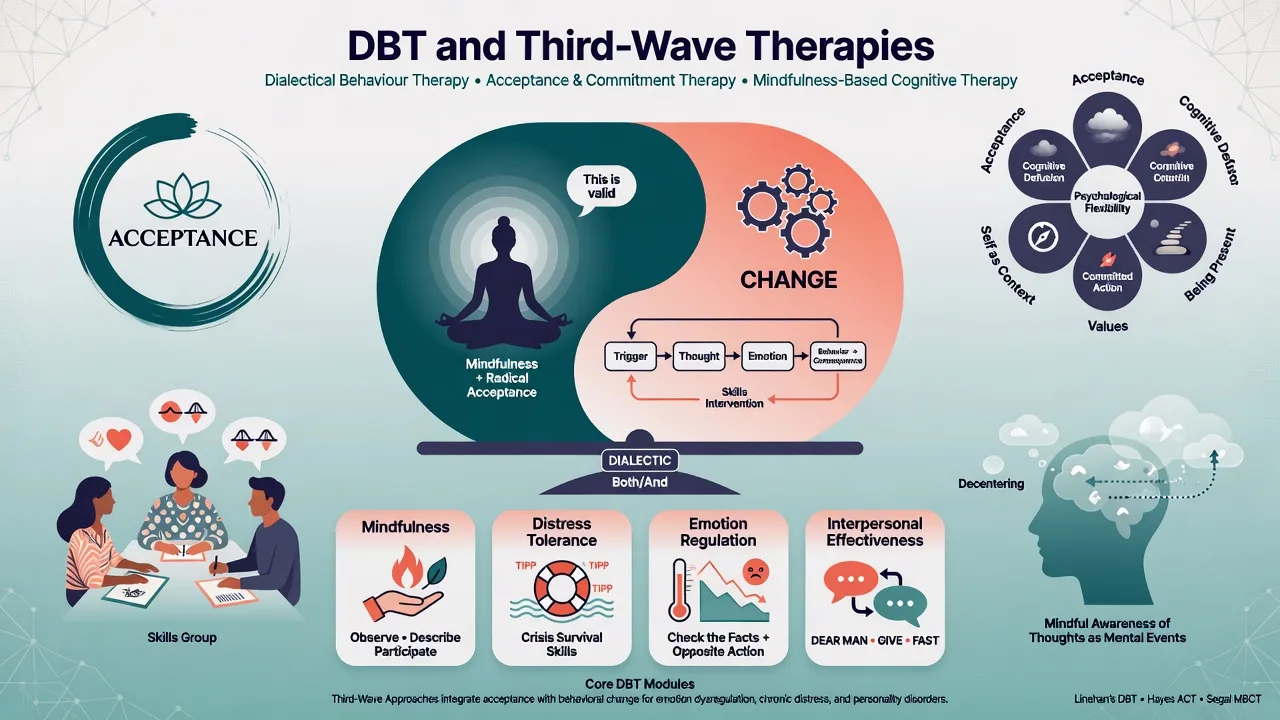
Definition and classification (third wave)
First-wave behavioural therapies emphasised contingency and exposure. Second-wave cognitive therapies targeted maladaptive thoughts and beliefs. Third-wave approaches retain behavioural technology but prioritise mindfulness, acceptance, metacognition, values, and contextual functional analysis rather than only content-challenging of thoughts.[11][13]
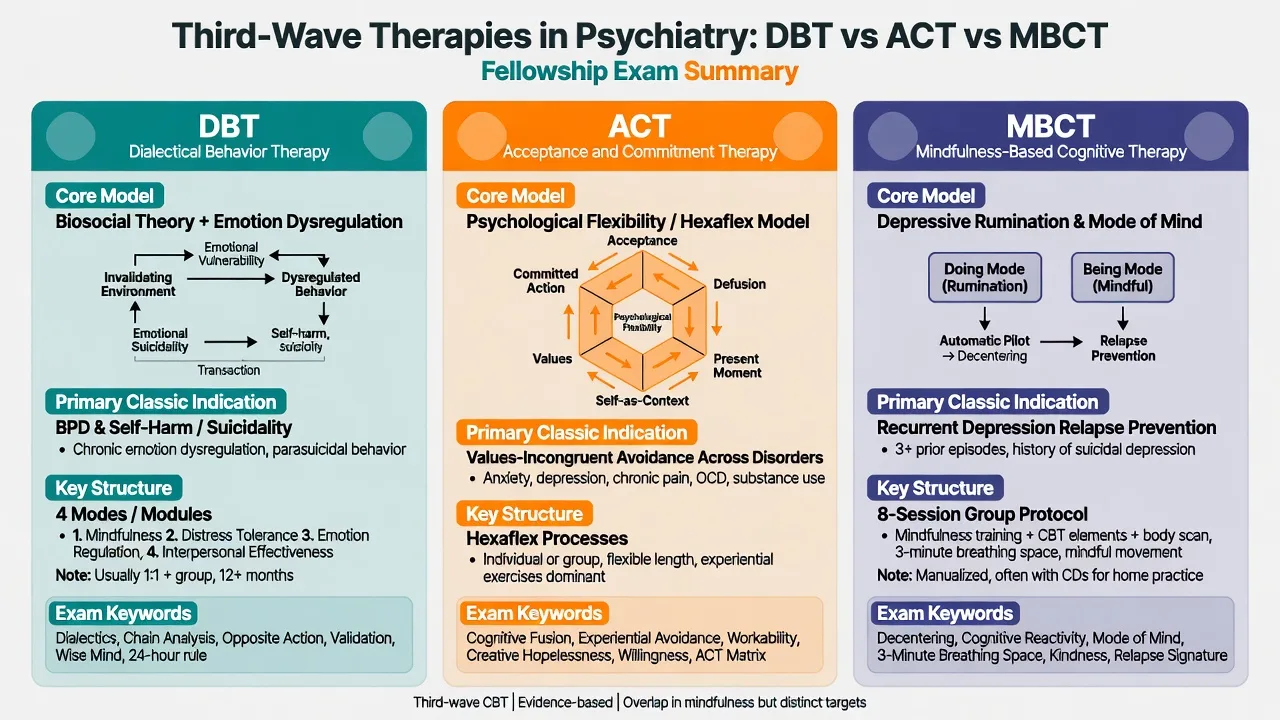
| Therapy | Core model | Classic exam indication | Structure high points |
|---|---|---|---|
| DBT | Biosocial emotion dysregulation; dialectic acceptance/change | BPD with self-harm/suicidality; severe emotion dysregulation | Four modes; four modules; stages; diary card |
| ACT | Psychological flexibility (hexaflex) | Transdiagnostic values-incongruent avoidance | Acceptance, defusion, present, self-as-context, values, committed action |
| MBCT | Depressive rumination and modes of mind | Recurrent major depression relapse prevention | Typically 8-session group + home practice |
Full-model DBT vs DBT-informed care: full model includes all four modes with consultation team and Stage 1 target hierarchy. Skills-only or “DBT-informed individual work” can help emotion dysregulation but is not interchangeable with comprehensive DBT for high-risk Stage 1 presentations when the full model is indicated.[3][18]
Biosocial theory (mechanism)
Linehan’s biosocial theory posits interaction of emotional vulnerability (high sensitivity, high reactivity, slow return to baseline), an invalidating environment (private experiences dismissed, punished, or oversimplified), and the outcome of pervasive emotion dysregulation with secondary interpersonal chaos, identity instability, and maladaptive regulation (including self-harm).[6]
Crowell, Beauchaine and Linehan elaborate a developmental biosocial model linking early impulsivity/emotional vulnerability with reinforcement of extreme emotional displays and invalidation over time.[6]
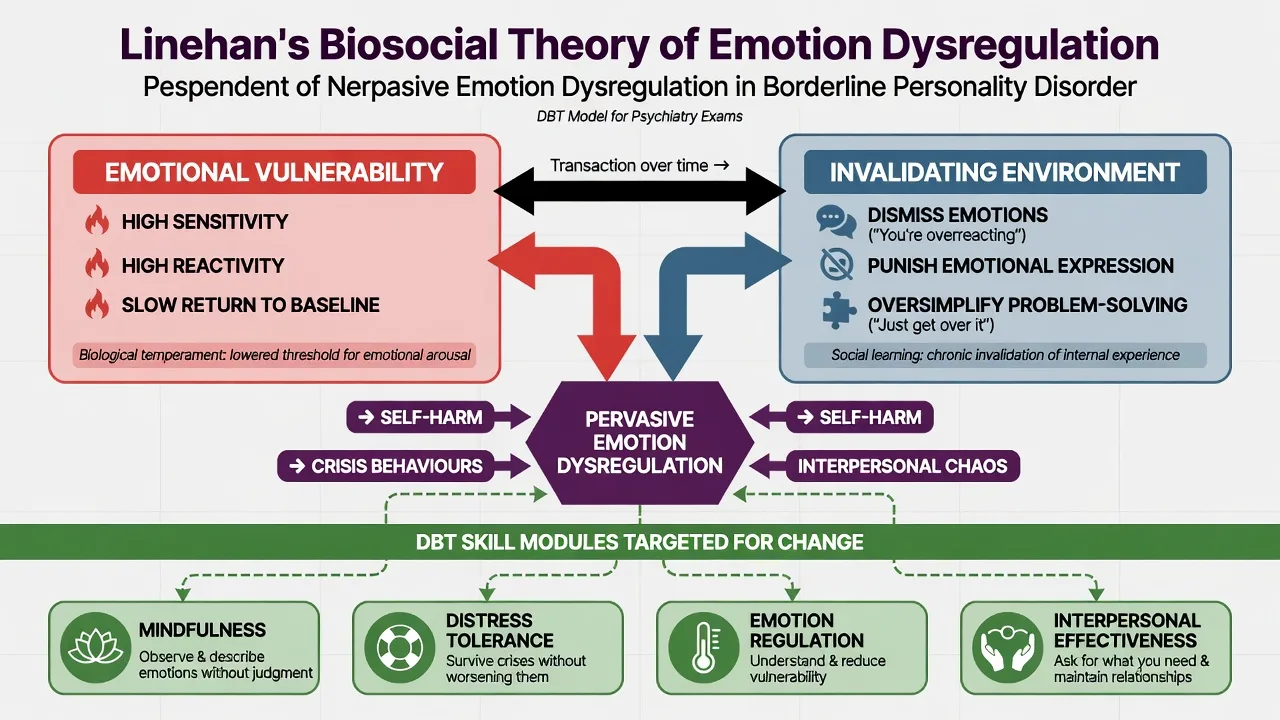
Exam mapping (high yield): awareness/self → mindfulness; crisis survival without making it worse → distress tolerance; chronic mood lability and vulnerability factors → emotion regulation; relationship chaos and assertion → interpersonal effectiveness.[6]
Standard DBT structure
Four modes
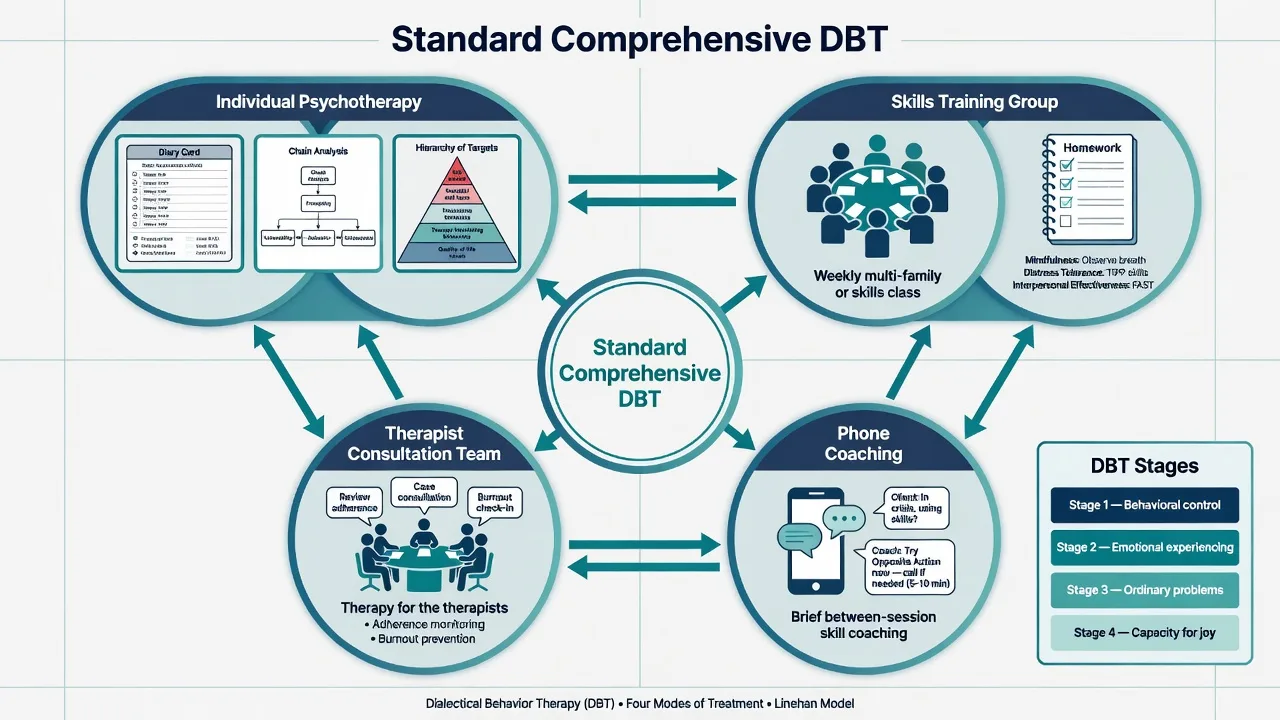
Individual psychotherapy uses diary card review, behavioural chain analysis, solution analysis, validation, contingency management, and commitment strategies. Skills training group provides didactic teaching and practice of the four modules with homework. Phone coaching is brief between-session coaching to generalise skills in real time (local protocols define after-hours limits and the classic “24-hour rule” after self-harm — know principles, do not invent local policy). Therapist consultation team is “therapy for the therapists”: adherence, dialectics, burnout prevention, and reduced iatrogenic invalidation.[1][2]
Stages and hierarchy of targets (Stage 1)
Stage 1 focuses on behavioural control: stop life-threatening behaviours and reduce therapy-interfering and severe quality-of-life interfering behaviours. Stage 2 addresses emotional experiencing / trauma-related suffering (e.g. PTSD work) once safety and behavioural control improve. Stage 3 targets ordinary happiness, life goals, and residual problems in living. Stage 4 (optional advanced teaching) concerns capacity for joy and freedom.[1][2]
Stage 1 session hierarchy (individual): (1) life-threatening behaviours → (2) therapy-interfering behaviours → (3) quality-of-life interfering behaviours → (4) skills generalisation.[1][2]
Four skills modules
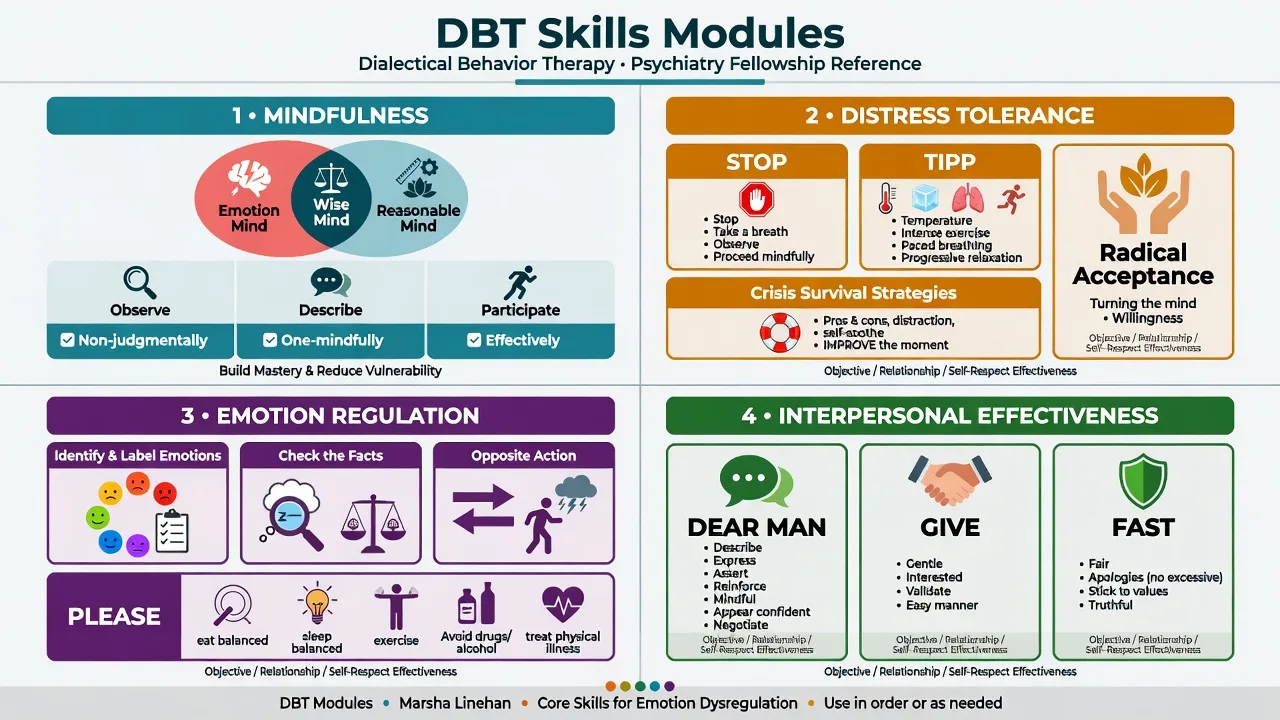
Mindfulness covers wise mind; “what” skills (observe, describe, participate); and “how” skills (non-judgementally, one-mindfully, effectively). Distress tolerance covers crisis survival (e.g. STOP, TIPP, ACCEPTS, IMPROVE, pros/cons), radical acceptance, and reality acceptance. Emotion regulation covers naming emotions, check the facts, opposite action, problem-solving, and PLEASE / reduce vulnerability. Interpersonal effectiveness covers objectives effectiveness (DEAR MAN), relationship effectiveness (GIVE), and self-respect (FAST). Adolescent programmes often add family “middle path” skills (dialectics, validation, behaviourism for families).[1][18]
Skills groups in practice
Skills groups are structured classes, not process psychotherapy. Expect orientation, teaching, practice, homework review, and clear attendance rules. Group is where skills are taught; individual therapy is where skills are applied to personal behavioural chains and motivation is sustained.[1][18]
ACT overview
Acceptance and commitment therapy targets psychological flexibility: contacting the present moment fully as a conscious human, and changing or persisting in behaviour in service of chosen values.[11]
Hexaflex processes: acceptance; cognitive defusion; contact with the present moment; self-as-context; values; committed action. Opposite processes (inflexibility) include experiential avoidance, cognitive fusion, dominance of the conceptualised self, and values-incongruent living.[11]
Meta-analytic evidence supports ACT for a range of mental and physical health problems versus control conditions, with ongoing debate about superiority over well-delivered CBT for all indications — know both the supportive meta-analysis and the critical third-wave review tradition.[12][13]
MBCT overview
Mindfulness-based cognitive therapy combines mindfulness practice with cognitive therapy elements to prevent depressive relapse/recurrence, particularly in people with recurrent depression. Classic programme structure is an eight-session group with daily home practice, teaching recognition of early relapse signatures and a shift from ruminative “doing” mode to “being” mode.[14][16]
Key evidence anchors: replication work showed differential prevention effects, historically strongest teaching for those with multiple prior episodes;[14] PREVENT (Kuyken et al., Lancet) found MBCT with support to taper medication was not inferior to maintenance antidepressant for relapse prevention in the trial’s primary analysis framework, with cost-effectiveness implications;[15] individual patient data meta-analysis supports MBCT for reducing relapse risk versus control conditions.[16]
Exam trap: MBCT is not first-line crisis treatment for acute severe depression with high suicide risk or for Stage 1 BPD behavioural dyscontrol.[14][16]
Evidence for BPD and self-harm
Landmark DBT trials
- Linehan 1991: foundational RCT in chronically parasuicidal borderline patients — reduced parasuicide and inpatient days versus treatment-as-usual in the classic early evidence base.[1]
- Linehan 2006: two-year RCT of DBT versus community treatment by experts — benefits on suicide attempts, emergency care, and treatment retention for many key outcomes.[2]
- Linehan 2015: high suicide risk BPD; component analysis comparing DBT interventions — informs which components matter for suicide/self-harm outcomes (skills vs individual components teaching point).[3]
- McMain 2009: DBT versus general psychiatric management (GPM) — both groups improved substantially; specialist DBT was not clearly superior on primary outcomes in the way candidates sometimes mythologise. This is a core FRANZCP/MRCPsych teaching point against DBT exceptionalism.[4]
- McMain 2022: 6 versus 12 months of DBT — non-inferiority findings for 6 months on key outcomes in that trial context; duration decisions remain clinical and service-dependent.[5]
- Bohus 2004: inpatient DBT programme effectiveness data supporting adapted intensive settings.[17]
Meta-analyses and specialised comparators
Psychotherapies for BPD (DBT among several specialised treatments) show overall efficacy versus control conditions for borderline-relevant and self-harm outcomes, though heterogeneity and comparator quality matter.[7][8][9] Mentalization-based treatment (MBT) versus structured clinical management is another high-yield specialised vs structured-generalist contrast.[10] Schema-focused therapy versus transference-focused psychotherapy and STEPPS group systems training expand the specialised/adjunct landscape beyond third-wave labels.[19][20]
Assessment and selection
Suitability for comprehensive DBT (typical): recurrent self-harm and/or chronic suicidality with emotion dysregulation / BPD features; willingness to work on staying alive and reducing target behaviours; ability (with adaptations) to attend individual + group commitments; and team capacity for consultation and phone coaching protocols.[1][2]
Assess and document: risk hierarchy; substance use; bipolar/psychosis; medical sequelae of self-harm/eating disorders; trauma load and Stage readiness; literacy/language/cultural needs; prior therapy dropouts.[2][6]
Chain analysis elements (individual session technology): vulnerability factors → prompting event → links (thoughts, emotions, sensations, behaviours, events) → problem behaviour → short- and long-term consequences → solution analysis (skills, prevention, repair).[1]
Acute and definitive management
Acute
Medical stabilisation and standard suicide/self-harm risk assessment outrank skills vocabulary. After safety is addressed, re-engage crisis survival skills and repair plans; avoid punitive discharge that recreates invalidation.[2][6]
Definitive / stepped care
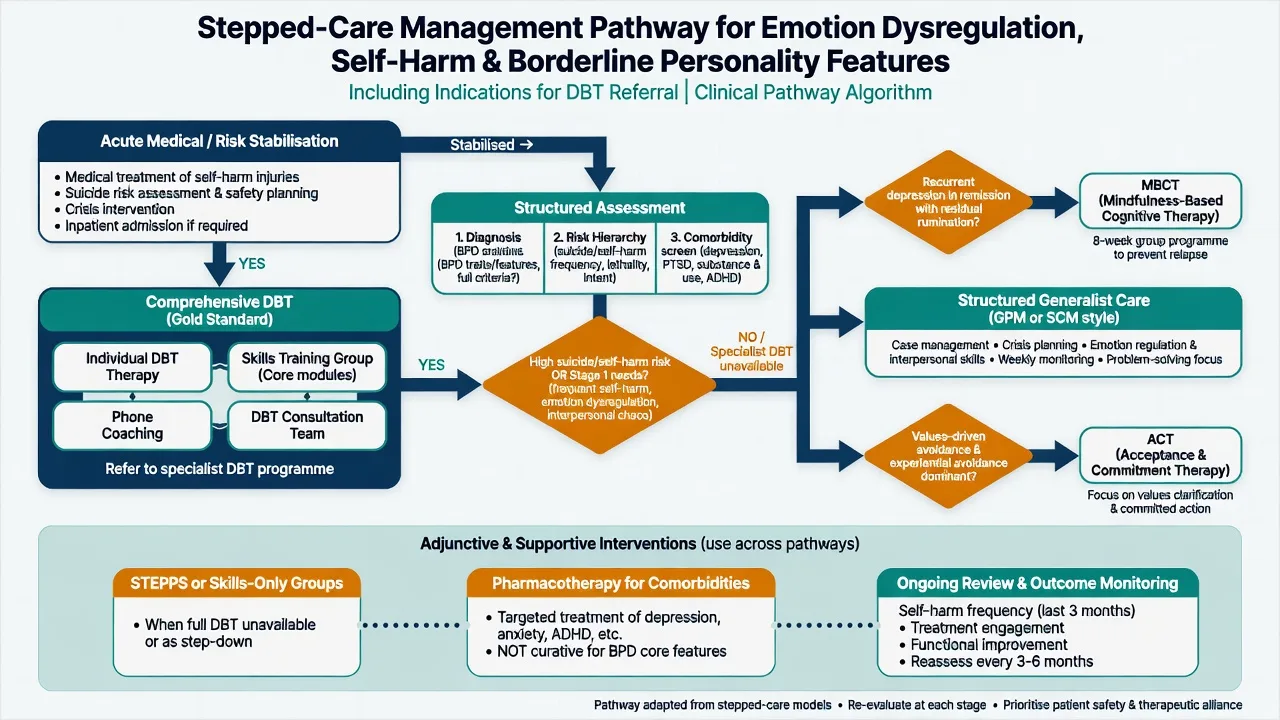
| Presentation | Prefer |
|---|---|
| BPD/emotion dysregulation with recurrent self-harm, Stage 1 targets | Comprehensive DBT if available and acceptable |
| Same presentation, specialist DBT unavailable | Structured generalist care (GPM/SCM-style): scheduled sessions, crisis plan, psychoeducation, treat comorbidities, clear goals |
| Recurrent depression in remission, relapse risk | MBCT (or maintenance antidepressant per shared decision) |
| Values-incongruent avoidance across disorders | ACT |
| Need for group skills adjunct without full DBT modes | STEPPS / DBT skills-informed groups (know limits for high-risk Stage 1) |
Medication: no pharmacological cure for BPD. Treat comorbid depression, anxiety, ADHD, substance use, sleep, and medical issues; avoid polypharmacy as a substitute for structured therapy and safety planning.[8]
Comparators and differentials (therapy choice)
- Emotion dysregulation + self-harm/suicide focus
- Four modes; skills modules; Stage hierarchy
- Biosocial theory and validation/change dialectic
- Psychological flexibility and values
- Hexaflex processes; defusion and acceptance
- Transdiagnostic applications with meta-analytic support
- Depressive relapse prevention
- 8-session mindfulness + CBT elements
- Strong evidence in recurrent depression pathways
Also distinguish MBT (mentalizing under attachment arousal), schema therapy, TFP, and GPM/SCM as examinable non-identical alternatives rather than synonyms for DBT.[4][10][20]
Pitfalls, special populations, prognosis
Special populations. Adolescents: multi-family DBT-A adaptations for self-harm. Trauma: sequence Stage 1 before intensive exposure. Cultural care: mindfulness and validation must be offered with cultural humility; adapt metaphors and group norms. Neurodivergence/intellectual disability: simplify skills, extend teaching, involve systems. Perinatal: safety, sleep, bonding, and joint perinatal planning first.[6][18]
Prognosis. Specialised psychotherapies improve borderline symptoms and reduce self-harm relative to poorly structured care in aggregate evidence; individual response varies. Engagement, alliance, practical access, substance use, and therapist adherence influence outcome. Plan for maintenance skills, booster contact, and step-down rather than abrupt discharge after crisis only.[7][8][9]
Regional practice notes
ANZ (FRANZCP). Public services often deliver partial DBT (skills groups ± individual work). Examiners expect honest stepped-care reasoning: full model when available and indicated; structured generalist care when not; clear crisis plans; local MH legislation principles without invented section numbers. Align with RANZCP clinical practice guidance themes: treat BPD as valid and treatable; offer structured psychological therapy; avoid therapeutic nihilism.[3][7]
UK (MRCPsych). NICE-aligned teaching emphasises structured psychological treatments for BPD and self-harm pathways; CASC stations test engagement, validation without collusion, and skills coaching tone.[7][8]
US (ABPN). APA-aligned evidence for specialised psychotherapies including DBT for BPD; know component analysis and generalist alternatives.[3][7]
Exam pearls
DBT skeleton (modes)
Map biosocial theory → four modules in one breath. Quote McMain 2009 when someone claims “only DBT works”. Name ACT hexaflex six processes under time pressure. MBCT = relapse prevention, not acute BPD crisis care. Chain analysis is the individual session “technology” examiners want. Consultation team protects patients from therapist burnout and invalidation. Third-wave ≠ “just accept everything”: includes change, skills, and committed action.[4][6][11][16]
References
See frontmatter PMIDs (all live-verified title/year). Landmark anchors: Linehan 1991/2006/2015; McMain 2009/2022; Cristea 2017; Storebø Cochrane 2020; Stoffers-Winterling 2022; Bateman 2009; Hayes 2006; A-Tjak 2015; Öst 2008; Ma and Teasdale 2004; Kuyken 2015/2016; Bohus 2004; Neacsiu 2014; Blum 2008; Giesen-Bloo 2006.[1][7][15]
References
- [1]Linehan MM, Armstrong HE, Suarez A, et al. Cognitive-behavioral treatment of chronically parasuicidal borderline patients Arch Gen Psychiatry, 1991.PMID 1845222
- [2]Linehan MM, Comtois KA, Murray AM, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder Arch Gen Psychiatry, 2006.PMID 16818865
- [3]Linehan MM, Korslund KE, Harned MS, et al. Dialectical behavior therapy for high suicide risk in individuals with borderline personality disorder: a randomized clinical trial and component analysis JAMA Psychiatry, 2015.PMID 25806661
- [4]McMain SF, Links PS, Gnam WH, et al. A randomized trial of dialectical behavior therapy versus general psychiatric management for borderline personality disorder Am J Psychiatry, 2009.PMID 19755574
- [5]McMain SF, Chapman AL, Kuo JR, et al. The Effectiveness of 6 versus 12 Months of Dialectical Behavior Therapy for Borderline Personality Disorder: A Noninferiority Randomized Clinical Trial Psychother Psychosom, 2022.PMID 35738244
- [6]Crowell SE, Beauchaine TP, Linehan MM A biosocial developmental model of borderline personality: Elaborating and extending Linehan's theory Psychol Bull, 2009.PMID 19379027
- [7]Cristea IA, Gentili C, Cotet CD, et al. Efficacy of Psychotherapies for Borderline Personality Disorder: A Systematic Review and Meta-analysis JAMA Psychiatry, 2017.PMID 28249086
- [8]Storebø OJ, Stoffers-Winterling JM, Völlm BA, et al. Psychological therapies for people with borderline personality disorder Cochrane Database Syst Rev, 2020.PMID 32368793
- [9]Stoffers-Winterling JM, Storebø OJ, Kongerslev MT, et al. Psychotherapies for borderline personality disorder: a focused systematic review and meta-analysis Br J Psychiatry, 2022.PMID 35088687
- [10]Bateman A, Fonagy P Randomized controlled trial of outpatient mentalization-based treatment versus structured clinical management for borderline personality disorder Am J Psychiatry, 2009.PMID 19833787
- [11]Hayes SC, Luoma JB, Bond FW, et al. Acceptance and commitment therapy: model, processes and outcomes Behav Res Ther, 2006.PMID 16300724
- [12]A-Tjak JG, Davis ML, Morina N, et al. A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems Psychother Psychosom, 2015.PMID 25547522
- [13]Ost LG Efficacy of the third wave of behavioral therapies: a systematic review and meta-analysis Behav Res Ther, 2008.PMID 18258216
- [14]Ma SH, Teasdale JD Mindfulness-based cognitive therapy for depression: replication and exploration of differential relapse prevention effects J Consult Clin Psychol, 2004.PMID 14756612
- [15]Kuyken W, Hayes R, Barrett B, et al. Effectiveness and cost-effectiveness of mindfulness-based cognitive therapy compared with maintenance antidepressant treatment in the prevention of depressive relapse or recurrence (PREVENT): a randomised controlled trial Lancet, 2015.PMID 25907157
- [16]Kuyken W, Warren FC, Taylor RS, et al. Efficacy of Mindfulness-Based Cognitive Therapy in Prevention of Depressive Relapse: An Individual Patient Data Meta-analysis From Randomized Trials JAMA Psychiatry, 2016.PMID 27119968
- [17]Bohus M, Haaf B, Simms T, et al. Effectiveness of inpatient dialectical behavioral therapy for borderline personality disorder: a controlled trial Behav Res Ther, 2004.PMID 15033496
- [18]Neacsiu AD, Eberle JW, Kramer R, et al. Dialectical behavior therapy skills for transdiagnostic emotion dysregulation: a pilot randomized controlled trial Behav Res Ther, 2014.PMID 24974307
- [19]Blum N, St John D, Pfohl B, et al. Systems Training for Emotional Predictability and Problem Solving (STEPPS) for outpatients with borderline personality disorder: a randomized controlled trial and 1-year follow-up Am J Psychiatry, 2008.PMID 18281407
- [20]Giesen-Bloo J, van Dyck R, Spinhoven P, et al. Outpatient psychotherapy for borderline personality disorder: randomized trial of schema-focused therapy vs transference-focused psychotherapy Arch Gen Psychiatry, 2006.PMID 16754838