Psych · Professional — doctor health, burnout and impairment
Doctor health, burnout and impairment
Also known as Physician burnout · Doctor wellbeing · Occupational burnout · Physician impairment · Physician health programme · Junior doctor mental health · Presenteeism · Moral injury in medicine · Maslach burnout
Exam-exhaustive fellowship reference on doctor health, Maslach three-dimension burnout, ICD-11 occupational framing, epidemiology and suicide risk, differential from depression and substance use, assessment, organisation- vs individual-directed interventions, impairment and mandatory reporting principles, physician health programmes, trainee risks, stigma and help-seeking, and regional doctor-health systems. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Doctor health is the physical, psychological, and occupational wellbeing that enables safe, compassionate practice. Fellowship exams test it because psychiatrist candidates will supervise trainees, manage impaired colleagues, sit on clinical governance committees, and are themselves high-risk for occupational distress.[11][3]
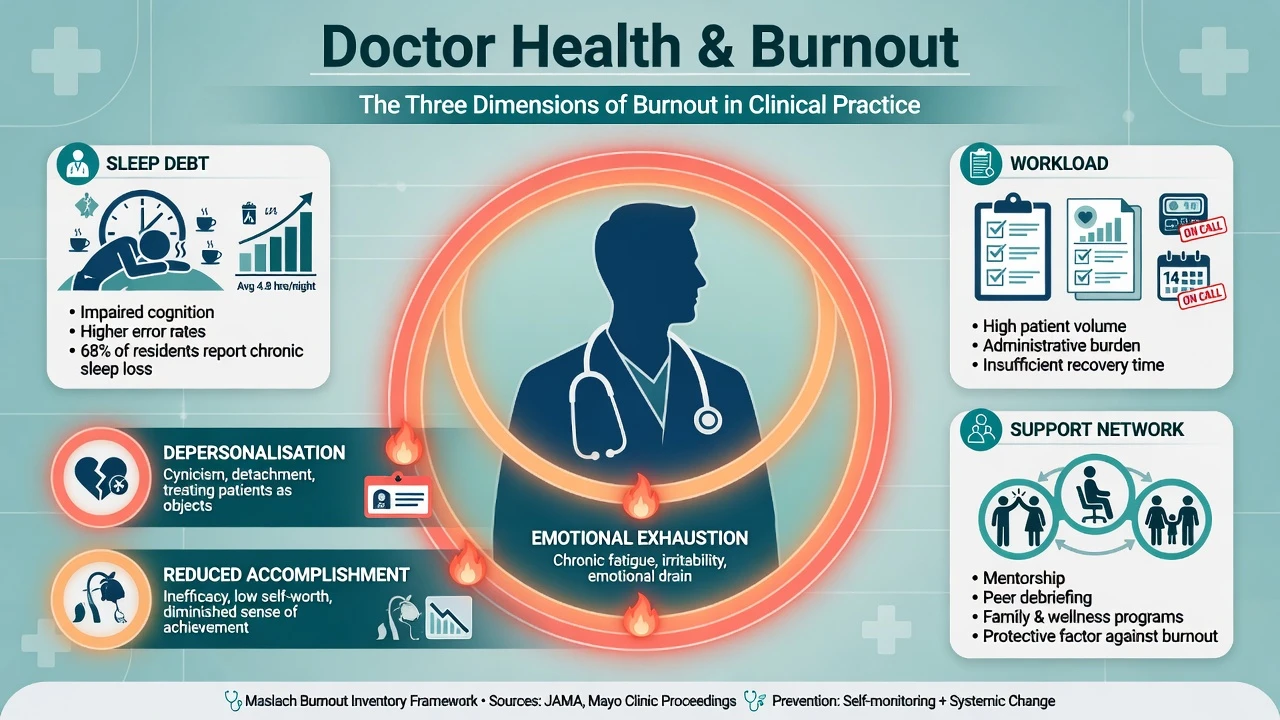
Burnout is a prolonged response to chronic emotional and interpersonal job stressors. The Maslach framework defines three core dimensions: emotional exhaustion (depleted capacity), depersonalisation/cynicism (detached, callous, or objectifying stance toward people one serves), and reduced personal accomplishment (sense of inefficacy).[1]
ICD-11 lists burnout as an occupational phenomenon associated with employment (not a free-standing mental disorder classification equivalent to major depression). DSM-5-TR does not diagnose “burnout” as a primary psychiatric disorder. Exam language: burnout is a signal of person–job mismatch, not a personal moral failure, and it can coexist with or progress to clinical mental illness.[1][3]
Impairment means a health condition (including substance use, severe mental illness, cognitive decline, or extreme fatigue) that adversely affects the ability to practise medicine safely. Not every burned-out doctor is impaired; not every impaired doctor looks “burned out.” Confusing the two is a classic viva trap.[11][12]
Related constructs examiners may mix in stems. Burnout sits alongside depression, moral injury, compassion fatigue, presenteeism, and engagement as non-identical occupational and clinical concepts.[1][3][14]
| Construct | Core idea | Exam discriminator |
|---|---|---|
| Burnout | Work-tied EE + cynicism + inefficacy | Improves with job redesign more than pure “self-care” |
| Major depression | Pervasive mood syndrome | Anhedonia, worthlessness, neurovegetative signs beyond work |
| Compassion fatigue | Secondary cost of caring | Trauma exposure salience |
| Moral injury | Betrayal of deeply held values by system constraints | Guilt/anger at forced care compromise |
| Presenteeism | Working while unwell | Culture of stoicism; safety risk |
| Engagement | Maslach antithesis — energy, involvement, efficacy | Organisational target state |
Classification — Maslach dimensions and framing
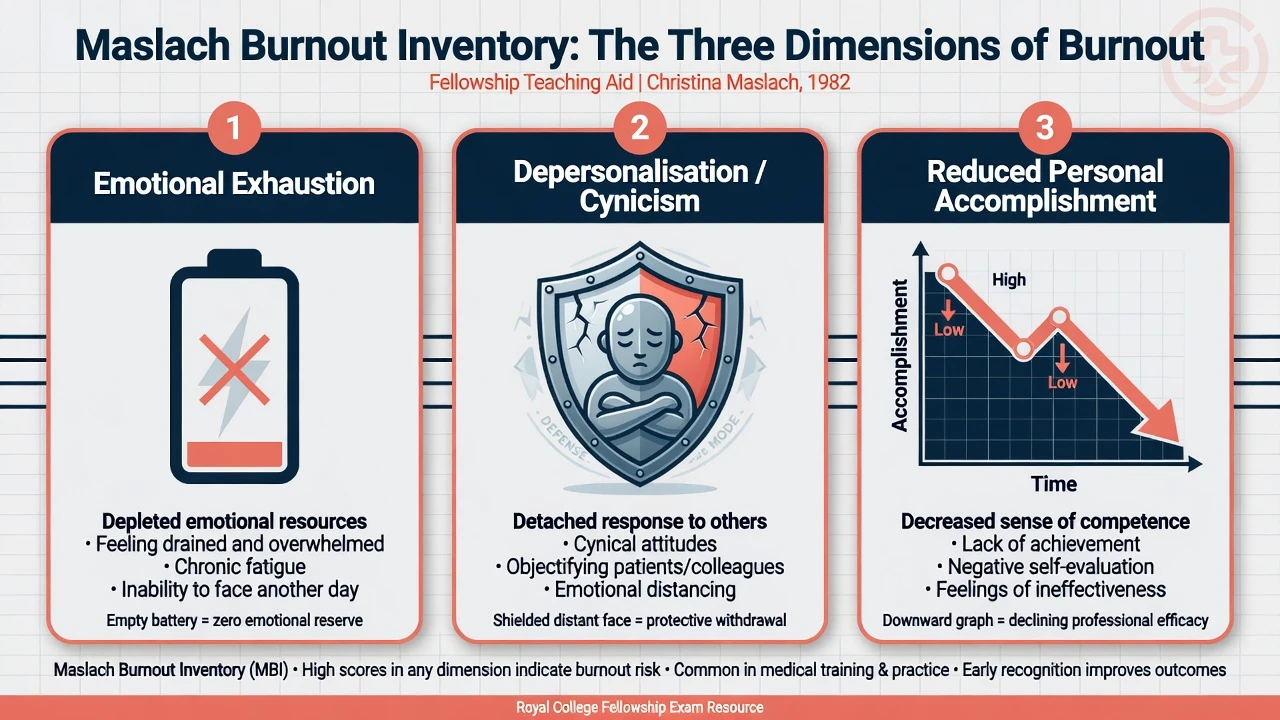
The Maslach Burnout Inventory (MBI) operationalises the three dimensions and underpins most physician research, but thresholds and prevalence definitions vary widely across studies — a point Rotenstein and colleagues emphasised when overall burnout estimates ranged from essentially zero to over 80% depending on definition.[1][4]
- Feeling drained
- Cannot face another day
- Core of most self-reports
- Often first to rise with overload
- Cynicism about patients
- Emotional distancing
- Objectifying language
- Protective armour that harms care
- Sense of inefficacy
- Lost meaning
- Self-doubt despite competence
- Linked to disengagement
Epidemiology and risk
National US samples found physicians more burned out and less satisfied with work–life balance than the general working population, with further worsening between 2011 and 2014 in longitudinal comparisons.[5][6] Front-line access specialties often show higher rates; measurement heterogeneity means candidates should quote patterns and ranges, not a single global percentage as gospel.[4][5]
Among residents, meta-analysis estimated depression or depressive symptoms at roughly 29% (range about 21–43% by instrument), far above general population expectations for comparable age groups.[7] Narrative synthesis confirms substantial burnout across medical students and residents, with training-structure drivers (hours, hierarchy, mistreatment, debt, evaluation threat).[15]
In Australia, junior doctor surveys link longer average weekly working hours with common mental disorder and suicidal ideation, and identify modifiable workplace stressors beyond hours alone.[13][17]
Physician suicide remains a critical red-thread topic. Classic meta-analysis found elevated suicide rate ratios for physicians versus the general population, with a particularly high elevation among women physicians.[9] Later systematic work continues to identify physicians as an at-risk group, with gender differentials and secular trends that candidates should discuss carefully rather than with outdated single-number certainty.[10]
Mechanisms — why doctors burn out
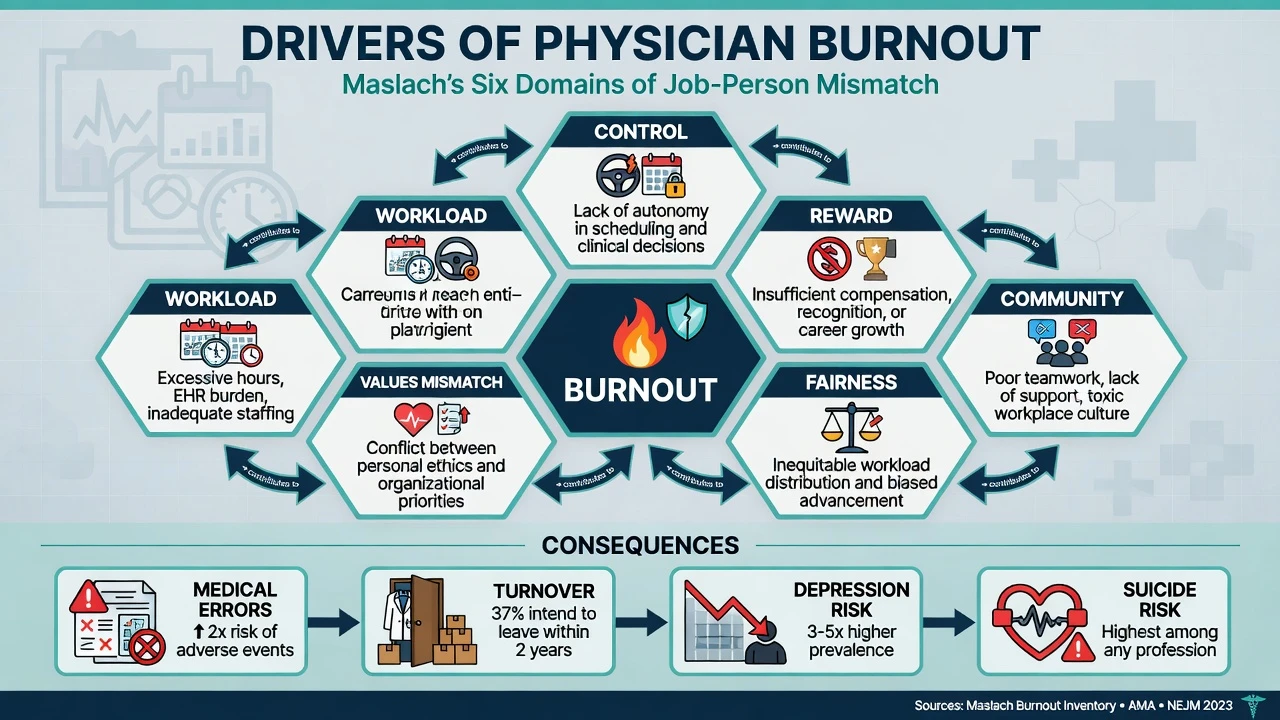
Burnout is best understood as chronic mismatch between the person and job across domains of workload, control/autonomy, reward (financial and recognition), community/collegiality, fairness, and values alignment.[1][3] Work-related risk factors for common mental disorders more broadly include high job demands, low control, effort–reward imbalance, bullying, and organisational injustice — all highly relevant to medical workplaces.[14]
Mechanistic layers examiners expect combine job-demand models with emotional labour, moral injury, stigma, and safety cascades.[1][3][14]
- Demand overload — hours, after-hours inbox, documentation burden, understaffing → sleep debt and decision fatigue.[3][13]
- Autonomy erosion — loss of control over schedule, targets, and clinical decision space.[3]
- Emotional labour — continuous empathy under time pressure; depersonalisation as maladaptive armour.[1]
- Moral injury — being forced to deliver care below one’s standard by system constraints → shame, anger, cynicism.[3]
- Stigma loop — perfectionism and identity as “the strong helper” block help-seeking until crisis.[11]
- Safety cascade — exhaustion and detachment associate with higher reported medical error and poorer unit safety climates.[16]
Clinical presentations (exam stems)
Classic stems: the exhausted registrar with a near-miss prescribing error; the consultant smelling of alcohol before clinic; the trainee with progressive cynicism and tears after nights; the rural psychiatrist isolated with dual roles and no peer cover; the doctor with suicidal ideation after a complaint or serious adverse event; the mid-career clinician planning to leave medicine; the senior clinician with subtle cognitive slips.[3][11][13]
Symptoms and signs: exhaustion, irritability, insomnia, somatic complaints, detachment from patients, dark humour that becomes cruelty, rising substance use, presenteeism, documentation decline, lateness, isolation from peers, and clusters of patient or staff complaints.[3][11]
Differential diagnosis
| Presentation | Favours burnout | Favours clinical illness / other |
|---|---|---|
| Low mood | Worse on workdays; improves on leave | Pervasive anhedonia, guilt, morning severity |
| Detachment | Cynical about “the system/patients” | Blunted affect of severe depression or psychosis |
| Substance use | Self-medication for sleep/stress | Loss of control, withdrawal, diversion |
| Cognitive slips | Fatigue-related, reverse with rest | Progressive decline, neurological red flags |
| Suicidality | May still occur in pure burnout context | Always treat as psychiatric emergency regardless of label |
| Performance issues | Correlates with roster/load | May need fitness-for-duty assessment |
Never stop at “burnout” without screening depression, anxiety, PTSD/secondary trauma, substance use, bipolar disorder if indicated, and suicide risk. Mislabeling major depression as burnout delays treatment and can kill.[7][11]
Assessment
There is no blood test for burnout. Assessment is clinical, occupational, and safety-focused.[3][11]
SAFER-DOC
Practical steps: private conversation with specific behavioural observations (not vague character attack); screen PHQ-9 or equivalent, substance use, and suicide; clarify whether immediate removal from duties is required; offer confidential physician-health support; involve clinical lead when patient safety is at stake; document facts objectively.[11][12]
MBI and similar scales are useful in research and programme evaluation; clinical decisions about fitness rest on functional safety, not a single cut-score alone, given threshold heterogeneity.[4]
Investigations and “work-up”
- Medical work-up as indicated for depression differentials, cognitive decline, or substance sequelae — not for burnout per se.[11]
- Occupational health / fitness-for-duty assessment when impairment is suspected.[12]
- Systems review: rostering, staffing ratios, bullying, complaint load, electronic health record burden.[3][17]
- Separate voluntary confidential care (where law protects it) from mandatory public-protection reporting when thresholds are met — jurisdiction-specific.[12]
Immediate management (resuscitation of safety)
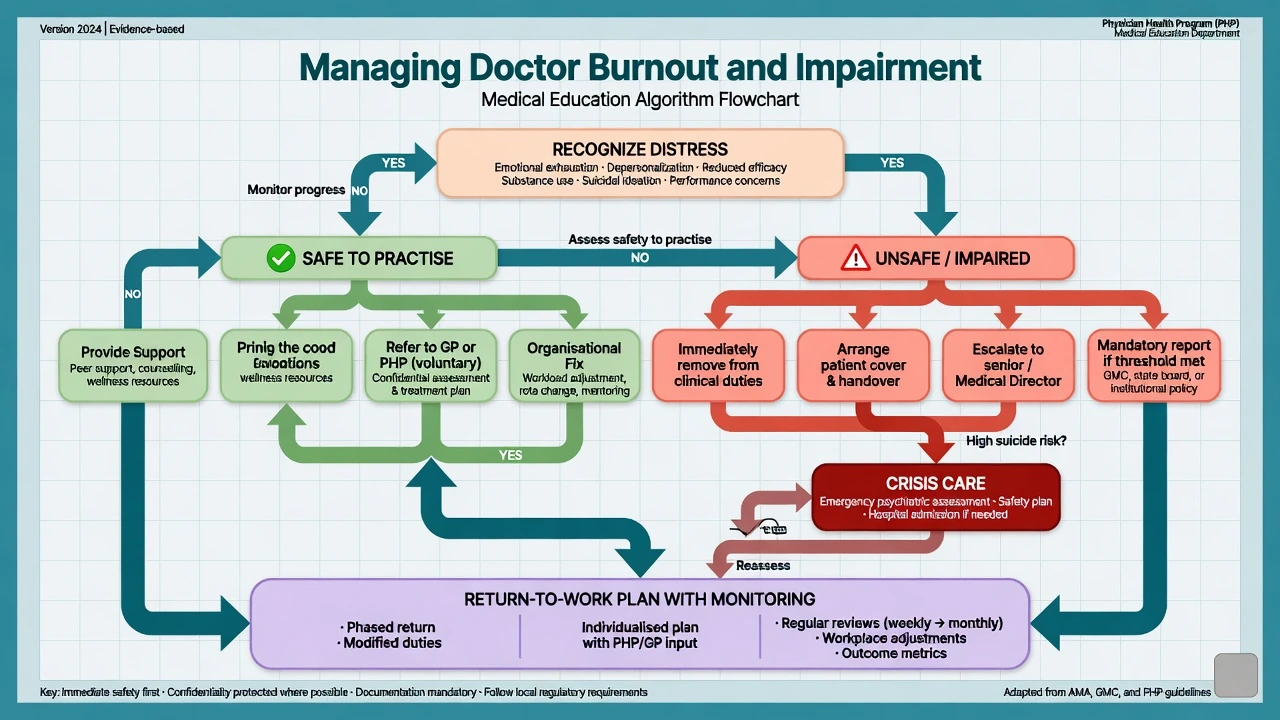
If unsafe to practise (intoxication, severe cognitive impairment, acute suicidality with inability to work safely, gross boundary collapse): remove from clinical duties immediately; arrange patient cover and handover; escalate to senior/medical director; do not allow further independent care; arrange crisis psychiatric care if suicide risk is high; follow local mandatory reporting when thresholds for risk to the public are met.[11][12]
If distressed but currently safe: validate; reduce acute load if possible; ensure they have a treating GP/psychiatrist pathway; peer support; consider temporary roster adjustment; monitor; address organisational drivers, not only individual coping.[2][3][8]
Do not shame. Do not ignore. Do not collude with secrecy that endangers patients. Loyalty never outranks safety.[12]
Definitive management — individual and organisational
Evidence hierarchy
Systematic reviews and meta-analyses show that interventions can reduce physician burnout, with organisation-directed approaches (workflow redesign, staffing, local practice modifications, reduced clerical load, improved team support) often producing larger effects than physician-directed strategies alone (mindfulness, small-group discussion, individual skills).[2][8] Individual programmes still help; the exam pearl is that resilience workshops without system change are incomplete.[2][3][8]
| Level | Examples | Evidence note |
|---|---|---|
| Organisation-directed | Roster redesign, scribes/EHR optimisation, leadership, staffing, psychological safety | Larger effects in meta-analyses |
| Physician-directed | Mindfulness, CBT skills, small peer groups, coaching | Modest benefits; adjunctive |
| Clinical treatment | Antidepressants, psychotherapy, SUD treatment for comorbid illness | Treat as for any patient — evidence-based care |
| PHP / regulated pathway | Assessment, monitoring, RTW agreements | For impairment / public protection interface |
Individual care
Treat sleep debt, depression, anxiety, and substance use with the same standard of care offered to any patient. Psychotherapy (CBT, IPT, trauma-focused work when indicated), social support, exercise, and negotiated workload matter. Encourage a treating relationship outside the workplace hierarchy when feasible.[3][11] For major depression, standard antidepressant selection and monitoring apply as for non-physician patients; doses and agents are not unique because the patient is a doctor — confidentiality and dual-role risks are the special features.[7][11]
Organisational care
Address the six worklife domains: reduce excessive hours and after-hours messaging culture; restore autonomy where possible; ensure fair recognition; build community and peer debrief; improve procedural justice in complaints; align stated values with resource reality.[1][3][17] Mentally healthy workplace frameworks emphasise multi-level prevention (job design, culture, manager capability, early intervention, and recovery supports) rather than individual resilience alone.[18]
Physician Health Programmes (PHP)
PHPs (names and structures vary by jurisdiction) offer assessment, facilitated treatment, and monitoring for doctors with mental illness, substance use, or other impairing conditions, often aiming for safe return to practice. Candidates should know the concept — confidential support where possible, public protection when necessary — without inventing local form codes.[11][12]
Return to work
Staged duties, clear supervision, measurable safety markers, ongoing treatment engagement, and scheduled review. Premature full unrestricted return after severe impairment is an exam fail.[11][12]
Special populations and scenarios
Trainees and medical students. High rates of burnout and depressive symptoms; hierarchy and evaluation fear block disclosure; duty-hour and culture reforms are organisational duties, not optional kindness.[7][15][13]
Women physicians. Classic suicide meta-analysis showed particularly elevated rate ratios; work–home conflict and gendered career penalties remain exam-relevant social determinants.[9][10]
Rural and remote. Isolation, dual relationships, limited locum cover, and distant PHP access amplify risk; telehealth peer support and proactive rostering matter.[3][11]
Psychiatrists. High emotional labour, vicarious trauma, complex risk decisions, and boundary strain (see ethics topic) contribute; supervision and consultation groups are protective infrastructure, not luxury.[3][11]
After complaint or serious adverse event. Second-victim phenomenon: shame, hypervigilance, suicide risk spike — early structured support and fair process reduce harm.[11]
Older clinicians. Consider cognitive impairment, sensory loss, and illness; fitness assessment must be respectful and safety-based, not ageist prejudice alone.[11]
Complications and pitfalls
Classic pitfalls: treating burnout as personal weakness; resilience theatre without redesign; missing depression/SUD; failing to act on an impaired colleague from loyalty; inventing mandatory-reporting statute numbers; breaching confidentiality of voluntary treatment when not required; punishing help-seeking; ignoring suicide risk after regulatory stress; equating presenteeism with professionalism; and quoting a single burnout prevalence as if measurement were uniform.[4][8][11][12]
Prognosis and disposition
Burnout is often reversible when job mismatch is corrected and recovery time is protected. Untreated trajectories include chronic illness, medical error, early exit from medicine, relationship breakdown, and suicide.[3][16] Impairment outcomes depend on insight, illness type, engagement with treatment/PHP, and monitoring quality.[11][12]
Disposition options: continue with support; temporary leave; restricted practice; full return with monitoring; career transition. Document fitness reasoning factually.[12]
Evidence, guidelines, and regional differences
Landmark anchors: Maslach construct review; Shanafelt national samples and time trends; Rotenstein prevalence heterogeneity; West Lancet intervention meta-analysis; Panagioti organisation-vs-individual meta-analysis; Mata resident depression; Dyrbye trainee narrative; Schernhammer and Dutheil on suicide; Brooks on doctors’ mental health services; Harvey work-and-mental-illness meta-review; Petrie ANZ junior doctor studies; Tawfik on burnout and reported errors; Bismark on Australian mandatory reporting tensions.[1][2][4][5][7][8][9][12][13][16]
[11] [12]Exam pearls
Hero overview figure
References
- [1]Maslach C, Schaufeli WB, Leiter MP Job burnout Annu Rev Psychol, 2001.PMID 11148311
- [2]West CP, Dyrbye LN, Erwin PJ, Shanafelt TD Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis Lancet, 2016.PMID 27692469
- [3]West CP, Dyrbye LN, Shanafelt TD Physician burnout: contributors, consequences and solutions J Intern Med, 2018.PMID 29505159
- [4]Rotenstein LS, Torre M, Ramos MA, et al. Prevalence of Burnout Among Physicians: A Systematic Review JAMA, 2018.PMID 30326495
- [5]Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population Arch Intern Med, 2012.PMID 22911330
- [6]Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in Burnout and Satisfaction With Work-Life Balance in Physicians and the General US Working Population Between 2011 and 2014 Mayo Clin Proc, 2015.PMID 26653297
- [7]Mata DA, Ramos MA, Bansal N, et al. Prevalence of Depression and Depressive Symptoms Among Resident Physicians: A Systematic Review and Meta-analysis JAMA, 2015.PMID 26647259
- [8]Panagioti M, Panagopoulou E, Bower P, et al. Controlled Interventions to Reduce Burnout in Physicians: A Systematic Review and Meta-analysis JAMA Intern Med, 2017.PMID 27918798
- [9]Schernhammer ES, Colditz GA Suicide rates among physicians: a quantitative and gender assessment (meta-analysis) Am J Psychiatry, 2004.PMID 15569903
- [10]Dutheil F, Aubert C, Pereira B, et al. Suicide among physicians and health-care workers: A systematic review and meta-analysis PLoS One, 2019.PMID 31830138
- [11]Brooks SK, Gerada C, Chalder T Review of literature on the mental health of doctors: are specialist services needed? BMC Med, 2011.PMID 21275504
- [12]Bismark MM, Mathews B, Morris JM, et al. Views on mandatory reporting of impaired health practitioners by their treating practitioners: a qualitative study from Australia BMJ Open, 2016.PMID 27993902
- [13]Petrie K, Crawford J, LaMontagne AD, et al. Working hours, common mental disorder and suicidal ideation among junior doctors in Australia: a cross-sectional survey BMJ Open, 2020.PMID 31964674
- [14]Harvey SB, Modini M, Joyce S, et al. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems Occup Environ Med, 2017.PMID 28108676
- [15]Dyrbye L, Shanafelt T A narrative review on burnout experienced by medical students and residents Med Educ, 2016.PMID 26695473
- [16]Tawfik DS, Profit J, Morgenthaler TI, et al. Physician Burnout, Well-being, and Work Unit Safety Grades in Relationship to Reported Medical Errors Mayo Clin Proc, 2018.PMID 30001832
- [17]Petrie K, Crawford J, Shand F, Harvey SB Workplace stress, common mental disorder and suicidal ideation in junior doctors Intern Med J, 2021.PMID 33135841
- [18]Petrie K, Joyce S, Tan L, et al. A framework to create more mentally healthy workplaces: A viewpoint Aust N Z J Psychiatry, 2018.PMID 28835112