Psych · Professional practice — epidemiology and public mental health
Epidemiology and public mental health
Also known as Psychiatric epidemiology · Public mental health · Global burden of disease mental disorders · DALY mental health · Treatment gap psychiatry · Social determinants mental health · Prevention continuum mental disorders · WMH survey · National Survey of Mental Health and Wellbeing
Exam-exhaustive epidemiology and public mental health for FRANZCP and MRCPsych: measures of occurrence; GBD/YLD/DALY; global and Australian prevalence; age-of-onset and sex patterns; social determinants and ACEs; Rose and Gordon prevention strategies; treatment gap, stepped care and task-sharing; suicide population rates; stigma; STROBE-linked critical appraisal of surveys. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags

1. Definitions and the examiner map
Psychiatric epidemiology studies how mental disorders are distributed (person, place, time) and what determines that distribution. Goals include aetiology, natural history, prevention targets, and rational service planning.[3][5]
Public mental health is the population application of that knowledge: mental health promotion, disorder prevention, early intervention, equitable treatment coverage, and recovery-oriented systems, including rights and anti-stigma work.[9][23]
Distinguish carefully in viva (measures and treatment-gap concepts are examinable staples of WMH/GBD-informed teaching):[1][5][16]
| Construct | Meaning | Exam trap |
|---|---|---|
| Disorder (threshold) | Meets operational diagnostic criteria | Not equal to distress or low wellbeing |
| Psychological distress | Symptom burden, often continuous | High distress ≠ automatic DSM/ICD case |
| Incidence | New cases per population-time | Confused with admission rates |
| Point prevalence | Cases at a single time | Underestimates episodic disorders |
| Period prevalence (e.g. 12-month) | Cases during interval | Best single metric for current need |
| Lifetime prevalence | Ever met criteria | Recall bias; not current caseload |
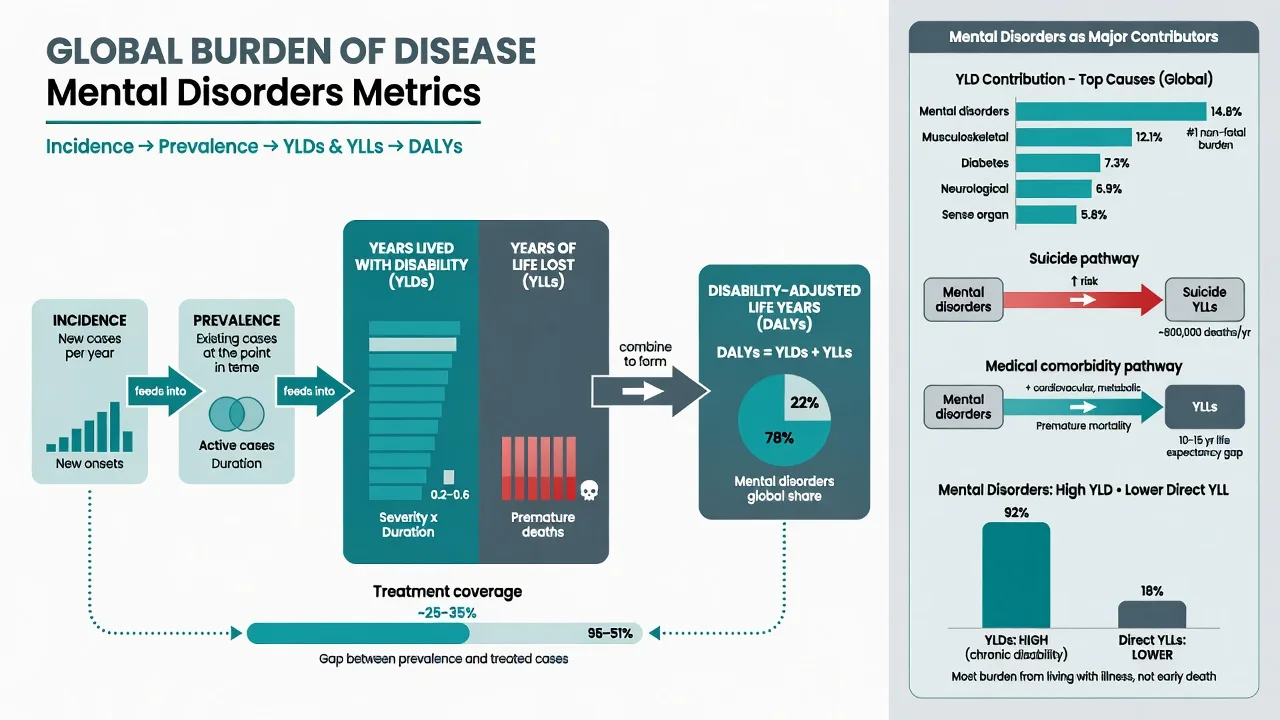
| DALY | YLD + YLL | Mental disorders: high YLD, lower direct YLL |
| Treatment gap | Proportion needing care who do not receive it | Not the same as "never sought help once" |
Classification for surveys. Fully structured instruments (e.g. CIDI) enable large samples with lay interviewers; semi-structured clinical interviews (e.g. SCAN) trade scale for clinical depth. DSM vs ICD thresholds change prevalence — always ask which system and which version.[5][6]
2. Measures of occurrence and burden
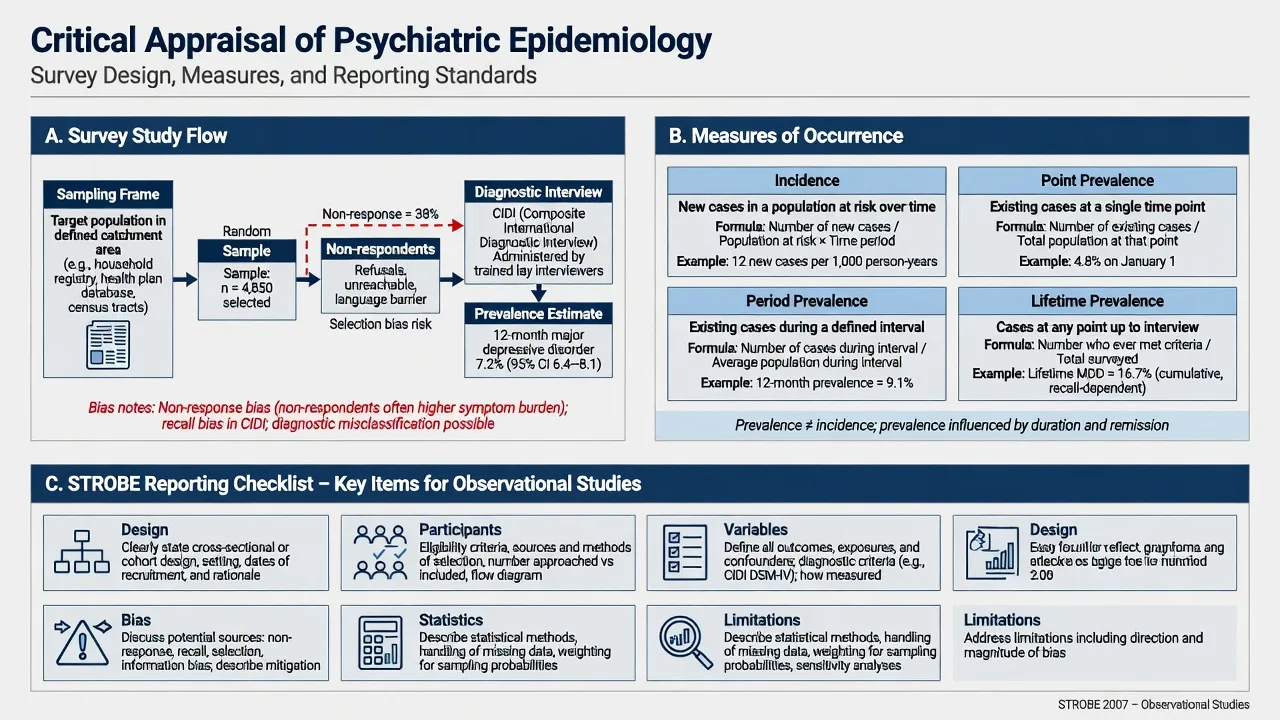
2.1 Core formulae (must-state)
- Incidence rate ≈ new cases / population-time at risk.
- Point prevalence ≈ existing cases / population at a time point.
- Period prevalence ≈ cases during a defined period / average population.
- Lifetime prevalence ≈ ever-affected / surveyed population (cumulative, recall-sensitive).
- Prevalence ≈ incidence × average duration (steady-state heuristic) — chronic or poorly treated disorders accumulate prevalence; these measures underpin survey reporting and service-need estimation.[5][6][22]
2.2 Disability and mortality metrics
YLDs capture non-fatal health loss (prevalence × disability weight). YLLs capture premature mortality. DALYs = YLDs + YLLs. Mental and substance use disorders are major contributors to global disability; direct cause-coded deaths are fewer than for many physical NCDs, but suicide and excess medical mortality matter clinically and for policy.[1][2]
Vigo and colleagues argue conventional GBD framing underestimates true mental illness burden when self-harm coding, some neurological interfaces, and risk-factor pathways are incompletely attributed — use this as a critical-appraisal pearl, not as a reason to invent alternative percentages in exams.[7]
2.3 Association metrics (link to critical appraisal)
Relative risk (RR), odds ratio (OR), risk difference, and population attributable fraction translate determinants into prevention impact. Always pair relative with absolute measures — classic Paper B / FRANZCP trap shared with the critical appraisal topic and with STROBE-disciplined interpretation of observational estimates.[22][10]
3. Prevalence, age-of-onset, and patterns
3.1 Common mental disorders globally
Steel and colleagues' meta-analysis of surveys (1980–2013) found substantial period prevalence of common mental disorders with heterogeneity by region, instrument, and conflict exposure — examiners want the order of magnitude and sources of variation, not a single magic percentage memorised out of context.[3]
3.2 Lifetime risk and age-of-onset (NCS-R classic)
In the US National Comorbidity Survey Replication, lifetime prevalence of any DSM-IV disorder was high (about half of respondents met criteria for at least one disorder at some point), with median ages of onset earliest for anxiety disorders and impulse-control disorders, intermediate for substance use, and later for mood disorders.[4] Pearl: half of lifetime cases start by adolescence/early adulthood — prevention and youth services are not optional extras.
3.3 World Mental Health Surveys
WHO WMH surveys documented cross-national prevalence, severity gradients, and large unmet need for treatment, with mild cases numerous but severe cases still frequently untreated.[5]
3.4 Australia — NSMHWB
The 2007 Australian National Survey of Mental Health and Wellbeing established methods and key national prevalence estimates for policy; later national studies update figures — cite the survey generation you mean.[6] For FRANZCP, know the logic (household survey, CIDI-based, 12-month prevalence, service use) more than every cell of a table.
3.5 Sex, comorbidity, psychotic experiences
- Sex: depressive and anxiety disorders more common in females; substance use and some externalising patterns more common in males (pattern replicated across many surveys).[3][4]
- Comorbidity: the rule, not the exception; multimorbidity drives disability and service intensity.[4][5]
- Psychotic experiences in the general population are far more common than schizophrenia diagnoses — dimensional risk signals, not automatic psychosis care pathways.[21]
3.6 COVID-19 shock
Santomauro and colleagues estimated large additional global burdens of major depressive and anxiety disorders in 2020 attributable to the COVID-19 pandemic — a worked example of population mental health under systemic stress and of GBD-style modelling under uncertainty.[8][24]
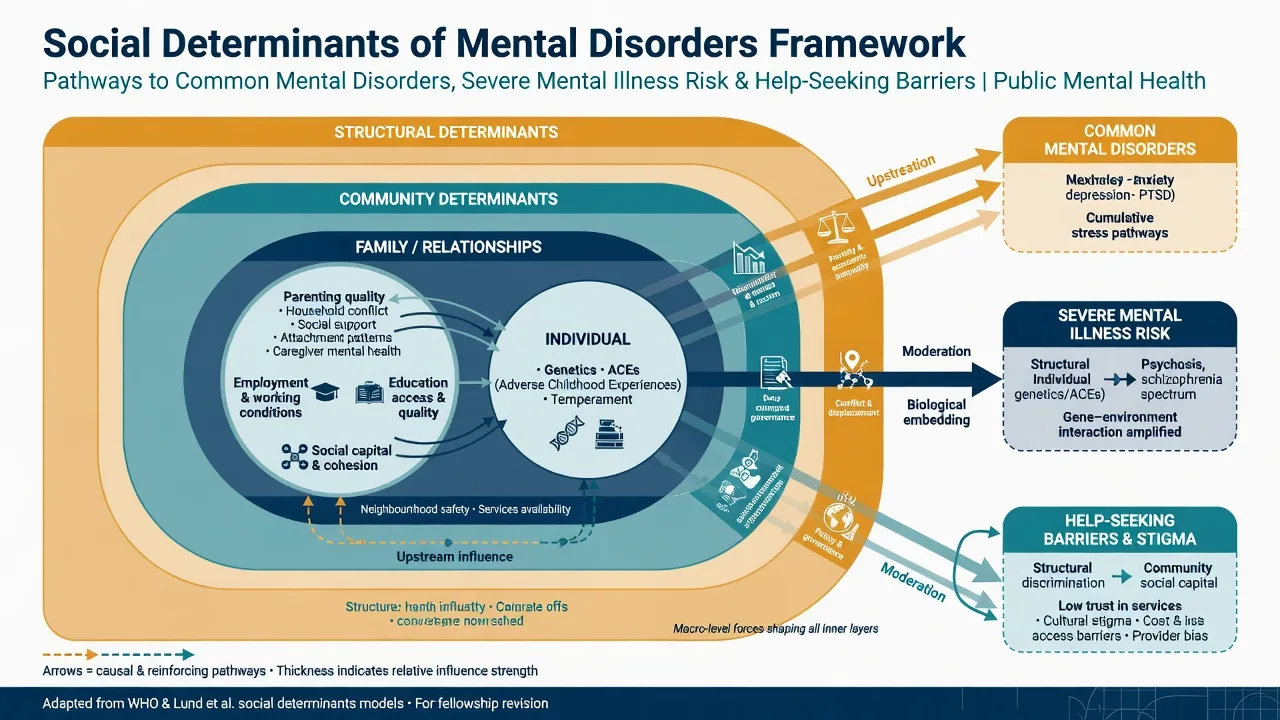
4. Social determinants and life-course risk
Mental disorders track the social gradient. Marmot's determinants framework (income, education, power, environment) applies with force to mental health inequalities.[11] Lund and colleagues mapped social determinants of mental disorders onto the Sustainable Development Goals: poverty, education, housing, food insecurity, violence, discrimination, conflict, and climate-related stressors among others.[10]
Adverse childhood experiences (ACEs) show a graded relationship with adult health risk behaviours and disease outcomes, including mental health pathways — foundational for selective prevention and trauma-informed systems.[12]
Stigma and discrimination operate as population barriers to help-seeking, employment, and recovery; evidence supports multi-level anti-stigma interventions (contact-based approaches often strongest).[19]
5. Prevention science
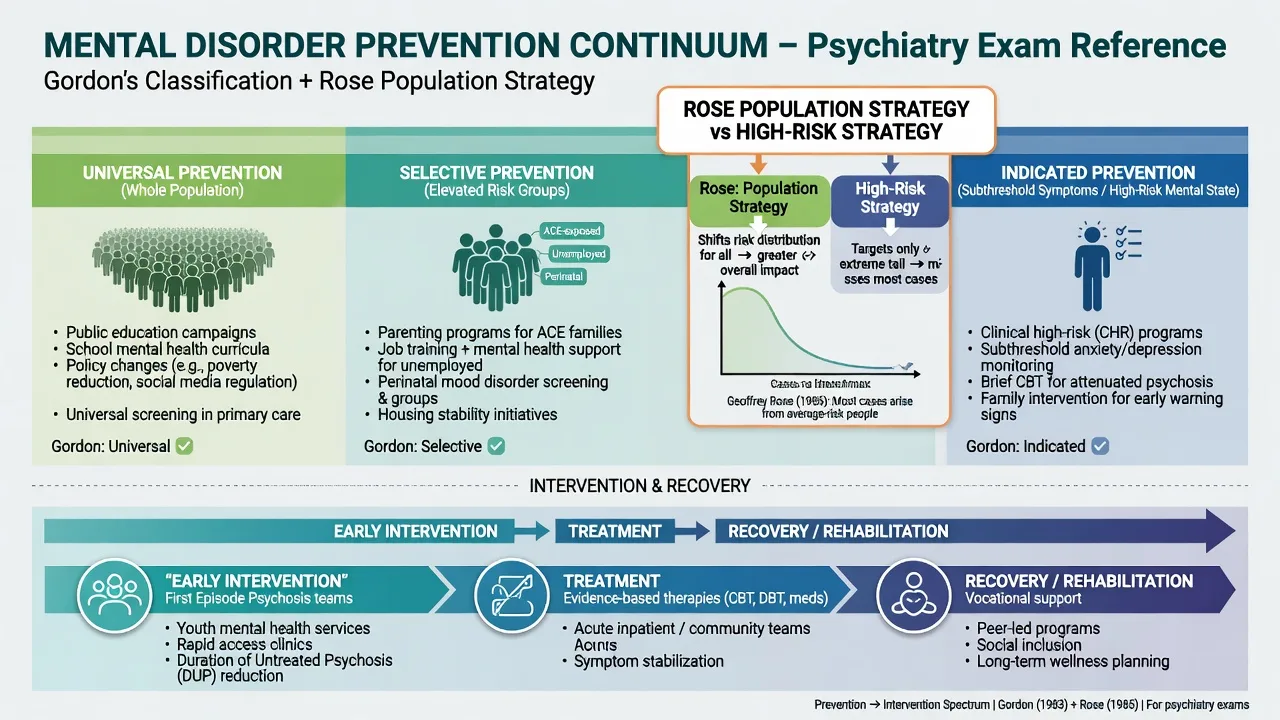
5.1 Gordon classification
Universal prevention targets whole populations regardless of risk; selective targets groups with elevated risk (e.g. ACE-exposed families, unemployed persons, perinatal populations); indicated targets individuals with subthreshold symptoms or high-risk mental states.[14]
5.2 Rose: sick individuals and sick populations
Rose's core insight: when risk is continuously distributed, shifting the population mean (population strategy) can prevent more cases than only treating the high-risk tail — the prevention paradox (many cases arise from average-risk people).[13] High-risk strategies remain essential for efficiency and ethics (e.g. indicated psychosis prevention, perinatal high-risk pathways) but cannot replace structural action.[13][15]
5.3 Preventive psychiatry agenda
Arango and colleagues synthesise prevention across development: risk-factor reduction, early detection of high-risk states, and stage-specific interventions — link to clinical early-intervention services without overclaiming primary prevention of schizophrenia as solved.[15]
6. Treatment gap, resources, and services
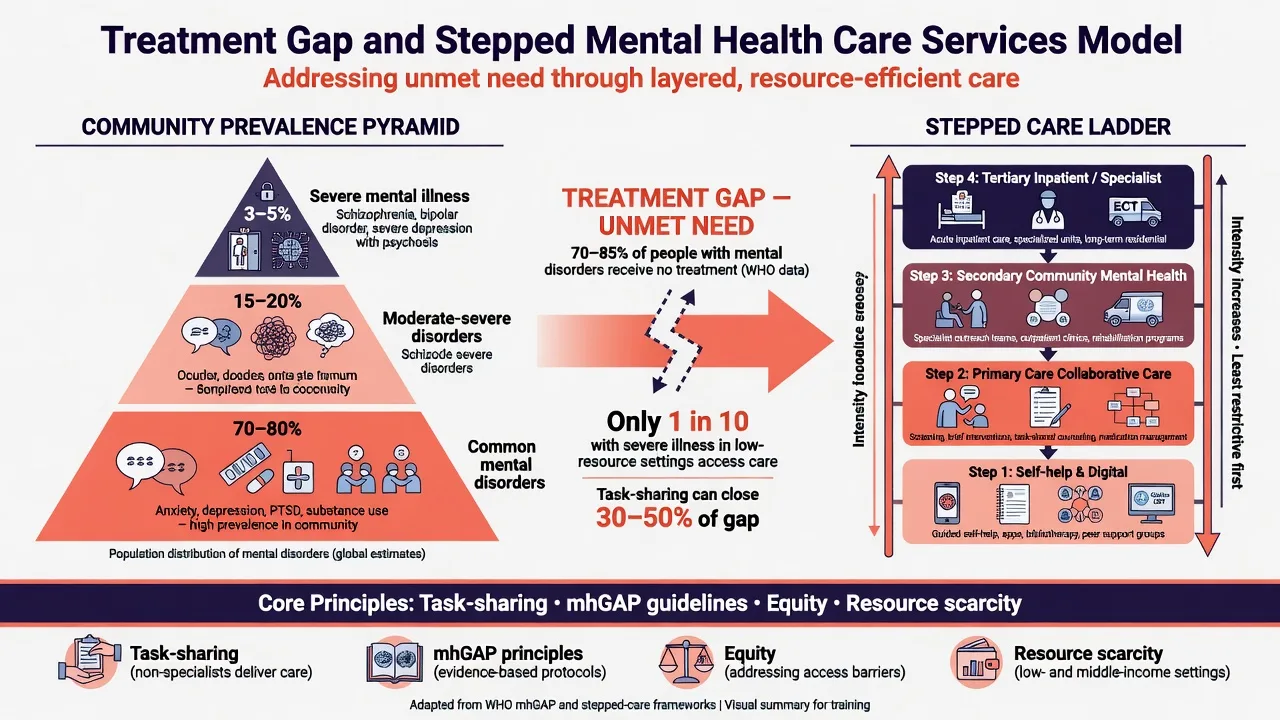
6.1 Treatment gap
Kohn and colleagues formalised the treatment gap: a large fraction of people with mental disorders in many settings receive no treatment; gaps are generally larger in low- and middle-income countries and for milder disorders, yet severe disorders are not fully covered either.[16][5]
6.2 Scarcity, inequity, inefficiency
Saxena and colleagues described mental health resources as scarce, inequitably distributed (between and within countries; hospital vs community), and often inefficiently used — the triad still structures FRANZCP health-systems viva answers.[17]
6.3 Global mental health and SDGs
The Lancet Commission on global mental health and sustainable development reframes mental health as a global public good linked to development goals, rights, and scaled evidence-based care, including task-sharing.[9] Prince and colleagues' earlier maxim — no health without mental health — remains a high-yield opener for essays.[18]
6.4 Stepped care and public mental health implementation
Public mental health action requires implementation, not only evidence catalogues: promotion, prevention, early intervention, treatment coverage, and recovery supports, with explicit attention to COVID-era and other system shocks.[23][24] Stepped care matches intensity to need: self-help/digital and primary care collaborative models for common disorders; specialist community and inpatient care for severe illness and risk.
7. Suicide as a population outcome
Cross-national WMH analyses show ideation, plans, and attempts are not rare; transition probabilities and risk correlates (mental disorders, demographic factors) vary by country.[20] Population prevention levers examiners expect: means restriction, responsible media, crisis and aftercare pathways, alcohol policy, and treatment of mood/substance disorders — distinct from individual risk prediction, which has low positive predictive value at community base rates.[20][23]
8. Critical appraisal of psychiatric epidemiology
Surveys fail in predictable ways: non-representative sampling frames, non-response bias (often sicker or more marginalised non-respondents), diagnostic instrument limits, cultural validity of criteria, recall bias for lifetime estimates, and conflating distress scales with diagnoses.[22]
STROBE provides the reporting backbone for observational designs (cohort, case-control, cross-sectional): design, setting, participants, variables, bias, study size, statistics, and limitations.[22] Link to the critical appraisal topic for RR/OR/NNT and for diagnostic screening PPV collapse in low-prevalence settings.[22]
Clinic ≠ community. Specialist caseloads over-represent comorbidity, severity, and treatment resistance (selection/Berkson-type biases). Service admission rates are not incidence.[5][22]
9. Special populations (exam flashpoints)
- Children and youth: early age-of-onset distribution mandates school-based promotion, youth mental health platforms, and family-level selective prevention.[4][15]
- Perinatal: high public-health yield for mother–infant outcomes; selective screening pathways.[15]
- Older adults: under-detection of depression; multimorbidity; avoid attributing all cognitive change to "ageing."[10]
- Indigenous and minoritised groups: inequities driven by structural determinants, racism, and service mismatch — measure and co-design, do not pathologise culture.[10][11]
- Conflict/refugee populations: elevated trauma-related burden; surveys in conflict settings partly explain global CMD heterogeneity.[3]
- Intellectual disability: dual diagnosis under-ascertained in general surveys.[5]
10. From numbers to action (synthesis for MEQ/viva)
- Define the question — incidence for aetiology/prevention; 12-month prevalence and severity for service need; DALYs for cross-disease priority setting.[1][2]
- Map determinants — proximal clinical risks plus upstream social drivers and ACEs.[10][12]
- Choose prevention mix — universal structural measures + selective programmes + indicated clinical prevention.[13][14][15]
- Close the treatment gap — stepped care, primary care capacity, task-sharing where specialist scarcity exists, anti-stigma, rights-based access.[16][17][19]
- Implement and evaluate — public mental health fails more from implementation gaps than from total absence of interventions.[23]
- Appraise evidence — STROBE for observational work; do not over-extrapolate clinic trials to population coverage.[22]
PUBLIC-MH (public mental health stack)
11. Exam pearls (rapid-fire)
- Lifetime prevalence ≠ current need; use 12-month + severity + disability.[5][6]
- Mental disorders: high disability, mortality often indirect.[1][2][7]
- Treatment gap is global and examinable by name and concept.[16]
- Rose + Gordon together answer almost any prevention station.[13][14]
- COVID papers show population burden can jump under systemic shock.[8]
- Always state absolute risks alongside relative risks.[22]
- Admission rates and prescription volumes are health service statistics, not pure epidemiology.[5][6]
- "No health without mental health" is citable rhetoric with a real paper behind it.[18]
12. Related topics
Use critical appraisal for RR/OR/NNT and bias taxonomy; stigma/recovery/rights for anti-stigma and recovery systems detail; cultural formulation and Indigenous mental health for equity depth; disorder-specific topics for clinical management once population need is established.[9][19][22]
References
- [1]Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010 Lancet, 2013.PMID 23993280
- [2]GBD 2019 Mental Disorders Collaborators Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019 Lancet Psychiatry, 2022.PMID 35026139
- [3]Steel Z, Marnane C, Iranpour C, et al. The global prevalence of common mental disorders: a systematic review and meta-analysis 1980-2013 Int J Epidemiol, 2014.PMID 24648481
- [4]Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication Arch Gen Psychiatry, 2005.PMID 15939837
- [5]Demyttenaere K, Bruffaerts R, Posada-Villa J, et al. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization World Mental Health Surveys JAMA, 2004.PMID 15173149
- [6]Slade T, Johnston A, Oakley Browne MA, et al. 2007 National Survey of Mental Health and Wellbeing: methods and key findings Aust N Z J Psychiatry, 2009.PMID 19530016
- [7]Vigo D, Thornicroft G, Atun R Estimating the true global burden of mental illness Lancet Psychiatry, 2016.PMID 26851330
- [8]Santomauro DF, Mantilla Herrera AM, Shadid J, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic Lancet, 2021.PMID 34634250
- [9]Patel V, Saxena S, Lund C, et al. The Lancet Commission on global mental health and sustainable development Lancet, 2018.PMID 30314863
- [10]Lund C, Brooke-Sumner C, Baingana F, et al. Social determinants of mental disorders and the Sustainable Development Goals: a systematic review of reviews Lancet Psychiatry, 2018.PMID 29580610
- [11]Marmot M Social determinants of health inequalities Lancet, 2005.PMID 15781105
- [12]Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study Am J Prev Med, 1998.PMID 9635069
- [13]Rose G Sick individuals and sick populations Int J Epidemiol, 2001.PMID 11416056
- [14]Gordon RS Jr An operational classification of disease prevention Public Health Rep, 1983.PMID 6856733
- [15]Arango C, Díaz-Caneja CM, McGorry PD, et al. Preventive strategies for mental health Lancet Psychiatry, 2018.PMID 29773478
- [16]Kohn R, Saxena S, Levav I, Saraceno B The treatment gap in mental health care Bull World Health Organ, 2004.PMID 15640922
- [17]Saxena S, Thornicroft G, Knapp M, Whiteford H Resources for mental health: scarcity, inequity, and inefficiency Lancet, 2007.PMID 17804062
- [18]Prince M, Patel V, Saxena S, et al. No health without mental health Lancet, 2007.PMID 17804063
- [19]Thornicroft G, Mehta N, Clement S, et al. Evidence for effective interventions to reduce mental-health-related stigma and discrimination Lancet, 2016.PMID 26410341
- [20]Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts Br J Psychiatry, 2008.PMID 18245022
- [21]McGrath JJ, Saha S, Al-Hamzawi A, et al. Psychotic Experiences in the General Population: A Cross-National Analysis Based on 31,261 Respondents From 18 Countries JAMA Psychiatry, 2015.PMID 26018466
- [22]von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies Lancet, 2007.PMID 18064739
- [23]Campion J, Javed A, Lund C, et al. Public mental health: required actions to address implementation failure in the context of COVID-19 Lancet Psychiatry, 2022.PMID 35065723
- [24]Campion J, Javed A, Sartorius N, Marmot M Addressing the public mental health challenge of COVID-19 Lancet Psychiatry, 2020.PMID 32531299