Psych · Professional — ethics, boundaries and professionalism
Ethics, boundaries and professionalism
Also known as Professional boundaries · Boundary crossings and violations · Dual relationships · Sexual boundary violations · Confidentiality and duty to protect · E-professionalism · Impaired colleague · RANZCP Code of Ethics · Four principles of biomedical ethics
Exam-exhaustive fellowship reference on psychiatric ethics and professionalism — four principles, Gutheil–Gabbard boundary theory, dual relationships (including rural ANZ), sexual boundary violations, confidentiality limits and duty-to-protect principles, social media/e-professionalism, gifts and self-disclosure, impaired colleagues and mandatory reporting principles, and RANZCP Code of Ethics themes. Jurisdiction-specific law stated as principles only. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Overview and definition
Ethics, boundaries, and professionalism are examined continuously across FRANZCP, MRCPsych, ABPN, and MD/DNB pathways because psychiatry concentrates power, intimacy, secrecy, and vulnerability in one relationship. Ethics asks what ought to be done; law sets enforceable minimums; professionalism is the day-to-day enactment of both under College and board codes. Passing the legal minimum is not always enough for good psychiatric care.[9][10][11]
A professional boundary is the edge of appropriate role behaviour that keeps the relationship therapeutic rather than personal, sexual, financial, or otherwise exploitative. The frame includes role, time, place, fee, confidentiality, and non-sexual physical contact rules. Boundaries are not coldness; they make authentic empathy safe.[1][5]
The RANZCP Code of Ethics is a living College document that has been revised to reflect contemporary values of Australian and New Zealand psychiatrists; candidates should know its themes (patient welfare, respect, integrity, confidentiality, collegial responsibility, justice) without treating every clause as universal statute.[9][10][11]
Classification — four principles and the boundary spectrum
Four principles of biomedical ethics
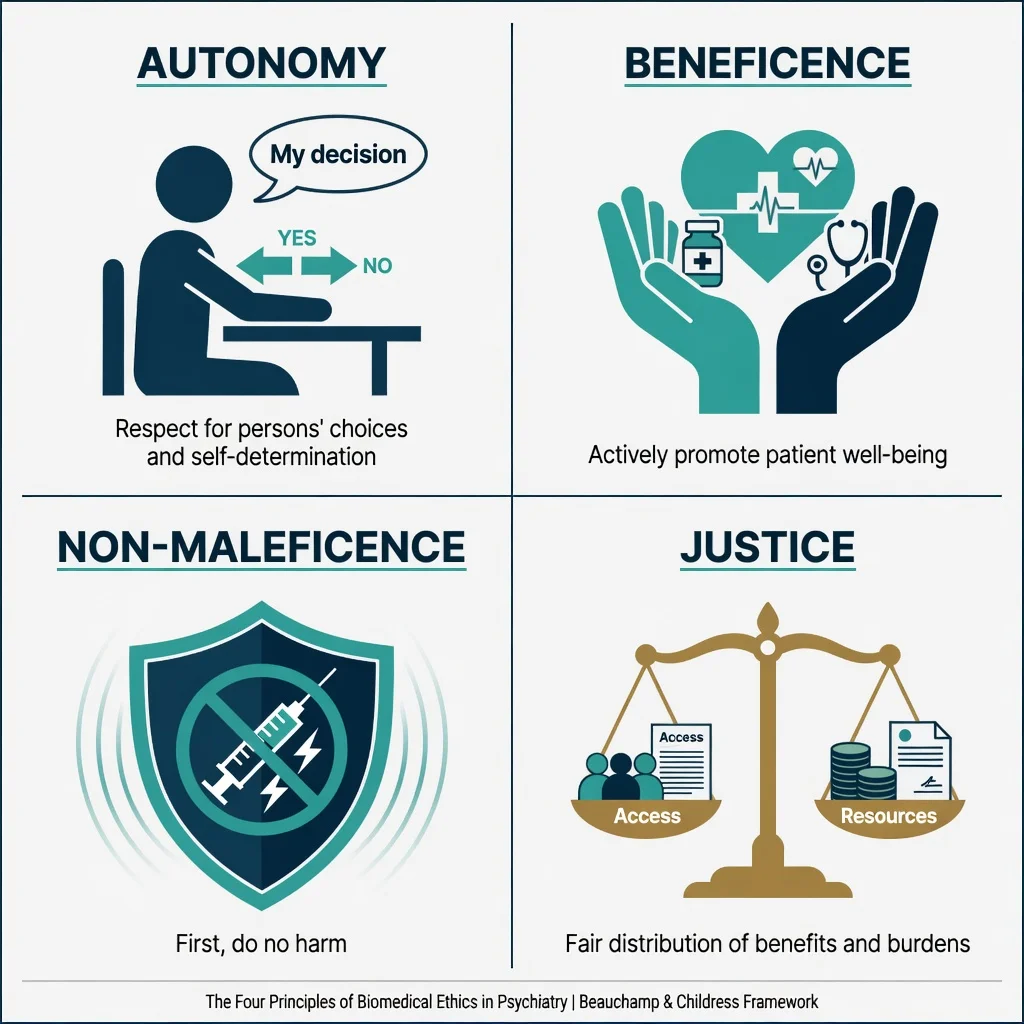
| Principle | Core meaning in psychiatry | Classic tension |
|---|---|---|
| Autonomy | Respect capable choices, informed consent, privacy | Compulsory treatment; risk management |
| Beneficence | Act to promote welfare | Overriding short-term preference for longer-term safety |
| Non-maleficence | Avoid harm (including iatrogenic and boundary harm) | Side-effects, restraint, dual-role harm |
| Justice | Fair access, non-discrimination, resource stewardship | Resource rationing; forensic dual roles |
Principles rarely point one way only. The exam skill is naming the conflict, listing options, choosing the least harmful defensible path, and documenting consultation.[9][11]
Boundary crossings versus violations
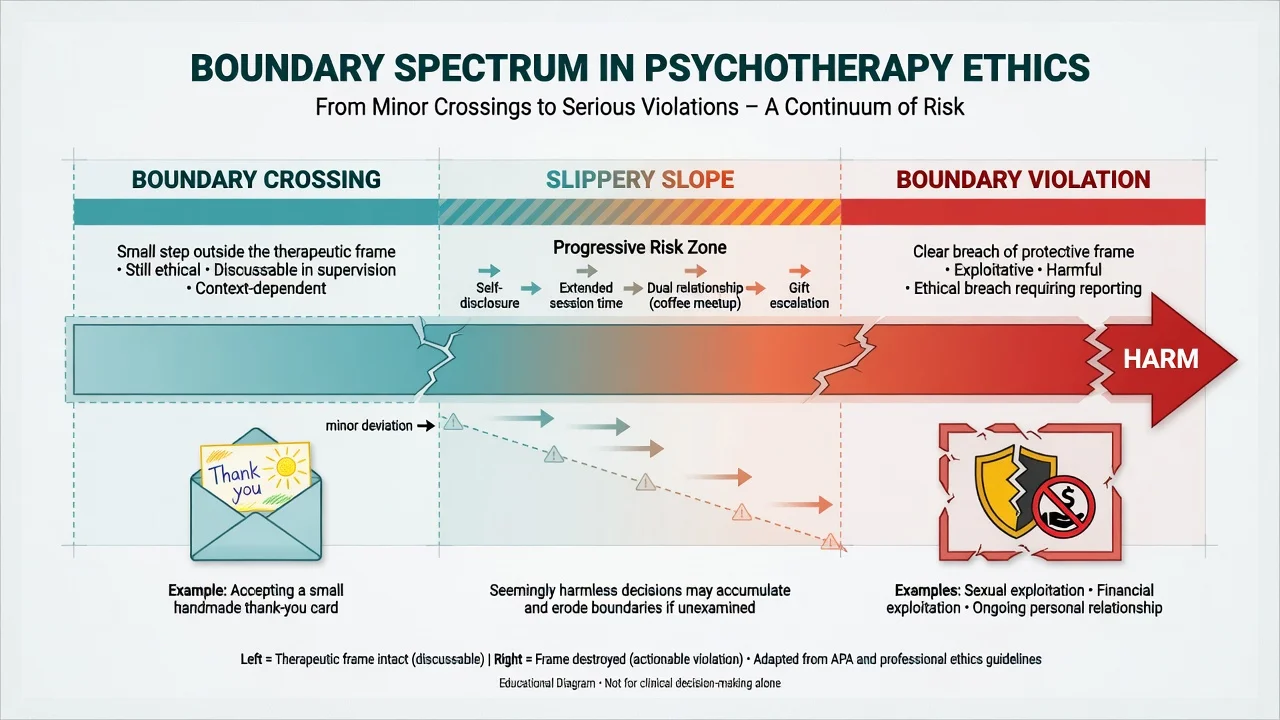
Boundary crossing: a departure from usual practice that is not exploitative and may be harmless or even helpful (e.g. accepting a low-value handmade card; a carefully considered brief self-disclosure; extending a session after acute distress). Crossings should be examinable in supervision, reversible, and oriented to patient need rather than clinician need.[1][2][5]
Boundary violation: a harmful or exploitative breach of the therapeutic frame — sexual contact, financial exploitation, using the patient for the clinician's emotional needs, or a pattern of progressive specialness and secrecy. Sexual misconduct is the prototype serious violation.[1][2][20]
Gutheil and Gabbard also warned that misuse of boundary theory can turn every human gesture into a violation or, conversely, can rationalise misconduct as "flexible technique". Context, exploitability, power, and harm matter — but some acts (sex with current patients) are violations regardless of claimed intent.[2]
- Non-exploitative
- Discussable in supervision
- Often reversible
- Patient-centred rationale
- Document if significant
- Exploitative or harmful
- Often secretive
- Serves clinician needs
- Sexual/financial prototypes
- Report and protect
- Specialness language
- Extended sessions
- After-hours contact
- Personal disclosure shift
- Secrecy from colleagues
Epidemiology and risk contexts
Boundary problems are under-reported. Physician health programme and board series document that boundary violations occur across specialties and career stages; a 19-year PHP review of physician boundary violations underscores that these cases are real, recurrent, and often involve patterns rather than a single impulsive act.[12]
High-risk contexts examiners love include long-term psychotherapy with intense transference; isolation (solo private practice, limited peer contact); clinician personal crisis, loneliness, or substance use; after-hours digital contact without governance; rural and small-community dual roles; work with severe personality pathology without supervision; and hierarchical relationships (supervisor–trainee; senior–junior).[1][6][12][20]
Managing boundaries is also a source of clinician stress; reflective practice and supervision protect both patient and psychiatrist, whereas unexamined boundary strain contributes to burnout risk.[13][15]
Mechanisms — why boundaries exist
Psychiatry concentrates asymmetric power: the patient discloses secrets, depends on the clinician for care, and often idealises or fears the clinician. Transference and countertransference make the relationship emotionally charged. Boundaries protect against exploitation of that asymmetry and preserve the conditions under which psychological treatment can work.[1][20]
The classic slippery-slope pathway moves from small, self-serving deviations (extra time "only for this special patient", personal texting, meeting outside the clinic) to progressive role collapse and sexual or financial exploitation. Secrecy is the accelerant: what cannot be discussed in supervision is already ethically dangerous.[1][5][20]
Dual roles create role conflict — judgment is compromised when the clinician is simultaneously friend, employer, business partner, or lover. Even well-intentioned dual roles can damage trust and therapeutic neutrality.[6][7]
Clinical presentations (exam stems)
Expect stems such as a patient offering an expensive gift or dinner invitation; a social-media friend request or late-night personal texts; rural dual roles with a neighbour; disclosure of attraction or erotic countertransference; a former patient seeking romance; an intoxicated colleague or a trainee reporting a supervisor's sexualised comments; a credible threat to an identifiable person; or a media request about a currently admitted high-profile patient.[1][5][6][14][16]
Early warning signs of boundary erosion in the dyad: language of "specialness", session overruns that become the norm, avoidance of notes, personal rather than professional self-disclosure, meetings outside clinical settings, secrecy from colleagues, and feeling "only I understand this patient".[1][5][20]
Differential and discriminators
| Dilemma pair | Discriminator |
|---|---|
| Crossing vs violation | Exploitability, harm, secrecy, who benefits, reversibility |
| Warmth vs over-disclosure | Is disclosure for the patient's therapy or the clinician's needs? |
| Unavoidable rural dual role vs chosen dual role | Alternatives available? Documented? Sexual/financial absolute bans still apply |
| Confidentiality vs duty to protect | Identifiable victim, serious imminent harm, local legal duty |
| Cultural gift vs unethical gift | Value, expectation of favour, ability to refuse gracefully, documentation |
| Collegial support vs mandatory report | Patient safety threshold and local reporting law |
Assessment — ethical analysis framework
There is no blood test for ethics. "Investigate" means gather facts, policies, and consultation.[5][9]
ETHICS
For dual-relationship risk specifically, assess power differential, duration of both relationships, risk of exploitation or compromised judgment, alternatives (refer out), transparency, and whether sexual or financial interests are involved (automatic no).[5][6][7]
Dual relationships
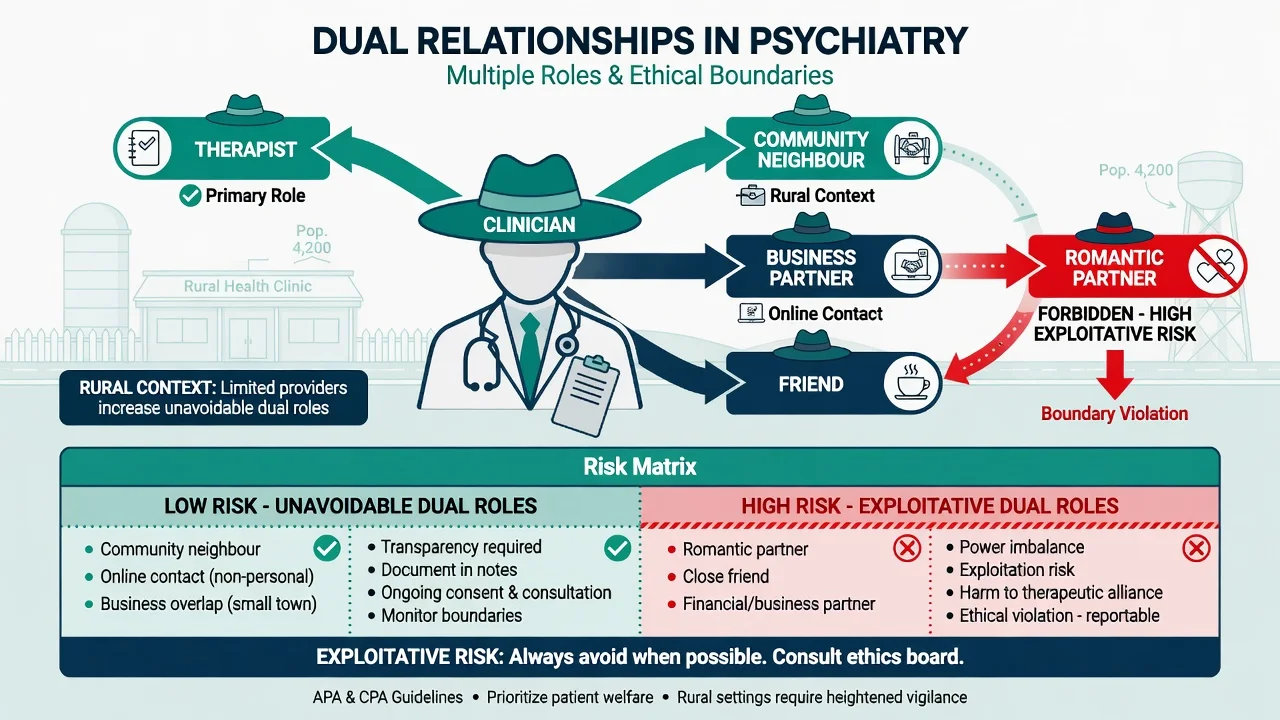
A dual (multiple) relationship exists when the clinician has a second significant relationship with the patient (or their close family) outside the professional role — social, business, supervisory, online, or romantic.[6][7]
ANZ evidence is directly exam-relevant: rural mental-health clinicians face frequent unavoidable dual relationships; metropolitan practice is not immune. Impact includes compromised confidentiality, role confusion, and pressure to treat beyond competence. Management strategies include acknowledging the dual role early, setting explicit limits, documenting, seeking supervision, and referring when feasible.[6][7]
Sexual dual relationships with current patients are forbidden. Business dual relationships (hiring a patient, investing together) are almost always unethical because of power and exploitation risk. Sequential relationships (former patient becomes friend/partner) remain high-risk; many codes treat post-termination sexual relationships as prohibited or as serious misconduct for prolonged periods — know your local code language rather than inventing a universal "two-year rule" as law.[3][6]
Sexual boundary violations
Sexual contact with a current patient is always a boundary violation and professional misconduct. It is never justified by claimed mutual consent: power asymmetry voids the moral force of "consent" in this context. Trainees and supervisees are similarly protected from sexualised hierarchical relationships.[1][19][20]
Post-termination sexual boundary violations remain ethically and clinically high-risk because of residual dependency and power; Gabbard's analysis of post-termination sexual boundary violations is a classic viva anchor.[3][4]
Immediate response algorithm (when alleged or discovered)
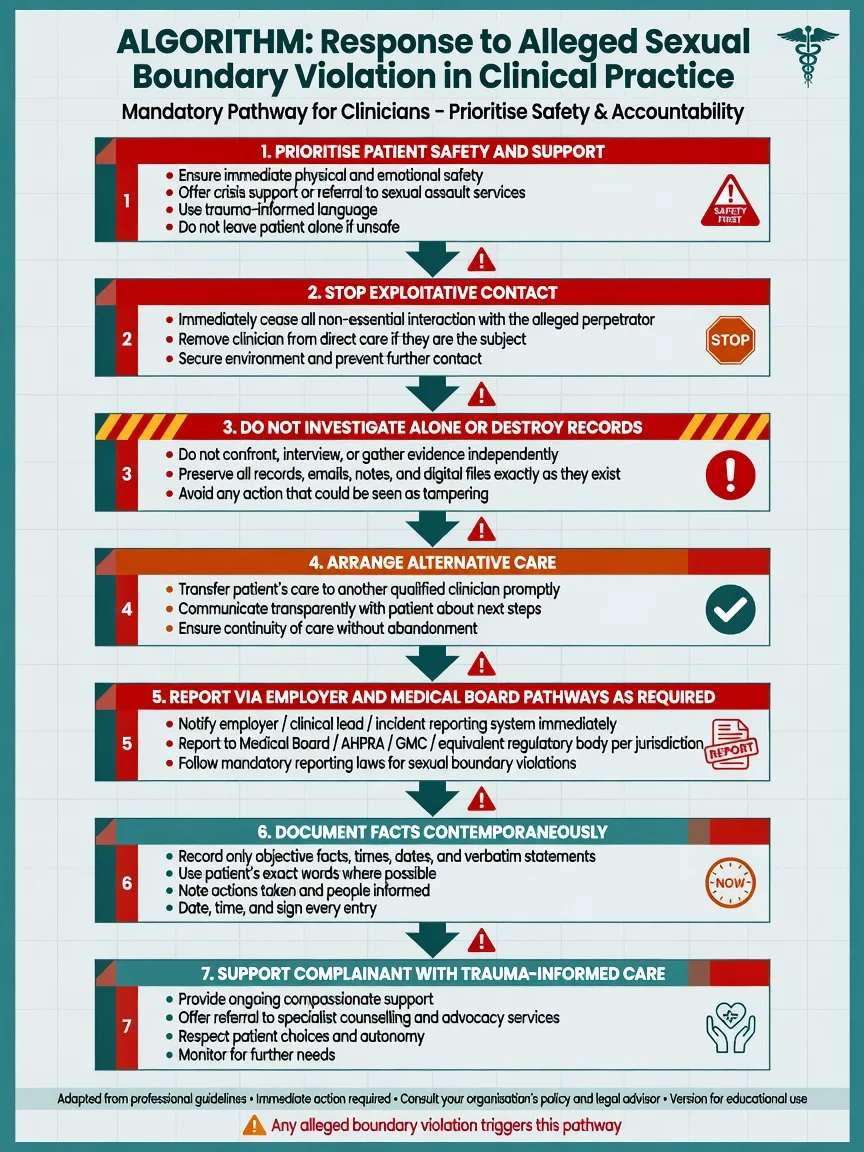
Immediate steps: prioritise the patient's physical and psychological safety; stop the exploitative relationship and remove the alleged clinician from that patient's care; do not investigate alone, confront secretly, or destroy records; arrange alternative care promptly; report via employer incident systems and medical board / regulator pathways as required by local law and policy; document objective facts contemporaneously; and offer trauma-informed support and advocacy while protecting the complainant from retaliation.[19][20]
Never blame the patient ("seductive patient" myth). The ethical duty sits with the professional.[19][20]
Confidentiality and its limits
Confidentiality is a cornerstone of psychiatric care and underpins autonomy and trust. It is not absolute. Classic limits (exact duties are jurisdiction-specific) are summarised below.[16]
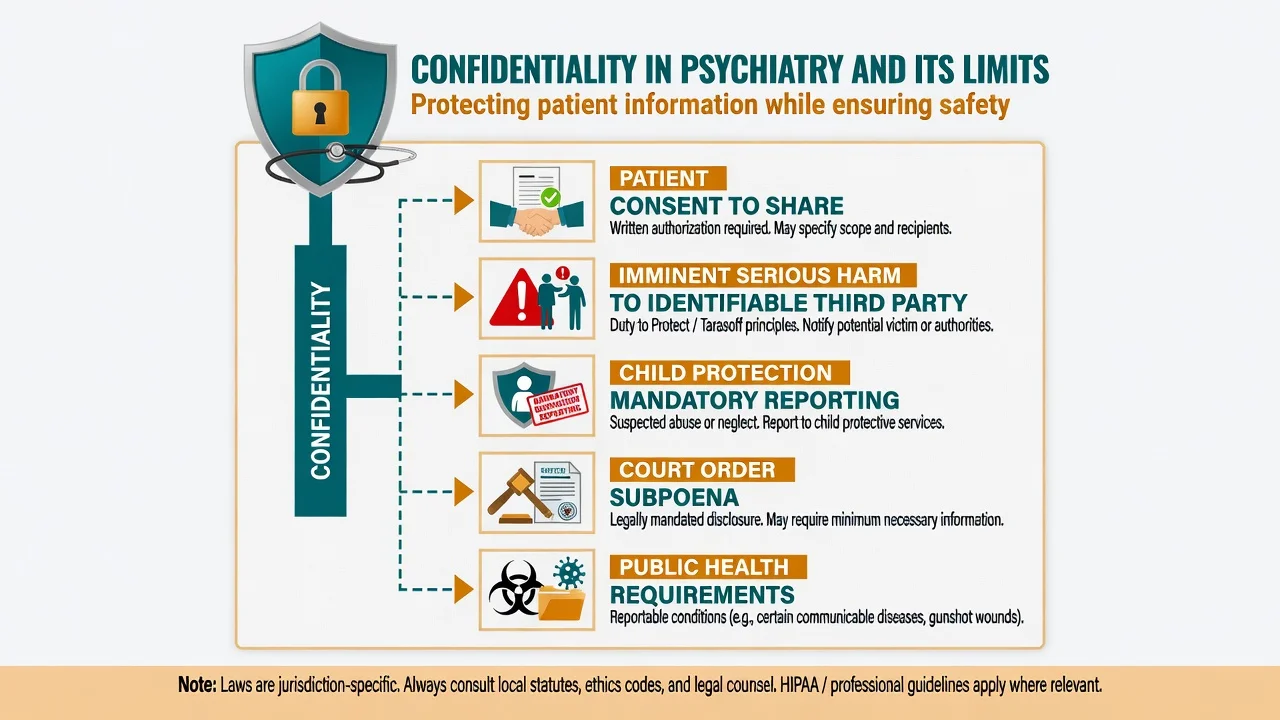
| Situation | Principle-level action |
|---|---|
| Patient consents to share | Disclose within agreed scope; document |
| Imminent serious harm to identifiable third party | Duty-to-protect / warn principles (Tarasoff lineage in US literature; local equivalents vary) |
| Child abuse / neglect suspicion | Mandatory reporting under local child-protection law |
| Court order / lawful subpoena | Disclose as legally required; seek advice on scope |
| Public health notifiable issues | Follow local public-health reporting rules |
| Risk of serious harm to the patient (e.g. suicide) | Safety planning; may share need-to-know with carers under local rules |
The Tarasoff lineage concerns a clinician's duty when a patient poses a serious threat of violence to an identifiable victim; subsequent case law and statutes have narrowed, broadened, or redefined duties differently across jurisdictions. In exams: assess imminence and identifiability, take protective steps available under local law (warn victim and/or police as appropriate), document, and consult seniors/legal — do not claim a single universal statute.[16]
Social media and e-professionalism
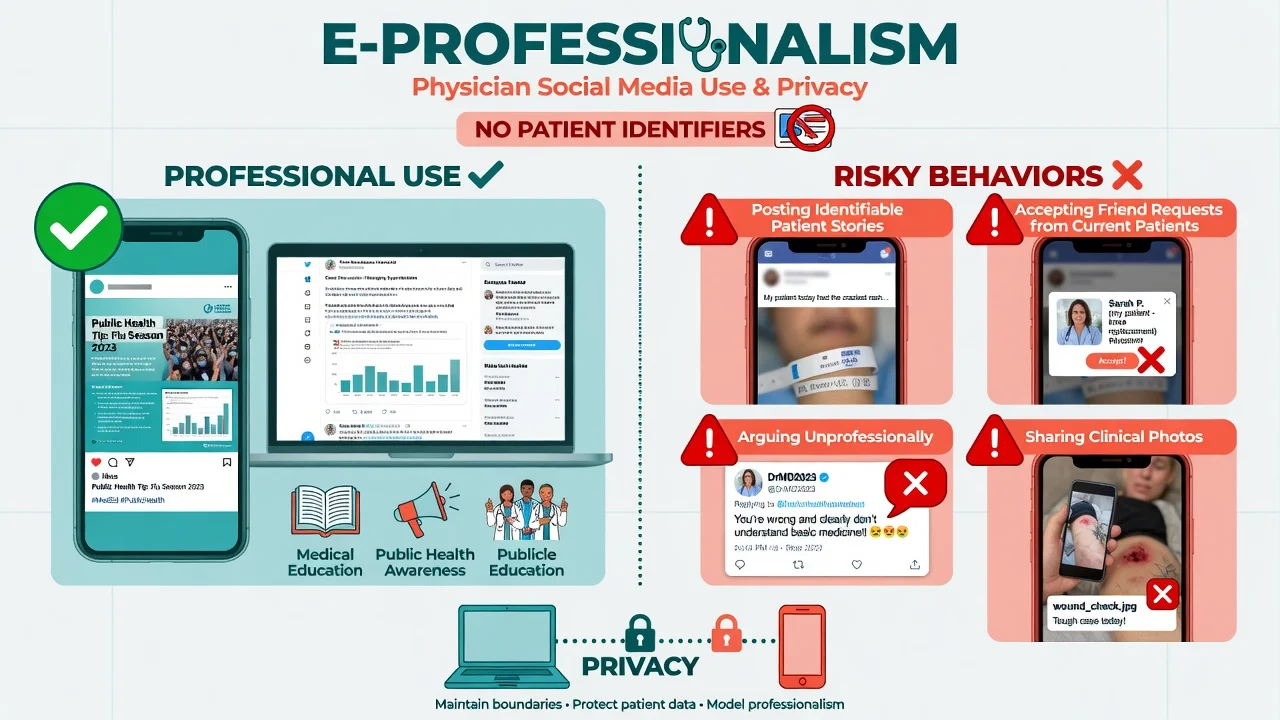
Scoping evidence on health-care professionals' social media use highlights both benefits (education, public health communication) and dangers (privacy breaches, boundary collapse, reputational harm, blurred personal–professional identities).[14]
Practical rules for candidates: never post patient-identifiable information (including "anonymised" stories that re-identify); decline friend/follow requests from current patients and discuss the boundary in session if clinically relevant; assume anything posted can be screenshotted and subpoenaed; separate personal and professional online presence where feasible; keep clinical messaging in governed systems rather than private ungoverned chats; and model professionalism, avoiding public arguments or denigration of patients or colleagues.[14][15]
Gifts, self-disclosure, and everyday frame issues
Gifts. Small token gifts of low value may be acceptable crossings if refusal would harm the alliance and acceptance creates no obligation; high-value gifts, cash, or gifts that create indebtedness should be declined with a kind explanation and documentation. Cultural gift practices require curiosity without automatic acceptance of exploitative value.[1][5][15]
Self-disclosure. Therapist self-disclosure is not forbidden, but it is a clinical intervention with risks. Qualitative and clinical reviews show mixed effects; ethical use is brief, patient-centred, non-sexual, non-burdensome, and processed in supervision when significant. Disclosure that seeks comfort for the clinician is a warning sign.[17][18]
Time, place, fee, touch. Keep appointments professional; avoid social venues for therapy; maintain transparent fees; limit physical contact to culturally appropriate handshakes or clinically necessary examination with consent. The "transition zone" between the chair and the door is a classic site of informal boundary slips.[1][5]
Impaired and unethical colleagues
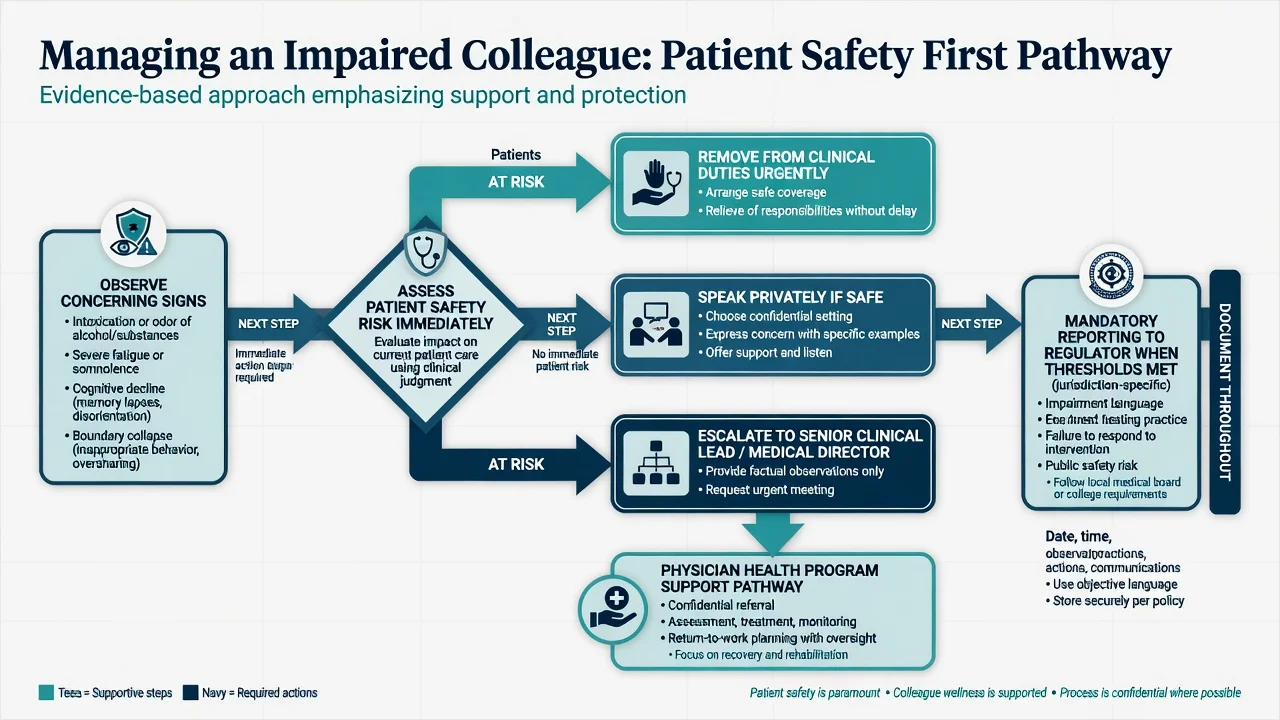
Impairment includes substance use, severe untreated mental illness, cognitive decline, and extreme fatigue or illness that compromises safe practice. Professionalism requires action when patient safety is at risk. Loyalty, fear of career damage, and uncertainty about thresholds are common barriers; Australian qualitative work on mandatory reporting of impaired practitioners highlights the moral and practical tension for treating clinicians.[8]
Principle-level pathway: protect patients first and remove from clinical duties if immediate risk; if safe, speak privately with specific observations; escalate to clinical lead or medical director; offer physician-health support pathways; report to the regulator when local mandatory-reporting thresholds are met; and document facts objectively.[8][9]
Do not invent AHPRA section numbers in exams; state "under local mandatory reporting and medical board requirements". Threshold language commonly turns on risk of harm to the public and whether the practitioner is not managing the risk — check current local guidance in practice.[8][9]
Management — prevention and definitive practice
Prevention (the real "definitive treatment")
Prevention means maintaining a clear frame (role, time, place, fee, confidentiality); using regular supervision and peer review — especially for long-term psychotherapy; attending to self-care and treating personal crises before they leak into the dyad; avoiding dual relationships when alternatives exist; using governed communication channels; knowing College codes and employer policies; and seeking early consultation when specialness, secrecy, or attraction appears.[5][9][13]
Response ladder for emerging boundary concern
| Stage | Action |
|---|---|
| Mild concern / single crossing | Reflect; document rationale; discuss in supervision |
| Pattern emerging | Modify practice; tighten frame; consider transfer of care |
| Exploitation risk or sexualised content | Stop; transfer care; senior consultation; report as required |
| Alleged misconduct by other | Safety; formal pathways; no solo investigation |
Special populations and scenarios
Rural and remote ANZ. Dual relationships are often unavoidable. Minimise scope, document, maintain sexual and financial red lines, and use telehealth referral networks when dual-role risk is high.[6][7]
Child and adolescent. Boundaries extend to parents, schools, and social media; clarity about who the patient is and what will be shared is essential.[1][5]
Forensic interface. Separate treater and expert-witness roles when possible; dual agency must be disclosed.[1][9]
Cultural and Indigenous contexts. Kinship, gift, and community roles may create dual relationships; non-exploitation, transparency, and cultural supervision are required — not rigid urban private-practice rules applied without reflection.[6][11]
Trainees. Supervisors hold hierarchical power; sexual or romantic relationships with current trainees are misconduct. Trainees should have safe reporting pathways.[19]
Personality disorder work. Intense attachment and idealisation increase crossing pressure; a firmer frame is protective, not punitive.[1][13]
Complications and pitfalls
Classic pitfalls include rationalising progressive crossings as "special technique"; blaming the patient for clinician sexual misconduct; confusing legal minimums with ethical ideals; over-sharing on social media or using ungoverned messaging; failing to report an impaired colleague out of loyalty; treating Tarasoff as universal statute outside its jurisdictional context; accepting sexual contact after engineered "termination for sex"; ignoring cultural gift practices without analysis of power and expectation; and destroying records or silencing complainants after an allegation.[2][3][8][14][19]
Prognosis, professional consequences, and disposition
Consequences of serious boundary violations include medical-board sanctions, conditions on practice, suspension or deregistration, civil liability, criminal charges for sexual assault, and lasting reputational harm. Patients may experience betrayal trauma, deterioration, and avoidance of future care — arrange trauma-informed alternative treatment.[12][19][20]
Some non-sexual boundary and impairment issues can be rehabilitated through physician health programmes with monitoring; sexual misconduct is frequently career-ending and should be treated as such in risk planning.[12]
Disposition of care after a boundary crisis: transfer to another clinician, avoid ongoing dual roles, document handover factually, and protect the patient's access to care without abandonment.[12][19][20]
Evidence, guidelines, and regional differences
Landmark anchors: Gutheil and Gabbard boundary theory (1993, 1998); Gabbard on post-termination sexual boundary violations; Norris/Gutheil on "this couldn't happen to me"; Pope and Keith-Spiegel practical boundary decision-making; ANZ dual-relationship studies (Scopelliti; Endacott); Brooks PHP series; Bismark mandatory reporting qualitative study; social-media e-professionalism scoping review; RANZCP Code revision and anniversary literature; Robertson values study.[1][2][3][6][8][9][12][14]
Exam pearls
References
- [1]Gutheil TG, Gabbard GO The concept of boundaries in clinical practice: theoretical and risk-management dimensions Am J Psychiatry, 1993.PMID 8422069
- [2]Gutheil TG, Gabbard GO Misuses and misunderstandings of boundary theory in clinical and regulatory settings Am J Psychiatry, 1998.PMID 9501754
- [3]Gabbard GO Post-termination sexual boundary violations Psychiatr Clin North Am, 2002.PMID 12232973
- [4]Celenza A, Gabbard GO Analysts who commit sexual boundary violations: a lost cause? J Am Psychoanal Assoc, 2003.PMID 12866759
- [5]Pope KS, Keith-Spiegel P A practical approach to boundaries in psychotherapy: making decisions, bypassing blunders, and mending fences J Clin Psychol, 2008.PMID 18386835
- [6]Scopelliti J, Judd F, Grigg M, et al. Dual relationships in mental health practice: issues for clinicians in rural settings Aust N Z J Psychiatry, 2004.PMID 15555031
- [7]Endacott R, Wood A, Judd F, et al. Impact and management of dual relationships in metropolitan, regional and rural mental health practice Aust N Z J Psychiatry, 2006.PMID 17054567
- [8]Bismark MM, Mathews B, Morris JM, et al. Views on mandatory reporting of impaired health practitioners by their treating practitioners: a qualitative study from Australia BMJ Open, 2016.PMID 27993902
- [9]Bloch S, Kenn F, Smith G Revising the Royal Australian and New Zealand College of Psychiatrists code of ethics Australas Psychiatry, 2018.PMID 30058364
- [10]Lim I, Kenn F, Bloch S The 30th anniversary of the code of ethics of the Royal Australian and New Zealand College of Psychiatrists-a worthy milestone Australas Psychiatry, 2022.PMID 35077253
- [11]Robertson M, Kerridge I, Walter G Ethnomethodological study of the values of Australian psychiatrists: towards an empirically derived RANZCP Code of Ethics Aust N Z J Psychiatry, 2009.PMID 19373701
- [12]Brooks E, Gendel MH, Early SR, et al. Physician boundary violations in a physician's health program: a 19-year review J Am Acad Psychiatry Law, 2012.PMID 22396343
- [13]Lampe L, Hitching R, Hammond TE, et al. Being a 'good' doctor: Understanding and managing professional boundaries is challenging and can lead to stress and burnout Australas Psychiatry, 2023.PMID 37563780
- [14]Vukušić Rukavina T, Viskić J, Machala Poplašen L, et al. Dangers and Benefits of Social Media on E-Professionalism of Health Care Professionals: Scoping Review J Med Internet Res, 2021.PMID 34662284
- [15]Reyes Nieva H, Ruan E, Schiff GD Professional-Patient Boundaries: a National Survey of Primary Care Physicians' Attitudes and Practices J Gen Intern Med, 2020.PMID 31755012
- [16]Walcott DM, Cerundolo P, Beck JC Current analysis of the Tarasoff duty: an evolution towards the limitation of the duty to protect Behav Sci Law, 2001.PMID 11443695
- [17]Henretty JR, Levitt HM The role of therapist self-disclosure in psychotherapy: a qualitative review Clin Psychol Rev, 2010.PMID 19837497
- [18]Barnett JE Psychotherapist self-disclosure: ethical and clinical considerations Psychotherapy (Chic), 2011.PMID 22141415
- [19]Gulrajani C A Duty to Protect Our Patients from Physician Sexual Misconduct J Am Acad Psychiatry Law, 2020.PMID 32393516
- [20]Norris DM, Gutheil TG, Strasburger LH This couldn't happen to me: boundary problems and sexual misconduct in the psychotherapy relationship Psychiatr Serv, 2003.PMID 12663839