Psych · Professional — psychosocial interventions
Family and systemic interventions
Also known as Family therapy · Systemic therapy · Family psychoeducation · Expressed emotion · Multifamily groups · Behavioural family therapy · Family-focused therapy · Structural family therapy
Exam-exhaustive fellowship reference on family and systemic interventions — expressed emotion and psychosis relapse, structural and systemic models, behavioural family therapy, multifamily psychoeducation groups, FFT, ABFT, FBT, MST, engagement without blame, and CASC technique. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Definition and scope
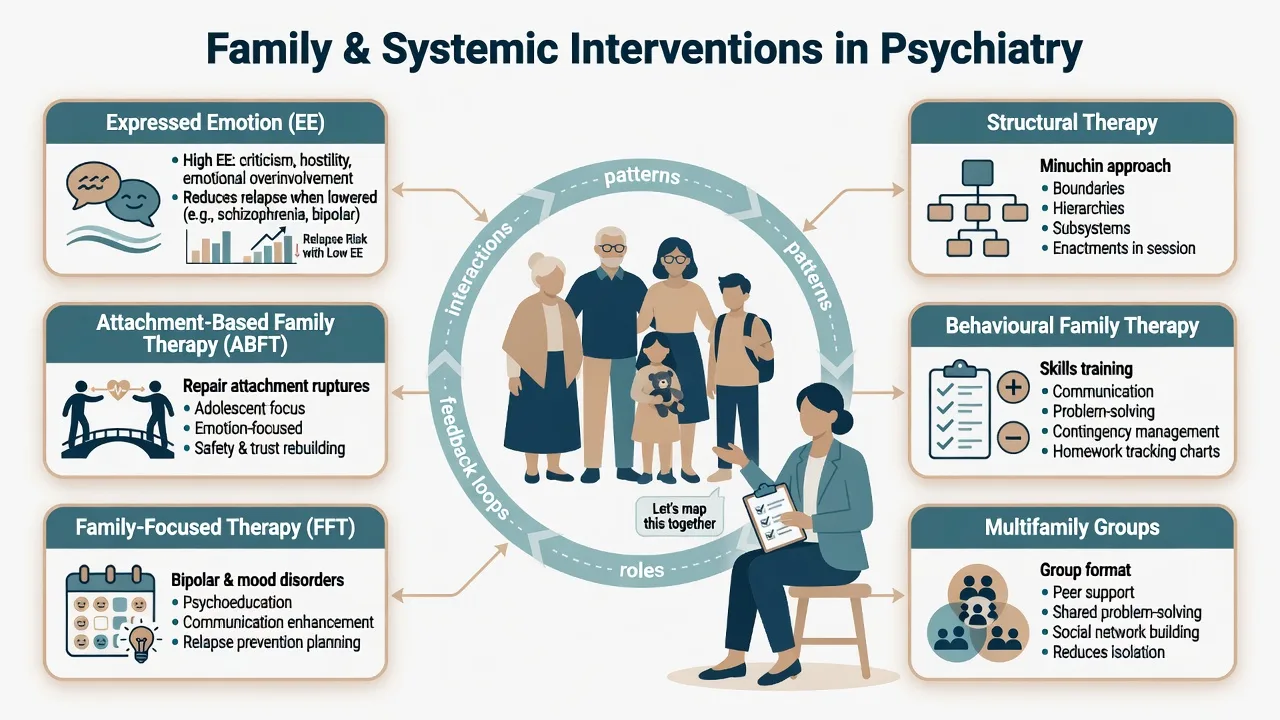
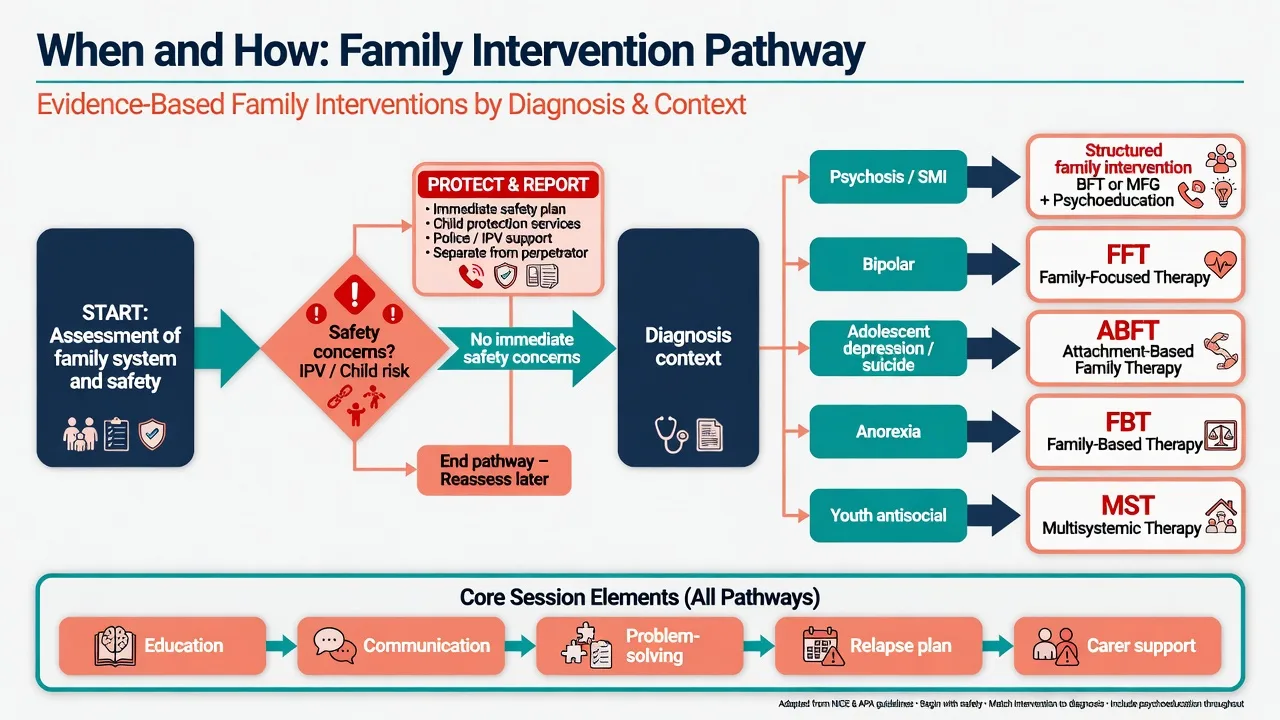
Family intervention is any structured clinical work that engages relatives or significant others to improve outcomes for a person with mental illness and/or for the family system itself. It spans:
[12] [13]- Family psychoeducation — illness education, early warning signs, treatment alliance, carer coping.[13][22]
- Behavioural / skills-based family therapy (BFT) — communication training and structured problem-solving (Falloon lineage).[9][10]
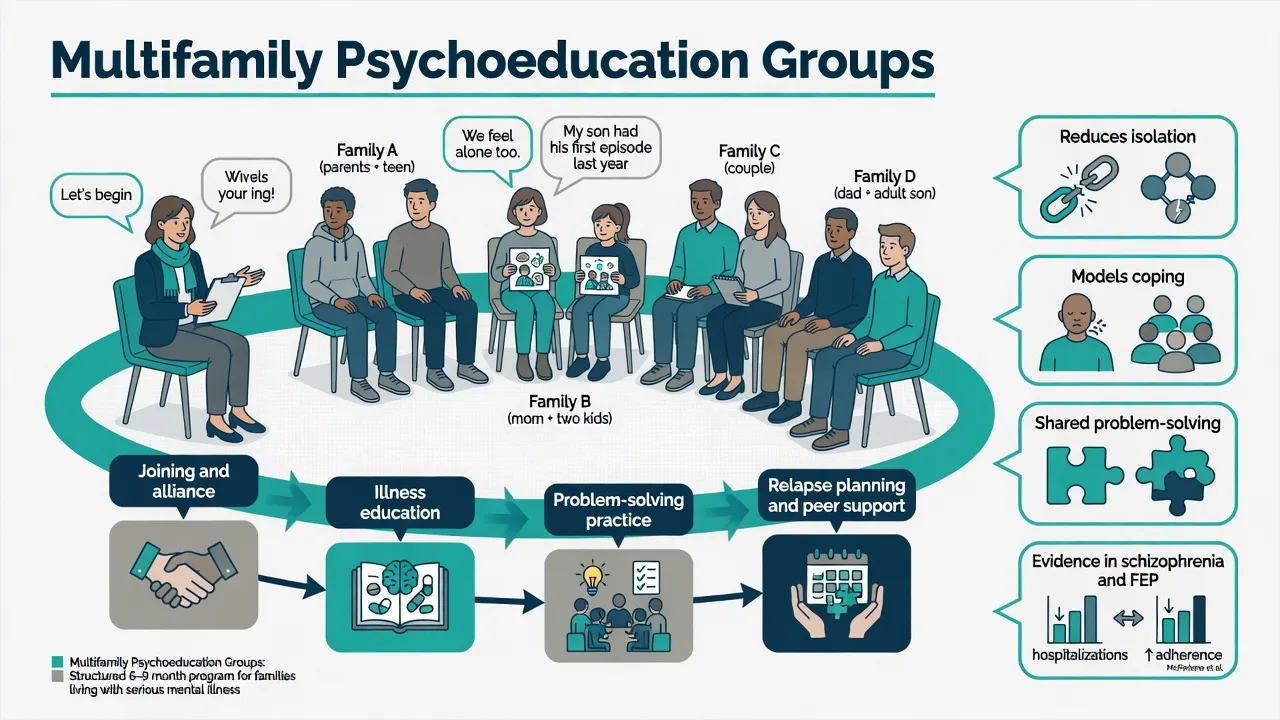
- Multifamily groups (MFG) — several families together with a facilitator (McFarlane lineage).[12][14]
- Systemic / structural therapies — pattern, boundary, hierarchy, and meaning-focused work.[19][20]
- Diagnosis-specific packages — FFT, ABFT, FBT, MST.[15][17][18]
Systemic stance: symptoms and interactions co-evolve (circular causality); the unit of observation may be the network, not only the identified patient. Structural stance (Minuchin lineage): focus on boundaries, subsystems, hierarchy, alliances/coalitions, and enactments in session.[19][20]
Exam distinction. Diagnosis classifies the person's syndrome. Family work asks: what patterns maintain distress or protect recovery, and what can this network learn and change? Family work is usually adjunct to indicated individual treatment (including medication for SMI), not a substitute.[5][12]
Classification of models (viva map)
| Model | Core ideas | High-yield indications |
|---|---|---|
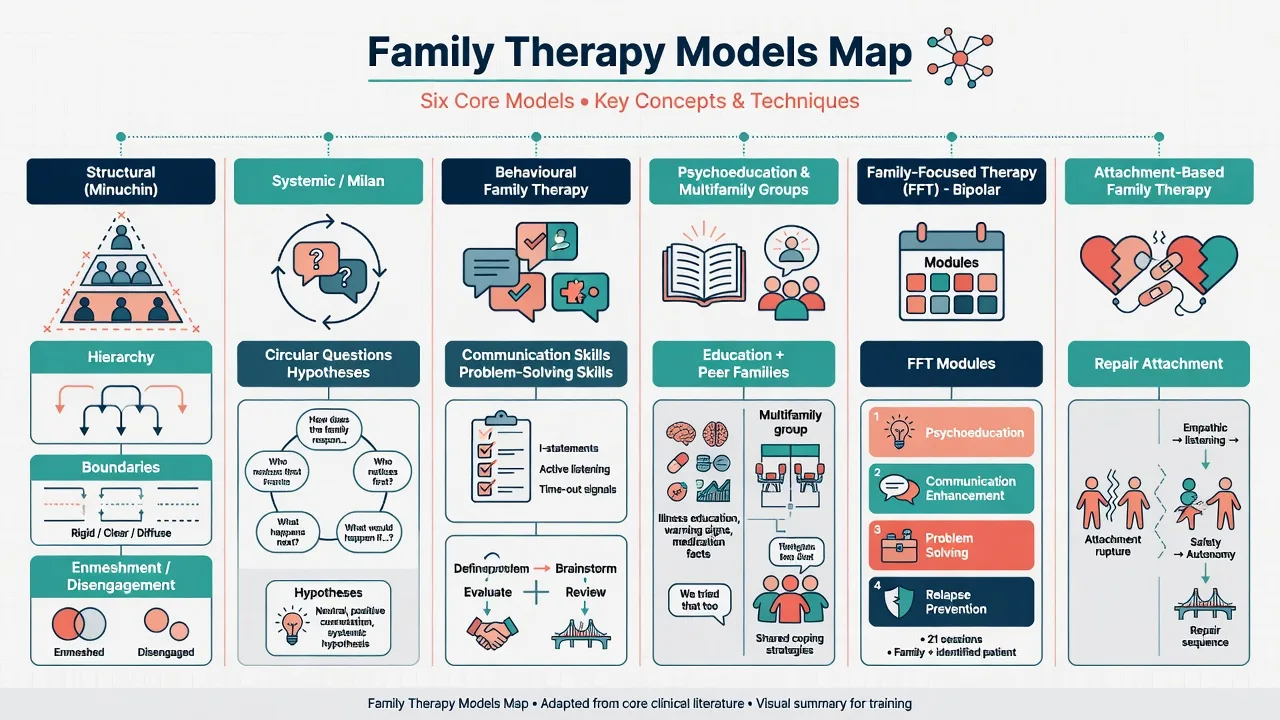
| Structural | Hierarchy, boundaries, enmeshment/disengagement, triangulation, enactment | Eating disorders historically; hierarchical/boundary problems |
| Systemic / Milan-influenced | Circular questions, neutrality, hypothesising, circular causality | Relational stuckness; meaning systems; adult and child meta-analyses support systemic approaches across disorders |
| Behavioural family therapy | Assessment, education, communication skills, problem-solving | Schizophrenia / SMI community care |
| Family psychoeducation / MFG | Illness education, peer families, problem-solving | Psychosis, FEP, severe mental illness |
| FFT (Miklowitz) | Education, communication enhancement, problem-solving with pharmacotherapy | Bipolar disorder (and related youth mood packages) |
| ABFT (Diamond) | Relational reframe, alliance building, attachment tasks, autonomy | Adolescent depression and suicidal ideation |
| FBT / Maudsley (Lock–Le Grange) | Parent-led refeeding → return control → adolescent issues | Adolescent anorexia nervosa |
| MST (Henggeler) | Ecological multi-system intensive home-based work | Serious youth antisocial / offending pathways |
Expressed emotion (EE) — examiner core
Definition
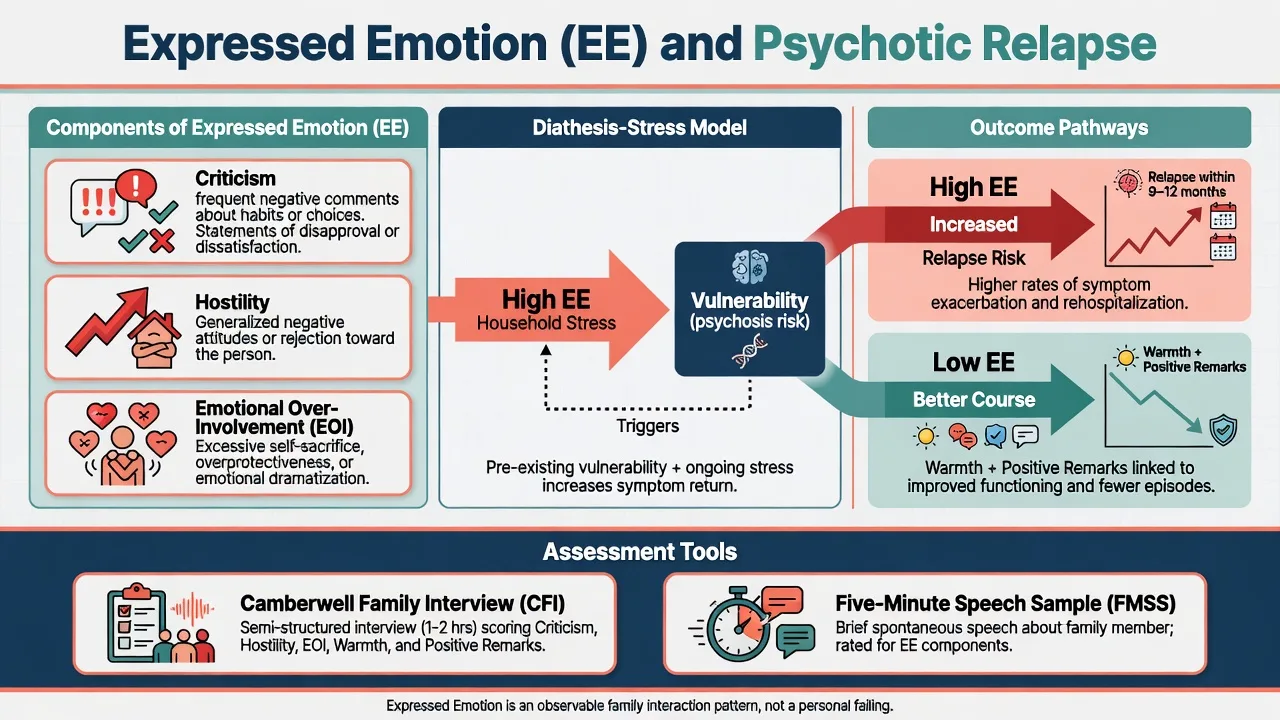
Expressed emotion is a research construct describing relatives' affective attitudes toward the person with illness, classically scored from the Camberwell Family Interview (CFI):
[2] [3]- Criticism — negative comments about behaviour or personality.[2][3]
- Hostility — global rejection or denigration of the person.[2][3]
- Emotional over-involvement (EOI) — excessive self-sacrifice, overprotection, or dramatic emotional response.[2][3]
- Also scored: warmth and positive remarks (protective valence).[2][3]
A briefer proxy is the Five-Minute Speech Sample (FMSS). Clinic proxies (not equivalent to CFI): tone of blame, global rejection, enmeshed rescue behaviours, vs collaborative problem-solving.[1][3]
Why it matters
Seminal work linked family affective climate to course of schizophrenia (Brown, Birley, Wing; Vaughn and Leff).[2][3] Aggregate and meta-analytic evidence shows high EE predicts relapse; Butzlaff and Hooley's meta-analysis is the classic viva citation for EE–relapse association across psychiatric conditions, strongest for schizophrenia.[1][4]
Critical exam sentence: High EE is a stressor interacting with vulnerability, not proof that families cause schizophrenia. Historical "schizophrenogenic mother" models are obsolete and harmful.[1][21]
Caregiving model
Kuipers and colleagues' cognitive model of caregiving in psychosis links appraisals of illness and burden to coping and EE-related pathways — useful for formulating carers as people with needs, not villains.[21]
Structural and systemic concepts
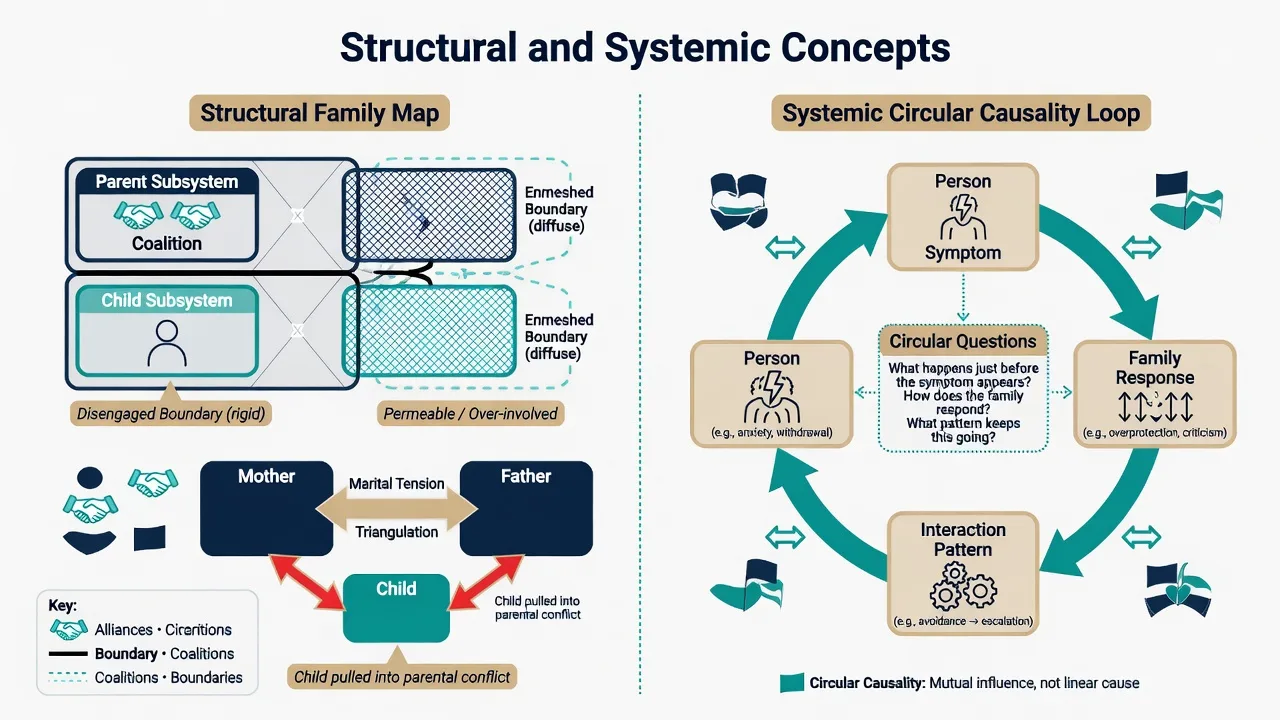
Boundary types: clear (flexible, appropriate), rigid/disengaged, diffuse/enmeshed. Triangulation: child (or patient) pulled into parental conflict. Coalition: two members allied against a third. Enactment: invite the pattern into the room and restructure it live.[19][20]
Circular questions (examples): "When X becomes withdrawn, who notices first? What does Y do next? What happens if Z tries something different?" Aim: map sequences without linear blame.[19]
Assessment for family work
- Genogram (2–3 generations): who lives where, contact hours, losses, illnesses, alliances.
- Explanatory models of each member (illness as moral failing vs brain disorder vs spiritual) — feeds psychoeducation tone.[22]
- EE proxies, warmth, problem-solving capacity, carer burden/mood/sleep/substances.[1][21]
- Confidentiality contract before joint sessions: what from individual care may be shared; what stays private.
- Safety screen every time: intimate partner violence, child protection, elder abuse, weapons, acute intoxication. Separate interviews if fear of speaking freely.
- Children of parents with mental illness (COPMI): developmental needs and protection, not only adult agenda.
- Cultural / Indigenous networks: who counts as family; elders; collective decision-making norms.
Evidence-based packages by indication
Psychosis and schizophrenia
What works: structured family intervention combining education, communication training, and problem-solving, typically over months (guideline principles often cite ≥10 sessions across ≥3 months, including the service user when possible).[5][7][13]
Landmark lines of evidence for structured family intervention in psychosis include controlled social-intervention and behavioural family-management programmes, psychoeducation trials, Cochrane synthesis, and network meta-analysis of relapse prevention formats.[5][6][7][8][9][11]
- Leff social intervention / educating relatives trials.[8]
- Falloon behavioural family management — clinical and social outcomes over two years.[9][10]
- Hogarty / Anderson family psychoeducation with maintenance medication and social skills components.[11]
- Cochrane (Pharoah et al.): family intervention can reduce relapse and hospital admission risk.[5]
- Pilling meta-analysis of family intervention and CBT in schizophrenia.[7]
- Rodolico et al. 2022 network meta-analysis: multiple family intervention formats reduce relapse versus treatment as usual — useful modern viva update.[6]
Session skeleton (BFT-style): engagement without blame → assessment of problem list and EE climate → illness and medication education → communication skills (I-statements, turn-taking, active listening) → structured problem-solving (define → brainstorm → evaluate → action → review) → relapse signature and crisis plan → carer self-care.[9][22]
Multifamily psychoeducation groups
McFarlane-line MFGs bring several families together: joining, education, problem-solving, peer modelling, reduced isolation. Reviews position family psychoeducation / MFG as an evidence-based practice in severe mental illness; FEP programmes have trialled MFG with other psychosocial components.[12][13][14]
Bipolar disorder — Family-Focused Therapy (FFT)
FFT plus pharmacotherapy improves outcomes versus less intensive comparators in RCTs (Miklowitz and colleagues; Rea et al. comparing family-focused vs individual approaches).[15][16] Modules: psychoeducation (including EE-relevant stress), communication enhancement training, problem-solving. Emphasise sleep regularity, early warning signs, and medication alliance as family tasks.
Adolescent depression and suicidality — ABFT
Attachment-based family therapy targets ruptured caregiver–adolescent attachment: relational reframe, building alliances, attachment/emotion-processing tasks, then promoting autonomy. Treatment-development and later trials support its use in depressed and suicidal adolescents, including adaptations for sexual and gender minority youth in subsequent literature.[17]
Anorexia nervosa — Family-Based Treatment (FBT)
Lock and colleagues' RCT found family-based treatment superior to adolescent-focused individual therapy on full remission rates at follow-up for adolescent anorexia — parents are empowered to lead refeeding before control is returned to the adolescent.[18]
Systemic therapy evidence (broad)
Meta-content analyses of RCTs support efficacy of systemic therapy for selected adult disorders and for many child/adolescent internalising and other presentations — cite von Sydow (adults) and Retzlaff (youth) as breadth evidence, then narrow to the disorder-specific package above when examiners want clinical specificity.[19][20]
Other high-yield applications
- OCD / anxiety: reduce family accommodation (reassurance loops, participating in rituals).[19][20]
- Dual diagnosis: align family messages about substances; avoid enabling vs punitive extremes.[12][21]
- Dementia carers: EE and criticism still matter for behavioural outcomes and carer wellbeing.[1][21]
- Open Dialogue and network-oriented approaches: emerging observational/register data; examiners expect curiosity without overselling as equivalent to NICE-level family intervention evidence.[12]
Acute vs definitive priorities
Acute / emergency: ABC, medical stability, individual risk (suicide/violence), least-restrictive legal framework. Use brief family contact for collateral, safety planning, and leave/discharge logistics — do not delay necessary treatment for a perfect family formulation.[5]
Definitive: diagnose-matched package; medication and individual therapy as indicated; carer assessment; COPMI needs; cultural adaptation; review EE climate and adherence barriers over time.[6][12]
Pitfalls and professionalism
| Pitfall | Why it fails | Better move |
|---|---|---|
| Blaming family for causing schizophrenia | False + alliance-destroying | Stress–vulnerability + collaboration |
| Pathologising culture as EOI | Racist/culturally unsafe care | Explore function and burden |
| Therapist triangulation | Reinforces split system | Neutrality, multi-partiality |
| Confidentiality blur | Ethical/legal breach | Explicit sharing contract |
| IPV in joint room | Safety catastrophe | Separate, protect, report |
| "Supportive chat" only | Misses relapse-prevention effect | Structured skills + education |
| Ignoring carer depression | Hidden morbidity | Assess and treat carers |
Prognosis and disposition
Family intervention for schizophrenia reduces relapse and readmission risk relative to usual care in systematic reviews and network meta-analysis; effects depend on delivery fidelity and duration.[5][6][7] Disposition planning should include: who the person returns to, EE climate, early warning signs card shared with consent, carer crisis contacts, and review of accommodation stress.
Step up family intensity when: repeated relapses with high-contact high-criticism home, family-driven non-adherence, carer collapse, or FEP with confused/conflictual illness models.[6][12]
Special populations
- Youth: ABFT, FBT, MST — developmental consent and child protection always active.[17][18]
- Older adults: carer EE, grief, capacity interfaces, elder abuse screening.[1][21]
- Perinatal: couple conflict and infant safety; do not force joint work if coercive.[12][21]
- Indigenous / minority cultural families: expand "who is family"; use cultural liaison; avoid individualistic assumptions.[12][21]
- LGBTQ youth: family rejection is a major risk amplifier; ABFT-style repair or alternative chosen-family supports.[17]
Exam pearls
FAMILY — psychosis family intervention checklist
- EE triad = criticism, hostility, EOI — not "emotional family".[1][2][3]
- High EE ≈ increased relapse risk (meta-analysis); intervention can lower risk.[1][5][6]
- NICE-style package: education + communication + problem-solving, multi-session, multi-month.[5][13]
- FFT for bipolar; FBT for adolescent anorexia; ABFT for adolescent depression/suicide.[15][17][18]
- Structural viva words: enmeshment, disengagement, triangulation, hierarchy, coalition.[19][20]
- Confidentiality and safety before joint therapy.[12][21]
- Illness facts, early warning signs, treatment alliance
- Reduces fear and misattribution
- Necessary but often not sufficient alone for high-conflict systems
- Adds communication and problem-solving skills
- Strong psychosis evidence lineage (Falloon)
- Homework and rehearsal essential
- Peer modelling and reduced isolation
- Efficient for services; McFarlane tradition
- Needs skilled facilitation and structure
References
- [1]Butzlaff RL, Hooley JM Expressed emotion and psychiatric relapse: a meta-analysis Arch Gen Psychiatry, 1998.PMID 9633674
- [2]Brown GW, Birley JL, Wing JK Influence of family life on the course of schizophrenic disorders: a replication Br J Psychiatry, 1972.PMID 5073778
- [3]Vaughn CE, Leff JP The influence of family and social factors on the course of psychiatric illness. A comparison of schizophrenic and depressed neurotic patients Br J Psychiatry, 1976.PMID 963348
- [4]Bebbington P, Kuipers L The predictive utility of expressed emotion in schizophrenia: an aggregate analysis Psychol Med, 1994.PMID 7991753
- [5]Pharoah F, Mari J, Rathbone J, et al. Family intervention for schizophrenia Cochrane Database Syst Rev, 2010.PMID 21154340
- [6]Rodolico A, Bighelli I, Avanzato C, et al. Family interventions for relapse prevention in schizophrenia: a systematic review and network meta-analysis Lancet Psychiatry, 2022.PMID 35093198
- [7]Pilling S, Bebbington P, Kuipers E, et al. Psychological treatments in schizophrenia: I. Meta-analysis of family intervention and cognitive behaviour therapy Psychol Med, 2002.PMID 12171372
- [8]Leff J, Kuipers L, Berkowitz R, et al. A controlled trial of social intervention in the families of schizophrenic patients: two year follow-up Br J Psychiatry, 1985.PMID 3893605
- [9]Falloon IR, Boyd JL, McGill CW, et al. Family management in the prevention of morbidity of schizophrenia. Clinical outcome of a two-year longitudinal study Arch Gen Psychiatry, 1985.PMID 2864032
- [10]Falloon IR, McGill CW, Boyd JL, et al. Family management in the prevention of morbidity of schizophrenia: social outcome of a two-year longitudinal study Psychol Med, 1987.PMID 3575578
- [11]Hogarty GE, Anderson CM, Reiss DJ, et al. Family psychoeducation, social skills training, and maintenance chemotherapy in the aftercare treatment of schizophrenia. II. Two-year effects of a controlled study on relapse and adjustment Arch Gen Psychiatry, 1991.PMID 1672589
- [12]McFarlane WR Family Interventions for Schizophrenia and the Psychoses: A Review Fam Process, 2016.PMID 27411376
- [13]Lucksted A, McFarlane W, Downing D, et al. Recent developments in family psychoeducation as an evidence-based practice Psychiatr Serv, 2012.PMID 22283383
- [14]Breitborde NJ, Moreno FA, Mai-Dixon N, et al. Multifamily group psychoeducation and cognitive remediation for first-episode psychosis: a randomized controlled trial Early Interv Psychiatry, 2011.PMID 21226941
- [15]Miklowitz DJ, George EL, Richards JA, et al. A randomized study of family-focused psychoeducation and pharmacotherapy in the outpatient management of bipolar disorder Arch Gen Psychiatry, 2003.PMID 12963672
- [16]Rea MM, Tompson MC, Miklowitz DJ, et al. Family-focused treatment versus individual treatment for bipolar disorder: results of a randomized clinical trial J Consult Clin Psychol, 2003.PMID 12795572
- [17]Diamond GS, Reis BF, Diamond GM, et al. Attachment-based family therapy for depressed adolescents: a treatment development study J Am Acad Child Adolesc Psychiatry, 2002.PMID 12364840
- [18]Lock J, Le Grange D, Agras WS, et al. Randomized clinical trial comparing family-based treatment with adolescent-focused individual therapy for adolescents with anorexia nervosa Arch Gen Psychiatry, 2010.PMID 20921118
- [19]von Sydow K, Beher S, Schweitzer J, et al. The efficacy of systemic therapy with adult patients: a meta-content analysis of 38 randomized controlled trials Fam Process, 2010.PMID 21083549
- [20]Retzlaff R, von Sydow K, Beher S, et al. The efficacy of systemic therapy for internalizing and other disorders of childhood and adolescence: a systematic review of 38 randomized trials Fam Process, 2013.PMID 24329407
- [21]Kuipers E, Onwumere J, Bebbington P Cognitive model of caregiving in psychosis Br J Psychiatry, 2010.PMID 20357299
- [22]Bäuml J, Froböse T, Kraemer S, et al. Psychoeducation: a basic psychotherapeutic intervention for patients with schizophrenia and their families Schizophr Bull, 2006.PMID 16920788