Psych · Professional — clinical skills
Formulation: biopsychosocial and 4Ps
Also known as Case formulation · Biopsychosocial formulation · 4P formulation · 5P formulation · Clinical formulation · Case conceptualisation · Cultural formulation · Multiperspective formulation
Exam-exhaustive fellowship reference on psychiatric case formulation — biopsychosocial model, 4Ps (predisposing, precipitating, perpetuating, protective), BPS×4P matrix, multiperspective and CBT/psychodynamic conceptualisations, DSM cultural formulation and CFI, worked examples, and CASC/viva technique linking formulation to a treatment plan. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Psychiatric exams (FRANZCP clinical assessments, MRCPsych CASC, MD/DNB viva) punish candidates who can recite criteria but cannot make sense of a person. Formulation is that sense-making skill: a living clinical hypothesis, not a one-off essay.[6][7][8]
Overview and definition
A case formulation is a structured clinical inference that:
[6] [7]- Names the presenting problem(s) in plain clinical language.
- Integrates biological, psychological, and social information (and cultural meaning).
- Organises factors across time: predisposing → precipitating → perpetuating, plus protective.
- States mechanisms (how factors interact), not only lists.
- Generates prioritised interventions and explicit uncertainties to re-test.[2][6][7]
Owen’s conceptual analysis emphasises that formulation is not a single fixed product; it is a family of practices with shared aims of explanation, communication, and treatment guidance.[7] Macneil and colleagues argue diagnosis alone is insufficient to guide individualised intervention in mental health — formulation bridges the gap between generic evidence and the person in front of you.[6]
Classification of formulation frameworks
Examiners accept several legitimate frameworks if used rigorously. Know the relationships, not tribal loyalty to one grid.
[6] [7]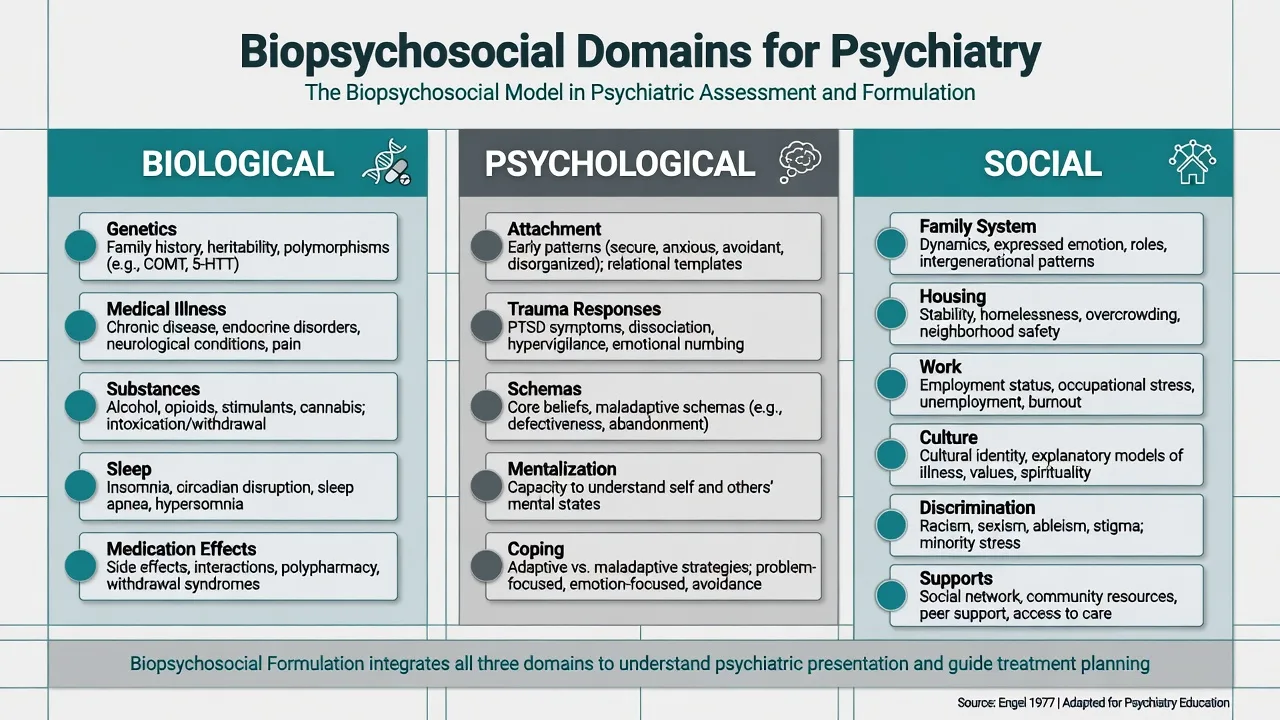
Biopsychosocial (BPS) model
Engel challenged biomedical reductionism and argued that clinical care must integrate biological, psychological, and social levels of organisation.[1][2] Later scientific commentaries retain the model’s clinical usefulness while demanding more rigorous, patient-centred, and empirically disciplined application — not a vague slogan.[3] Ghaemi’s critique is examinable: BPS can become an unfalsifiable eclecticism that excuses imprecise thinking if every factor is listed and none is prioritised.[4]
Exam stance: use BPS as levels of analysis, then force yourself to name mechanisms and priorities so the critique does not apply to your formulation.[3][4]
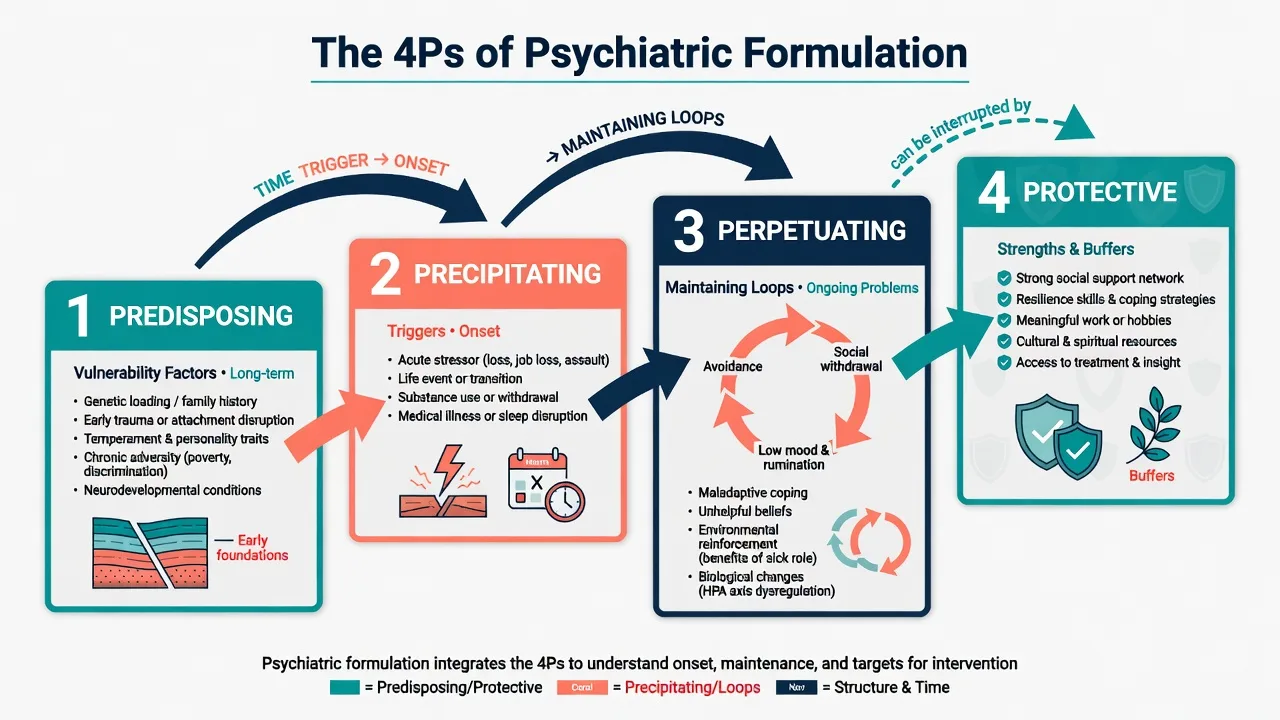
The 4Ps (and optional 5th P)
| P | Time orientation | Core question | Typical content |
|---|---|---|---|
| Presenting problem (optional 5th P / problem list) | Now | What exactly is wrong / distressing / risky? | Symptoms, MSE findings, functional impairment, risk behaviours |
| Predisposing | Long-term vulnerability | Why was this person vulnerable? | Genetics, early adversity, temperament, developmental disorders, chronic medical illness, structural disadvantage |
| Precipitating | Proximal trigger | Why now? | Loss, substances, sleep loss, medical illness, trauma, transition, non-adherence |
| Perpetuating | Maintaining loops | Why does it continue? | Avoidance, EE, isolation, untreated psychosis, substance loops, secondary gain, iatrogenic factors |
| Protective | Buffers | What reduces severity / enables recovery? | Attachments, skills, insight, employment, cultural/spiritual resources, service engagement |
BPS × 4P matrix
The high-yield exam tool is a matrix: rows = 4Ps; columns = bio / psycho / social (add culture as a cross-cutting column or integrate into social/psychological cells with explicit cultural content).
[12] [13]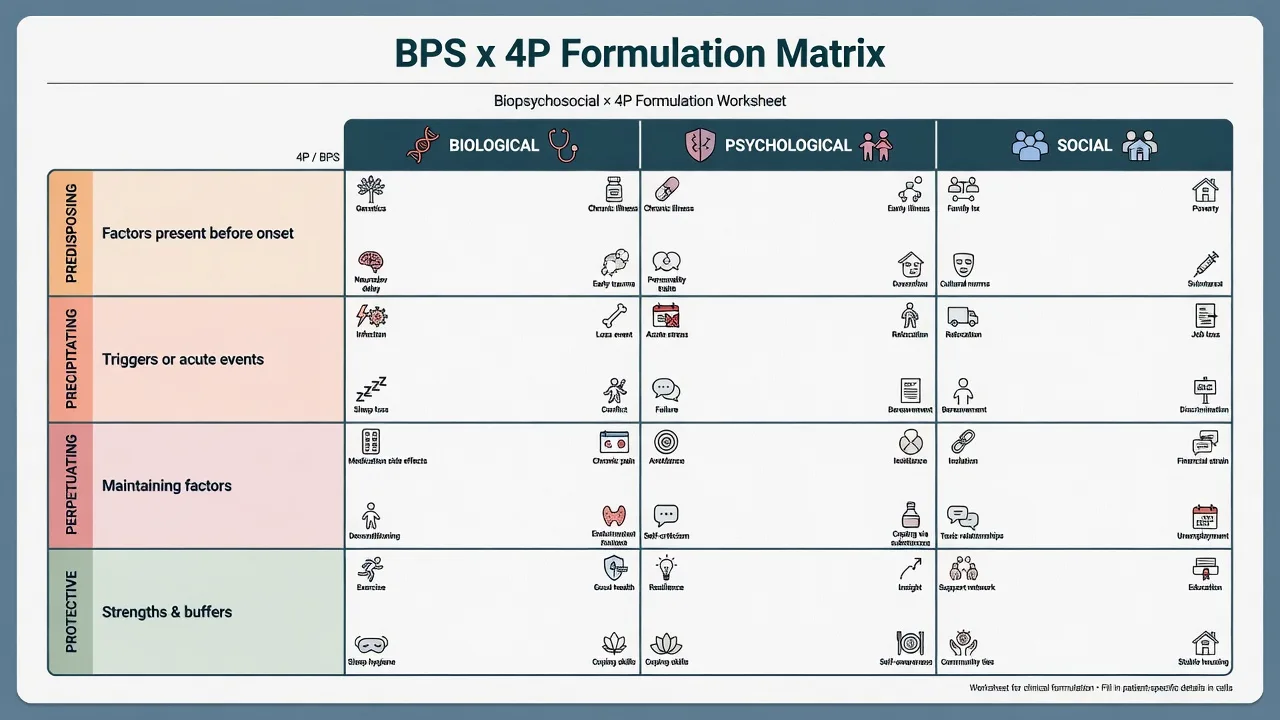
Other legitimate models
- Systematic lenses: biological, behavioural, cognitive, psychodynamic, social/systemic
- Forces breadth when candidates cling to one theory
- Still needs prioritisation for a usable plan
- Situation–cognition–emotion–behaviour cycles; core beliefs; compensatory strategies
- Collaborative; competence can be rated (e.g. CCCRS literature)
- Ideal when therapy is the main modality
- Development, conflict, defence, object relations, mentalization, transferential patterns
- Integrates with neurobiology rather than opposing it
- Must stay testable and non-jargon for general exams
Weerasekera’s multiperspective model remains a classic teaching scaffold for breadth.[5] Expert psychotherapy formulators use richer, more organised reasoning than novices — a research observation useful when examiners probe depth.[9] Collaborative CBT conceptualisation competence has measurement literature; formulation quality is a skill, not a vibe.[10] Psychodynamic formulation can be integrated with contemporary neuroscience rather than treated as anti-biological.[16] Sociocultural frameworks further specify how meaning, identity, and structural factors enter psychiatric case formulation.[17]
Epidemiology and clinical stakes
Formulation is not a disease with prevalence. Its “epidemiology” is the frequency of formulation failure in practice: polypharmacy without targets, ignored perpetuating factors, missed strengths, cultural misattunement, and plans that do not match the person’s world.[6][7]
Stakes rise when:
[6] [7]- Suicide or violence risk is active (formulation must connect risk to mechanisms and protections).
- First-episode psychosis, dual diagnosis, personality disorder, or complex trauma presentations invite oversimplification.
- C-L / capacity / forensic interfaces require multi-domain reasoning without inventing law.
- Team splitting is present — shared formulation is an antidote.
Mechanisms — how a formulation “works”
Think of formulation as a causal map, not a CV of the patient.
[6] [7]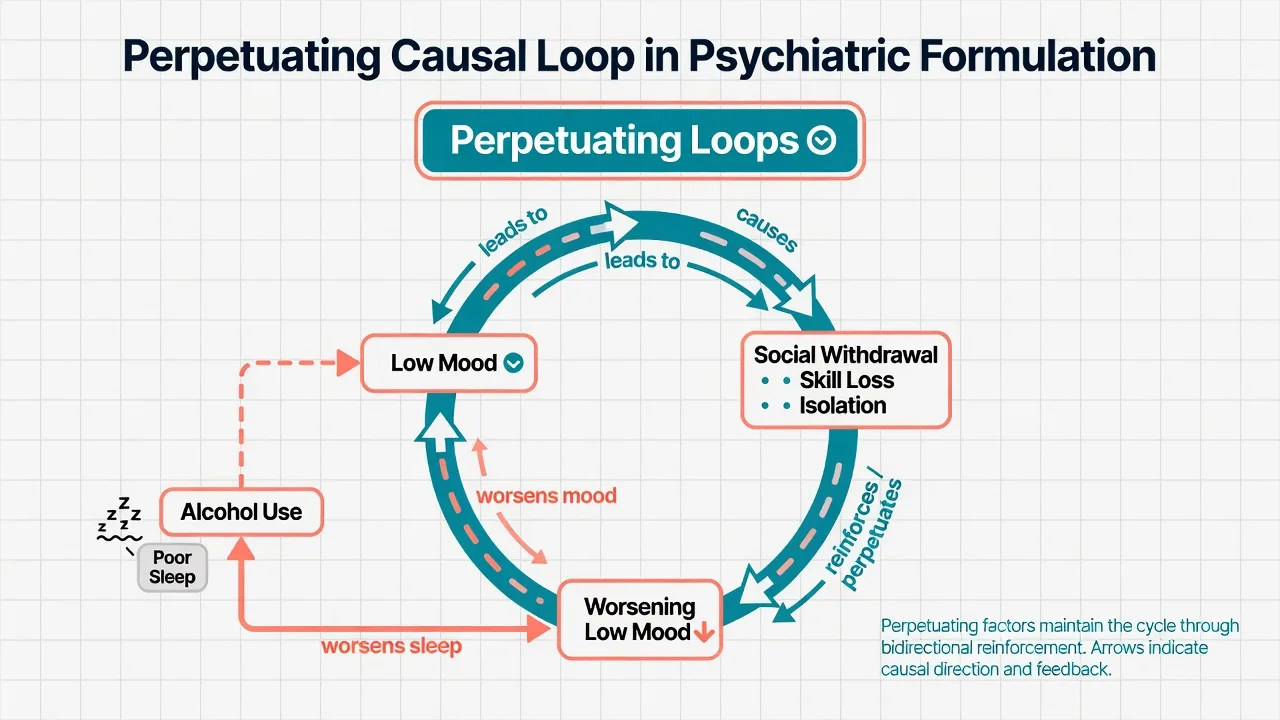
Core causal grammar:
[6] [7]- Predisposing factors raise baseline vulnerability (diathesis).
- Precipitating factors push the system over threshold (stress).
- Perpetuating factors create feedback loops that maintain symptoms after the trigger fades.
- Protective factors raise the threshold for relapse and create leverage for change.[6][7]
Level examples (illustrative mechanisms, not universal laws):
[6] [7]- Biological: cannabis + sleep loss + genetic loading → psychosis threshold; hypothyroidism → depressive syndrome.
- Psychological: threat appraisal + avoidance → anxiety maintenance; mentalization failure under stress → interpersonal crisis.
- Social: high expressed emotion + isolation → relapse risk; racism/housing precarity → chronic allostatic load and help-seeking barriers.[3][15][17]
Anti-pattern: listing “family history of depression, job loss, poor sleep” without saying how they connect. Examiners reward: “Job loss precipitated collapse of routine and self-worth; insomnia and alcohol then perpetuated low mood via reward-system disruption and missed morning activation.”
[6] [7]Clinical presentation of good vs weak formulations
What good looks like
- Opens with a clear problem statement and relevant diagnosis/differential status.
- Selects few high-impact factors per cell rather than dumping the entire history.
- Names mechanisms and modifiability.
- Includes protective factors and cultural meaning.
- Ends with a plan that maps 1:1 onto the formulation.
- Labels inferences as hypotheses open to revision.[6][7][8]
What weak looks like
- Diagnosis restated in longer sentences.
- Chronology without causality.
- Missing protections.
- Pejorative tone (“manipulative”, “secondary gain” used carelessly).
- No link to treatment.
- Culture omitted or reduced to ethnicity alone.[4][12]
Differential — what formulation is not
| Construct | Relation to formulation | Examiner trap |
|---|---|---|
| Diagnosis | Necessary input; not a substitute | Stopping at criteria |
| Problem list | Starting point only | Lists without mechanisms |
| Risk assessment | Overlaps; risk factors should appear in 4Ps | Risk form without explanatory model |
| MSE | Data source | Reading MSE as formulation |
| Therapy conceptualisation | Specialty depth within a modality | Forcing full CBT diagram in a general medical emergency |
| Storytelling | May feel coherent | Untestable, uncited-by-data narrative |
Assessment method — how to gather and present
History that feeds formulation
Systematically collect: developmental and attachment history; education/work; relationships; trauma and adversity; substances; medical/neurological; forensic; cultural identity and illness explanations; strengths and past coping; current stressors and supports.[2][12][15]
MSE and risk data are inputs, not an afterthought. Collateral and prior records often reveal perpetuating patterns the patient minimises.
[6] [7]Collaborative stance
Invite the person’s own model: “What do you think is going on? What helps even a little?” Collaborative conceptualisation is central in CBT literature and improves alliance when done well.[10][11] Cultural interviews repeatedly show that if you do not ask, patients often do not volunteer identity- and meaning-laden material relevant to care.[18]
Sixty-to-ninety-second exam structure (CASC / viva)
- Problem — one sentence.
- Diagnosis / differential status — one sentence.
- Predisposing — two to three high-yield factors.
- Precipitating — the tip-over.
- Perpetuating — the loops.
- Protective — the levers.
- Plan — bio / psycho / social + risk, each mapped to the above.
- Uncertainty — one thing you will re-test.
P4PLAN
Investigations and formulation revision
Formulation is reasoning, not a lab panel — but investigations rewrite the biological cells. Delirium work-up, thyroid function, substance screens, neuroimaging or autoimmune testing when indicated can convert a “functional” story into a medical–psychiatric formulation.[2][6] Serial rating scales and behavioural observations test hypotheses (“If we restore sleep, does mood follow?”).
Document formulation in the clinical record as a short structured paragraph or matrix plus plan; update after major new data.
[6] [7]Acute priorities (“resuscitation” of formulation)
In crisis, safety and medical stability first. Do not delay intramuscular sedation for NMS work-up discussion, or delay means restriction for a perfect essay.
[6] [7]Emergency formulation still helps disposition:
[6] [7]- What precipitated tonight?
- What perpetuates imminent risk (intoxication, command hallucinations, isolation)?
- What protects tonight (ally, housing, willingness to stay, plans for tomorrow)?
Then refine the full matrix when safe.
[6] [7]Definitive management — formulation to plan
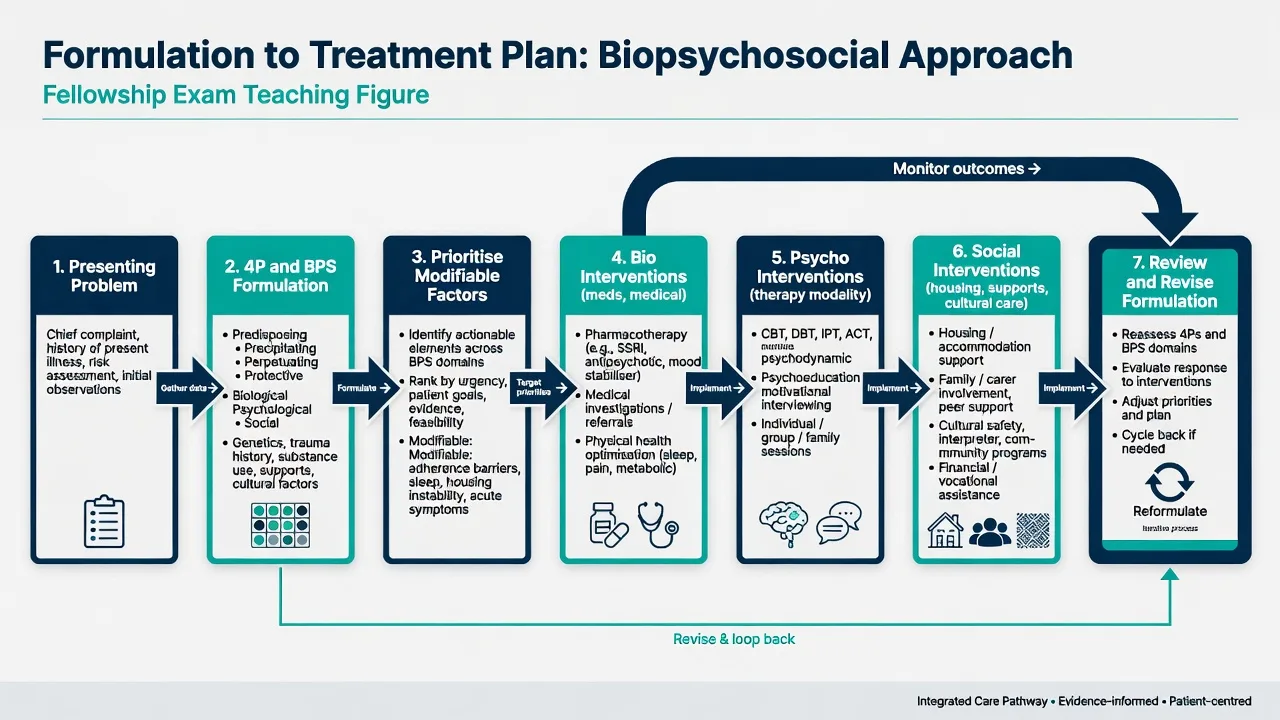
Translation rules:
[6] [7]| Formulation finding | Plan implication |
|---|---|
| Biological precipitant/perpetuator (substance, medical illness, insomnia, untreated psychosis) | Medical work-up; detox pathways; sleep restoration; evidence-based pharmacotherapy with a named target symptom |
| Psychological loops (avoidance, self-criticism, mentalization failure, trauma re-experiencing) | Matched therapy (CBT, trauma-focused, DBT/MBT/schema as indicated) with collaborative goals |
| Social perpetuators (housing, debt, EE, isolation, workplace stress) | Care coordination, family work, benefits/housing advocacy, vocational support |
| Protective factors | Amplify deliberately (re-engage sister, restore sport, spiritual community, study structure) |
| Cultural meaning / mistrust | Adapt engagement, use CFI-informed questions, involve preferred supports, avoid imposed explanatory models |
Evidence for formulation-driven psychotherapy practice supports individualised conceptualisation as a core clinical tool, even where trial designs vary.[8][11] Team formulation reduces inconsistent care when multiple clinicians hold different “theories of the patient.”
Review: formulation is a living document. After two weeks of abstinence, resolved mania, or new trauma disclosure, rewrite the matrix.
[6] [7]Worked examples
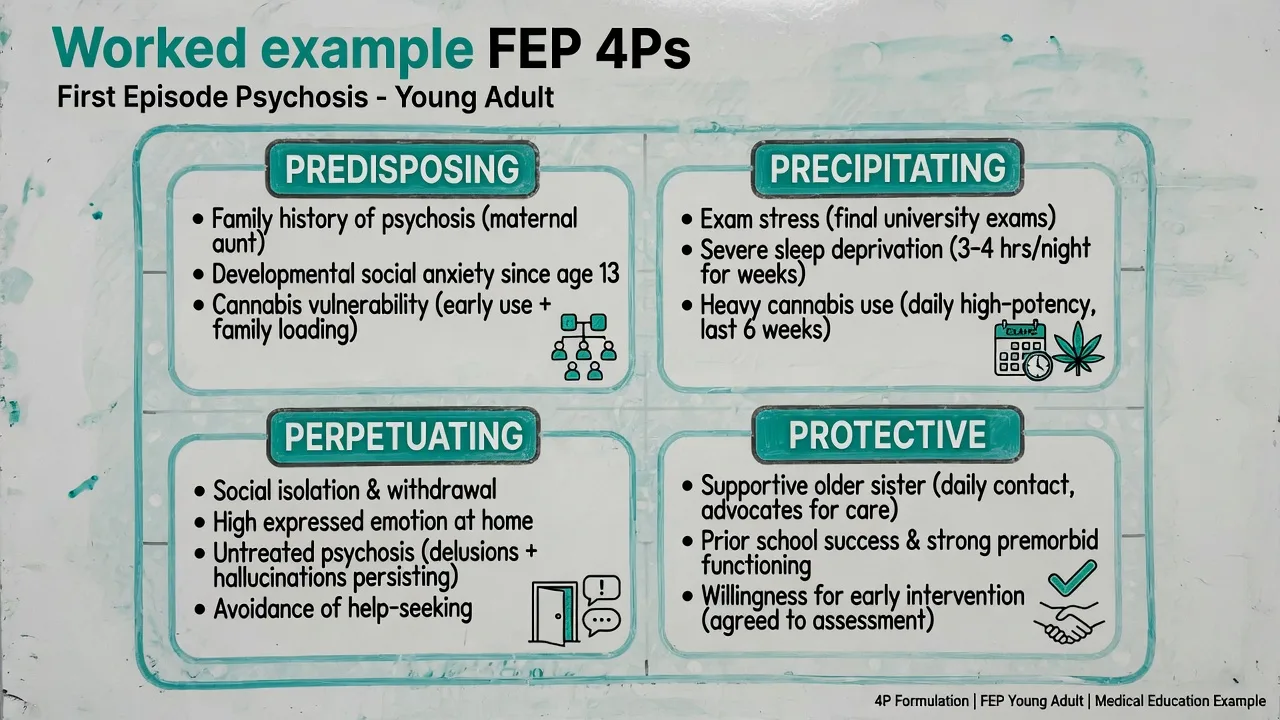
Example A — first-episode psychosis (condensed)
Problem. 19-year-old student with 6 weeks of persecutory delusions, auditory hallucinations, and functional collapse; cannabis use; first presentation.
[6] [7]Predisposing. First-degree family history of psychosis; longstanding social anxiety; heavy intermittent cannabis from age 16.
[6] [7]Precipitating. Exam period; progressive sleep restriction; daily high-potency cannabis.
[6] [7]Perpetuating. Social withdrawal; family high EE; untreated psychosis; ongoing cannabis; online echo chambers reinforcing threat beliefs.
[6] [7]Protective. Supportive older sister; prior academic competence; no forensic history; tentative willingness to try early intervention service.
[6] [7]Plan map. Medical/organic screen + antipsychotic trial targeting positive symptoms and sleep; cannabis psychoeducation and harm reduction; sleep hygiene and family psychoeducation to lower EE; early intervention psychosocial package; safety plan; CFI-style exploration of illness meaning with family if culturally relevant.[6]
Example B — major depression after job loss (condensed)
Problem. 47-year-old with 3 months of major depressive episode after redundancy; insomnia; alcohol escalation; passive death wish without plan.
[6] [7]Predisposing. Prior depressive episode age 30; anxious temperament; limited confiding relationships.
[6] [7]Precipitating. Sudden job loss and perceived status collapse.
[6] [7]Perpetuating. Alcohol → fragmented sleep → anergia → bed avoidance of job search → shame; cognitive rumination.
[6] [7]Protective. Partner support; no prior attempts; past response to an SSRI; values around parenting.
[6] [7]Plan map. Risk assessment and safety planning; alcohol reduction plan; sleep focus; restart previously effective antidepressant with monitoring; behavioural activation targeting avoidance; couples session for support without criticism; vocational rehab timing after partial response.[6][11]
Example C — emotion dysregulation crisis (BPD pattern)
Emphasise attachment trauma / invalidating environments (predisposing), interpersonal rejection (precipitant), self-harm as emotion regulation and reinforcing responses (perpetuating), and skills, alliances, structured therapy (protective). Plan privileges structured psychological therapy and crisis plan consistency over polypharmacy as first-line personality treatment logic (link to BPD topic for drug detail).
[6] [7]Cultural formulation
Culture is not an optional appendix. DSM’s Outline for Cultural Formulation (OCF) was operationalised for clinical use, and the Cultural Formulation Interview (CFI) provides a practical question set.[12][13][14]
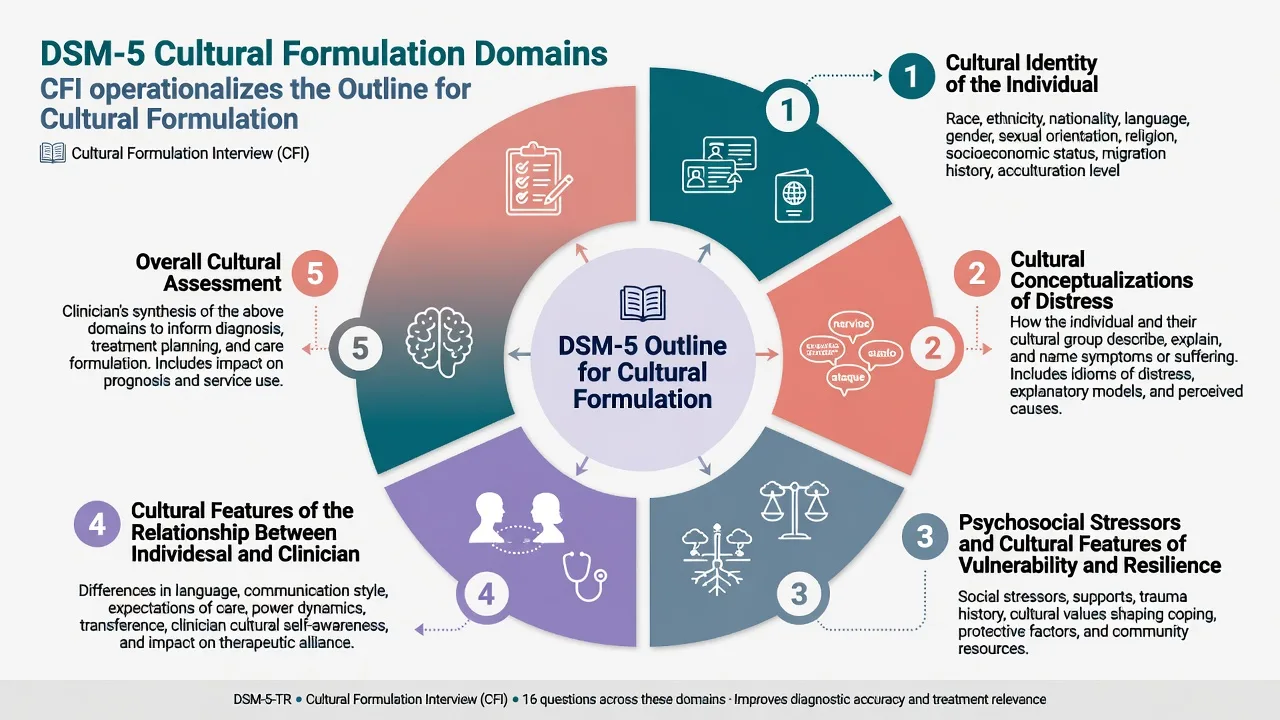
OCF domains (know these for exams):
[12] [13]- Cultural identity of the individual.
- Cultural conceptualisations of distress.
- Psychosocial stressors and cultural features of vulnerability and resilience.
- Cultural features of the relationship between the individual and the clinician.
- Overall cultural assessment for diagnosis and care.[12]
DSM-5 international field-trial mixed-methods work found the CFI generally feasible, acceptable, and clinically useful, while also identifying training and implementation barriers.[13] Subsequent work shows CFI content can surface social determinants, supports, and stressors that standard interviews miss, and that asking changes the clinical relationship.[14][15][18]
Practical exam tips:
[6] [7]- Use selected CFI-style questions; do not robotically recite all items in a 7-minute station.
- Culture includes migration, religion, occupation, military, LGBTQ+ communities, disability cultures — not only ethnicity.
- Avoid essentialism (“all X patients believe Y”).
- Do not let cultural respect become neglect of organic disease or risk.
In Aotearoa New Zealand and Australia, formulation should engage Indigenous cultural safety frameworks and local protocols (e.g. Māori models of health, Aboriginal and Torres Strait Islander cultural safety principles) as practice standards and relationship requirements, not as tokenistic checklist items. Exact organisational protocols are service-specific; name the need for cultural consultation and family/whānau involvement when appropriate.
[12][13]Specific scenarios (exam stems)
- Dual diagnosis: substances as predisposing and precipitating and perpetuating — draw the loop; integrated care plan.
- C-L: medical illness as bio precipitant; hospital environment as social perpetuator; family conflict over goals of care as meaning conflict.
- Perinatal: dual focus on parent and infant system; sleep deprivation and attachment threats as bio-psycho-social.
- Old age: vascular/neurocognitive contributors; grief; isolation; polypharmacy iatrogenesis.
- Forensic interface: formulation of offence-related pathways without replacing structured risk tools; legal tests remain jurisdiction-specific.
- Child/adolescent: development and family system dominate matrix cells; school as social domain.
Complications and pitfalls
Other traps: confusing correlation with causation; single-theory arrogance; over-culturalising encephalitis; under-culturalising trauma in majority patients; iatrogenic perpetuating factors (chaotic team responses, unnecessary polypharmacy, invalidating ward cultures).
[12] [13]Prognosis and disposition
Formulation informs prognosis by separating modifiable from fixed factors and by naming supports that make community care safe. Disposition decisions should cite risk and environmental perpetuators/protections (cannot return to violent household tonight; sister can supervise medication). Handover formulations should be short, mechanism-focused, and plan-linked.
[6] [7]Special populations
- Indigenous and minority groups: cultural humility, CFI, local cultural workers, power/history awareness.[12][14]
- Neurodevelopmental / intellectual disability: simplify language; behavioural phenotypes; carer system as co-formulated.
- Refugee/asylum: trauma, detention, legal uncertainty, language — avoid pathologising survival strategies.
- LGBTQ+: minority stress may be predisposing/perpetuating when relevant; do not assume it always is.
- Pregnancy/lactation: system formulation (parent–infant); medication decisions need separate evidence topics.
Evidence, guidelines, and controversies
| Anchor | Contribution |
|---|---|
| Engel 1977/1980 | BPS challenge to reductionism; clinical application |
| Borrell-Carrió et al. 2004 | Principles and scientific inquiry update |
| Ghaemi 2009 | Critique of woolly eclecticism |
| Weerasekera 1993 | Multiperspective teaching model |
| Macneil et al. 2012 | Diagnosis insufficient; formulation guides intervention |
| Owen 2023 | Conceptual clarification of formulation practices |
| Eells 2011/2025 | Expert reasoning; role of formulation in psychotherapy |
| Kuyken et al. 2016; Persons et al. 2006 | Collaborative conceptualisation competence; formulation-driven CBT outcomes |
| Lewis-Fernández / Aggarwal CFI programme | Operationalising cultural formulation; field-trial utility |
Controversy to defend either side briefly: Is BPS still useful? Yes, as levels of analysis with prioritisation. No, if it becomes unfalsifiable factor-dumping — then use sharper models (e.g. explicit mechanistic or therapy-specific conceptualisations) while retaining social determinants.[3][4]
There is no single RANZCP/NICE “mandatory formulation form.” What is mandatory in exams is demonstrable clinical reasoning.
[6] [7]Exam pearls
- Protective factors are the most common omission.
- Every factor needs a so what? for treatment.
- Culture ≠ ethnicity alone.
- Hypotheses are allowed — dogma is not.
- Link risk statement to the same matrix.
- In CASC, speak to the patient in human language; save denser jargon for the examiner discussion if asked.
- If challenged “that is just a list,” answer with one mechanism sentence and one plan link.
Self-test: convert this list into a formulation sentence
List: childhood neglect; recent breakup; binge drinking; supportive football coach; panic attacks.
[6][7]Model: Childhood neglect predisposed to abandonment sensitivity and limited emotion-regulation skills; the breakup precipitated acute panic and insomnia; binge drinking and avoidance of training now perpetuate physiological arousal and isolation; the coach relationship is a protective re-engagement lever — plan targets alcohol reduction, sleep, graded return to training with coach, and trauma-informed CBT for panic/abandonment appraisals.
[10][11]Summary one-pager
- Define problem and diagnosis status.
- Fill BPS × 4P matrix (include culture).
- Prune to high-impact mechanisms.
- Map each priority factor to an intervention.
- State risk/protective balance for disposition.
- Label uncertainties and review date.
- Revise as the person and data change.
Formulation is how psychiatrists show they can think. In fellowship exams, that is not optional colour — it is the skill under test.[6][7][8]
References
- [1]Engel GL The need for a new medical model: a challenge for biomedicine Science, 1977.PMID 847460
- [2]Engel GL The clinical application of the biopsychosocial model Am J Psychiatry, 1980.PMID 7369396
- [3]Borrell-Carrió F, Suchman AL, Epstein RM The biopsychosocial model 25 years later: principles, practice, and scientific inquiry Ann Fam Med, 2004.PMID 15576544
- [4]Ghaemi SN The rise and fall of the biopsychosocial model Br J Psychiatry, 2009.PMID 19567886
- [5]Weerasekera P Formulation: a multiperspective model Can J Psychiatry, 1993.PMID 8348476
- [6]Macneil CA, Hasty MK, Conus P, et al. Is diagnosis enough to guide interventions in mental health? Using case formulation in clinical practice BMC Med, 2012.PMID 23016556
- [7]Owen G What is formulation in psychiatry? Psychol Med, 2023.PMID 36878884
- [8]Eells TD The role of case formulation in the current practice of psychotherapy World Psychiatry, 2025.PMID 40948051
- [9]Eells TD, Lombart KG, Salsman N, et al. Expert reasoning in psychotherapy case formulation Psychother Res, 2011.PMID 21240834
- [10]Kuyken W, Beshai S, Dudley R, et al. Assessing Competence in Collaborative Case Conceptualization: Development and Preliminary Psychometric Properties of the Collaborative Case Conceptualization Rating Scale Behav Cogn Psychother, 2016.PMID 25629820
- [11]Persons JB, Roberts NA, Zalecki CA, et al. Naturalistic outcome of case formulation-driven cognitive-behavior therapy for anxious depressed outpatients Behav Res Ther, 2006.PMID 16209865
- [12]Lewis-Fernández R, Aggarwal NK, Bäärnhielm S, et al. Culture and psychiatric evaluation: operationalizing cultural formulation for DSM-5 Psychiatry, 2014.PMID 24865197
- [13]Lewis-Fernández R, Aggarwal NK, Lam PC, et al. Feasibility, acceptability and clinical utility of the Cultural Formulation Interview: mixed-methods results from the DSM-5 international field trial Br J Psychiatry, 2017.PMID 28104738
- [14]Lewis-Fernández R, Aggarwal NK, Kirmayer LJ The Cultural Formulation Interview: Progress to date and future directions Transcult Psychiatry, 2020.PMID 32838656
- [15]Aggarwal NK, Chen D, Lewis-Fernández R Eliciting social stressors, supports, and determinants of health through the DSM-5 cultural formulation interview Front Psychiatry, 2023.PMID 37056400
- [16]Newman LK Psychodynamic formulation in the era of the brain - towards integration Australas Psychiatry, 2017.PMID 28486814
- [17]Weiss MG, Deshmukh A, Sarmukaddam SB, et al. Sociocultural Framework for Psychiatric Case Formulation J Nerv Ment Dis, 2024.PMID 37874984
- [18]Aggarwal NK, Chen D, Lewis-Fernández R If You Don't Ask, They Don't Tell: The Cultural Formulation Interview and Patient Perceptions of the Clinical Relationship Am J Psychother, 2022.PMID 35430870