Psych · Professional — leadership and clinical governance
Leadership and clinical governance
Also known as Clinical governance · Patient safety culture · Quality improvement psychiatry · Just culture · Open disclosure · Clinical audit · Transformational leadership healthcare · High reliability organisation · Systems approach to error · Psychological safety teams
Exam-exhaustive fellowship reference on clinical governance (Scally–Donaldson), Donabedian quality, systems vs person approaches to error, just culture, leadership behaviours, clinical audit and PDSA, serious incident response, open disclosure, second victim support, high-reliability concepts, and regional governance frames for psychiatry. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Overview and definition
Fellowship exams test leadership and clinical governance because every consultant will chair multi-disciplinary meetings, supervise trainees, respond to serious incidents, sit on quality committees, and shape unit culture. The core claim is organisational, not charismatic: quality and safety are properties of systems led by people, not the private virtue of individual doctors alone.[1][4][10]
Clinical governance, classically defined by Scally and Donaldson for the NHS, is a framework of accountability for continuous quality improvement and the maintenance of high standards of care by creating an environment in which excellence in clinical care will flourish.[1] It is related to but not identical with corporate governance (boards, finance, strategy) or professional regulation (medical boards, college codes). Psychiatry candidates must hold all three layers without conflating them.
Clinical leadership is the set of behaviours and formal roles through which clinicians set direction, model safety, enable teams, and hold the service accountable for outcomes. Leadership is not synonymous with a job title; absent or toxic leadership is itself a patient-safety hazard.[10][19]
Quality of care, in Donabedian's enduring formulation, is assessed through structure (resources, staffing, facilities, policies), process (what is done for and with the patient), and outcome (health status, experience, harm).[2] Examiners expect candidates to map any service problem onto this triad rather than only listing outcomes.

Classification — pillars, quality triad, and leadership styles
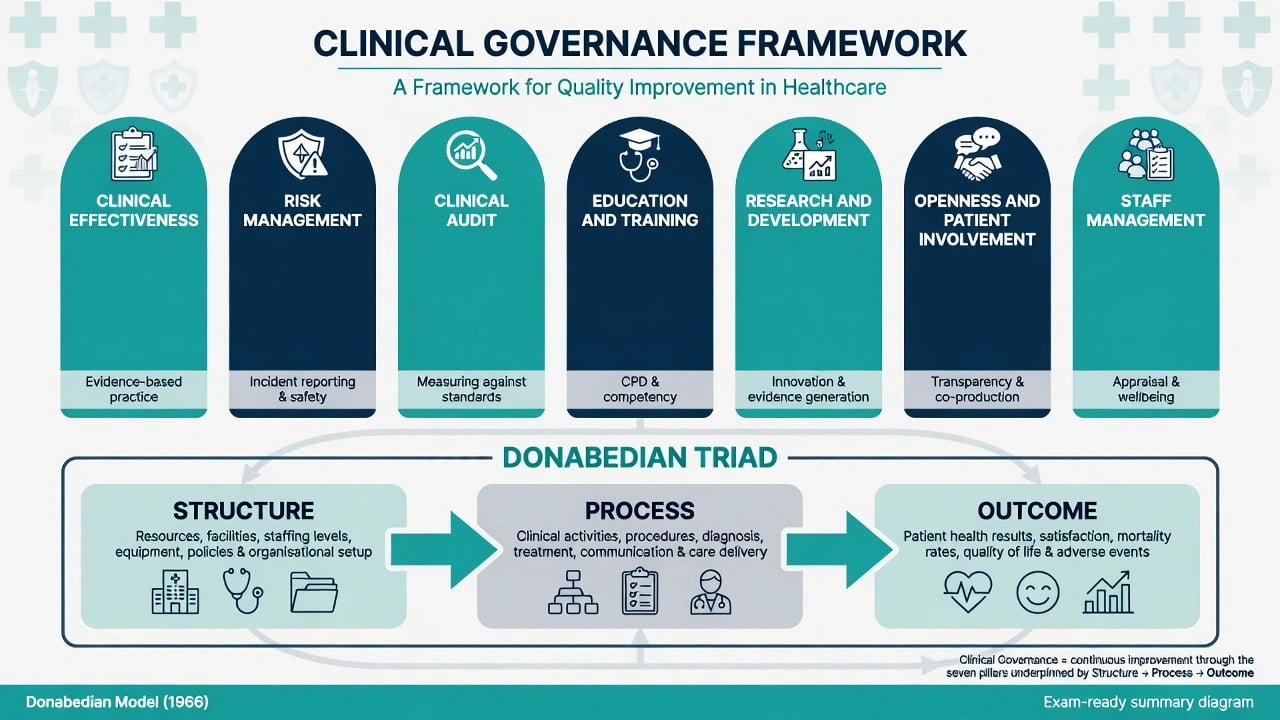
Classic teaching organises clinical governance into interlocking pillars (wording varies slightly by jurisdiction; the functions matter more than a fixed seven-name brand), consistent with Scally–Donaldson accountability for quality and Donabedian measurement domains.[1][2]
| Pillar / function | Psychiatry-facing content |
|---|---|
| Clinical effectiveness | Guidelines, evidence-based care, high-dose antipsychotic review, clozapine pathways |
| Risk management | Incident reporting, risk registers, restrictive practice, absconding, suicide aftercare |
| Clinical audit | Standards, measurement, change, re-audit |
| Education and training | Supervision, simulation, mandatory training fidelity |
| Research and development | Ethical research governance, knowledge translation |
| Openness and patient involvement | Open disclosure, co-design, complaints as signal |
| Staff management | Appraisal, rostering, wellbeing, just culture |
| (sources) | Scally–Donaldson functions; Donabedian quality domains [1][2] |
Leadership styles examiners commonly probe (transformational styles associate with safety culture; culture research shows how leadership behaviour shapes learning): Transformational — vision, inspiration, intellectual stimulation, individualised consideration; associated with stronger safety culture and engagement in care settings. Transactional — clear targets, monitoring, contingent reward; useful for reliability tasks, toxic when reduced to target-gaming. Collective / distributive — leadership as shared work across the multi-disciplinary team, not a heroic consultant myth. Authentic / servant — values-consistent behaviour and staff enablement; examined as antidote to authoritarian silence cultures.[10][11][14][19]
- Staffing ratios
- Policies and protocols
- Equipment and environment
- Committee architecture
- Risk assessment quality
- Handover fidelity
- Medication safety steps
- Open disclosure practice
- Harm rates
- Readmission
- Restraint episodes
- Patient experience
Epidemiology and risk context
The Institute of Medicine report To Err Is Human reframed preventable harm as a major public health problem produced largely by systems, not by a few reckless individuals — a watershed whose impact is visible in the subsequent patient-safety literature.[4] Leape's earlier synthesis of error in medicine similarly argued that punishing individuals without redesigning work is an ineffective safety strategy.[5]
Candidates should quote orders of magnitude and principles, not memorised single-year mortality numbers as if they were timeless constants. What examiners want is the shift: harm is common enough to demand systematic governance, and under-reporting means true rates exceed formal incident statistics.[4][5]
Unit-level risk signals for psychiatry services include rising restraint/seclusion without learning reviews, clustered medication incidents, failed clozapine monitoring, repeated AWOL events, suicide after discharge without case review, and trainee silence in meetings. Leader support and staff influence over decisions associate with better work and patient-related outcomes in multi-level studies; transformational leadership links to safety culture and work engagement.[13][14] Physician burnout and poorer unit safety grades associate with higher reported medical error — governance and workforce wellbeing are not separate silos.[15]
Mechanisms — how systems fail and how cultures learn
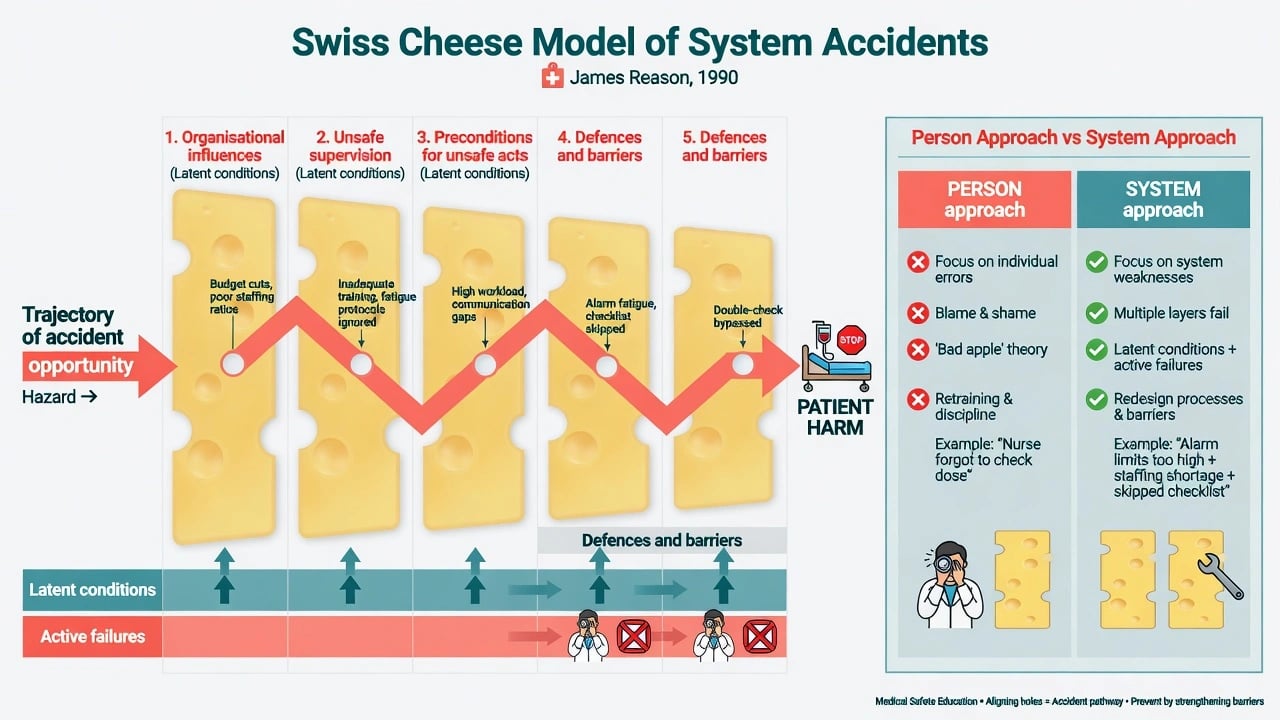
Reason distinguishes the person approach (errors as moral failings of individuals) from the system approach (errors as expected products of fallible humans in imperfect systems). Defences are like Swiss cheese slices; harm occurs when holes (active failures and latent conditions) align into a trajectory of accident opportunity.[3] Active failures are unsafe acts at the sharp end; latent conditions are resident pathogens in design, staffing, training, equipment, and culture.[3]
Vincent and colleagues provide a practical analytic frame spanning patient factors, task/technology, individual staff, team, work environment, organisation and management, and institutional context — a checklist for incident analysis that goes beyond "who forgot the checklist."[7] Vincent later argued that incident analysis should open a window on the system, not merely hunt a single root cause that ends at human error.[12]
Culture is the mechanism that turns policy into daily practice. Multimethod NHS work by Dixon-Woods and colleagues showed how cultural and behavioural patterns — including variation, problem-sensing versus problem-denying, and the quality of relationships — shape whether services improve or drift into harm.[19] Organisational trust and learning teamwork cultures are keystones of safety; fear destroys reporting.[11][10]
High-reliability organisation (HRO) principles (preoccupation with failure, reluctance to simplify interpretations, sensitivity to operations, commitment to resilience, deference to expertise) describe how high-hazard industries keep failure rare; Chassin and Loeb adapt the journey for healthcare reliability.[9] Continuous improvement as an ideal — not episodic inspection alone — is the Berwick thread running through modern QI.[6]
Clinical presentations (exam stems)
Classic stems: a ward with rising seclusion hours and a charge nurse who says "we just do not report near misses anymore"; a trainee who nearly prescribed a wrong depot dose and is terrified of the consultant; a serious suicide three days after discharge with known risk factors not escalated; a board paper demanding "the root cause person"; a family asking why no one apologised after a medication error; a QI project that ran one incomplete PDSA cycle and was declared finished; a private psychiatrist with no peer review or incident pathway.[3][12][18][20]
Differential — concepts examiners mix
| Concept | Is | Is not |
|---|---|---|
| Clinical governance | Organisational QI and safety accountability | Only a monthly committee meeting |
| Clinical audit | Measure against standards, change, re-measure | Research seeking generalisable new knowledge |
| QI / PDSA | Iterative local tests of change | One-off project theatre without data |
| Just culture | Fair accountability by intent/behaviour class | Pure "no blame" for reckless acts |
| Open disclosure | Honest apology and plan after harm | Legalistic script without empathy |
| Leadership | Behaviours creating conditions for safe care | Title alone or micromanagement |
Assessment of a service and of an incident
There is no blood test for governance quality. Assessment is multi-source and draws on culture, reporting, and human-factors frameworks.[7][11]
Unit culture scan (bedside leadership): speaking-up climate; incident and near-miss reporting trends; restraint, AWOL, medication, and complaint themes; supervision fidelity; consumer participation; whether bad news reaches leaders early; burnout signals and roster pressure.[11][15][19]
Serious incident assessment structure (window on the system, not a hunt for a single villain): immediate clinical facts and ongoing risk; chronology of work as done; care delivery problems and contributory factors across Vincent levels; latent conditions and redesign opportunities; just-culture behavioural classification (human error vs at-risk vs reckless); patient/family needs and second-victim staff needs; action plan with owners, dates, and measures of completion.[7][12][16][17]
SAFER-LEAD
Investigations and improvement methods
- Incident data and safety climate measures — interpret reporting rates carefully: rising reports can mean safer culture, not necessarily more harm.[11]
- Clinical audit cycle — agree standards → measure practice → compare → implement change → re-measure. An audit without re-audit is incomplete.
- PDSA — plan a small test, do it, study data, act (adopt/adapt/abandon). Taylor and colleagues found that published PDSA applications often lack full iterative cycles and robust measures — examiners may probe whether a candidate can run real PDSA rather than slogan PDSA.[20]
- Systems QI exemplars — Pronovost's multi-faceted central-line infection reduction showed large harm reduction through standardised processes, culture, and measurement — a classic systems success story transferable in spirit to psychiatry pathway reliability (e.g. clozapine monitoring, depot safety).[8]
Immediate management after harm
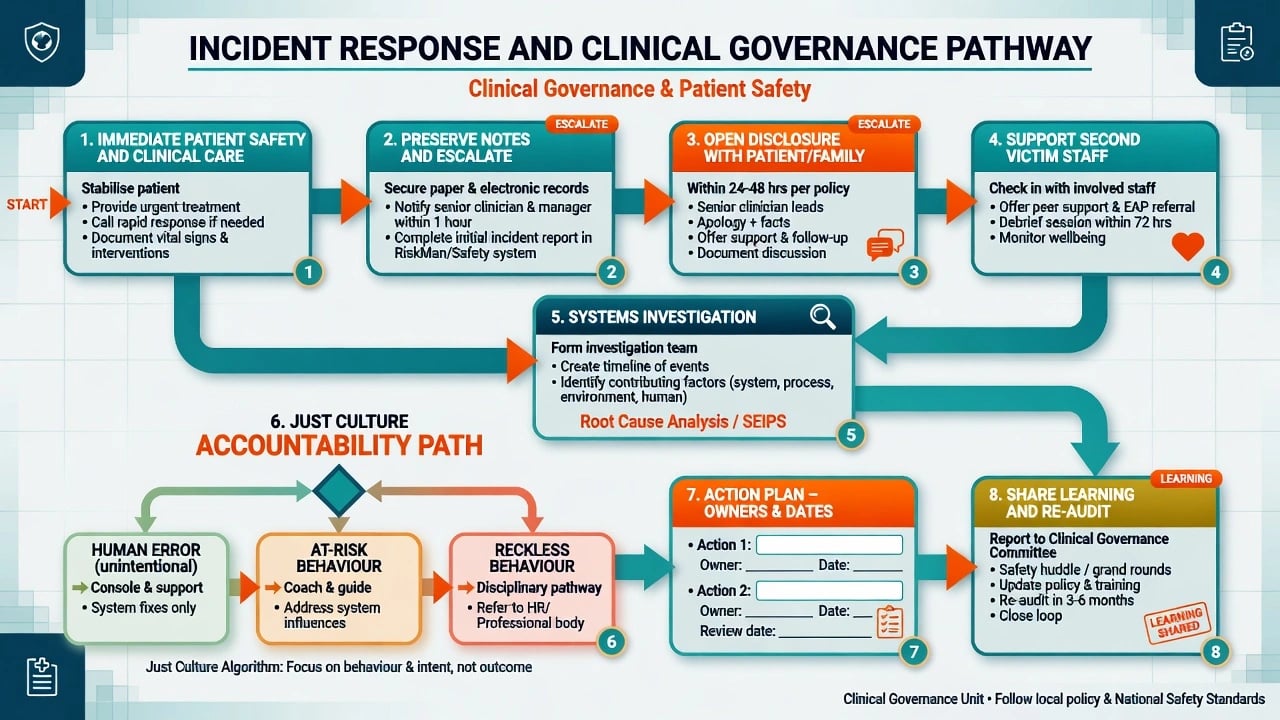
First priorities: clinical care of the patient; stop ongoing risk to others; preserve contemporaneous notes; escalate to seniors and governance pathways per local policy; avoid premature public or social-media commentary.[4][18]
Open disclosure / duty of candour principles: patients and families value timely, honest explanation, apology, what will happen next, and ongoing contact — not defensive silence.[18] Exact statutory wording is jurisdiction-specific; do not invent section numbers.
Second victim: the clinician involved in an error often experiences profound shame, isolation, and risk of further error or mental illness; leaders must arrange structured support, not only investigation.[17]
Definitive management — building and leading governance
Just culture
After Mid Staffordshire, Dekker and Hugh argued for just culture rather than pure blame or pure no-blame: console and redesign after human error; coach at-risk behaviour; reserve disciplinary pathways for reckless disregard.[16] Outcome severity alone must not determine blame (outcome bias).
Leadership behaviours that improve care
Firth-Cozens links leadership quality to care quality and describes how leaders shape learning cultures and teamwork.[10][11] Practical exam checklist (set a clear safety vision and model behaviour; invite challenge from juniors, nurses, peer workers, and consumers; resource improvement work with time and data; respond to bad news with curiosity not humiliation; align rewards with safe care not only throughput; close the loop with owners, dates, and re-measurement).[10][11][19]
Leader support and staff voice over decisions relate to better staff and patient-related outcomes; transformational leadership associates with safety culture.[13][14]
Continuous improvement infrastructure
Berwick's continuous improvement ideal requires measurement for learning, not only judgment.[6] HRO principles push preoccupation with failure and deference to expertise at the sharp end.[9] Board and clinical micro-system leadership must connect: assurance without frontline improvement is hollow; frontline projects without executive sponsorship die.[6][9]
Psychiatry-specific governance scenarios
Psychiatry applies the same governance pillars to high-risk pathways: restrictive practice (report, review thresholds, least-restrictive alternatives, consumer debrief); suicide and serious self-harm (serious incident review, family involvement principles, leave/discharge learning); medication safety (high-dose antipsychotic audit, lithium/clozapine monitoring reliability, depot missed-dose pathways); educational governance (supervision records, WBA quality, psychological safety for trainees to report near misses).[1][11][12]
Special populations and settings
Trainees and hierarchy. Juniors often know about hazards first and speak last; leaders must actively invite challenge and protect reporters from retaliation.[11][19]
Consumers, carers, peer workers. Openness and co-production are governance pillars, not optional soft skills.[1][18]
Indigenous and CALD communities. Culturally safe complaint and disclosure pathways; avoid governance that only works for majority language speakers — openness and patient involvement are core pillars.[1][18]
Forensic and involuntary care. Dual clinical–legal accountability; documentation and rights safeguards are structure measures with liberty consequences.[2]
Rural and private practice. Peer review networks, telehealth peer support, and deliberate incident pathways compensate for isolation that otherwise weakens learning cultures.[11][19]
Complications and pitfalls
Classic pitfalls: blame culture that silences reporting; target-gaming that displaces care; RCA that stops at human error; incomplete audit cycles; open disclosure as legal ritual without empathy; ignoring second victims; leadership by title without presence; inventing universal statute numbers; excluding consumers; treating burnout and safety as unrelated; declaring QI finished after a single weak PDSA cycle.[12][15][16][18][19][20]
Prognosis and disposition
Mature safety cultures report more, learn faster, and surprise less. Immature cultures look quiet until a catastrophic event. After a serious incident, disposition includes patient/family support, staff support, system actions with assurance, possible external notification per local rules, and spread of learning.[4][16][17] Sustained improvement needs standard work, monitoring for drift, and leadership continuity.[6][9]
Evidence, guidelines, and regional differences
Landmark anchors: Scally–Donaldson clinical governance; Donabedian quality triad; Reason person vs system and Swiss cheese; IOM To Err Is Human; Leape error in medicine; Berwick continuous improvement; Vincent risk framework and incident analysis; Pronovost systems QI exemplar; Chassin high reliability; Firth-Cozens leadership/culture/trust; Dixon-Woods NHS culture study; West/Ree leadership and safety culture associations; Tawfik burnout–error–safety grades; Dekker just culture; Wu second victim; Iedema open disclosure patient views; Taylor PDSA methods review.[1][2][3][4][8][9][16][18][19][20]
[1] [4] [16] [19]Exam pearls
References
- [1]Scally G, Donaldson LJ The NHS's 50 anniversary. Clinical governance and the drive for quality improvement in the new NHS in England BMJ, 1998.PMID 9651278
- [2]Donabedian A The quality of care. How can it be assessed? JAMA, 1988.PMID 3045356
- [3]Reason J Human error: models and management BMJ, 2000.PMID 10720363
- [4]Stelfox HT, Palmisani S, Scurlock C, Orav EJ, Bates DW The "To Err is Human" report and the patient safety literature Qual Saf Health Care, 2006.PMID 16751466
- [5]Leape LL Error in medicine JAMA, 1994.PMID 7503827
- [6]Berwick DM Continuous improvement as an ideal in health care N Engl J Med, 1989.PMID 2909878
- [7]Vincent C, Taylor-Adams S, Stanhope N Framework for analysing risk and safety in clinical medicine BMJ, 1998.PMID 9552960
- [8]Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU N Engl J Med, 2006.PMID 17192537
- [9]Chassin MR, Loeb JM High-reliability health care: getting there from here Milbank Q, 2013.PMID 24028696
- [10]Firth-Cozens J, Mowbray D Leadership and the quality of care Qual Health Care, 2001.PMID 11700372
- [11]Firth-Cozens J Cultures for improving patient safety through learning: the role of teamwork Qual Health Care, 2001.PMID 11700376
- [12]Vincent CA Analysis of clinical incidents: a window on the system not a search for root causes Qual Saf Health Care, 2004.PMID 15289620
- [13]West THR, Daher P, Dawson JF, et al. The relationship between leader support, staff influence over decision making, work pressure and patient satisfaction: a cross-sectional analysis of NHS datasets in England BMJ Open, 2022.PMID 35105577
- [14]Ree E, Wiig S Linking transformational leadership, patient safety culture and work engagement in home care services Nurs Open, 2020.PMID 31871709
- [15]Tawfik DS, Profit J, Morgenthaler TI, et al. Physician Burnout, Well-being, and Work Unit Safety Grades in Relationship to Reported Medical Errors Mayo Clin Proc, 2018.PMID 30001832
- [16]Dekker SW, Hugh TB A just culture after Mid Staffordshire BMJ Qual Saf, 2014.PMID 24505113
- [17]Wu AW Medical error: the second victim. The doctor who makes the mistake needs help too BMJ, 2000.PMID 10720336
- [18]Iedema R, Allen S, Britton K, et al. Patients' and family members' views on how clinicians enact and how they should enact incident disclosure: the IIPDS study BMJ Qual Saf, 2011.PMID 21788260
- [19]Dixon-Woods M, Baker R, Charles K, et al. Culture and behaviour in the English National Health Service: overview of lessons from a large multimethod study BMJ Qual Saf, 2014.PMID 24019507
- [20]Taylor MJ, McNicholas C, Nicolay C, et al. Systematic review of the application of the plan-do-study-act method to improve quality in healthcare BMJ Qual Saf, 2014.PMID 24025320