Psych · Professional — LGBTQ+ affirming psychiatric care
LGBTQ+ affirming psychiatric care
Also known as Sexual minority mental health · Gender minority mental health · Minority stress psychiatry · LGB affirming care · SOGI-affirming psychiatry · Conversion therapy harm · Sexual orientation change efforts · LGBTQIA+ mental health · Affirmative psychotherapy · ESTEEM therapy
Exam-exhaustive fellowship topic on LGBTQ+ affirming psychiatric care: Meyer minority stress, disparities in depression anxiety substance use and suicidality, family rejection versus acceptance, inclusive SOGI assessment, rejection of conversion practices, LGB-affirmative CBT evidence, structural stigma, and intersectional practice. Affirming and evidence-based. Gender dysphoria medical pathways cross-linked to specialty leaf. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Definition and classification
Core constructs
Do not conflate: sexual orientation (attraction, behaviour, identity — these dimensions can diverge), gender identity (internal sense of gender), gender expression, and sex assigned at birth. LGBTQ+ / LGBTQIA+ is an umbrella term spanning diverse sexual and gender minorities; within-group heterogeneity is large.[9][10]
Homosexuality is not a mental disorder. Depathologisation in psychiatric nosology was a scientific and human-rights correction; modern care does not treat orientation as a pathology to reverse.[13]
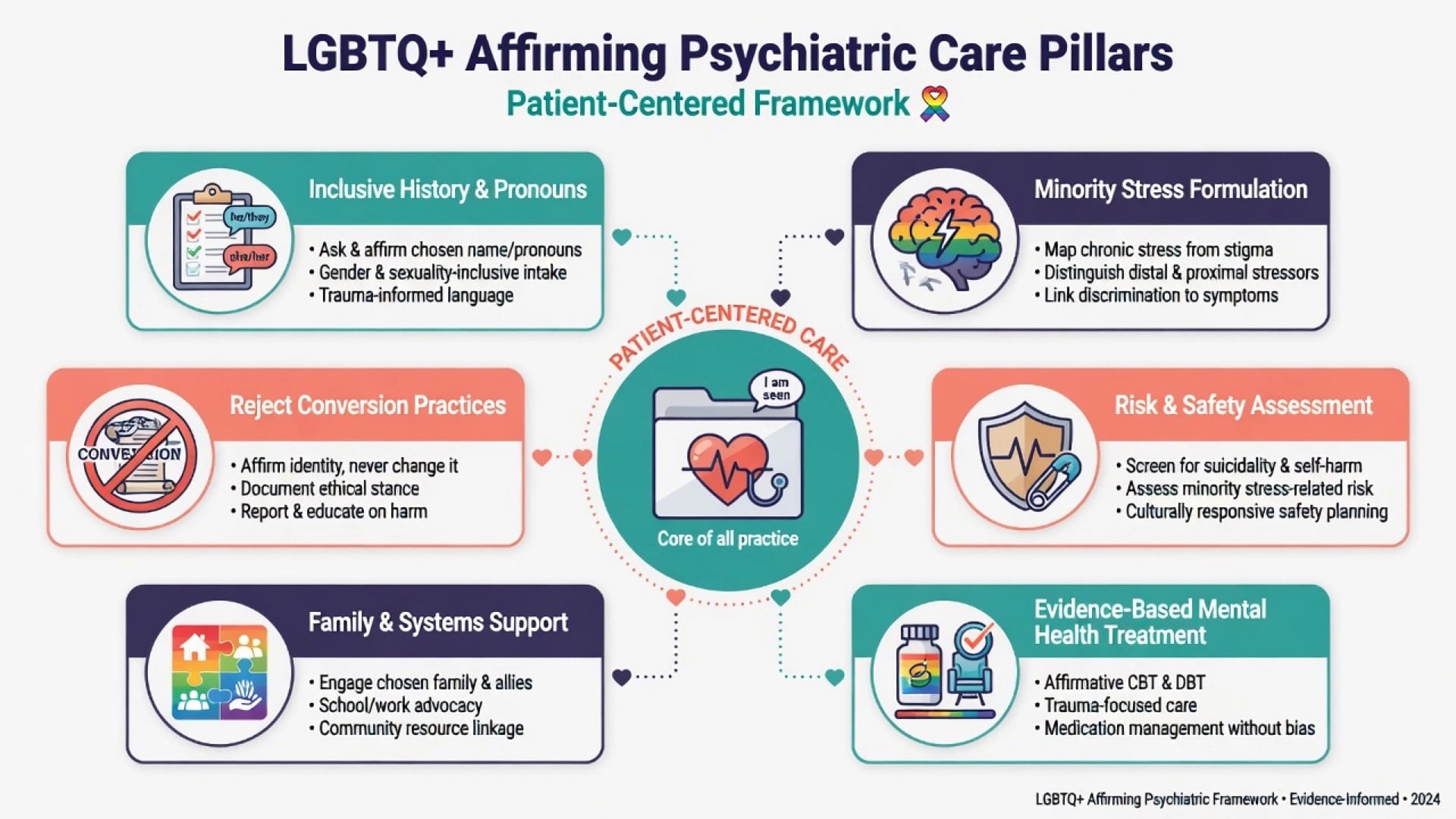
Affirming care means a non-pathologising stance: use affirmed names and pronouns, validate identity, formulate minority stress, treat concurrent psychiatric syndromes when present, and reduce iatrogenic harm. It is compatible with rigorous differential diagnosis and does not require inventing illness where none exists, nor withholding treatment where illness does exist.[1][7]
Gender dysphoria / gender incongruence medical and endocrine pathways are covered in the specialty leaf on gender dysphoria and affirming care. This professional topic covers affirming psychiatry across sexual and gender minorities, including people who never seek gender-affirming medical interventions.[6]
Minority stress model (Meyer)
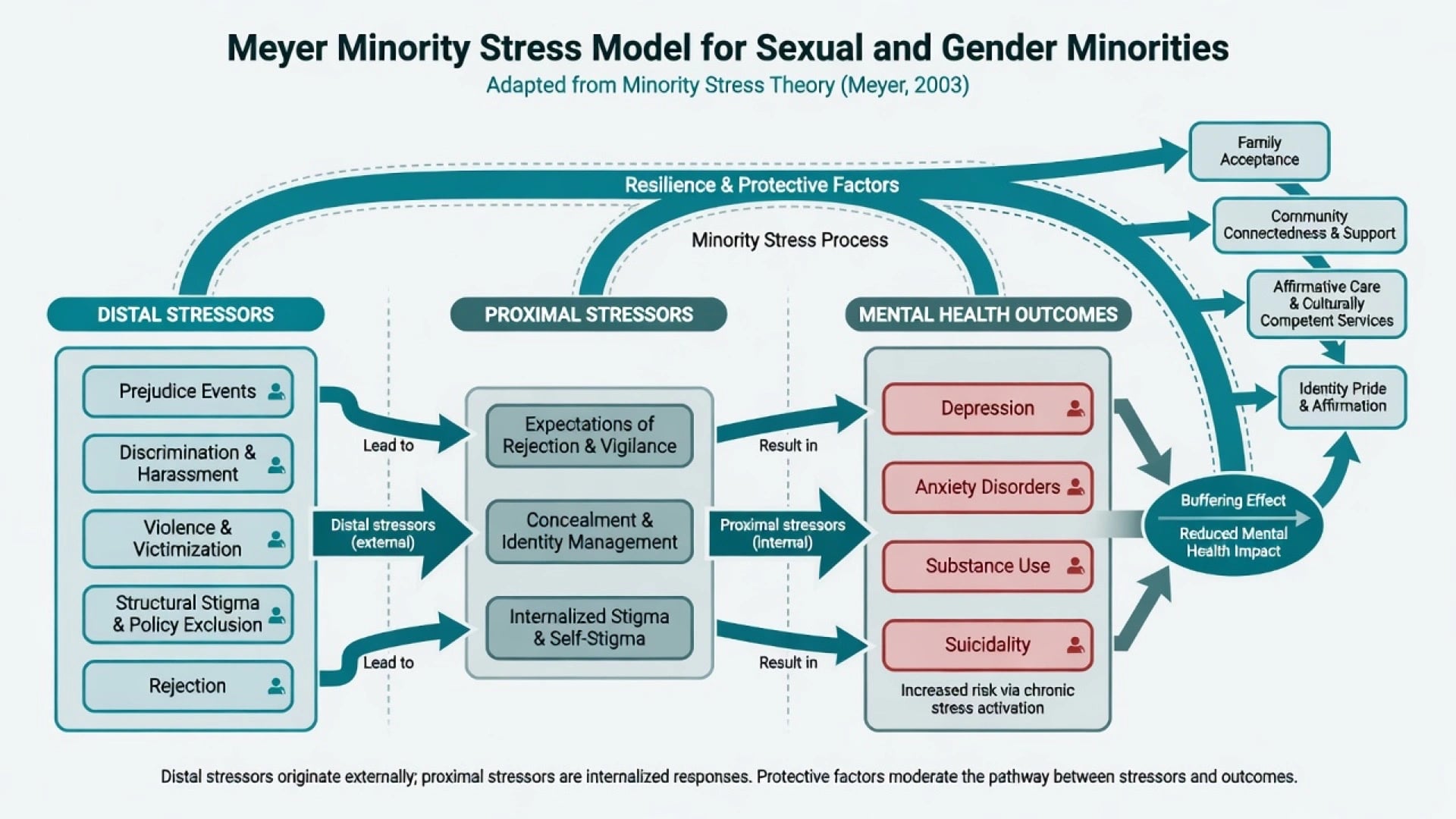
Meyer's minority stress framework is the examiner default for explaining elevated psychiatric morbidity without pathologising identity. Distal stressors include prejudice events, discrimination, violence, and structural stigma. Proximal stressors include expectations of rejection, identity concealment, and internalised stigma. Excess stress is chronic and socially produced, layered on general life stress.[1]
Hatzenbuehler's psychological mediation model links stigma to psychopathology via emotion regulation difficulties, social and interpersonal problems, and cognitive processes — a viva-ready "how does stigma get under the skin" answer.[2]
Conversion practices / SOCE
Sexual orientation change efforts (SOCE) and related conversion practices aim to change sexual orientation or gender identity. They lack a valid clinical indication, conflict with depathologisation, and are associated with adverse mental health and suicidality signals in observational research. Fellows refuse participation and referral, document harm discussions, and redirect to affirming care.[13][14]
Epidemiology and risk
Systematic reviews show elevated rates of depression, anxiety, substance use, self-harm, and suicide-related outcomes in lesbian, gay, and bisexual people compared with heterosexual peers.[3][10] Population analyses by orientation dimensions show mood and anxiety disparities that vary by identity and behaviour measures — bisexual subgroups often show particularly high burden.[9]
In youth, meta-analytic evidence demonstrates higher suicidality and depression in sexual minority versus heterosexual adolescents and young adults.[11] Social-environment and structural factors (for example county-level protective or hostile climates) associate with suicide attempt disparities in LGB youth.[12]
Transgender stigma literature summarises multilevel stigma (structural, interpersonal, individual) as a key driver of health inequities for transgender people.[6] Suicide risk reviews for LGBT populations document elevated attempt rates and call for stigma reduction, access, and affirming clinical responses.[8]
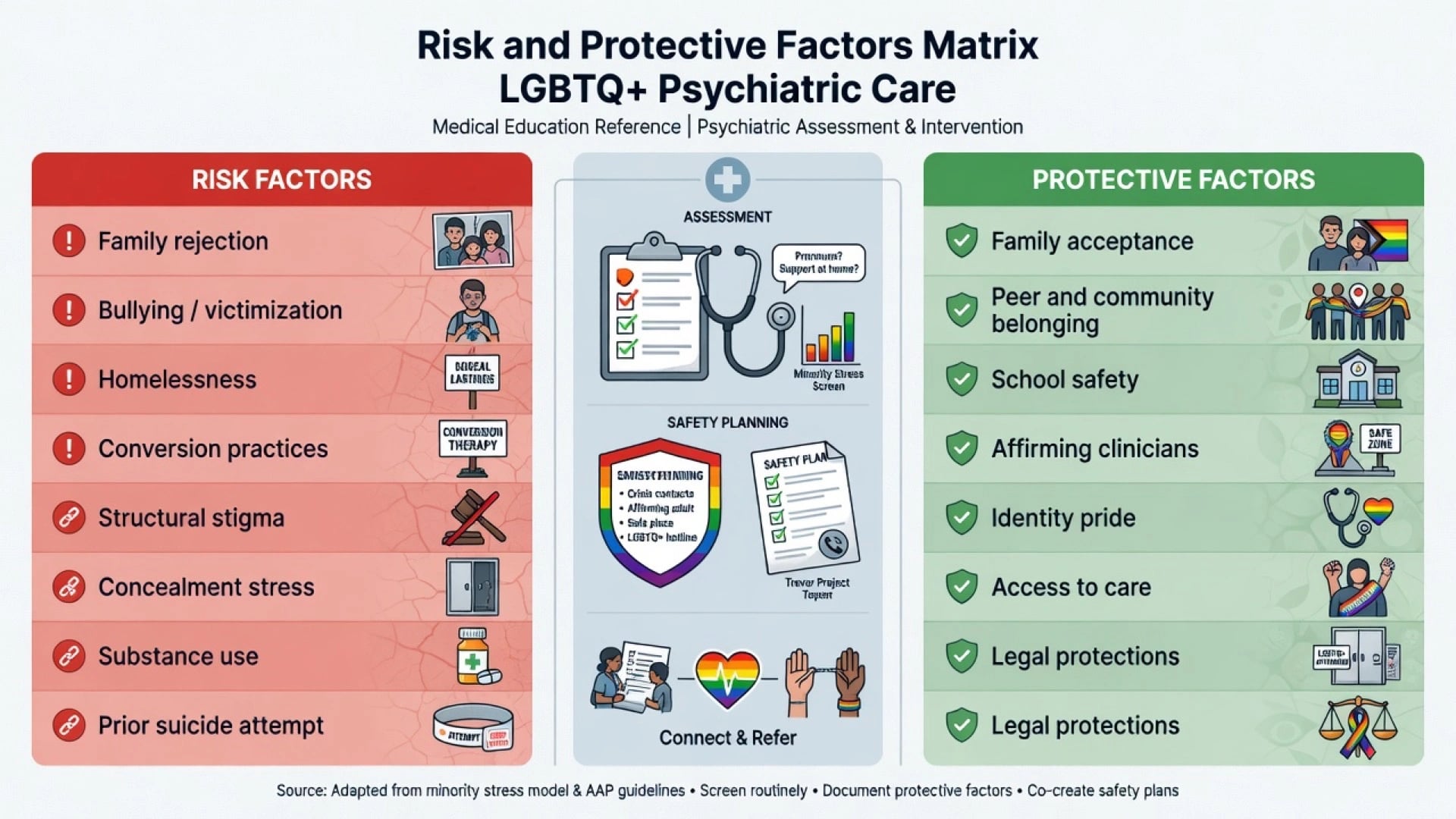
Family rejection predicts multiple negative health outcomes (including suicide attempts, depression, substance use, and risk behaviours) in LGB young adults; family acceptance is associated with better health and wellbeing.[4][5]
Mechanisms
- Distal stressors → acute and chronic threat (victimisation, discrimination, legal inequality).[1]
- Proximal processes → vigilance, concealment costs, internalised stigma, shame.[1][2]
- Mediators → emotion dysregulation, isolation, cognitive patterns that maintain anxiety and depression.[2]
- Structural pathways → policy climate and community stigma shape population suicide attempt rates and resource access.[12]
- Resilience → family acceptance, peer and community connectedness, identity pride, affirmative services buffer risk.[5][6]
Causal framing for exams: stigma and social determinants, not inherent pathology of LGBTQ identities, explain most excess morbidity.[1][3][13]
Clinical presentation
Common stems: adolescent with depression after coming out and parental rejection; young adult with panic and concealment stress at work; bisexual person with mood disorder and erasure from both straight and gay communities; transgender person presenting to general psychiatry with PTSD after assault (not only to a gender clinic); older gay man with late-life depression and historical pathologisation trauma; rural patient delaying care due to confidentiality fears.[4][6][8][11]
MSE may show shame, hypervigilance, or identity-related guilt content that reflects minority stress rather than primary psychotic guilt — always complete a full risk and syndromal assessment.[1][2]
Differential
| Compare | Discriminator |
|---|---|
| Minority stress distress vs major depression / anxiety disorder | Duration, neurovegetative signs, functional loss; both can coexist — treat the syndrome and the stressors |
| Gender dysphoria assessment vs body dysmorphic disorder | Identity congruence focus vs appearance defect preoccupation; specialist formulation when unclear |
| OCD sexual orientation / gender obsessions vs identity exploration | Ego-dystonic intrusive doubt loops with rituals vs authentic identity narrative over time |
| Internalised stigma vs melancholic guilt / psychosis | Stereotype content about LGBTQ identity vs mood-congruent delusions or first-rank symptoms |
| Trauma / PTSD after hate crime vs primary personality disorder labels | Event criterion, re-experiencing, avoidance — avoid pejorative labels for adaptive distrust |
| SOCE-related iatrogenic harm vs "treatment resistance" | History of conversion pressure; repair alliance and stop harmful practices |
Assessment
Inclusive SOGI history
Ask about sexual orientation and gender identity as routine clinical data when relevant to care, privately, without forcing disclosure. Use affirmed name and pronouns; if you err, correct briefly and continue. Do not assume partner gender. Document accurately; avoid pathologising language in notes.[6][8]
Minority stress inventory (bedside)
- Prejudice events, bullying, hate crime, workplace or housing discrimination
- Family rejection or acceptance; religious or cultural conflict
- Concealment and outing threats
- Internalised stigma and shame
- Community supports, chosen family, school or workplace climate
- Prior conversion pressure or SOCE exposure
Risk
Standard suicide and self-harm assessment plus minority-stress amplifiers: recent outing or threat of outing, family violence, homelessness after rejection, bullying, substance use, prior attempts, access to means. Intimate partner violence occurs in same-sex relationships and must not be missed.[8][11][12]
Investigations
There is no laboratory test for sexual orientation or gender identity. Investigate as for the presenting syndrome (metabolic baseline before antidepressants or antipsychotics, ECG when indicated, toxicology, imaging when red flags). Sexual health and HIV/STI risk assessment is behaviour-based, not identity-stereotyped. Screening tools (PHQ-9, GAD-7, structured suicide scales) remain useful when interpreted in context.[3][8]
Acute management
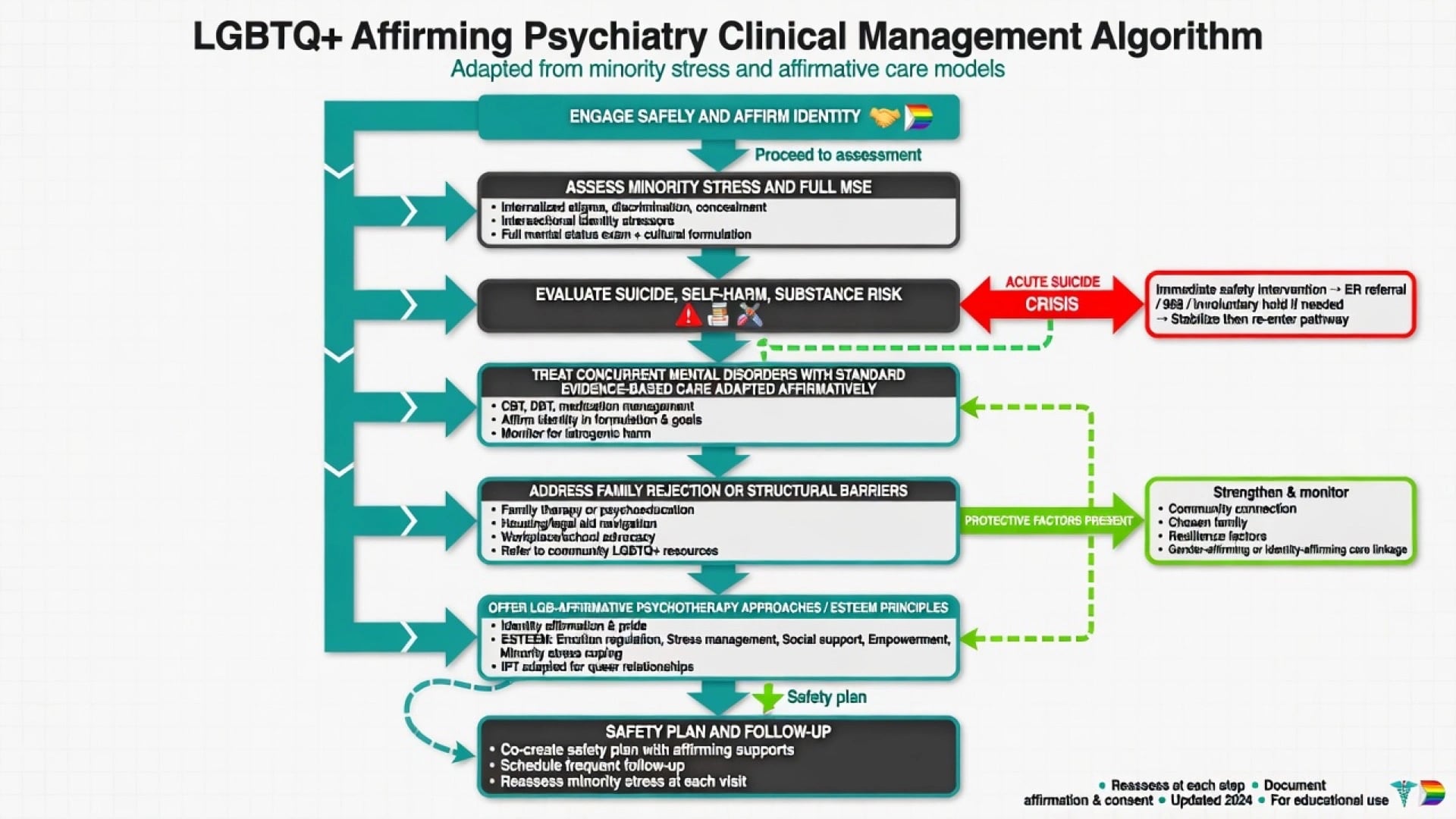
In crisis: standard emergency psychiatry (medical clearance as needed, risk stratification, least restrictive safe disposition) with affirming engagement. Do not frame identity as the problem to eliminate. Protect against forced outing on the ward; ensure respectful rooming and name use. If family demand conversion or threaten violence, prioritise patient safety, refuse collusion, and activate safeguarding pathways as indicated.[8][14]
Definitive management
Principles
- Affirm identity; treat illness. Depression, anxiety, PTSD, bipolar disorder, psychosis, and substance use disorders receive guideline-concordant care.[3][10]
- Formulate minority stress in the biopsychosocial plan (4Ps can include prejudice events as precipitants and concealment as maintaining factors).[1][2]
- Family work aims for acceptance and reduced rejection when safe; family acceptance is a measurable protective factor.[4][5]
- Affirmative psychotherapy. LGB-affirmative CBT targeting minority stress processes improved mental health outcomes in a randomised trial of young adult gay and bisexual men (Pachankis et al.) — the classic exam-named psychotherapy evidence anchor for this topic.[7]
- Social interventions: peer support, LGBTQ community connection, school safety advocacy, housing, legal and workplace supports within professional role limits.[6][12]
- Gender-affirming medical care when indicated: collaborative liaison; see gender dysphoria specialty topic for endocrine and surgical pathway detail.[6]
Pharmacotherapy notes (exam-safe)
Use standard agents at usual doses for the diagnosed syndrome (for example SSRIs for major depression or anxiety disorders per usual titration and monitoring schedules; mood stabilisers or antipsychotics when indicated). Affirming care does not create a parallel formulary. Monitor sexual side-effects carefully because they may interact with identity, relationships, and adherence — discuss openly with shared decision-making.[3][7]
Subtypes and scenarios
- Sexual minorities (LGB+): concealment, bisexual erasure, workplace discrimination, HIV-related dual stigma when relevant.[9][10]
- Transgender and gender diverse people in general psychiatry: stigma-related PTSD, mood disorders, barriers to care; do not reduce all distress to hormones alone or ignore hormones when relevant.[6][8]
- Youth: family rejection/acceptance, school bullying, online harassment, homelessness risk.[4][5][11]
- Older LGBTQ adults: historical criminalisation and pathologisation eras, bereavement, residential care stigma.[13]
- Intersectional ANZ contexts: Aboriginal and Torres Strait Islander LGBTQ people including Sistergirls and Brotherboys; CALD and refugee patients; rural confidentiality constraints — combine with cultural formulation skills without stereotyping.[1][6]
- Religious conflict: explore meaning without anti-religion blanket stance; refuse spiritual abuse and conversion collusion.[14]
Complications and pitfalls
Pitfalls: pathologising identity; conversion referral; outing; repeated misgendering without repair; assuming identity from appearance; over-attributing all symptoms to LGBTQ status; under-treating major syndromes; bisexual erasure; stereotyped HIV assumptions; pejorative notes; colluding with rejecting families against the patient's safety.[4][8][13][14]
Prognosis and disposition
Prognosis improves with reduced rejection, safer social environments, treatment of concurrent disorders, and access to affirmative care.[5][7][12] Disposition follows risk and supports: crisis admission if needed for suicide risk; otherwise community follow-up with affirming clinicians, family work when safe, and social determinants action (housing, school, workplace). Intensity is driven by clinical risk, not identity label.[8][11]
Special populations
Children and adolescents need developmentally appropriate assessment, school safety, and careful capacity and consent processes under local law (do not invent statute numbers). Perinatal LGBTQ parents face dual minority and perinatal risks. Intellectual disability interfaces require supported decision-making and protection from coercion. Rural and small-community care prioritises confidentiality and telehealth access.[5][8][11]
Evidence and guidelines (exam anchors)
| Anchor | Take-home |
|---|---|
| Meyer (2003) | Distal and proximal minority stress |
| Hatzenbuehler (2009, 2011) | Mediation pathways; social environment and youth suicide attempts |
| King (2008); Plöderl and Tremblay (2015) | Systematic evidence of elevated morbidity |
| Marshal (2011) | Youth depression and suicidality meta-analysis |
| Bostwick (2010) | Disparities by orientation dimensions |
| Ryan (2009, 2010) | Family rejection harms; acceptance protects |
| White Hughto (2015) | Transgender stigma multilevel model |
| Haas (2011) | LGBT suicide review and recommendations |
| Pachankis (2015) | LGB-affirmative CBT RCT |
| Drescher (2015) | Depathologisation history |
| Blosnich (2020) | SOCE associated with suicide outcomes |
ANZ: College position statements and public health frameworks increasingly endorse affirmative, non-discriminatory care and oppose conversion practices — learn local professional guidance and any jurisdictional bans separately; do not invent statute text in general exams. UK: GMC and college equality guidance and CASC communication standards emphasise respectful practice. USA: APA practice guidelines for sexual minority and transgender and gender nonconforming people are high-yield; state laws on conversion practices and youth care vary. Global/MD-DNB: criminalisation contexts amplify structural stigma and concealment — formulate safety carefully; still refuse conversion and treat concurrent illness.[6][12][13][14]
Exam pearls
AFFIRM — affirming encounter
Exam pearls: identity is not a disorder; Meyer distal/proximal list wins marks; family rejection vs acceptance is a classic risk/protective pair; name Pachankis RCT for affirmative psychotherapy; Hatzenbuehler for mediation and structural climate; never convert; do not out; treat the depression or anxiety fully; gender medical pathways live mainly on the specialty leaf.[1][2][5][7][13]
Worked micro-formulation (exam style)
Person: 17-year-old bisexual student with two months of major depressive symptoms, insomnia, and passive death wishes after a parent said "fix this or leave home." Conceals identity at school after bullying. No psychotic symptoms. Uses alcohol on weekends to sleep. Precipitant: parental rejection and bullying. Predisposing: minority stress vulnerability, possible family conflict history. Perpetuating: concealment, internalised stigma, insomnia–alcohol cycle, isolation. Protective: one accepting friend, still attending school, help-seeking today. Plan: safety assessment and means restriction; affirm identity and correct name/pronouns; diagnose and treat major depression with usual first-line options and sleep hygiene; address alcohol; family session only if safe, aiming for acceptance education (Ryan evidence); school liaison for bullying; explicit statement against conversion; follow-up and crisis plan; consider affirmative CBT elements targeting rejection sensitivity and shame.[1][4][5][7][11]
References
- [1]Meyer IH Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence Psychol Bull, 2003.PMID 12956539
- [2]Hatzenbuehler ML How does sexual minority stigma "get under the skin"? A psychological mediation framework Psychol Bull, 2009.PMID 19702379
- [3]King M, Semlyen J, Tai SS, et al. A systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay and bisexual people BMC Psychiatry, 2008.PMID 18706118
- [4]Ryan C, Huebner D, Diaz RM, Sanchez J Family rejection as a predictor of negative health outcomes in white and Latino lesbian, gay, and bisexual young adults Pediatrics, 2009.PMID 19117902
- [5]Ryan C, Russell ST, Huebner D, et al. Family acceptance in adolescence and the health of LGBT young adults J Child Adolesc Psychiatr Nurs, 2010.PMID 21073595
- [6]White Hughto JM, Reisner SL, Pachankis JE Transgender stigma and health: A critical review of stigma determinants, mechanisms, and interventions Soc Sci Med, 2015.PMID 26599625
- [7]Pachankis JE, Hatzenbuehler ML, Rendina HJ, et al. LGB-affirmative cognitive-behavioral therapy for young adult gay and bisexual men: A randomized controlled trial of a transdiagnostic minority stress approach J Consult Clin Psychol, 2015.PMID 26147563
- [8]Haas AP, Eliason M, Mays VM, et al. Suicide and suicide risk in lesbian, gay, bisexual, and transgender populations: review and recommendations J Homosex, 2011.PMID 21213174
- [9]Bostwick WB, Boyd CJ, Hughes TL, McCabe SE Dimensions of sexual orientation and the prevalence of mood and anxiety disorders in the United States Am J Public Health, 2010.PMID 19696380
- [10]Plöderl M, Tremblay P Mental health of sexual minorities. A systematic review Int Rev Psychiatry, 2015.PMID 26552495
- [11]Marshal MP, Dietz LJ, Friedman MS, et al. Suicidality and depression disparities between sexual minority and heterosexual youth: a meta-analytic review J Adolesc Health, 2011.PMID 21783042
- [12]Hatzenbuehler ML The social environment and suicide attempts in lesbian, gay, and bisexual youth Pediatrics, 2011.PMID 21502225
- [13]Drescher J Out of DSM: Depathologizing Homosexuality Behav Sci (Basel), 2015.PMID 26690228
- [14]Blosnich JR, Henderson ER, Coulter RWS, et al. Sexual Orientation Change Efforts, Adverse Childhood Experiences, and Suicide Ideation and Attempt Among Sexual Minority Adults in the United States Am J Public Health, 2020.PMID 32437277