Psych · Professional skills — mental state examination
Mental state examination
Also known as MSE · Mental status examination · Psychiatric mental status exam · Descriptive psychopathology interview · Psychiatric interview MSE · CASC mental state
Exam-exhaustive fellowship reference on the Mental State Examination — all core domains (appearance, behaviour, speech, mood, affect, thought form and content, perception, cognition, insight, judgement), documentation standards, worked patterns for psychosis/depression/mania, organic discriminators, cultural caveats, rating-scale adjuncts, and CASC skills. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
The MSE is the psychiatric equivalent of a focused systems examination: a disciplined record of how the person presents now. It sits beside the history (longitudinal story) and formulation (integrative judgment). Domain lists vary slightly across textbooks, but core structure is stable enough for multi-board exams. [1][2]
| What the MSE is | What the MSE is not |
|---|---|
| Cross-sectional clinical description | A diagnosis or ICD/DSM code |
| Mix of observation + structured elicitation | A full psychiatric history |
| Reassessable over hours/days | A permanent trait inventory |
| Feeds risk, capacity-adjacent, and treatment decisions | A legal verdict on its own |
| Compatible with rating scales | Replaced by a single scale score |
Training literature emphasises that MSE skill is teachable with deliberate instructional design (simulation, structured feedback, OSCE/CASC practice) rather than passive observation alone. [2]
Classification of domains
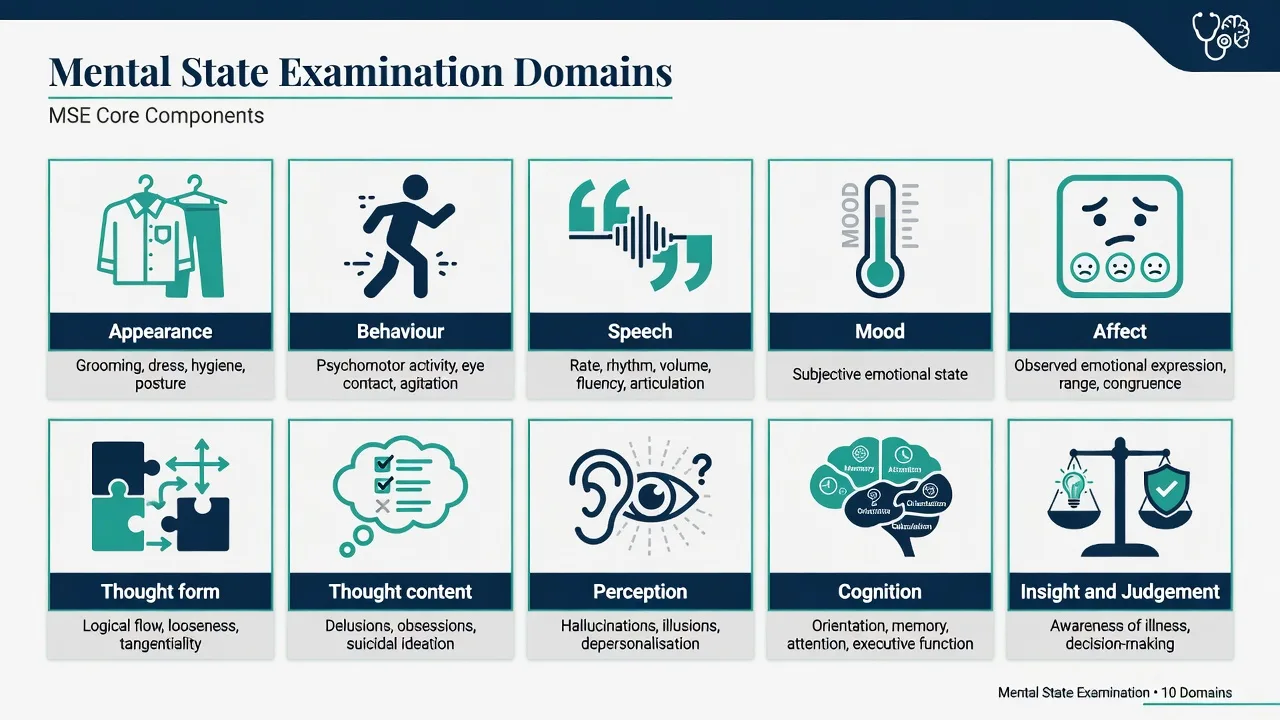
A practical fellowship domain set examiners recognise: [1][2]
- Appearance
- Behaviour / attitude / rapport (motor included)
- Speech
- Mood (subjective)
- Affect (observed)
- Thought form (process)
- Thought content
- Perception
- Cognition
- Insight and judgement[3][4]
Local templates may add risk, level of consciousness, or motivation. Map your hospital proforma to this spine so nothing is skipped under time pressure. [1]
Epidemiology and clinical stakes
MSE quality problems are common educational targets: incomplete domain coverage, pejorative language, and failure to separate observation from inference appear repeatedly in training reviews. [1][2] Incomplete cognition or perception documentation is a classic route to missing delirium or underestimating risk. High-stakes contexts include emergency psychiatry, first-episode psychosis, older adults, CASC stations, and any note that may be read in a tribunal or coronial setting.
Mechanisms and phenomenological basis
MSE vocabulary is descriptive psychopathology: you name the form of experience (e.g. auditory verbal hallucination, derailment) before you explain it. Formal thought disorder terms were operationalised for reliability in Andreasen's Thought, Language, and Communication (TLC) work — definition of terms and reliability, then diagnostic significance across disorders. [3][4]
High-level mechanism anchors (viva depth, not speculative fluff): [1][2]
- Attention/arousal networks — fluctuation and inattention drive the organic MSE signature of delirium.
- Language and associative networks — derailment, tangentiality, neologisms.
- Affective systems — range, reactivity, congruence of observed affect with reported mood.
- Metacognition / self-appraisal — insight dimensions (awareness of illness, relabelling of symptoms, treatment attitude). [5]
Intoxication, metabolic encephalopathy, autoimmune encephalitis, and medication toxicity alter arousal and perception and can mimic primary psychosis — the MSE alone does not prove aetiology, but organic red-flag patterns force investigation. [1][2]
Clinical presentation by domain
Appearance
Describe grooming, hygiene, clothing appropriateness to weather/context, body habitus, scars/tattoos if clinically relevant, apparent age versus chronological age, and any signs of neglect, self-harm, or extrapyramidal side effects. Prefer concrete description over labels ("stained clothing, unwashed hair" not "looks schizophrenic"). [1][2]
Behaviour, attitude, and rapport
Psychomotor activity (agitation, retardation, catatonic features), eye contact, cooperation, hostility, overfamiliarity, distractibility, mannerisms, stereotypies, and ability to establish rapport. Note responses to limit-setting without moralising language. [1][2]
Speech
Rate, rhythm, volume, prosody, latency, spontaneity, dysarthria, mutism, pressure of speech, poverty of speech. Speech is the vehicle through which thought form is inferred — document both. [3][4]
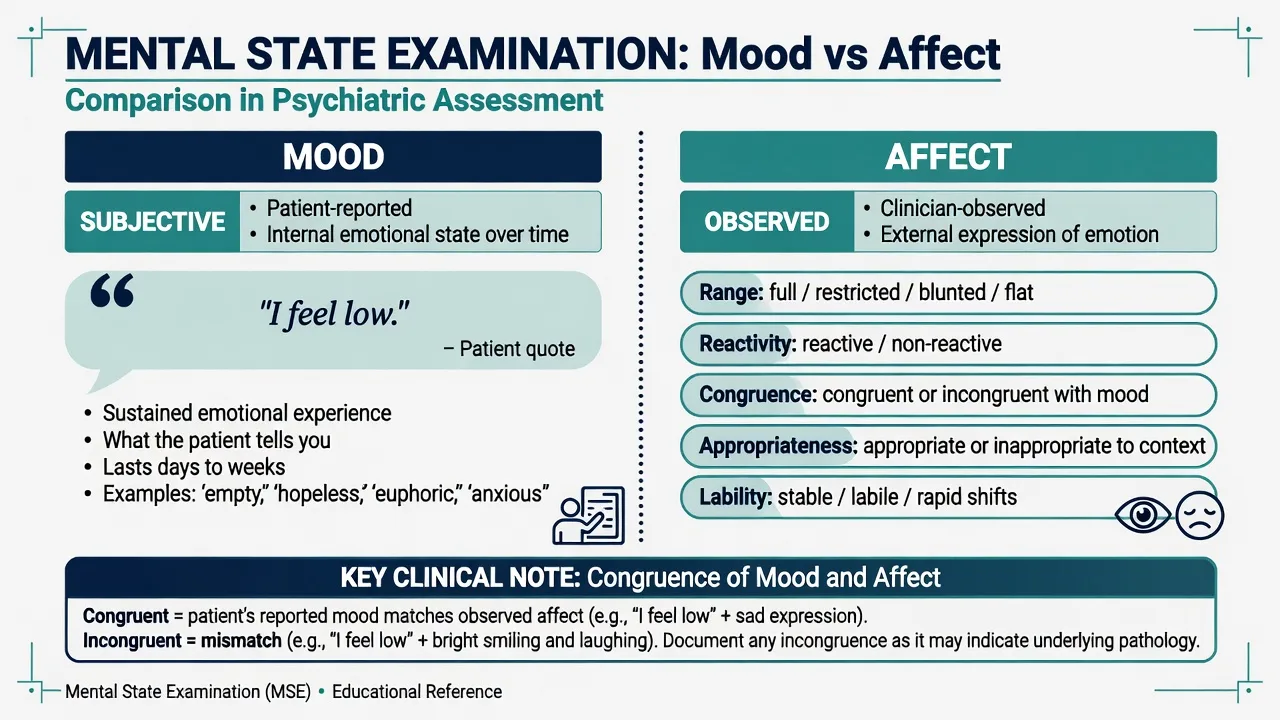
Mood versus affect
Mood is the patient's subjective emotional state (use their words in quotes). Affect is the observed emotional expression: range (full, restricted, blunted, flat), reactivity, appropriateness to context, congruence with stated mood, and lability. [1]
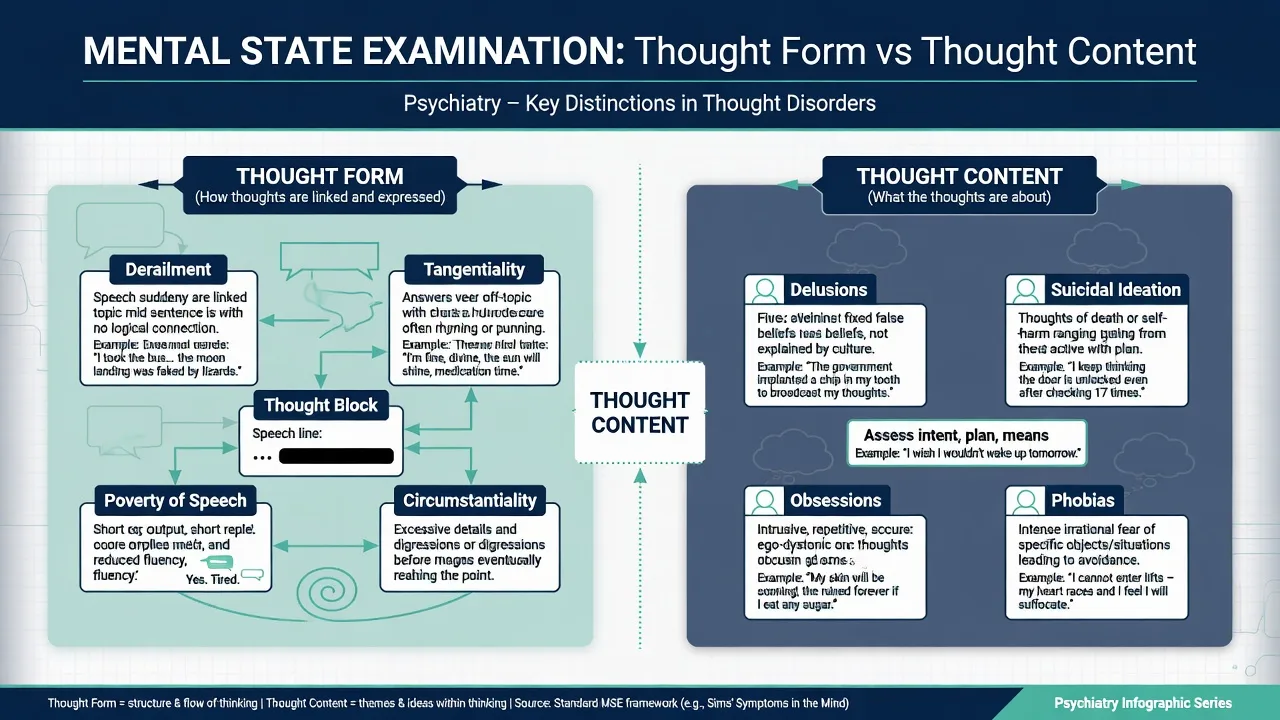
Thought form versus thought content
Form = how thoughts are linked and expressed (circumstantiality, tangentiality, derailment/loose associations, flight of ideas, thought block, poverty of content, neologisms, clang associations, perseveration). Andreasen's TLC framework provides reliable definitions examiners still recognise. [3][4]
Content = what thoughts are about: delusions (persecutory, referential, grandiose, somatic, nihilistic, erotomanic, passivity/control), overvalued ideas, obsessions, ruminations, phobias, suicidal or homicidal ideation, and preoccupations. [16]
| Phenomenon | Core feature | Exam trap |
|---|---|---|
| Delusion | Fixed false belief, not amenable to reason, not explained by culture | Cultural/religious belief mislabelled as delusion |
| Overvalued idea | Emotionally charged belief held with less than delusional conviction | Calling every strong belief a delusion |
| Obsession | Intrusive, ego-dystonic, resisted | Confusing with delusion (insight usually better) |
| Derailment | Topic shifts without logical bridge | Anxious circumstantial speech in non-psychosis |
| Flight of ideas | Rapid associations, often with pressure of speech | Normal quick wit without illness signs |
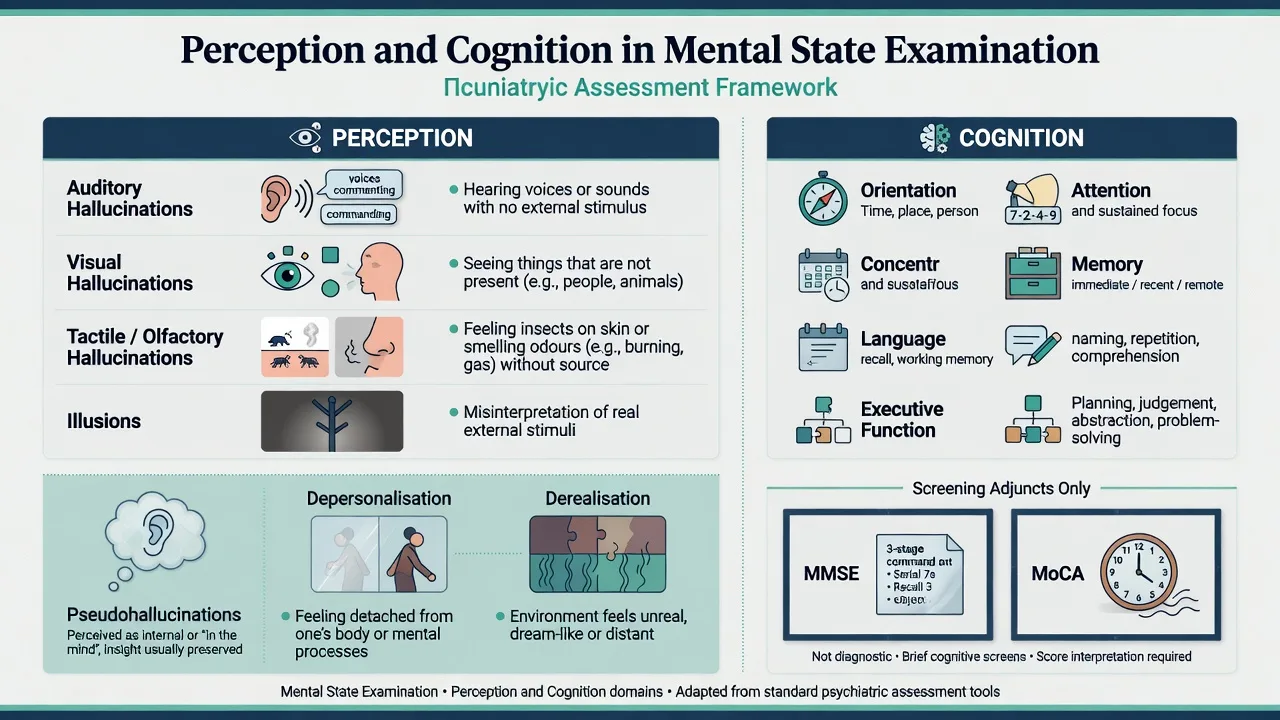
Perception
Hallucinations (modality: auditory, visual, tactile, olfactory, gustatory), illusions, pseudohallucinations, depersonalisation, and derealisation. For auditory verbal hallucinations, record person (second/third), content (including commands), frequency, power, emotional impact, and resistance/acting. Do not lead with "Do you hear voices?" as the only probe — open with unusual sensory experiences, then focus. [1][2]
Schneiderian first-rank symptoms (e.g. thought insertion/broadcast/withdrawal, voices commenting/discussing, passivity phenomena) remain historically important but are not pathognomonic for schizophrenia and lack superior diagnostic validity compared with other psychotic phenomena in modern analyses. [6][7]
Cognition
Level of consciousness/arousal, orientation (time, place, person), attention/concentration, memory (immediate, recent, remote), language, and executive function. Use bedside tests first; formal screens second. [1][2]
- MMSE — practical brief cognitive grading tool; limited for mild cognitive impairment and executive function. [8]
- MoCA — more sensitive for mild impairment; interpret cutoffs carefully (education, culture, hearing/vision); published re-examination of cutoffs warns against rigid single thresholds. [9][10]
Scores never replace a free-text cognitive domain description or a delirium work-up when attention fluctuates. [1][2]
Insight and judgement
Insight is multidimensional. David's model remains the viva standard: (1) awareness of illness, (2) ability to relabel symptoms as pathological, (3) treatment acceptance / compliance attitudes — each may dissociate. [5] Never write only "insight poor."
Judgement is the person's ability to make reasonable decisions in real-world scenarios discussed in interview (e.g. what they would do if they smelled smoke at home). It is related to but not identical with legal decision-making capacity for a specific medical decision. [1][2]
Differential diagnosis using the MSE
| MSE pattern | Favours | Discriminators |
|---|---|---|
| Fluctuating attention, altered arousal, visual hallucinations | Delirium / encephalopathy | Serial MSE, vital signs, organic work-up |
| Stable clear consciousness, auditory hallucinations, systematised delusions | Primary psychosis more likely (still exclude organic) | Onset, drug screen, neuro red flags |
| Pressured speech + flight of ideas + elevated/irritable mood | Mania / mixed | Sleep need history, collateral, YMRS as adjunct |
| Psychomotor retardation + low mood + negative content | Depression | Melancholic features, psychotic depression content |
| Circumstantial speech without derailment | Anxiety, OCD, personality, cultural narrative style | Anxiety signs; no bizarre content |
| Flat affect + social communication difference from early life | Consider autism spectrum contribution | Developmental history, not only cross-section |
Clinical and bedside assessment method
- Set the frame — privacy, safety of room, introductions, purpose, approximate time, permission to take notes.
- Open, then focus — free speech reveals form and content; then domain-specific probes.
- Elicit safely — explore unusual experiences without collusion or mockery; for delusions, understand the belief's function and distress rather than debating truth.
- Screen risk content within thought content (suicide, harm to others, neglect of dependants) using structured approaches when needed (e.g. C-SSRS constructs for ideation intensity). [16]
- Cognition last or mid-interview depending on engagement — do not start with serial sevens if rapport is fragile.
- Insight and judgement near the end when you have enough shared language about symptoms.
- Close — summarise, check understanding, explain next steps.
Instructional design literature supports simulation, structured checklists for feedback, and repeated deliberate practice for MSE competence. [2]
Investigations and scales (adjuncts)
When MSE triggers investigation: first episode; atypical age; rapid fluctuation; fever; seizures; focal neurology; catatonia; new visual hallucinations; severe cognitive change; immunosuppression; substance unknown. [1][2]
Scales do not replace free-text MSE, but examiners expect name recognition: [1][2]
| Scale | Role |
|---|---|
| PANSS | Dimensional positive/negative/general psychopathology in schizophrenia research/clinical trials; structured symptom coverage. [11] |
| YMRS | Mania severity adjunct. [12] |
| HAM-D | Clinician-rated depression severity classic scale. [13] |
| PHQ-9 | Brief depression severity measure; includes suicide item screening utility. [14] |
| GAD-7 | Brief generalised anxiety measure. [15] |
| C-SSRS | Structured suicidal ideation and behaviour severity language. [16] |
| MMSE / MoCA | Cognitive screening adjuncts only. [8][9][10] |
Collateral history is an essential "investigation" of mental state over time when the cross-section is incomplete or disputed. [1][2]
Management interface — resuscitation and safety
MSE findings that change the room immediately: [1][2]
- Active suicidal plan, intent, or rehearsal; access to means.
- Command hallucinations to harm with high perceived power and low resistance.
- Severe agitation with imminent violence risk.
- Delirium with medical instability (airway, hypoxia, sepsis signs). [16]
These trigger environmental safety, senior review, medical stabilisation, and structured risk assessment — the MSE documents the phenomena that feed legal pathways under jurisdiction-specific mental health legislation (do not invent section numbers). Capacity for a specific treatment decision is a separate functional assessment even when MSE insight is poor. [5]
Definitive use — serial MSE and treatment response
Use the same domain structure at each review so change is detectable. Typical early treatment signals: reduced agitation/pressure of speech, quieter perceptual phenomena, improved sleep (history), then slower shifts in delusional conviction and insight. Teaching programmes should give explicit MSE feedback rather than only diagnostic feedback. [2]
Specific scenarios and worked patterns
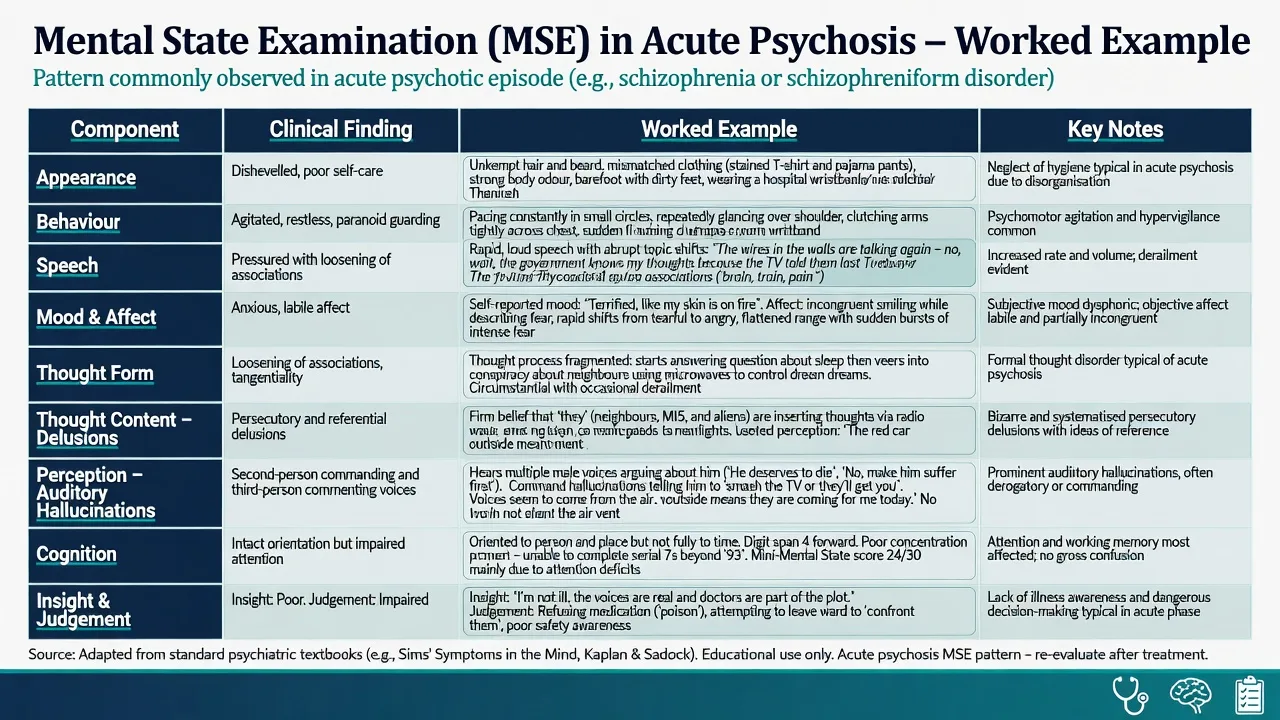
Acute psychosis (worked pattern)
Appearance may show self-neglect; behaviour guarded or agitated; speech pressured or with derailment; mood fearful or perplexed; affect restricted or incongruent; thought form loosened; content persecutory/referential; auditory hallucinations (commenting/commanding); cognition often oriented but attention impaired; insight partial or absent; judgement impaired for safety decisions. [3][4][5]
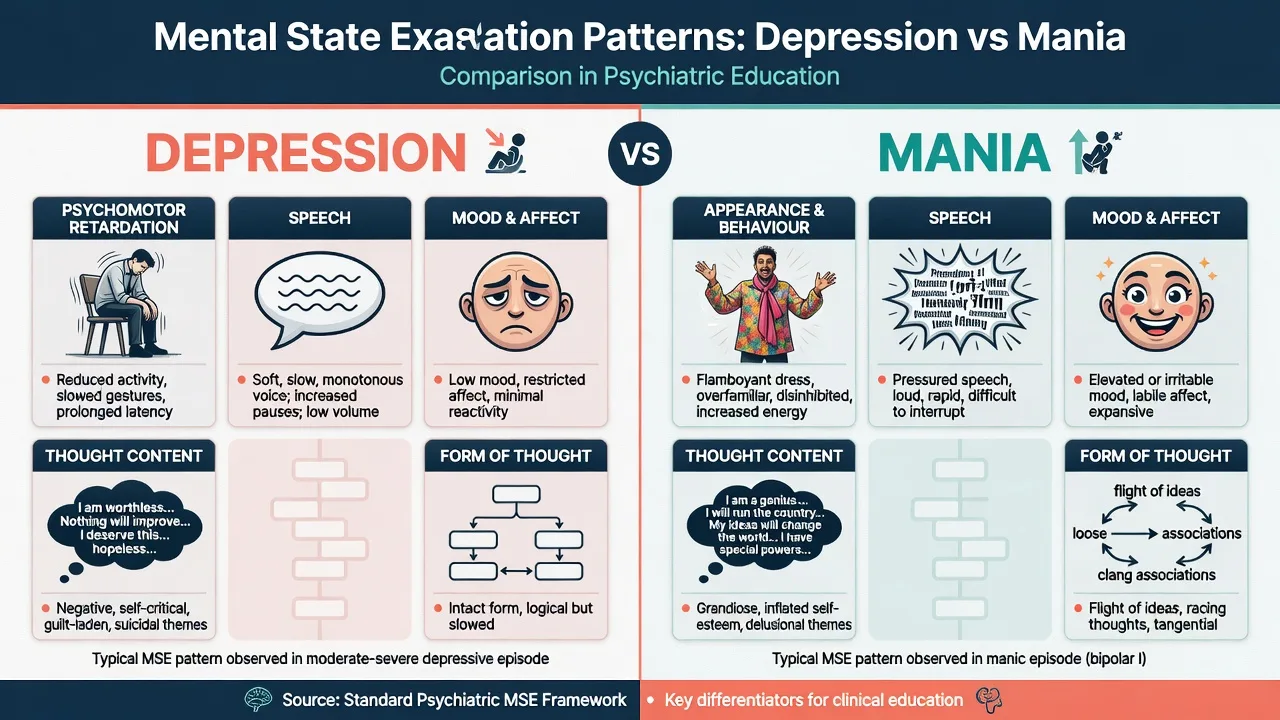
Depression versus mania (contrast)
Depression: psychomotor retardation, soft/slow speech, low mood with restricted affect (usually congruent), negative or suicidal content, form often intact though poverty of speech/content may appear, cognition may show impaired concentration ("pseudodementia" pattern in older adults). [13][14]
Mania: flamboyant or inappropriate dress, overfamiliarity, pressured speech, elevated or irritable mood with expansive or labile affect, flight of ideas, grandiose content, distractible attention, insight often limited into need for treatment. [12]
Delirium versus primary psychosis
Prioritise arousal/attention fluctuation, disorientation, and visual phenomena for delirium. Primary psychosis more often preserves orientation with prominent auditory hallucinations and systematised delusions — but overlap exists; when unsure, investigate and treat reversible causes. [1][2]
Anxiety and OCD
Anxious affect, increased speech rate without true flight of ideas, obsessional content with preserved insight more often than delusion, no true hallucinations. Do not force a psychosis narrative. [5]
Substance intoxication or withdrawal
Document level of consciousness, autonomic signs (history/physical), perceptual phenomena (e.g. formication in stimulant use), and fluctuating cooperation. MSE alone cannot identify the substance. [1][2]
Complications and pitfalls
- Leading questions that create false-positive "voices."
- Colluding with delusions or aggressively arguing them away.
- Pejorative documentation that poisons future care and fails forensic scrutiny.
- Equating poor insight with incapacity or moral failure. [5]
- Missing delirium by never testing attention.
- Over-interpreting a single MMSE/MoCA number. [8][9][10]
- Cultural misreading of eye contact, emotional display, or spiritual experience. [17][18]
- Treating first-rank symptoms as diagnostic gold. [6][7]
- Confusing mood with affect; form with content.
Prognosis and disposition
Serial MSE tracks recovery and relapse. Disposition (home with supports, voluntary admission, compulsory pathway under local law, medical ward for delirium) depends on risk content, cognition, support system, and treatability — always named in the formulation that follows the MSE, not inside the MSE as a legal conclusion. [1][2]
Handover should include a compressed domain summary plus risk bullets so night staff inherit the cross-section accurately. [1][2]
Special populations
| Population | MSE adaptation |
|---|---|
| Children/adolescents | Developmental norms for imagination, suggestibility, emotional display; caregiver collateral essential |
| Older adults | Sensory impairment, delirium risk, MoCA often preferred over MMSE for mild impairment screening; education-adjusted interpretation. [9][10] |
| Intellectual disability | Baseline function; behavioural equivalents of psychosis; avoid diagnostic overshadowing |
| Non-English speakers | Professional interpreter; do not equate limited English or idioms with thought disorder |
| Culturally diverse / Indigenous | Cultural Formulation Interview elements; explanatory models; avoid pathologising cultural practice. [17][18] |
| Perinatal | Mood/content regarding infant safety; shame may suppress suicidal ideation disclosure |
Evidence, guidelines, and regional notes
- Domain teaching and textbook structure — Daza et al. map variability across popular psychiatry textbooks; use a stable local template but know the full examinable set. [1]
- How to teach MSE — Lenouvel et al. scoping review of instructional design strategies for MSE and psychiatric interview. [2]
- Thought disorder reliability — Andreasen TLC I and II. [3][4]
- Insight — David multidimensional model. [5]
- First-rank symptoms — Nordgaard review; Peralta and Cuesta on limited diagnostic specificity. [6][7]
- Cognitive screens — Folstein MMSE; Nasreddine MoCA; Carson cutoff re-examination. [8][9][10]
- Symptom scales — PANSS, YMRS, HAM-D, PHQ-9, GAD-7, C-SSRS. [11][12][13][14][15][16]
- Culture — CFI rationale and OSCE cultural milestones work. [17][18]
ANZ (FRANZCP): Expect precise MSE documentation in clinical notes, WBAs, and OSCE-style assessments; descriptive psychopathology language rewarded; cultural safety expected. [17][18]
UK (MRCPsych CASC): Naturalistic interview skill marks heavily; robotic domain checklists lose rapport marks; still must cover risk, mood, psychosis screen, and cognition when relevant. [2]
US (ABPN): Mental status exam is core interview skill; cognitive screening integration common in older adults; risk documentation standards high. [1][2]
India (MD/DNB, NEET-SS): Classic domain viva; Schneiderian phenomena still asked — answer with historical importance and modern non-pathognomonic status.
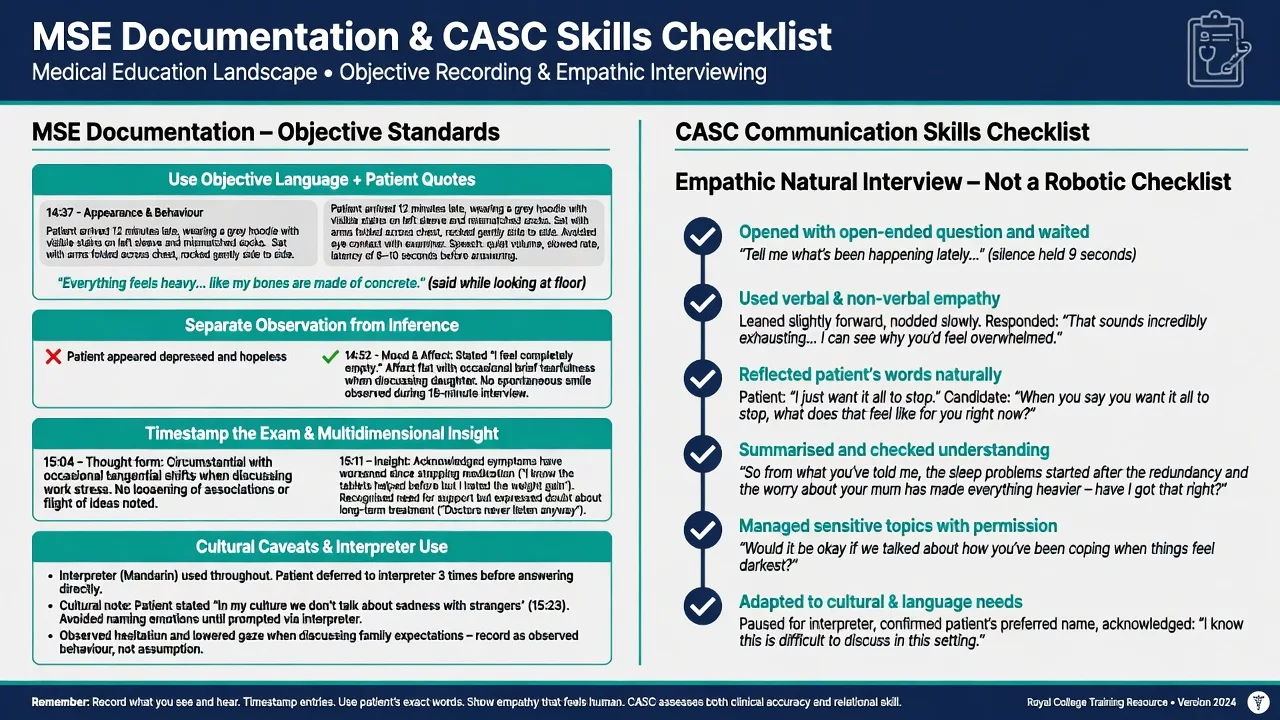
Documentation and CASC skills
Write objective prose with timestamps and quotes. Separate observation ("sat rocking, avoided eye contact") from inference ("appeared anxious"). Record multidimensional insight. Note interpreter use and cultural context without pathologising it. [2][17]
CASC technique: open questions, empathic reflection, permission before sensitive topics, summary checks, and flexible domain coverage woven into conversation — not a checklist read aloud. [2][18]
Exam pearls
- Mood is said; affect is seen — always both.
- Thought form versus content — always both.
- Insight is three dimensions, not good/poor. [5]
- First-rank symptoms are not pathognomonic. [6][7]
- Fluctuation + inattention + visual hallucinations → organic first.
- Scales adjunct, free-text MSE core. [11][12][13]
- CASC rewards empathic structure, not recitation.
- Quote key phrases; timestamp the exam.
- Cultural belief ≠ delusion without formulation. [17]
ASEPTIC — optional memory hook for rapid domain sweep
| Domain pair | Keep distinct |
|---|---|
| Mood / affect | Subjective vs observed |
| Form / content | How vs what of thought |
| Hallucination / illusion | No stimulus vs misperceived real stimulus |
| Insight / capacity | Multidimensional clinical appraisal vs decision-specific legal-functional test |
| MSE / history | Cross-section vs longitudinal narrative |
References
- [1]Daza C, Mauriziano C, Liberona A, et al. Mapping the Mental Status Examination: Insights from a Scoping Review of Popular Psychiatry Textbooks Acad Psychiatry, 2025.PMID 40495096
- [2]Lenouvel E, Chivu C, Mattson J, et al. Instructional Design Strategies for Teaching the Mental Status Examination and Psychiatric Interview: a Scoping Review Acad Psychiatry, 2022.PMID 35318592
- [3]Andreasen NC Thought, language, and communication disorders. I. Clinical assessment, definition of terms, and evaluation of their reliability Arch Gen Psychiatry, 1979.PMID 496551
- [4]Andreasen NC Thought, language, and communication disorders. II. Diagnostic significance Arch Gen Psychiatry, 1979.PMID 496552
- [5]David AS Insight and psychosis Br J Psychiatry, 1990.PMID 2207510
- [6]Nordgaard J, Arnfred SM, Handest P, et al. The diagnostic status of first-rank symptoms Schizophr Bull, 2008.PMID 17562695
- [7]Peralta V, Cuesta MJ Schneider's first-rank symptoms have neither diagnostic value for schizophrenia nor higher clinical validity than other delusions and hallucinations in psychoses Psychol Med, 2023.PMID 32943125
- [8]Folstein MF, Folstein SE, McHugh PR "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician J Psychiatr Res, 1975.PMID 1202204
- [9]Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment J Am Geriatr Soc, 2005.PMID 15817019
- [10]Carson N, Leach L, Murphy KJ A re-examination of Montreal Cognitive Assessment (MoCA) cutoff scores Int J Geriatr Psychiatry, 2018.PMID 28731508
- [11]Kay SR, Fiszbein A, Opler LA The positive and negative syndrome scale (PANSS) for schizophrenia Schizophr Bull, 1987.PMID 3616518
- [12]Young RC, Biggs JT, Ziegler VE, et al. A rating scale for mania: reliability, validity and sensitivity Br J Psychiatry, 1978.PMID 728692
- [13]Hamilton M A rating scale for depression J Neurol Neurosurg Psychiatry, 1960.PMID 14399272
- [14]Kroenke K, Spitzer RL, Williams JB The PHQ-9: validity of a brief depression severity measure J Gen Intern Med, 2001.PMID 11556941
- [15]Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7 Arch Intern Med, 2006.PMID 16717171
- [16]Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults Am J Psychiatry, 2011.PMID 22193671
- [17]Lam PC, Lewis-Fernández R, Aggarwal NK The Cultural Formulation Interview: Building the Case for Cultural Competence in Clinical Care Psychiatr Serv, 2023.PMID 36722093
- [18]Padilla A, Benjamin S, Lewis-Fernandez R Assessing Cultural Psychiatry Milestones Through an Objective Structured Clinical Examination Acad Psychiatry, 2016.PMID 27084719