Psych · Professional — spirituality and religion in psychiatry
Spirituality and religion in psychiatry
Also known as Spirituality in psychiatry · Religion and mental health · Religious coping · Spiritual assessment · HOPE spiritual history · FICA spiritual history · WPA spirituality position statement · Psychoreligious problems · Spiritually significant voices
Exam-exhaustive fellowship reference on spirituality and religion in psychiatric practice: definitions, WPA position, HOPE/FICA assessment, religious coping, distinguishing normative faith experience from psychosis content, chaplaincy, and professional boundaries. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Most patients bring some map of meaning into the clinic — faith, secular philosophy, family ritual, connection to Country, or none of the above. Fellowship exams test whether you can ask without stereotyping, use R/S data clinically, and keep professional boundaries.[1][2]
| Construct | Working definition | Exam trap |
|---|---|---|
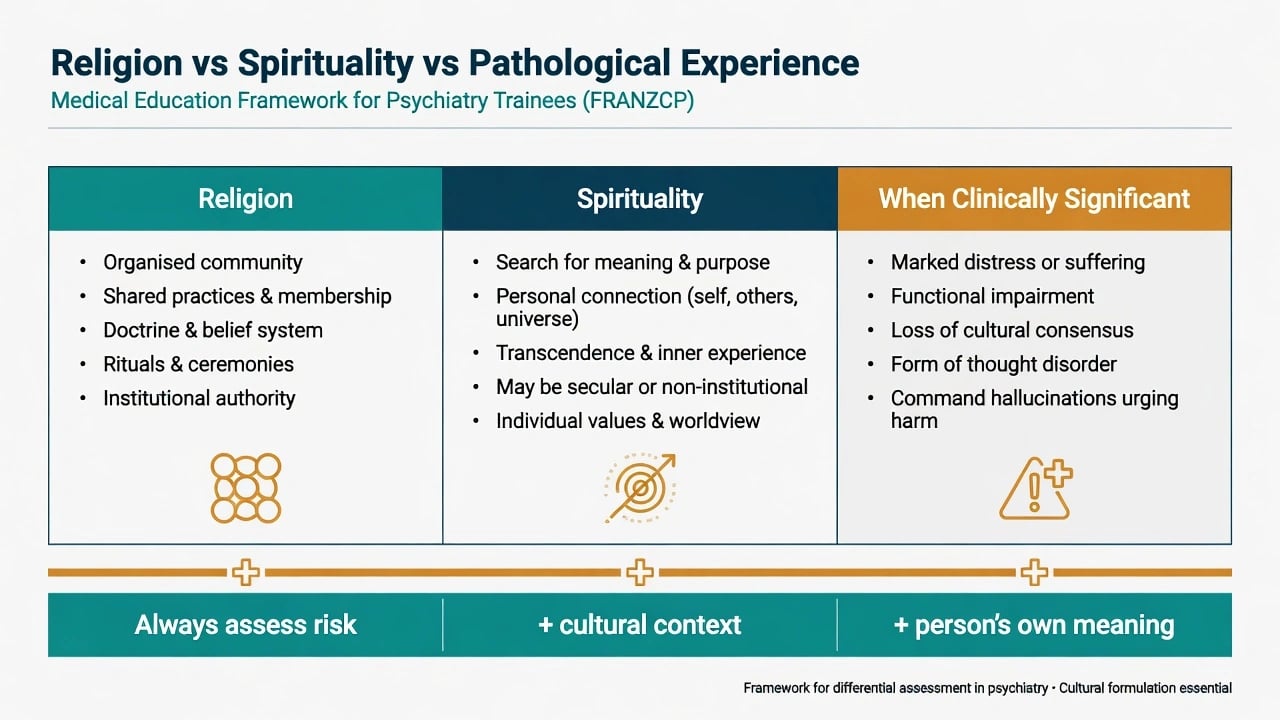
| Spirituality | Meaning, purpose, connection, transcendence; may be non-religious | Equating spirituality only with church attendance |
| Religion | Organised community, doctrine, practices, institutions | Assuming one label predicts all beliefs |
| Religious coping | Using faith resources to manage stress (positive or negative) | Treating all religious talk as protective |
| Spiritual struggle | Conflict with the sacred, community, or meaning that causes distress | Missing it as mere personality or non-compliance |
| Spiritually significant experience | Experience meaningful within a tradition that may not be illness | Automatic diagnosis of psychosis |
The DSM cultural-sensitivity lineage for psychoreligious and psychospiritual problems (Lukoff, Lu, Turner) pushed clinicians to recognise R/S concerns that are not automatically psychopathology — without abolishing the need to diagnose genuine mental illness when criteria are met.[7]
Classification framework
WPA position (viva anchor)
The WPA Position Statement on Spirituality and Religion in Psychiatry holds that R/S are clinically relevant for many people; psychiatrists should take a respectful interest, should not impose their own beliefs, and should be competent to address R/S issues within ethical limits.[1]
Practical clinical reviews translate that stance into: take a brief spiritual history when appropriate, recognise associations between R/S and mental health outcomes, support healthy resources, and collaborate with spiritual care when wanted.[2]
Epidemiology and associations
Population and clinical literatures do not show that religion is always protective. The honest viva answer is bidirectional and moderated.[3][5]
- Meta-analysis of religiousness and depression supports a small main protective association, with moderation under life stress — not a cure claim.[4]
- Systematic review across mental disorders (1990–2010) finds generally favourable or mixed associations of R/S with better outcomes in several domains, while noting methodological limits and negative findings in some contexts.[5]
- Broader synthesis of R/S and health outlines social support, behavioural regulation, and meaning pathways as candidate mechanisms.[3]
- Weber and Pargament summarise clinical roles of R/S, including positive and negative religious coping and spiritual struggle as actionable constructs.[6]
In psychosis services, R/S is common, often under-asked, and can relate to coping and outcome trajectories when assessed carefully.[10][11]
Mechanisms
Protective pathways include social support from faith communities, behavioural norms (reduced substance use in some groups), hope, forgiveness practices, and coherent meaning in adversity.[3][6]
Risk pathways include divine-punishment appraisals, scrupulosity-driven guilt, exclusion or spiritual abuse, alienation after leaving a community, and using faith language to mask suicidality or coercion.[5][6]
In psychosis, attachment to spiritual figures and religious coping style can shape recovery narrative; spirituality and religiousness have been studied as outcome-relevant factors rather than decorative demographics.[11]
Dismissing spiritually significant voices or experiences as worthless noise risks epistemic injustice; the corrective is patient-centred exploration without abandoning psychiatric assessment.[13]
Clinical presentation (exam stems)
Expect stems such as: a devout patient who refuses medication because illness is a spiritual test; religious content in first-episode psychosis; bereavement with crisis of faith; LGBTQIA+ youth rejected by a faith community; older adult for whom chaplaincy is central to end-of-life care; or a trainee asked to pray with a patient.[2][6][12]
MSE language. Record the form of experience (hallucination vs imagery vs prayer dialogue), content, conviction, cultural congruence, affective tone (consoling vs terrifying), and behavioural consequences (including risk).[10][13]
Differential and discriminators
| Pair | Discriminators |
|---|---|
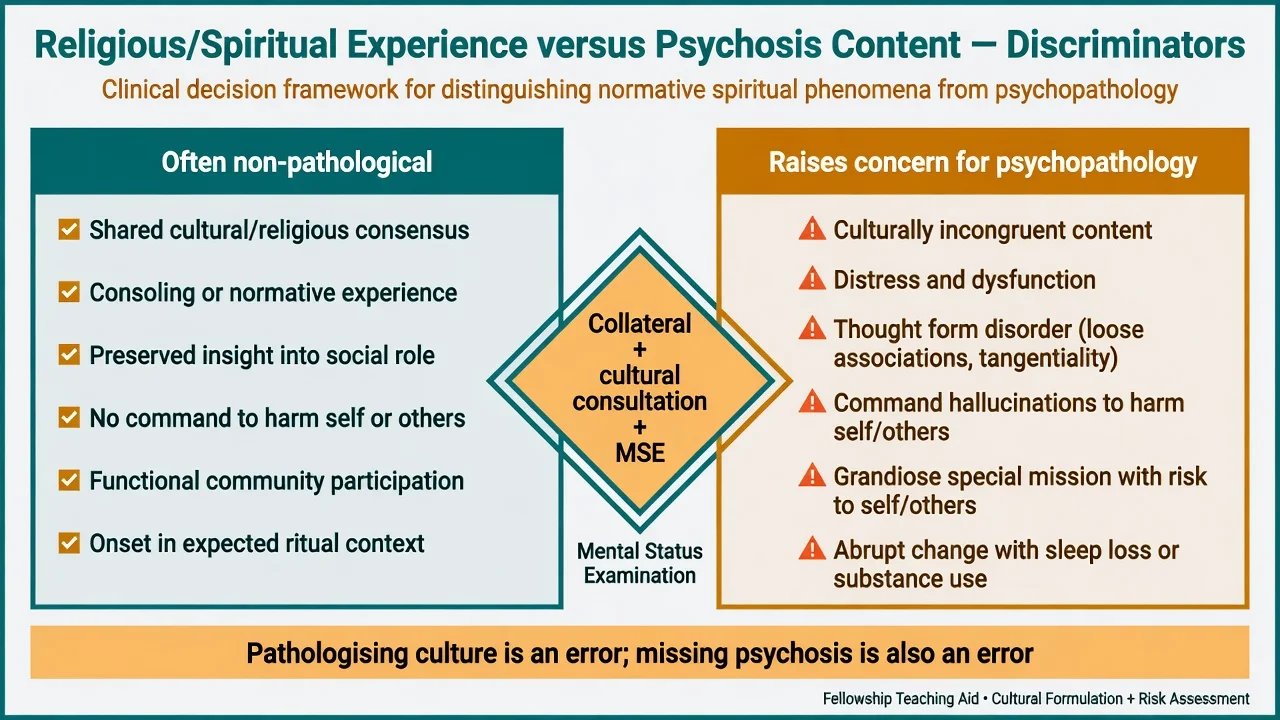
| Normative faith experience vs psychosis | Cultural consensus of community, onset context, thought form, insight into social role, distress/dysfunction, risk commands |
| Spiritual struggle vs major depression | Focus on sacred conflict vs pervasive anhedonia/neurovegetative syndrome; both can co-exist |
| Scrupulosity (OCD) vs devout practice | Ego-dystonic intrusive doubt, neutralizing rituals, time cost, impairment |
| Possession idiom vs dissociative/psychotic state | Local meaning, collateral, MSE, organic screen when indicated |
| Protective community vs coercive control | Freedom to leave, access to medical care, isolation, threats framed as doctrine |
| Spiritual care need vs boundary-seeking | Patient benefit vs clinician specialness, secrecy, dual role |
- Consoling or community-shared
- Preserved function
- Compatible with care
- Patient wants it named
- Can enter recovery plan
- Conflict with sacred or community
- Guilt/shame appraisals
- Withdrawal from supports
- Worsens mood/anxiety
- Needs gentle exploration
- Culturally incongruent or bizarre form
- Thought disorder
- Command harm risk
- Functional collapse
- Needs full psychiatric Rx
Assessment
There is no blood test for spirituality. Assessment is conversational, optional, and person-led.[2][8][9]
HOPE questions
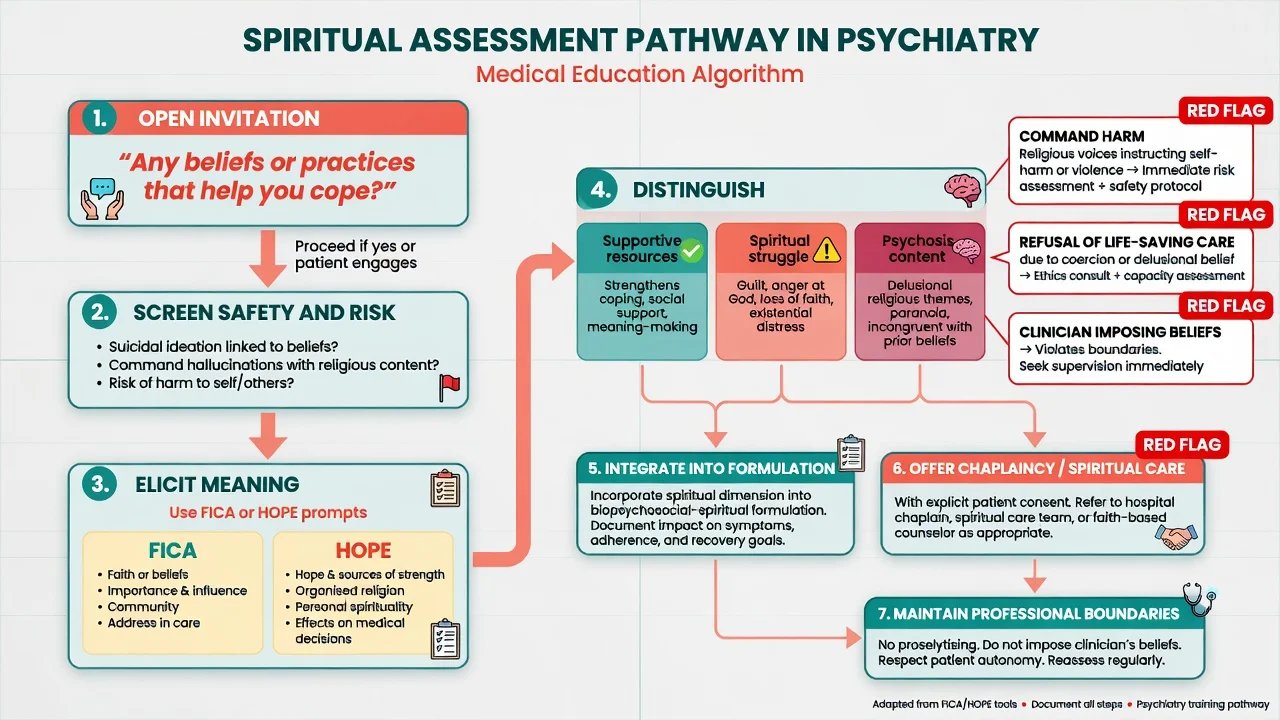
HOPE is a practical bedside framework: H — sources of Hope, meaning, comfort, strength; O — Organised religion; P — Personal spirituality and practices; E — Effects on medical care and end-of-life decisions.[8]
FICA tool
FICA structures a spiritual history: Faith and belief; Importance; Community; Address in care. Evaluation work supports its feasibility for spiritual assessment in clinical settings.[9]
Psychosis-specific assessment
A randomised trial of spiritual assessment for outpatients with schizophrenia found the approach acceptable to patients and useful for clinicians when done respectfully — countering the myth that asking about faith always destabilises psychosis care.[10]
Always complete standard risk assessment (suicide, violence, vulnerability), capacity when treatment is refused, and organic work-up when clinically indicated. R/S assessment supplements, never replaces, those steps.[2][10]
SACRED
Acute management
In crisis, prioritise medical stability and risk first; do not debate theology in the resus bay; use plain language such as "I hear this is spiritually important to you; my job right now is to keep you safe"; and involve preferred supports and, when wanted, spiritual care practitioners.[2][14]
Definitive management and boundaries
Integrate R/S findings into formulation, collaborative goals, and recovery planning when the patient wants them addressed.[1][2]
Offer spiritual care / chaplaincy pathways rather than providing pastoral counselling beyond competence. Australian work describes spiritual care practitioners as contributors within mental health teams when roles are clear.[14]
Medication and psychotherapy remain indicated by diagnosis and guidelines. Negotiate explanatory models (e.g. tablets plus prayer as complementary, not competitive) without ridiculing faith.[2][6]
Professional boundaries
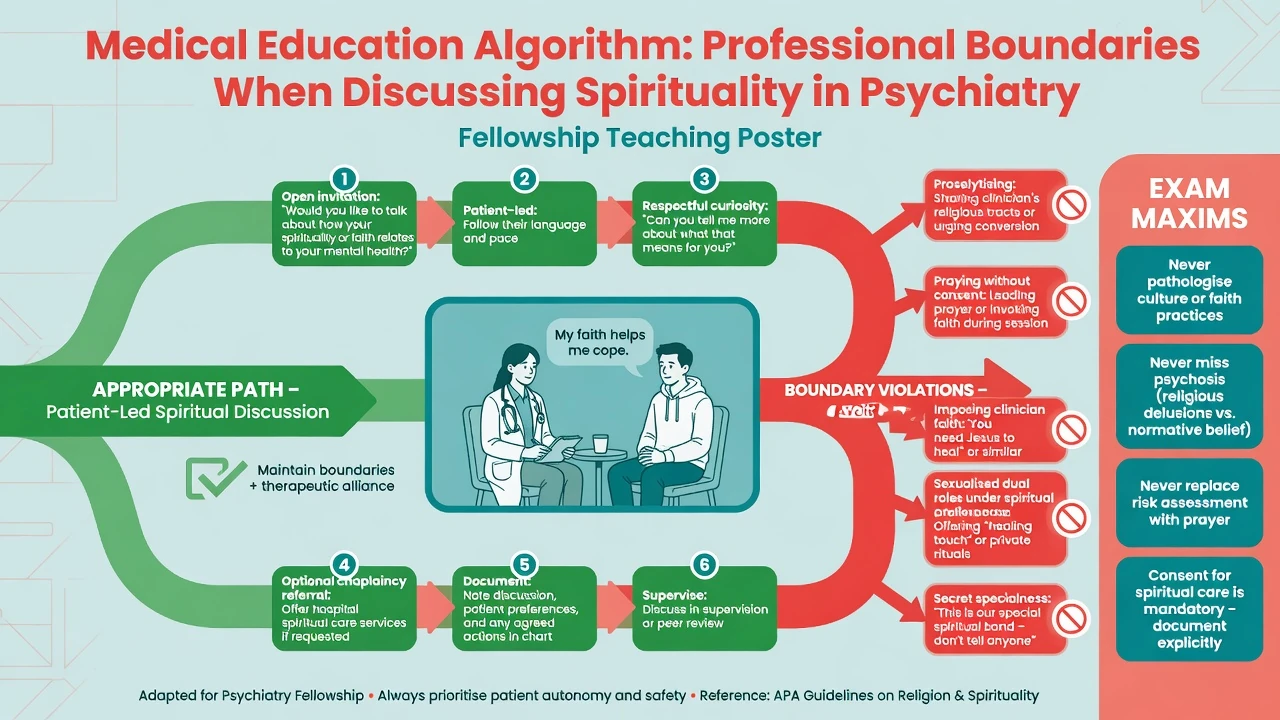
Psychiatrists vary in comfort with R/S topics; mixed-methods work on professional boundaries concerning spirituality and religion underscores the need for clear norms: curiosity is not conversion; self-disclosure of clinician faith is high-risk; prayer with patients requires careful consent and is often best deferred to chaplaincy.[12]
| Allowed / preferred | Avoid |
|---|---|
| Open invitation; patient-led depth | Proselytising or missionising |
| HOPE/FICA-style history | Forcing disclosure |
| Chaplaincy referral with consent | Clinician as dual religious leader for the patient |
| Document meaning in formulation | Secret special spiritual relationship |
| Supervision when countertransference is faith-related | Using spiritual intimacy as slippery slope to other boundary breaches |
Special populations and regional notes
- Older adults: meaning, legacy, and end-of-life spirituality often central; coordinate spiritual care with palliative needs.[2][3]
- Psychosis: ask; do not assume religious content equals religious life or equals illness severity alone.[10][11]
- Indigenous contexts (ANZ): spirituality may sit inside social and emotional wellbeing or wairua frameworks — do not force Christian/Western "religion" templates (link cultural formulation topic).
- Secular patients: meaning and values still matter; atheism is not a deficit.
Prognosis and disposition
Positive religious coping and community support can improve engagement and resilience; negative religious coping and spiritual struggle predict worse distress and need explicit attention.[4][5][6]
In schizophrenia and schizoaffective disorder, spirituality and religiousness have been studied as predictive factors of outcome — individualised assessment beats stereotype.[11]
Disposition plans should name preferred spiritual supports only with consent, alongside standard crisis contacts and clinical follow-up.[2][14]
Evidence and guidelines summary
| Anchor | Why examiners care |
|---|---|
| WPA R/S position statement | Global professional standard: relevance without imposition |
| Moreira-Almeida practical guidelines | Clinical how-to bridge |
| Koenig / Bonelli–Koenig / Smith | Evidence tone: associations, not miracles |
| Weber and Pargament | Coping and struggle vocabulary |
| HOPE / FICA | Bedside tools |
| Huguelet RCT | Spiritual assessment feasible in psychosis |
| Mohr outcome work | R/S can be outcome-relevant |
| Poole and Cook | Boundaries |
| Cullinan et al. | Spiritually significant hallucinations; epistemic justice |
| Malviya and Greenham | Australian spiritual care practitioners |
Exam pearls
[1] [8] [9] [12]References
- [1]Moreira-Almeida A, Sharma A, van Rensburg BJ, et al. WPA Position Statement on Spirituality and Religion in Psychiatry World Psychiatry, 2016.PMID 26833620
- [2]Moreira-Almeida A, Koenig HG, Lucchetti G Clinical implications of spirituality to mental health: review of evidence and practical guidelines Braz J Psychiatry, 2014.PMID 24839090
- [3]Koenig HG Religion, spirituality, and health: the research and clinical implications ISRN Psychiatry, 2012.PMID 23762764
- [4]Smith TB, McCullough ME, Poll J Religiousness and depression: evidence for a main effect and the moderating influence of stressful life events Psychol Bull, 2003.PMID 12848223
- [5]Bonelli RM, Koenig HG Mental disorders, religion and spirituality 1990 to 2010: a systematic evidence-based review J Relig Health, 2013.PMID 23420279
- [6]Weber SR, Pargament KI The role of religion and spirituality in mental health Curr Opin Psychiatry, 2014.PMID 25046080
- [7]Lukoff D, Lu F, Turner R Toward a more culturally sensitive DSM-IV. Psychoreligious and psychospiritual problems J Nerv Ment Dis, 1992.PMID 1431819
- [8]Anandarajah G, Hight E Spirituality and medical practice: using the HOPE questions as a practical tool for spiritual assessment Am Fam Physician, 2001.PMID 11195773
- [9]Borneman T, Ferrell B, Puchalski CM Evaluation of the FICA Tool for Spiritual Assessment J Pain Symptom Manage, 2010.PMID 20619602
- [10]Huguelet P, Mohr S, Betrisey C, et al. A randomized trial of spiritual assessment of outpatients with schizophrenia: patients' and clinicians' experience Psychiatr Serv, 2011.PMID 21209304
- [11]Mohr S, Perroud N, Gillieron C, et al. Spirituality and religiousness as predictive factors of outcome in schizophrenia and schizo-affective disorders Psychiatry Res, 2011.PMID 20869123
- [12]Poole R, Cook CCH, Song R, Robinson CA Psychiatrists' attitudes to professional boundaries concerning spirituality and religion: mixed-methods study BJPsych Open, 2023.PMID 37589193
- [13]Cullinan RJ, Woods A, Barber JMP, Cook CCH Spiritually significant hallucinations: a patient-centred approach to tackle epistemic injustice BJPsych Bull, 2024.PMID 37042321
- [14]Malviya S, Greenham J Exploration of Roles and Contribution of Spiritual Care Practitioners in Mental Health: An Australian Study J Relig Health, 2025.PMID 39862307