Psych · Professional — stigma, recovery and rights-based care
Stigma, recovery and rights-based care
Also known as Mental health stigma · Self-stigma and public stigma · Structural stigma · Personal recovery CHIME · Recovery-oriented practice · Rights-based mental health care · CRPD and psychiatry · Shared decision-making psychiatry · Supported decision-making · Anti-stigma interventions
Exam-exhaustive fellowship topic on mental health stigma (public, self, structural, courtesy), recovery models including CHIME, rights-based care and CRPD principles, shared decision-making, peer support, and anti-stigma strategy evidence. Legal frameworks stated as principles only; jurisdiction-specific statutes not invented. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags

Definition and classification
What stigma is
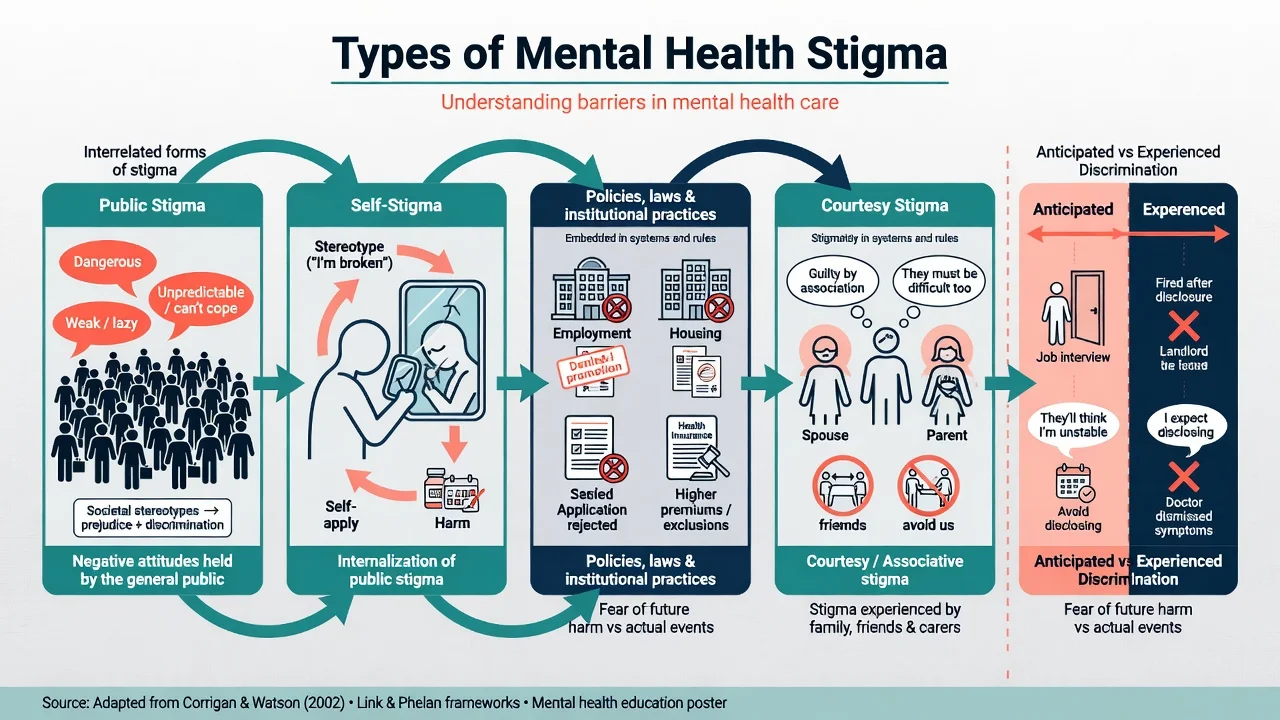
Mental health stigma is not merely "negative attitudes". In social science terms it involves labelling, stereotyping, separation ("us versus them"), status loss, and discrimination, operating when power differentials allow those processes to stick.[2][3]
Corrigan and Watson distinguish public stigma (society's stereotype–prejudice–discrimination pathway) from self-stigma (internalisation of those stereotypes with harm to self-esteem and self-efficacy).[1]
| Type | Core feature | Clinical clue |
|---|---|---|
| Public stigma | Stereotypes (dangerous, weak, incompetent) held by the general public | Avoidance of disclosure; media violence tropes |
| Self-stigma | Awareness → agreement → application of stereotype to self ("why try") | Shame, concealment, lowered goals, identity fusion with diagnosis |
| Structural stigma | Policies and institutional practices that systematically disadvantage | Employment/housing/insurance barriers; coercive defaults; low peer integration |
| Courtesy / associative stigma | Stigma transferred to family, friends, carers | Family isolation; carer shame about "causing" illness |
| Anticipated vs experienced discrimination | Fear of future harm vs actual discriminatory events | Both drive help-seeking delay and social withdrawal |
Recovery constructs
Examiners expect three recovery constructs to be distinguished without creating a false hierarchy: clinical recovery (symptom remission, relapse reduction, often clinician-defined metrics); functional recovery (roles in work, study, relationships, independent living); and personal recovery (living a meaningful life as defined by the person, with or without ongoing symptoms). These three constructs can diverge in the same person and must be named separately in exams.[9][11]
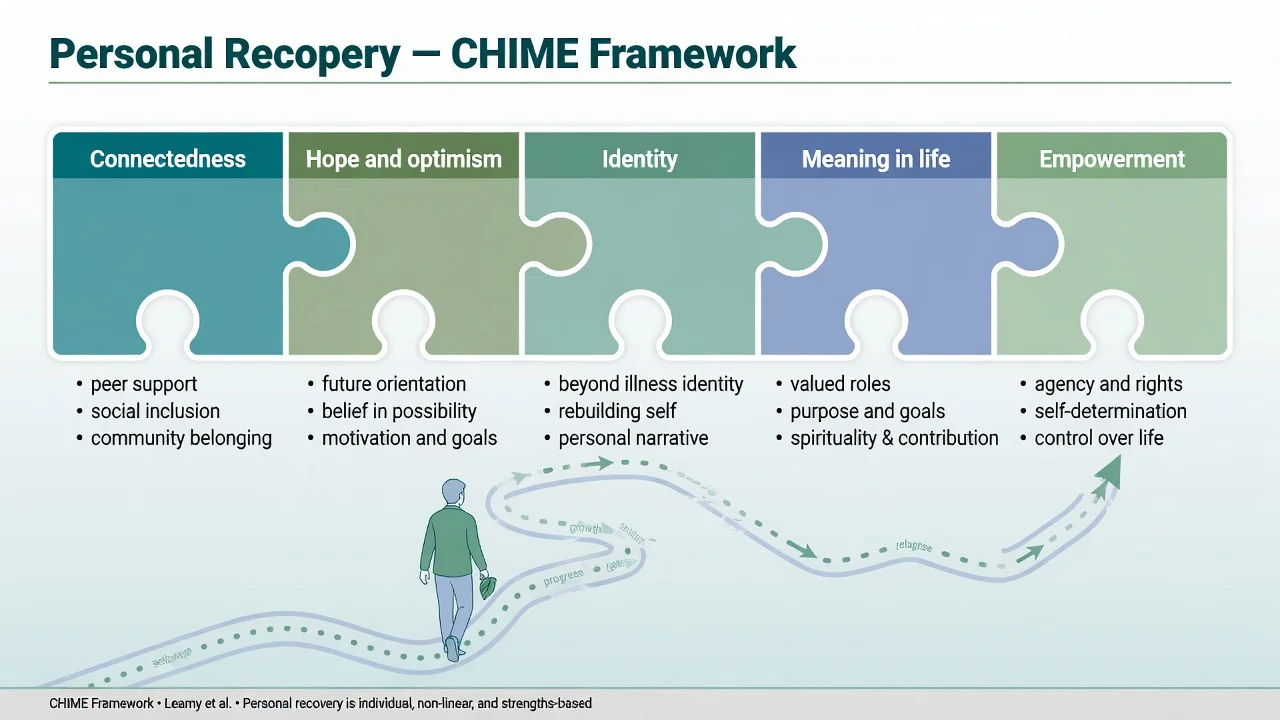
CHIME (Leamy and colleagues) organises personal recovery processes: Connectedness, Hope and optimism, Identity, Meaning in life, Empowerment.[9]
Recovery-oriented practice guidance emphasises hope, partnership, strengths, community inclusion, and meaningful roles — not a single KPI that pressures premature discharge.[10][11]
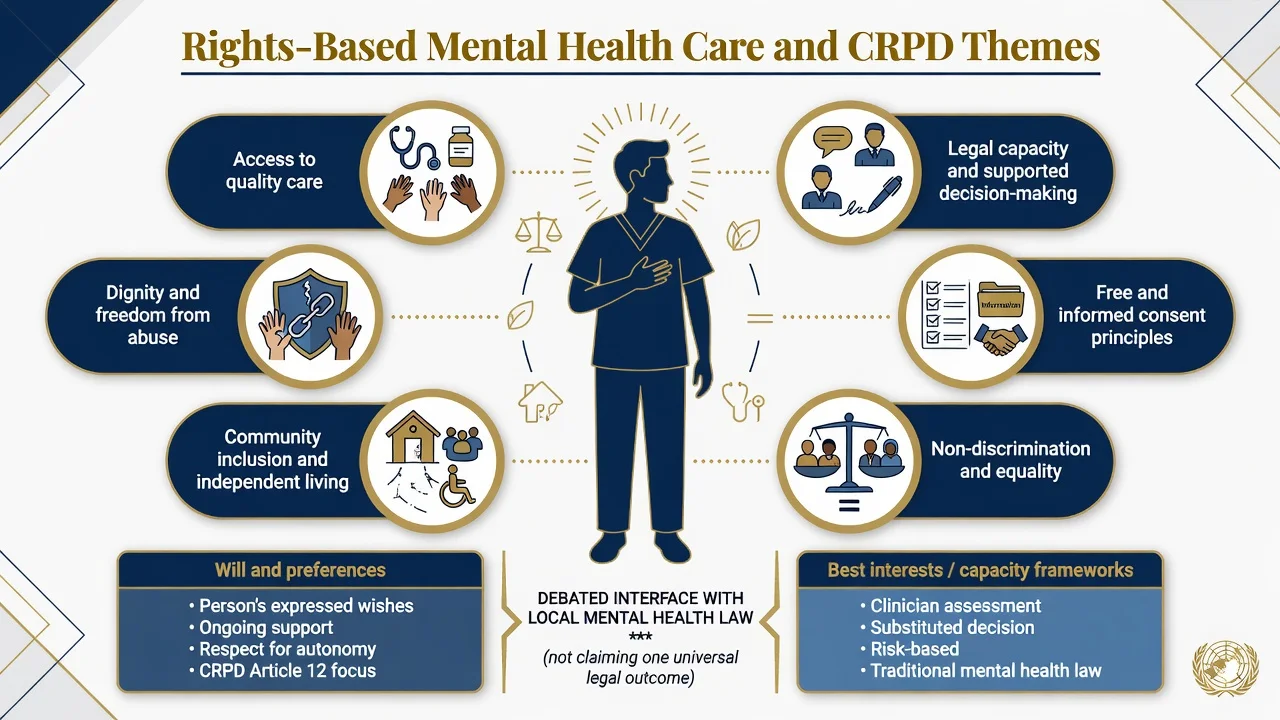
Rights-based care and CRPD themes
Rights-based care operationalises dignity, equality, community living, access to quality care, freedom from abuse, free and informed consent principles, and support for legal capacity. The UN Convention on the Rights of Persons with Disabilities (CRPD) is a major international human-rights instrument; Article 12 debates on legal capacity and supported decision-making are viva staples.[15][16]
Do not invent: that CRPD has a single national incorporation in every jurisdiction; that all involuntary treatment is abolished worldwide; or statute section numbers for Australian/UK/US mental health acts. State principles, name jurisdiction-specificity, and describe the live scholarly debate between will-and-preferences emphasis and capacity/best-interests frameworks.[15][16]
Shared decision-making (SDM)
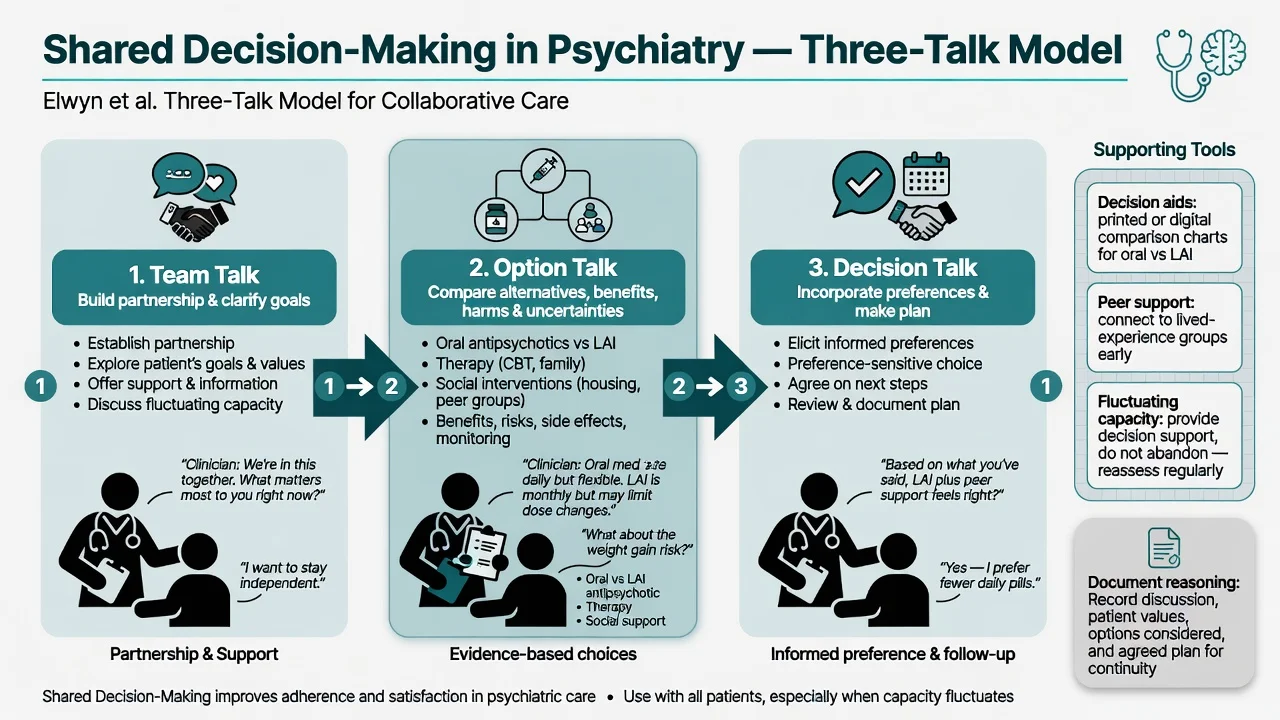
SDM is a collaborative process in which clinician expertise and the person's values/preferences jointly shape the plan. It sits between pure paternalism and pure consumerism. The Elwyn three-talk model is a practical scaffold: team talk (partnership and goals), option talk (alternatives, benefits, harms, uncertainty), decision talk (informed preferences and plan).[13][14]
Epidemiology and consequences
Stigma is common, global, and stubborn. Population surveys show that biogenetic "disease like any other" messaging can reduce blame yet increase desire for social distance for some conditions, especially schizophrenia and alcohol dependence — a critical exam pearl against naive anti-stigma campaigns.[4]
Experienced and anticipated discrimination against people with schizophrenia is widespread across countries (work, relationships, housing, help-seeking).[7] Stigma-related barriers are among the most important reasons for delayed or avoided help-seeking; systematic review evidence links stigma to reduced treatment engagement.[5]
Stigma functions as a fundamental cause of health inequality: it restricts resources (jobs, housing, social capital, quality care) that would otherwise protect health across many pathways.[3]
Mechanisms
Stereotype → prejudice → discrimination
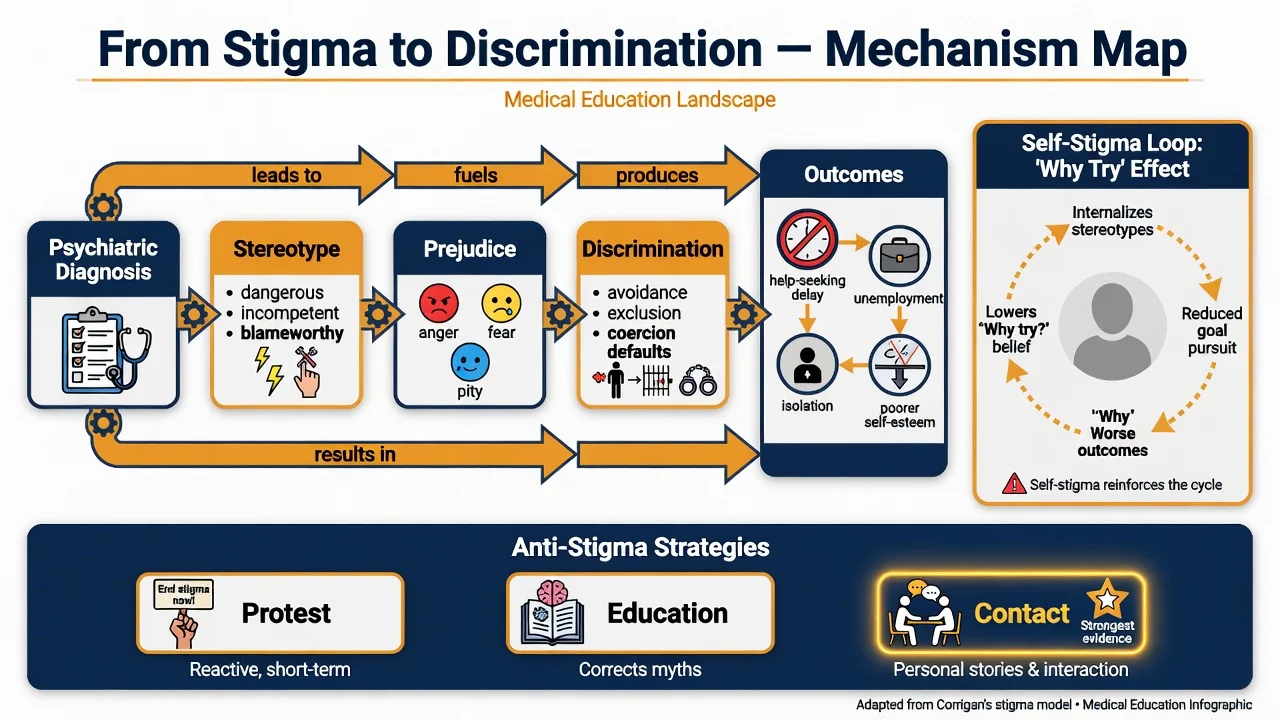
Public stigma operates when a psychiatric label activates stereotypes (dangerousness, incompetence, blameworthiness), emotional responses (fear, anger, pity), and discriminatory behaviours (avoidance, exclusion, coercive defaults).[1][2]
Self-stigma and the "why try" effect
Self-stigma is often staged: awareness of stereotype → agreement that it is true of "people like me" → application to the self → harm (shame, reduced self-efficacy). The why try effect describes reduced goal pursuit because the person expects failure or rejection.[8]
Structural pathways
Structural stigma embeds disadvantage in policy and service design: employment discrimination, insurance exclusions, underfunded community supports, institutional cultures that default to force, and documentation that permanently marks a person as unreliable.[3][7]
Clinical presentation and exam stems
Typical stems and bedside cues include delayed presentation of first-episode psychosis because of shame; refusal of diagnosis language while still wanting help; self-stigmatising MSE content ("I am the illness"); family concealment (courtesy stigma); workplace or housing discrimination after disclosure; clinician pejorative notes and diagnostic overshadowing; ward dignity failures (unexplained seclusion, exclusion from planning); and SDM conflict over long-acting injectable versus oral medication when recovery goals prioritise work.[1][5][7][8]
Rights-based care does not mean ignoring imminent risk of suicide, violence, or severe self-neglect. It means least-restrictive, dignity-preserving, partnership-oriented responses within legal frameworks that apply locally.[11][15]
Differential distinctions examiners test
| Compare | Discriminator |
|---|---|
| Public stigma vs accurate risk communication | Absolute-risk language and individualised assessment vs stereotype of universal dangerousness |
| Self-stigma vs depressive cognitions | Stereotype content about "mental illness" identity vs broader negative self-schema; both can coexist |
| Personal vs clinical recovery targets | Person-defined meaningful life vs CGI/symptom scales alone |
| Will-and-preferences vs best-interests/capacity | CRPD-influenced support for legal capacity vs substituted decision when capacity lacks and law permits |
| SDM vs token choice | Information, time, decision support, and documentation of options vs "sign here" |
| Contact programmes vs fear-based awareness | Lived-experience contact reduces stigma; sensational campaigns can worsen social distance |
Assessment — what to map
There is no laboratory test. Assessment is domain mapping across stigma experiences (public, self, anticipated, structural barriers such as work and housing), person-defined recovery priorities, decision-support needs and fluctuating capacity, intersectional factors (racism, gender, disability, poverty, forensic history, substance-use labels), service climate (peer access, dignity and seclusion metrics), and a documentation audit that rewrites pejorative language into behavioural description.[3][7][8][11]
"Investigations" and service evaluation
For this topic, investigation means mapping, not bloods: person-defined goals and barriers; legal status and rights information (jurisdiction-specific forms — do not invent); access to peer support, recovery education, and employment or education support; decision aids and SDM documentation quality; and restraint or seclusion reduction plus complaints themes as organisational quality signals.[10][11][12][13]
Acute and dignity-first management
In emergency or compulsory contexts, use the least restrictive option consistent with safety and local law; explain what is happening and why; provide rights information at principle level; minimise unnecessary force, seclusion, and public spectacle; avoid weaponised language in crisis notes; and maintain risk assessment — rights-based care is not neglect of imminent harm.[11][15]
Definitive management — multi-level
Individual
- Address self-stigma with psychoeducation, CBT-informed work on shame and identity, and carefully planned disclosure strategies (awareness, agreement, application, harm model).[8]
- Align medication and psychosocial care with person-defined goals (for example, "I want to keep my job" may drive side-effect trade-offs differently from "I want zero voices").[14]
- Offer peer support where available — evidence and experience support peer roles for engagement, hope, and practical navigation, when roles are real rather than token.[12]
Interpersonal and family
Family education should reduce blame without increasing social distance (avoid "genetic doom" messaging alone). Include carers as partners when the person consents, and address courtesy stigma openly.[1][4][6]
Clinical process — shared decision-making
Use team talk / option talk / decision talk; decision aids; explicit discussion of benefits, harms, and uncertainty; document values and agreed plan. SDM remains relevant when capacity fluctuates — provide support, reassess, and do not abandon partnership under partial insight.[13][14]
Service level — recovery-oriented practice
International guidance clusters around hope, partnership, strengths, community inclusion, identity beyond illness, and peer involvement. Implementation requires leadership, workforce development, and measurement beyond bed-days alone.[10][11]
Abuses of recovery to avoid: premature discharge as a "recovery KPI"; denial of medication framed as empowerment; peer workers without supervision, pay equity, or influence; empty slogans without structural change.[11]
Population — anti-stigma strategies
Corrigan's classic triad: protest (challenge harmful messages), education (correct myths), contact (personal interaction with people who have lived experience). Evidence syntheses favour contact-based approaches (often combined with education) over education alone for reducing stigma; long-term and population-level effects vary and campaigns must avoid fear-based content.[1][6]
Rights level
Support decision-making; explain options; involve trusted supporters chosen by the person when appropriate; promote non-discrimination in housing and employment advocacy within professional role limits; and when compulsory care is required under local law use least restrictive means, regular review, dignity, and clear documentation of reasoning — without inventing section numbers in the exam answer.[15][16]
Subtypes and scenarios
High-yield scenarios include first-episode psychosis (identity and self-stigma; early partnership and peer contact); media violence stereotyping (absolute-risk myths without abandoning individual risk assessment); structural stigma in insurance, employment, immigration, and custody; inpatient dignity and coercive-default reduction; forensic double stigma; clinician stigma toward substance use and personality disorder labels; Indigenous and culturally diverse recovery frames (for example social and emotional wellbeing — link cultural formulation topic, do not essentialise); and older-adult therapeutic nihilism as structural stigma.[7][8][11][12]
Complications and pitfalls
Pitfalls include treating recovery as a managerial KPI that pressures unsafe early discharge; using recovery rhetoric to withhold evidence-based care; biogenetic messaging that increases social distance; token peer roles without power or pay equity; claiming CRPD abolished all involuntary treatment as universal settled law (contested interpretation; local law still applies); coaching only coping with stigma while ignoring discrimination and structural reform; and pejorative documentation that becomes a permanent barrier.[4][11][12][15][16]
Prognosis and disposition
Personal recovery is non-linear. Hope, connectedness, and valued roles predict better trajectories beyond symptoms alone.[9][11] Disposition planning should include housing, education/employment supports, continuity of trusted relationships, peer contact, and a crisis plan that preserves dignity. Population stigma changes slowly; service-level dignity practices are immediately actionable.[6][7]
Special populations
Special populations include youth (identity, self-stigma, school disclosure); perinatal care (mothering competence stereotypes with careful risk and support balance); older adults (ageism plus mental illness stigma); intellectual disability and autism interfaces (diagnostic overshadowing and dual stigma); forensic pathways (public fear and reintegration barriers); and Indigenous ANZ contexts (culturally grounded recovery concepts and racism as structural stigma — see cultural formulation topic).[3][7][8][11]
Evidence and guidelines (exam anchors)
| Anchor | Take-home |
|---|---|
| Corrigan and Watson (2002) | Public vs self-stigma; stereotype–prejudice–discrimination |
| Rüsch et al. (2005) | Concepts, consequences, multi-level initiatives |
| Hatzenbuehler et al. (2013) | Stigma as fundamental cause of health inequality |
| Pescosolido et al. (2010) | "Disease like any other" can increase social distance |
| Clement et al. (2015) | Stigma impedes help-seeking |
| Thornicroft et al. (2009, 2016) | Global discrimination; contact-favouring intervention evidence |
| Leamy CHIME (2011); Le Boutillier (2011); Slade (2014) | Personal recovery framework; practice guidance; uses/abuses |
| Davidson peer support (2012) | Peer support evidence and experience |
| Elwyn three-talk (2012); Deegan and Drake (2006) | SDM process; medication decisions in recovery |
| Szmukler et al. (2014); Freeman et al. (2015) | CRPD/MH law interface and Article 12 debate |
ANZ: recovery-oriented practice expectations are embedded in many public mental health service frameworks; mental health acts and compulsory treatment rules are state/territory- or NZ-specific — learn local law separately; do not invent sections in a general exam answer. UK: recovery colleges and rights-focused advocacy are prominent; MHA frameworks are jurisdiction-specific. USA: SDM and peer-support movements are strong; ADA/disability rights interfaces matter; state civil commitment law varies. Global/MD-DNB: human-rights language is increasingly examined; local statutes and resource constraints shape what is feasible — state principles and least-restrictive care.[10][11][13][15]
Exam pearls
CHIME — personal recovery
Exam pearls: name stigma type plus mechanism plus intervention level in any stem; clinical recovery is not identical to personal recovery and both matter; contact is stronger than education alone for stigma reduction evidence synthesis; SDM is process (three talks), not a form; CRPD requires will-and-preferences language and legal capacity debate without inventing universal abolition of compulsory care; least restrictive practice, dignity, partnership, and documented reasoning win CASC/MEQ marks; avoid pejorative labels in notes and write behaviourally.[6][9][11][13][15][16]
Worked micro-formulation (exam style)
Person: 24-year-old with first-episode psychosis, delayed help-seeking for 10 months because of shame; family conceals diagnosis; declines LAI due to fear of "looking like a mental patient"; wants to return to apprenticeship. Stigma map: public (anticipated workplace discrimination), self ("I am dangerous/broken"), structural (possible workplace disclosure risk), courtesy (family concealment). Recovery goals (CHIME): reconnect with friends and trade school (C); belief that apprenticeship is possible (H); identity as apprentice not only "schizophrenia patient" (I); valued work role (M); choice about formulation and medication route (E). Plan: SDM three-talk for oral vs LAI with side-effect and lifestyle trade-offs; peer contact if available; family education that reduces blame without fear messaging; behavioural documentation; rights explanation if any compulsory pathway is considered under local law; employment support with carefully planned disclosure strategy.[8][9][12][13][14]
References
- [1]Corrigan PW, Watson AC Understanding the impact of stigma on people with mental illness World Psychiatry, 2002.PMID 16946807
- [2]Rüsch N, Angermeyer MC, Corrigan PW Mental illness stigma: concepts, consequences, and initiatives to reduce stigma Eur Psychiatry, 2005.PMID 16171984
- [3]Hatzenbuehler ML, Phelan JC, Link BG Stigma as a fundamental cause of population health inequalities Am J Public Health, 2013.PMID 23488505
- [4]Pescosolido BA, Martin JK, Long JS, et al. "A disease like any other"? A decade of change in public reactions to schizophrenia, depression, and alcohol dependence Am J Psychiatry, 2010.PMID 20843872
- [5]Clement S, Schauman O, Graham T, et al. What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies Psychol Med, 2015.PMID 24569086
- [6]Thornicroft G, Mehta N, Clement S, et al. Evidence for effective interventions to reduce mental-health-related stigma and discrimination Lancet, 2016.PMID 26410341
- [7]Thornicroft G, Brohan E, Rose D, et al. Global pattern of experienced and anticipated discrimination against people with schizophrenia: a cross-sectional survey Lancet, 2009.PMID 19162314
- [8]Corrigan PW, Rao D On the self-stigma of mental illness: stages, disclosure, and strategies for change Can J Psychiatry, 2012.PMID 22854028
- [9]Leamy M, Bird V, Le Boutillier C, et al. Conceptual framework for personal recovery in mental health: systematic review and narrative synthesis Br J Psychiatry, 2011.PMID 22130746
- [10]Le Boutillier C, Leamy M, Bird VJ, et al. What does recovery mean in practice? A qualitative analysis of international recovery-oriented practice guidance Psychiatr Serv, 2011.PMID 22193795
- [11]Slade M, Amering M, Farkas M, et al. Uses and abuses of recovery: implementing recovery-oriented practices in mental health systems World Psychiatry, 2014.PMID 24497237
- [12]Davidson L, Bellamy C, Guy K, et al. Peer support among persons with severe mental illnesses: a review of evidence and experience World Psychiatry, 2012.PMID 22654945
- [13]Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice J Gen Intern Med, 2012.PMID 22618581
- [14]Deegan PE, Drake RE Shared decision making and medication management in the recovery process Psychiatr Serv, 2006.PMID 17085613
- [15]Szmukler G, Daw R, Callard F Mental health law and the UN Convention on the rights of Persons with Disabilities Int J Law Psychiatry, 2014.PMID 24280316
- [16]Freeman MC, Kolappa K, de Almeida JM, et al. Reversing hard won victories in the name of human rights: a critique of the General Comment on Article 12 of the UN Convention on the Rights of Persons with Disabilities Lancet Psychiatry, 2015.PMID 26236004