Psych · Professional — teaching and supervision skills
Teaching and supervision skills for psychiatrists
Also known as Clinical supervision · Educational supervision · Clinical teaching · Workplace-based assessment · Feedback skills · One-minute preceptor · Trainee remediation · Faculty development · Miller pyramid · R2C2 feedback
Exam-exhaustive fellowship reference on teaching and supervision for psychiatrists: definitions of educational vs clinical vs managerial supervision, Proctor-style functions, Miller pyramid and CBME/WBA, one-minute preceptor microskills, feedback models (Ende, R2C2, Teaching on the run), deliberate practice, underperforming trainee and failure-to-fail, remediation, educational alliance, faculty development, and regional training frameworks. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Psychiatrists teach and supervise medical students, junior doctors, registrars, allied colleagues, and peers. Fellowship exams test this domain because consultants design rotations, complete workplace-based assessments (WBA), deliver critical feedback, remediate underperformance, and model professional culture. Supervision quality is variable in time, place, and effectiveness unless deliberately organised.[1][2]
Clinical teaching is the intentional facilitation of learning in real clinical settings (bedside, ward round, clinic, emergency). Educational supervision supports a trainee’s longitudinal curriculum progress, goal setting, and appraisal. Clinical (case) supervision focuses on formulation, risk, countertransference, and care decisions for specific patients. Managerial / line management addresses roster, service delivery, and employment standards — related but not identical to educational roles. Conflating these without naming the hat you are wearing confuses trainees and examiners alike.[1][2]
Formative assessment is for learning (feedback, coaching). Summative assessment is for progression decisions. High-quality programmes separate the purposes while ensuring formative data do not leave a trainee shocked at a summative gate.[4][5]
A useful organising triad for supervision functions (widely taught as Proctor-style roles) is normative (standards, patient safety, professional boundaries), formative (skill and knowledge development), and restorative (emotional support, wellbeing, sustainable practice). Effective supervisors flex across all three rather than only “being nice” or only “policing.”[1][2]
| Role | Primary aim | Typical activities |
|---|---|---|
| Clinical teacher | Skill acquisition in the moment | One-minute preceptor, bedside teaching, case discussion |
| Educational supervisor | Curriculum progress and outcomes | Learning plans, WBA review, mid/end-term appraisal |
| Clinical case supervisor | Safe, reflective care of patients | Formulation, risk, ethics, countertransference |
| Line manager | Service and employment standards | Roster, leave, conduct under employment framework |
| Mentor / coach | Career and growth (often non-assessing) | Career advice, sponsorship, reflective coaching |
Classification — frameworks examiners expect
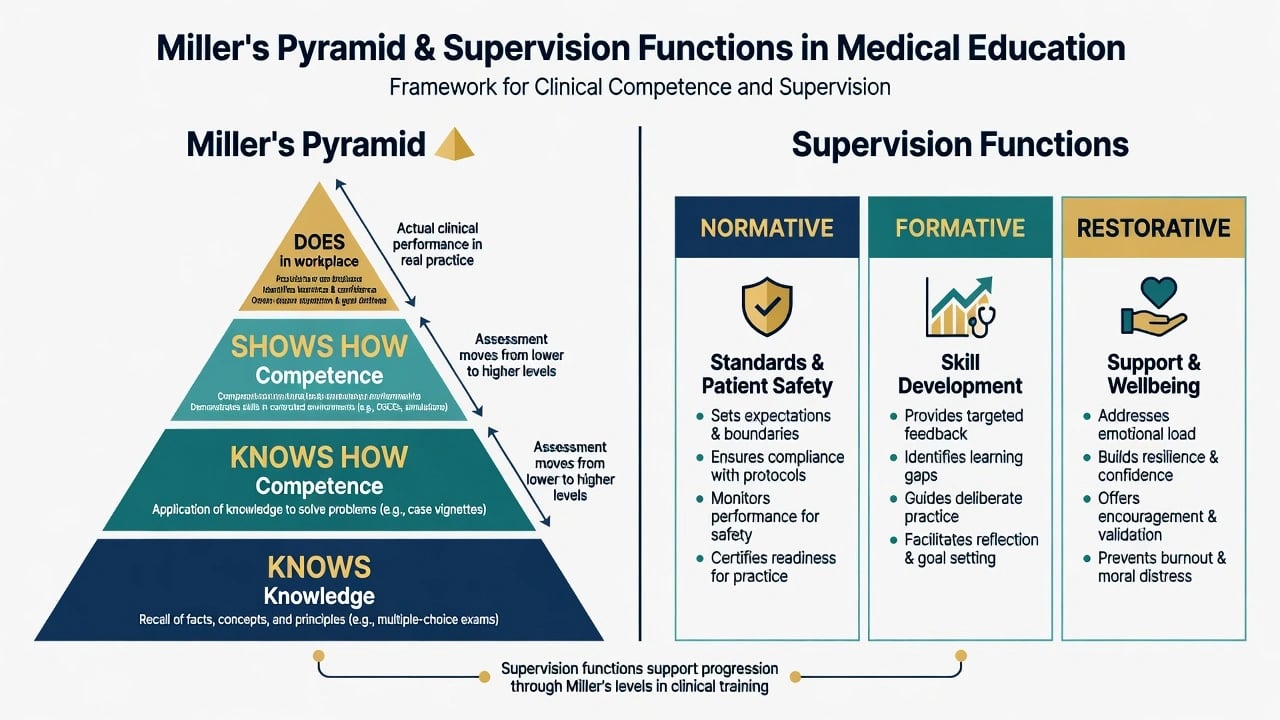
Miller’s pyramid (1990) stratifies assessment from Knows (knowledge) → Knows how (competence in reasoning) → Shows how (demonstrated performance in controlled settings) → Does (habitual performance in the workplace). Fellowship viva gold: WBA and entrustment language aim at Does, while MCQs sit lower on the pyramid.[3][4]
Competency-based medical education (CBME) organises training around predefined outcomes and abilities rather than time-served alone. Theory-to-practice frameworks emphasise clear outcomes, progressive sequencing, tailored learning experiences, and programmatic assessment rather than single high-stakes snapshots.[5]
Workplace-based assessment uses tools such as mini-CEX, case-based discussion, direct observation of procedural skills, and multisource feedback as educational tools when they generate conversation, sampling, and coaching — not mere tick-box compliance.[4]
- For learning
- Frequent, low-stakes
- Behaviour-specific coaching
- Should not surprise at end
- For progression
- Defensible standards
- Multiple samples preferred
- Document process carefully
- Aggregated samples over time
- Reduces single-event bias
- Supports entrustment decisions
- Needs faculty calibration
Epidemiology and system risk
Supervision often fails not from malice but from time pressure, cancelled sessions, lack of observation, and weak documentation. Literature reviews of clinical supervision emphasise structure, relationship quality, feedback, and organisational support as determinants of effectiveness.[1][2]
Failure to fail underperforming trainees is a documented system problem across health professions education: assessors cite lack of documentation, time, fear of appeals, personal relationship, and hope that “someone else will fail them later.” The BEME systematic review synthesises these drivers and harms (patients, future supervisors, the trainee’s eventual career crisis).[10]
Faculty development initiatives improve teaching effectiveness when sustained and multi-method, not one-off lectures; systematic reviews support this investment.[12]
Mechanisms of learning
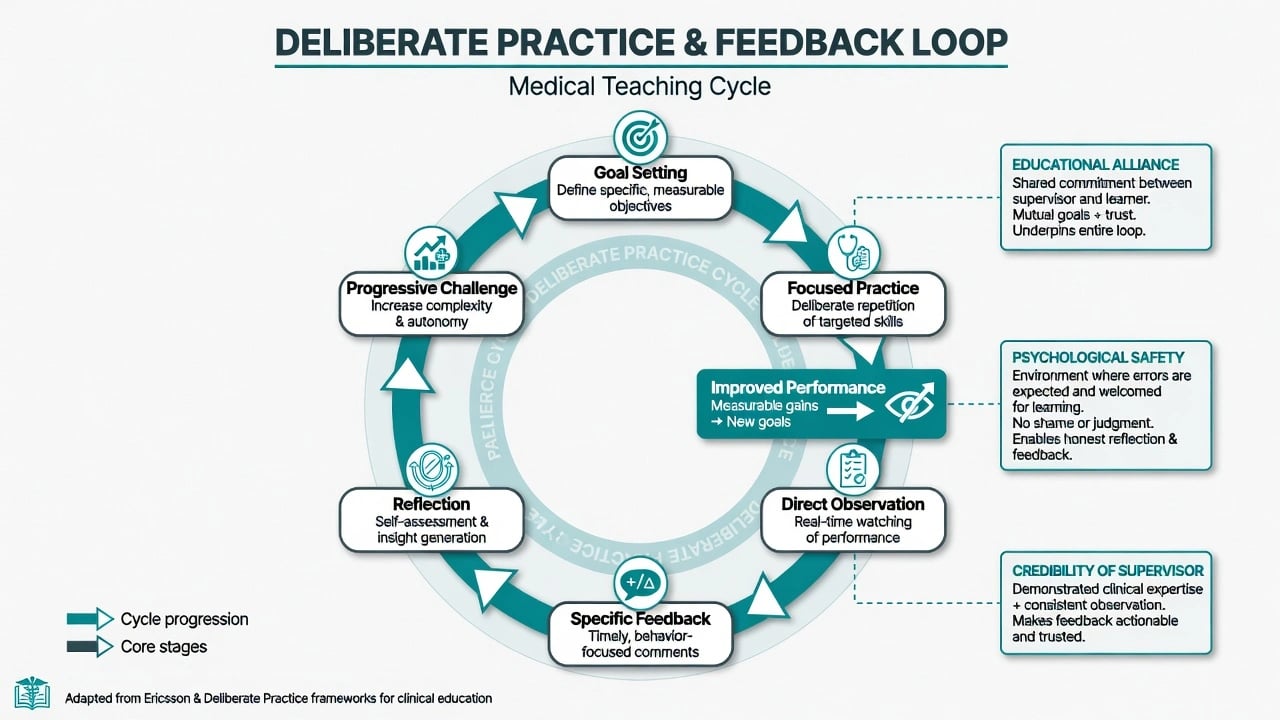
Deliberate practice (Ericsson) is goal-directed, effortful practice of defined tasks with feedback, reflection, and progressive challenge — distinct from mere repetition or years of service. Clinical teaching should create conditions for deliberate practice of formulation, risk assessment, interviewing, and decision-making.[8]
Feedback acceptance depends on credibility of the source, quality of the relationship, and learning culture. Classic feedback principles (Ende) remain examinable: feedback should be expected, timely, based on first-hand data, limited to remediable behaviours, phrased in descriptive non-judgemental language, and linked to specific goals.[6]
The R2C2 model structures facilitated reflective feedback as Relationship, Reaction, Content, and Coaching for change — useful when performance data are sensitive or multisource.[9]
Educational alliance (trust, respect, shared goals, psychological safety) mediates whether challenging feedback is used rather than dismissed. Humiliation destroys alliance; honest standards with respect build it.[1][2][6][9]
Clinical presentation — exam stems
Classic stems: a registrar who wants “any feedback” mid-term; a trainee whose risk assessments are thin; a consultant who never fails anyone; a WBA completed without observation; public shaming on the ward round; a dual-role conflict (you are treating the trainee’s relative / close friend of the trainee); CASC/OSCE teaching or feedback stations; a rural trainee with only tele-supervision; an IMG struggling with local communication norms; a distressed trainee after a critical incident.[1][2][10]
Differential of underperformance
Do not treat “poor trainee” as a single diagnosis.[10][11]
| Pattern | Favours educational gap | Favours other |
|---|---|---|
| Knowledge deficits on CBD | Curriculum gap; inadequate reading plan | Sleep debt; depression impairing concentration |
| Skill gaps on observed interview | Needs deliberate practice and coaching | Never observed before — sampling error |
| Professionalism lapses | Needs clear standards + consequences | Personality vs illness vs substance use |
| Sudden drop after prior excellence | Illness, crisis, bullying, overload | New supervisor calibration difference |
| Rejects all feedback | Fixed mindset / shame / alliance rupture | Unfair or non-specific feedback process |
Assessment of the learner (and of your supervision)
Structure a supervision session: protected time; co-created agenda; review of cases and learning goals; plan for direct observation; specific feedback; wellbeing check; documentation of decisions and action points.[1][2]
Map learning needs to Miller levels and curriculum outcomes; sample performance across contexts rather than relying on hallway reputation.[3][4]
When performance collapses, screen for illness, substance use, and safety (doctor-health principles) in parallel with educational diagnosis — not instead of it.[11]
Investigations — educational data, not labs
There is no blood test for teaching quality. Use multiple workplace samples, portfolio/logbook review, multisource perspectives, reflection entries, and observed encounters. Investigate systems factors (induction failure, impossible caseload, bullying). If impairment is suspected, use occupational health / physician-health pathways in parallel with educational process — jurisdiction-specific.[4][10][11]
Immediate management (safety first)
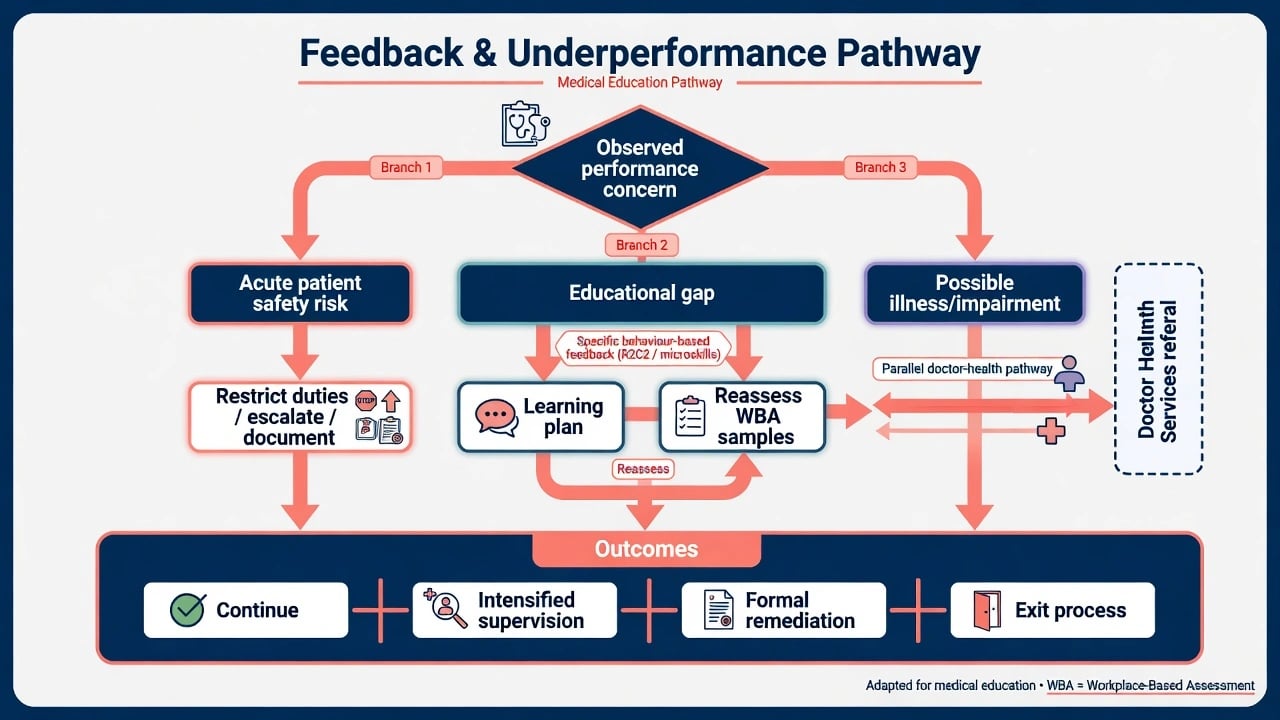
If a trainee’s practice creates acute patient risk: increase supervision intensity, restrict independent high-risk duties, ensure senior cover, document objective observations, escalate within the training and clinical governance structure. Do not leave an unsafe doctor unsupervised for service convenience.[1][2][10]
If the issue is an educational gap without acute danger: deliver timely behaviour-based feedback, set a learning plan, schedule observed reassessment, and involve the educational supervisor early rather than waiting for a catastrophic end-of-term report.[6][9][11]
Definitive management — how to teach and supervise well
One-minute preceptor (five microskills)
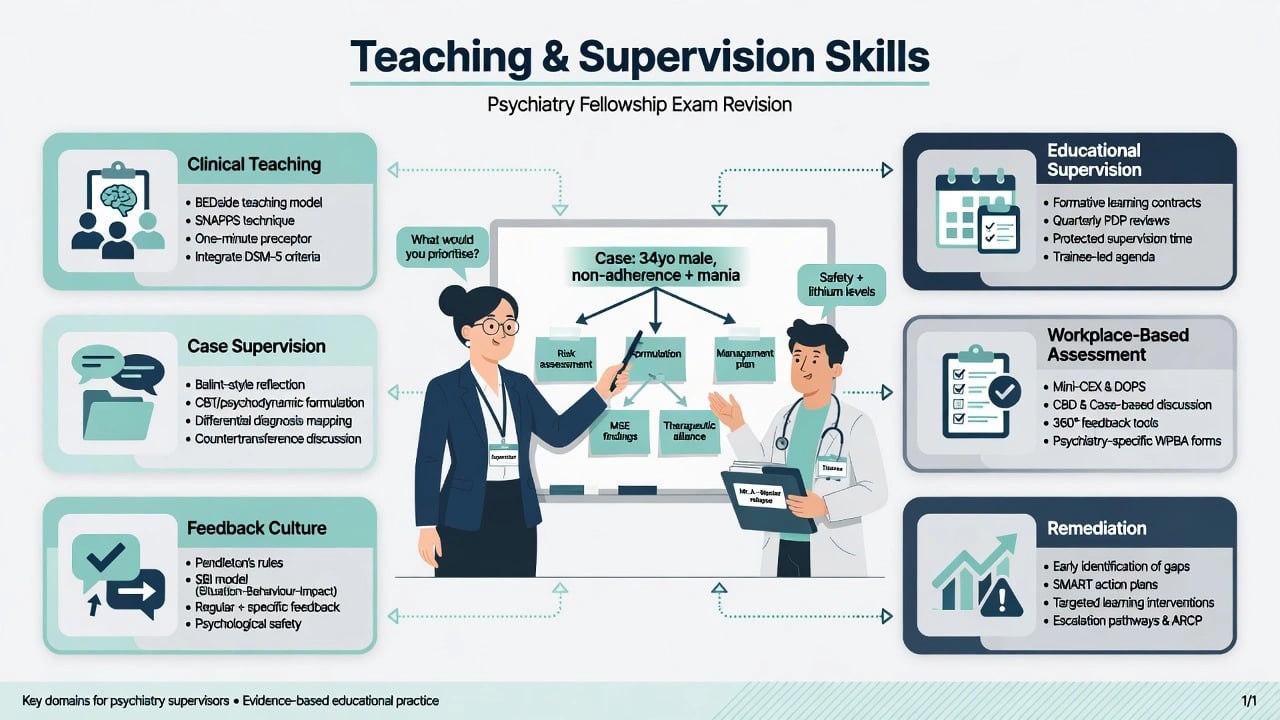
A high-yield bedside model for short clinical teaching encounters uses five microskills in order: get a commitment (“What do you think is going on?”); probe for supporting evidence (“What findings led you there?”); teach general rules (one transferable principle); reinforce what was done right (specific behaviours); and correct mistakes (specific, private when possible, with a plan).[7]
Feedback models
- Ende principles: expected, timely, first-hand, remediable behaviours, descriptive language, limited quantity, goal-linked.[6]
- R2C2: build relationship; explore reactions to data; discuss content; coach for change.[9]
- Prefer honest, respectful specificity over an empty “feedback sandwich” that buries the message.[6][9]
Deliberate practice design
Define the target skill (for example MSE structure, risk formulation, family meeting); arrange repeated observed practice; give specific feedback; increase complexity; reassess.[8]
Remediation
Literature on remediating physicians and trainees across the continuum emphasises early identification, multidimensional diagnosis of the deficit, tailored learning plans, coaching and resources, reassessment, and documentation. Remediation is an educational process with governance — not informal whispering — and programmes need clear outcomes rather than hope alone.[11]
Faculty development
Systematic reviews show multi-component faculty development improves teaching knowledge, skills, and behaviour; isolated one-hour talks are weak medicine for a skill domain.[12]
Clinical environment teaching
Teaching in the clinical environment should use authentic patient care as the curriculum, protect brief teaching moments, involve the learner actively, and respect patients as partners in teaching.[1][2][7]
Subtypes and psychiatry-specific scenarios
Psychiatry case supervision adds formulation depth, risk and capacity, countertransference, boundary vigilance, and ethics — not only “what drug next.” Educational supervision tracks WBAs, psychotherapy competencies, and training-stage outcomes without inventing form codes.[1][2][4]
Group and peer supervision support reflective practice and shared learning; they still need ground rules for confidentiality and safety.[1][2]
Remote / rural supervision requires scheduled tele-supervision, clear escalation, and attention to dual-role risks in small communities.[1][2]
Student and junior doctor teaching on psychiatry placements uses one-minute preceptor microskills, structured MSE teaching, destigmatising language, and safety framing.[7][2]
Complications and pitfalls
Classic fails: no observation; failure-to-fail; humiliation; grade inflation; summative surprise; dual relationships unmanaged; confusing line management with educational support without clarity; ignoring trainee illness; documenting opinions without behaviours; inventing college statutes; and treating faculty development as optional personality rather than a skill set.[6][10][11][12]
Prognosis and disposition
Most knowledge and skill gaps improve with deliberate practice, observation, and coaching. Insight and professionalism problems are harder and may require extended training, intensified supervision, or programme exit. Disposition options: continue with goals; intensified supervision; formal remediation; interrupted training; exit. Patient safety and public protection take priority when they conflict with a trainee’s career preference.[10][11]
Special populations
Junior doctors need scaffolding and high teaching density. IMGs need orientation to local systems and culturally safe feedback. Trainees with disability need reasonable adjustments that do not lower competence standards. Returners after leave need re-entry plans. Supervisors who are burned out or untrained need support and faculty development — supervision quality is an organisational duty.[1][12]
Evidence, guidelines, and regional differences
Landmark anchors: Kilminster supervision reviews and AMEE Guide 27; Miller pyramid; Norcini WBA AMEE Guide 31; Frank CBME theory-to-practice; Ende feedback; Neher microskills; Ericsson deliberate practice; Sargeant R2C2; Yepes-Rios failure-to-fail BEME; Hauer remediation review; Steinert faculty development reviews.[1][2][3][4][5][6][7][8][9][10][11][12]
[2] [4] [5] [10]Exam pearls
TEACH-SAFE
Hero overview figure
References
- [1]Kilminster SM, Jolly BC Effective supervision in clinical practice settings: a literature review Med Educ, 2000.PMID 11012933
- [2]Kilminster S, Cottrell D, Grant J, Jolly B AMEE Guide No. 27: Effective educational and clinical supervision Med Teach, 2007.PMID 17538823
- [3]Miller GE The assessment of clinical skills/competence/performance Acad Med, 1990.PMID 2400509
- [4]Norcini J, Burch V Workplace-based assessment as an educational tool: AMEE Guide No. 31 Med Teach, 2007.PMID 18158655
- [5]Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice Med Teach, 2010.PMID 20662574
- [6]Ende J Feedback in clinical medical education JAMA, 1983.PMID 6876333
- [7]Neher JO, Gordon KC, Meyer B, Stevens N A five-step "microskills" model of clinical teaching J Am Board Fam Pract, 1992.PMID 1496899
- [8]Ericsson KA Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains Acad Med, 2004.PMID 15383395
- [9]Sargeant J, Lockyer J, Mann K, et al. Facilitated Reflective Performance Feedback: Developing an Evidence- and Theory-Based Model That Builds Relationship, Explores Reactions and Content, and Coaches for Performance Change (R2C2) Acad Med, 2015.PMID 26200584
- [10]Yepes-Rios M, Dudek N, Duboyce R, et al. The failure to fail underperforming trainees in health professions education: A BEME systematic review: BEME Guide No. 42 Med Teach, 2016.PMID 27602533
- [11]Hauer KE, Ciccone A, Henzel TR, et al. Remediation of the deficiencies of physicians across the continuum from medical school to practice: a thematic review of the literature Acad Med, 2009.PMID 19940595
- [12]Steinert Y, Mann K, Anderson B, et al. A systematic review of faculty development initiatives designed to enhance teaching effectiveness: A 10-year update: BEME Guide No. 40 Med Teach, 2016.PMID 27420193