Psych · Professional — working with interpreters and CALD communities
Working with interpreters and CALD communities
Also known as Professional interpreters psychiatry · Limited English proficiency mental health · Language concordance · CALD mental health · Ad hoc interpreters · Video remote interpreting · Cultural broker · Language access psychiatry
Exam-exhaustive fellowship reference on working with professional interpreters and CALD communities in psychiatry — language concordance, ad hoc interpreter errors, interpreter workflow (brief, seating, first-person, debrief), MSE and risk through interpreters, cultural formulation interface, special populations, and equity. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Culturally and linguistically diverse (CALD) is a service-planning umbrella used widely in Australia and similar systems. It is not a clinical identity and must never become a stereotype checklist. People differ by language, dialect, migration pathway, literacy, religion, sexuality, disability, and power relative to services.[14][15][16]
Key constructs examiners expect by name include preferred language, LEP, language concordance, professional vs ad hoc interpreters, cultural brokers, and translation versus interpretation.[1][3][6][13]
| Construct | Clinical meaning | Exam trap |
|---|---|---|
| Preferred language | Language the person wants for care discussion | Assuming companion fluency equals patient fluency |
| Limited English proficiency (LEP) | Insufficient English for safe clinical communication | Equating accent or basic chat with capacity for consent |
| Language concordance | Clinician and patient share the care language fluently | Over-claiming "I speak a bit" as concordance |
| Professional interpreter | Trained, bound by confidentiality and accuracy standards | Treating bilingual staff or family as equivalent |
| Ad hoc interpreter | Family, friend, child, or untrained staff | "Better than nothing" for risk/consent/trauma |
| Cultural broker / liaison | Cultural mediation and navigation | Substituting for language interpreting |
| Translation vs interpretation | Written vs spoken/signed language transfer | Using machine translation for psychiatric assessment |
Language is one domain of culture. Fluent English does not remove the need for cultural formulation when identity, explanatory models, or racism shape care.[18][19][20]

Classification — roles, modalities, and frameworks
Who is speaking for whom?
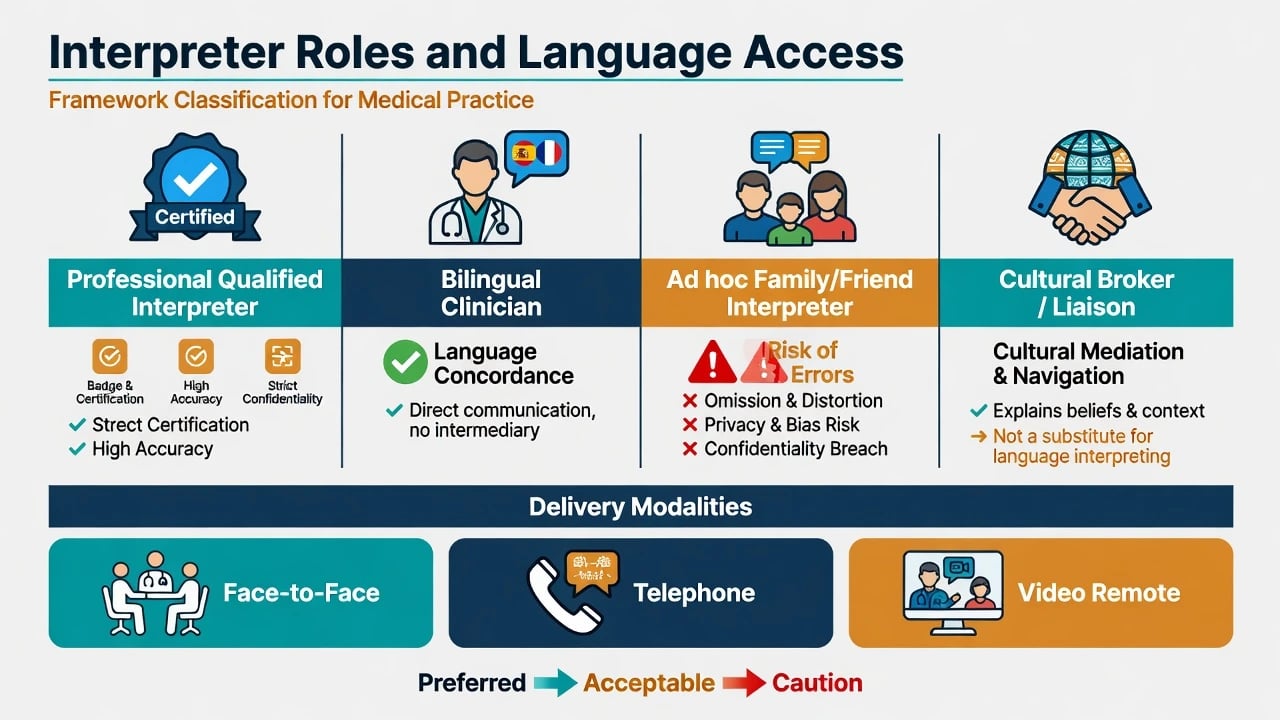
- Professional / accredited interpreter — preferred standard for assessment, risk, consent, and therapy when language-discordant.[1][3][12]
- Language-concordant bilingual clinician — can improve communication quality when truly fluent and clinically competent in both languages; partial concordance still needs optimisation.[6][13]
- Ad hoc interpreter — family, friends, children, random staff. Associated with more clinically significant interpretation errors than professional interpreters.[3][4]
- Cultural broker / Aboriginal or ethno-specific liaison — supports cultural safety and system navigation; still use a professional interpreter when languages differ.[1][17]
Modalities
Face-to-face consecutive interpretation is preferred for complex MSE and trauma work when available; telephone and video remote interpreting (VRI) are essential professional alternatives when delay would compromise acute risk or consent; simultaneous modes are uncommon at the bedside, so short consecutive segments remain the default.[1][9][12]
System-level language-access improvement can increase professional interpreter utilisation — design matters, not goodwill alone.[12]
Epidemiology, inequity, and access
Language barriers reduce access to psychiatric care and degrade care processes when services are reached.[2] Limited English proficiency associates with altered mental health service use patterns among people with mental disorders; quality of psychiatric care is sensitive to language proficiency and interpreter use.[1][5]
Language discordance associates with poorer communication-sensitive outcomes across medicine; language concordance tends to improve quality-related measures.[6][7] Depression collaborative-care literature in LEP populations highlights the need for intentional language-access design rather than assuming models transfer unchanged.[8]
Australian CALD communities face multi-level barriers to mental health service access and utilisation (need recognition, enabling resources, and service factors in Andersen-type frames).[14] Religion and spirituality may be central to meaning and help-seeking for some CALD groups and should be elicited, not pathologised or ignored.[15] Racism, xenophobia, and discrimination map to health outcomes through structural and interpersonal pathways — language access work that ignores racism is incomplete.[20]
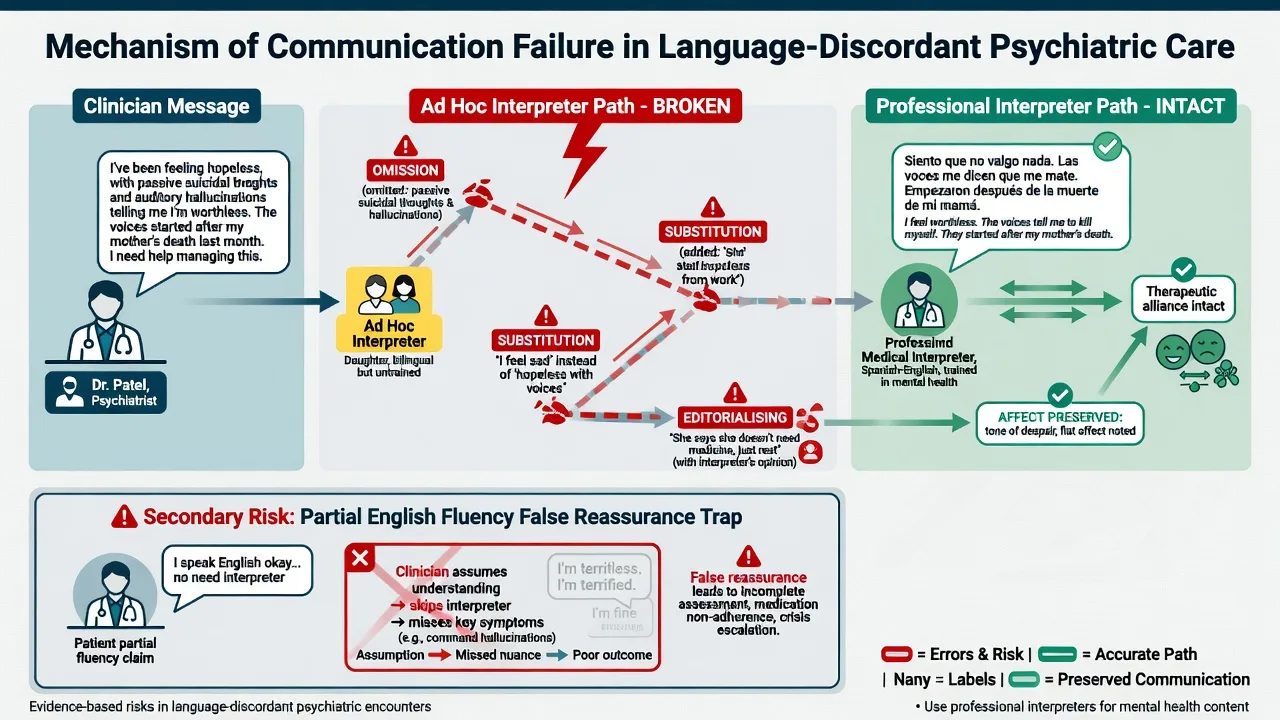
Mechanisms — how language discordance harms care
Information failure
Psychiatric diagnosis and risk rest on precise wording (intent vs ideation, command hallucinations, capacity reasoning). Errors of omission, addition, substitution, and editorialising distort that data. Comparative work shows professional interpreters produce fewer clinically significant errors than ad hoc interpreters or no interpreter.[3][4]
Alliance and power
Side conversations, third-person talk ("ask her if…"), and clinician–interpreter collusion shrink the patient. Forced migrants may fear interpreters from the same community, political faction, or small diaspora — confidentiality anxiety is clinical data, not "paranoia by default".[9][16]
Partial concordance trap
"Getting by" in English for social chat fails for suicide enquiry, sexual side effects, or involuntary treatment explanation. Partial language concordance can create false reassurance that full understanding occurred.[13]
Culture without language, language without culture
Kleinman-style disease/illness distinction and explanatory models still apply when language is shared; CFI field-trial evidence supports structured cultural interviewing as feasible and useful.[18][19] Language access without cultural humility still produces category fallacies and racist practice.[17][20]
Clinical presentation
Language-discordant presentations commonly feature delayed help-seeking; family as gatekeepers or sole historians; somatic idioms of distress; spiritual or religious framing of symptoms; apparent restricted affect, poverty of speech, or thought disorder that is actually English limitation; incomplete disclosure of suicidal ideation, domestic violence, or substance use in front of relatives; mistrust after prior racist or dismissive encounters; and preference for gender-matched or dialect-matched interpreters.[1][9][11][15][20]
Primary care surveys document clinician-recognised language barriers in mental health work — the problem is frontline and frequent, not rare exam trivia.[11]
Differential and discriminators
- Improves with professional interpreter
- Thought form clearer in preferred language
- History expands with trust and time
- Document residual uncertainty
- Persists in preferred language
- Derailment, neologisms, poverty of content
- Corroborated by bilingual collateral
- Course and function match psychosis
- Relative edits answers
- Protective minimisation of risk
- Child omits sexual/trauma content
- Clinician hears sanitised version
| Problem | Discriminators |
|---|---|
| Cognitive impairment / dementia | History, function, preferred-language cognitive testing, not English-only mini-tests |
| Cultural/spiritual experience vs psychosis | Distress, dysfunction, community consensus, course, MSE form |
| Trauma vs "non-engagement" | Avoidance, triggers, interpreter fears, post-migration living difficulties |
| Capacity refusal vs misunderstanding | Teach-back in preferred language; check interpreter fidelity |
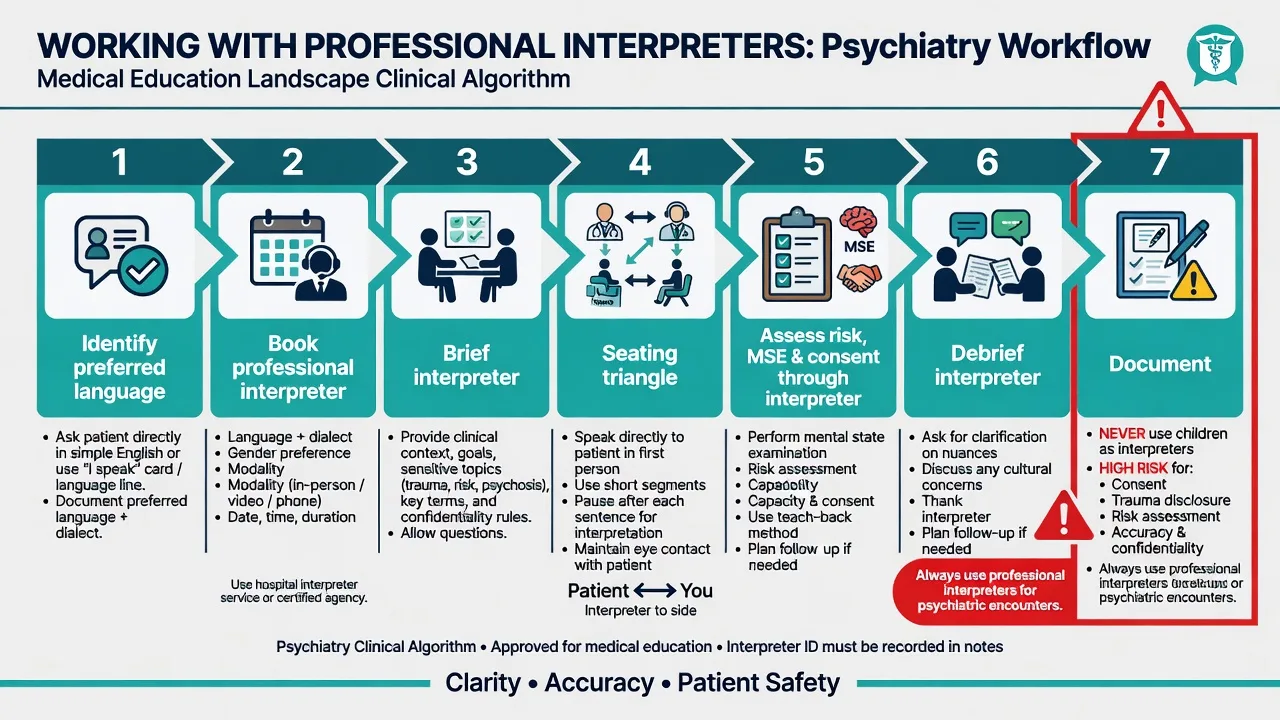
Bedside assessment — the interpreter workflow
Sequence (memorise for CASC/viva)
- Identify preferred language and dialect early — ask the patient, not only the relative.
- Book professional interpreter — language, dialect, gender preference, modality (face-to-face / phone / VRI).
- Brief the interpreter (2–3 minutes outside or aside): purpose of interview, expected sensitive topics (risk, trauma, sexual side effects), technical terms, seating, first-person rule, confidentiality, request for verbatim odd phrases rather than "cleaning up" speech.
- Introduce everyone; confirm patient comfort with this interpreter (especially small communities / political conflict).
- Seating triangle — patient and clinician eye-line primary; interpreter slightly aside.
- Speak to the patient in first person, short segments; pause for interpretation; watch non-verbals.
- Complete full risk assessment through the interpreter — ideation, intent, plan, means, protective factors, substances, domestic violence as indicated.
- Elicit explanatory model / CFI-relevant data in preferred language.[18][19]
- Debrief interpreter after traumatic or high-affect content; check for untranslated material or safety concerns.
- Document: languages used, interpreter name/ID/agency/modality, patient comfort, residual uncertainty, and any family present.
MSE through an interpreter
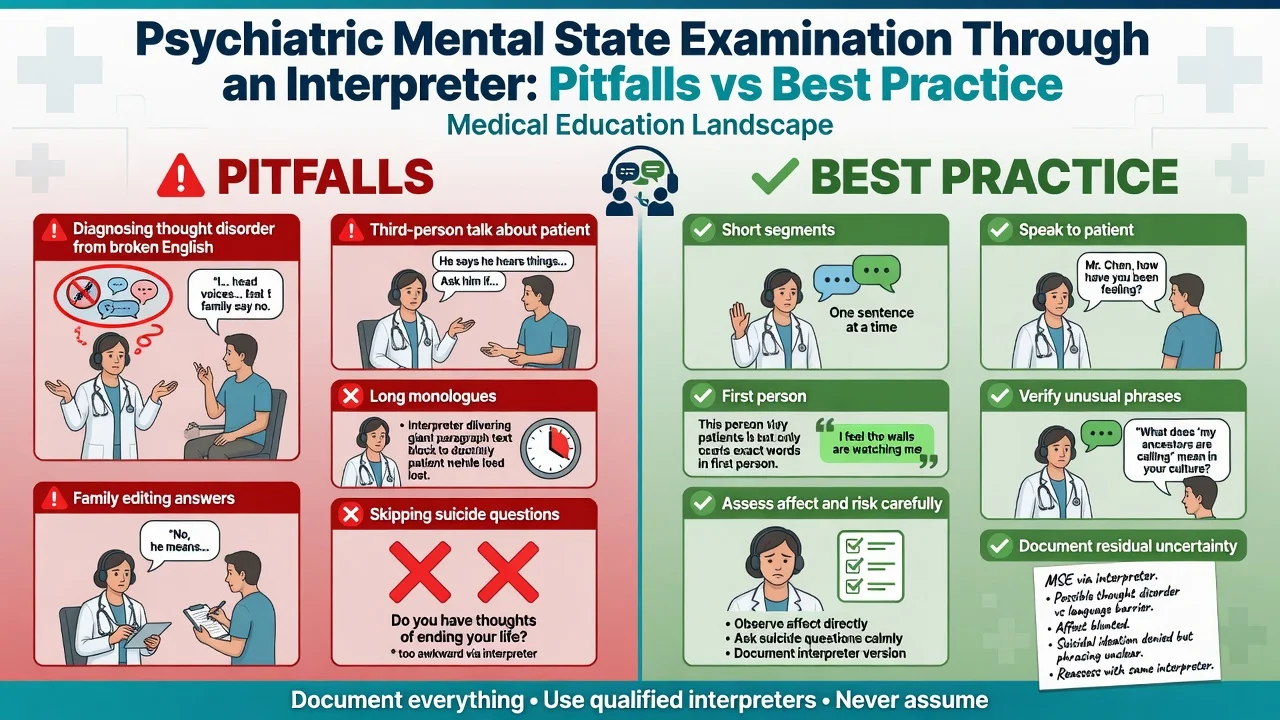
- Rate speech and thought form cautiously; ask interpreter to flag neologisms or disorganised language in the source language.
- Affect is partly non-verbal — still observe directly.
- Insight and judgement require teach-back, not yes/no assent.
- Cognitive screens need language-appropriate tools or interpreted administration with documented limits.[1]
Forced migrants and confidential interpreting
Working with interpreters for forced migrants requires extra attention to trust, political affiliations, gender, and trauma-related arousal during sessions. Contract roles; avoid turning the interpreter into an untrained therapist; plan session length generously.[9][16]
Investigations and scales
There is no "CALD blood test". Organic work-up follows clinical indication. Caution with English-only rating scales; prefer validated translations or interpreter-supported administration with explicit limitations. Document that scores may not be comparable to monolingual norms when tools are unvalidated for that language.[1][8]
Acute / emergency management
Priority order: life/limb medical issues → behavioural safety → professional language access (any professional modality) → full psychiatric assessment → disposition with interpreter needs named for next contact.[1][2][3]
Definitive management and systems of care
Clinical standard
- Professional interpreter for assessment, formulation, risk, consent, psychoeducation, and therapy when discordant.[1][2]
- Collaborative plan that integrates explanatory models and, where relevant, religion/spirituality as the person defines them.[15][18][19]
- Medication discussions with teach-back of indication, dose schedule, common adverse effects, and monitoring — in preferred language.[1][13]
- Psychotherapy: interpreter-mediated work needs explicit contracting (roles, confidentiality, seating, not answering for the patient); child/adolescent work needs a specific framework beyond "just book someone".[10]
- Depression collaborative care and other models require language-access adaptation for LEP populations.[8]
System standard
Language access policies, trained booking workflows, staff education, quality improvement of interpreter utilisation, ethno-specific and refugee services, and cultural psychiatry training competencies are part of safe services — not extras.[12][16][17]
Subtypes and high-yield scenarios
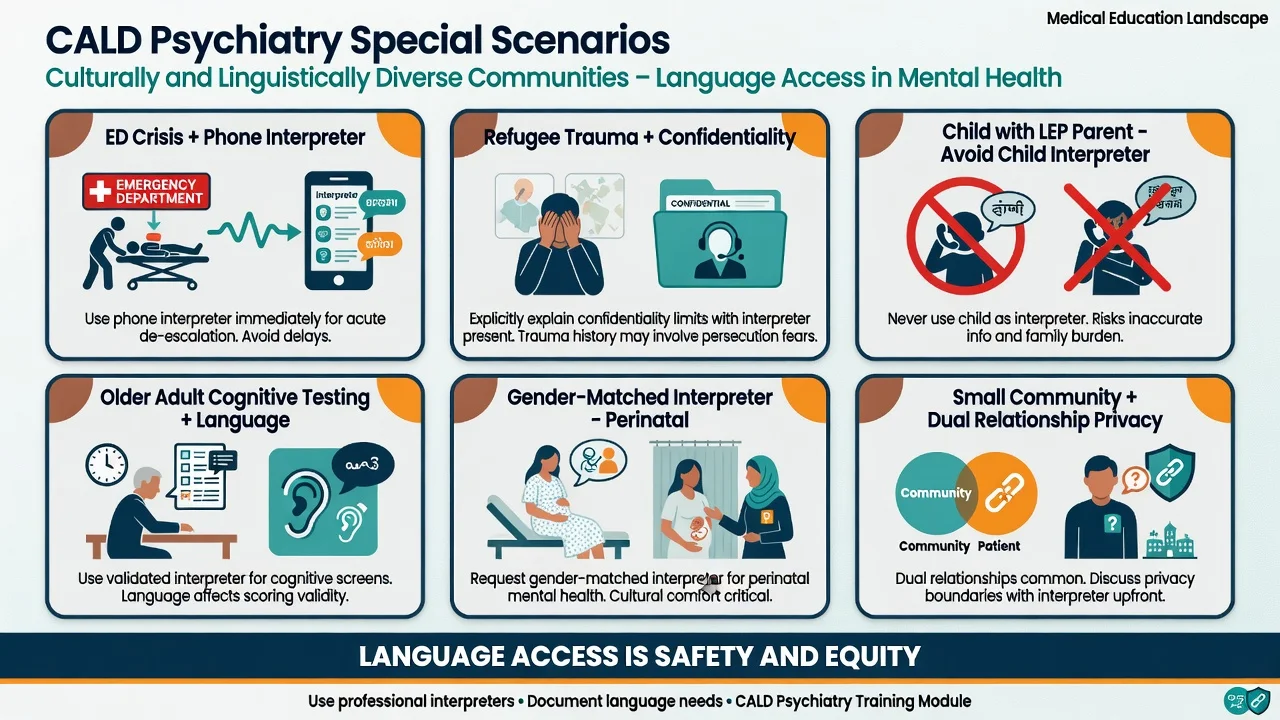
| Scenario | Priority moves |
|---|---|
| ED acute risk, LEP | Phone/VRI professional interpreter now; full risk; no child interpreter |
| Inpatient consent / capacity | Preferred-language discussion; teach-back; document interpreter |
| Depot / adherence clinic | Interpreter every visit if needed; explanatory model of "needles" |
| Refugee trauma history | Trusted interpreter; gender match; paced interview; confidentiality contract |
| Parent LEP, child English | Dual dynamic; do not make child the family interpreter for adult content |
| Older CALD cognition | Preferred-language testing; collateral; avoid English-only mini-mental as sole tool |
| Small community dual relationship | Offer remote interpreter from outside community if patient prefers |
| Forensic / medico-legal | Professional interpreter mandatory; document meticulously |
Complications and pitfalls
- Ad hoc interpreting → missed suicide intent, coerced "consent", false thought disorder.[3][4]
- Partial English → incomplete psychotropic counselling.[13]
- Machine translation apps for psychiatric assessment → unvalidated, confidentiality risks, tone loss.
- Stereotyping "CALD non-compliance" instead of addressing language, stigma, racism, and access.[14][20]
- Pathologising spiritual idioms — or missing psychosis labelled as "cultural".
- Interpreter burnout and secondary trauma without debrief after graphic content.[9]
Prognosis and disposition
Engagement, adherence, and safety planning improve when people understand and are understood. Disposition plans that forget the next interpreter booking recreate the barrier. Link dual pathways: mainstream psychiatry plus multicultural/refugee/ethno-specific supports as indicated.[2][8][14][16]
Special populations
- Children and adolescents — need an explicit framework for integrating interpreters; protect children from adult content interpreting roles.[10]
- Perinatal — intimate topics; offer gender-matched interpreters; partner presence is patient-defined.
- Older adults — sensory impairment + language + cognition compound; allow time.
- Deaf / hard of hearing — qualified sign language interpreters, not family lip-reading.
- Intellectual disability with CALD family — dual supports; plain language; professional interpreting for family meetings.
- LGBTQ+ CALD — privacy with community interpreters; do not out patients.
Evidence and guidelines (exam anchors)
- Bauer and Alegría (2010) — systematic review: language proficiency and interpreter use impact psychiatric care quality.[1]
- Ohtani et al. (2015) — systematic review: language barriers reduce access to psychiatric care.[2]
- Flores et al. (2003, 2012) — interpretation errors and clinical consequences; professional vs ad hoc vs none.[3][4]
- Diamond et al. (2019); Cano-Ibáñez et al. (2021) — concordance/discordance and outcomes.[6][7]
- Garcia et al. (2018) — collaborative care for depression in LEP populations.[8]
- Tribe and Thompson (2022) — interpreters with forced migrants.[9]
- WPA migrant/refugee report (2024); Kirmayer et al. cultural psychiatry training guidelines.[16][17]
- CFI field trial and Kleinman for formulation interface; Selvarajah et al. for racism–health pathways.[18][19][20]
RANZCP-aligned practice expects culturally safe, equitable care including communication supports. NICE/APA equity frameworks similarly treat accessible communication as quality of care. Regional logistics (accreditation systems, telephone interpreter services) differ — principles of professional language access, consent, and equity do not.[1][16][17][20]
Exam pearls
- Preferred language is a vital sign of communication.
- Professional interpreter before complex consent.
- Brief and debrief are not optional niceties.
- Document interpreter ID and residual uncertainty.
- Language access is equity and safety.
- Cultural formulation still applies when English is fluent.[1][3][18][20]
INTERPRET — working with interpreters
References
- [1]Bauer AM, Alegría M Impact of patient language proficiency and interpreter service use on the quality of psychiatric care: a systematic review Psychiatr Serv, 2010.PMID 20675834
- [2]Ohtani A, Suzuki T, Takeuchi H, Uchida H Language Barriers and Access to Psychiatric Care: A Systematic Review Psychiatr Serv, 2015.PMID 25930043
- [3]Flores G, Abreu M, Barone CP, et al. Errors of medical interpretation and their potential clinical consequences: a comparison of professional versus ad hoc versus no interpreters Ann Emerg Med, 2012.PMID 22424655
- [4]Flores G, Laws MB, Mayo SJ, et al. Errors in medical interpretation and their potential clinical consequences in pediatric encounters Pediatrics, 2003.PMID 12509547
- [5]Bauer AM, Chen CN, Alegría M English language proficiency and mental health service use among Latino and Asian Americans with mental disorders Med Care, 2010.PMID 21063226
- [6]Diamond L, Izquierdo K, Canfield D, et al. A Systematic Review of the Impact of Patient-Physician Non-English Language Concordance on Quality of Care and Outcomes J Gen Intern Med, 2019.PMID 31147980
- [7]Cano-Ibáñez N, Zolfaghari Y, Amezcua-Prieto C, Khan KS Physician-Patient Language Discordance and Poor Health Outcomes: A Systematic Scoping Review Front Public Health, 2021.PMID 33816420
- [8]Garcia ME, Ochoa-Frongia L, Moise N, et al. Collaborative Care for Depression among Patients with Limited English Proficiency: a Systematic Review J Gen Intern Med, 2018.PMID 29256085
- [9]Tribe R, Thompson K Working with interpreters when working with forced migrants in mental health Int Rev Psychiatry, 2022.PMID 36695209
- [10]Leanza Y, Boivin I, Moro MR, et al. Integration of interpreters in mental health interventions with children and adolescents: The need for a framework Transcult Psychiatry, 2015.PMID 25501490
- [11]Brisset C, Leanza Y, Rosenberg E, et al. Language barriers in mental health care: a survey of primary care practitioners J Immigr Minor Health, 2014.PMID 24375384
- [12]Karliner LS, Gregorich SE, Mutha S, et al. Language Access Systems Improvement initiative: impact on professional interpreter utilisation, a natural experiment BMJ Open, 2024.PMID 38176864
- [13]Leung G, Dea D, Ho EY, Diamond L Partial language concordance in primary care communication: What is lost, what is gained, and how to optimize Patient Educ Couns, 2025.PMID 39954380
- [14]Radhamony R, Cross WM, Townsin L, Banik B Culturally and Linguistically Diverse Community Access and Utilisation of the Mental Health Service: An Explanation Using Andersen's Behavioural Model Issues Ment Health Nurs, 2024.PMID 38954511
- [15]Malviya S The Need for Integration of Religion and Spirituality into the Mental Health Care of Culturally and Linguistically Diverse Populations in Australia: A Rapid Review J Relig Health, 2023.PMID 36780111
- [16]Schouler-Ocak M, Kastrup MC, Küey L, et al. A report from the WPA Working Group on Providing Mental Health Care for Migrants and Refugees World Psychiatry, 2024.PMID 39279400
- [17]Kirmayer LJ, Fung K, Rousseau C, et al. Guidelines for Training in Cultural Psychiatry Can J Psychiatry, 2021.PMID 32345034
- [18]Lewis-Fernández R, Aggarwal NK, Lam PC, et al. Feasibility, acceptability and clinical utility of the Cultural Formulation Interview: mixed-methods results from the DSM-5 international field trial Br J Psychiatry, 2017.PMID 28104738
- [19]Kleinman A, Eisenberg L, Good B Culture, illness, and care: clinical lessons from anthropologic and cross-cultural research Ann Intern Med, 1978.PMID 626456
- [20]Selvarajah S, Corona Maioli S, Deivanayagam TA, et al. Racism, xenophobia, and discrimination: mapping pathways to health outcomes Lancet, 2022.PMID 36502849