Psych · Psychopharmacology — antidepressants
Antidepressants
Also known as SSRIs · SNRIs · Tricyclic antidepressants · MAOIs · Mirtazapine · Bupropion · Vortioxetine · Antidepressant switching · STAR*D
Exam-exhaustive fellowship pharmacology of antidepressants — SSRI/SNRI/mirtazapine/bupropion/vortioxetine/TCA/MAOI maps, doses and monitoring, STAR*D logic, Cipriani NMA, augmentation (lithium, atypical AP, T3), sexual side-effects, hyponatraemia, serotonin syndrome, discontinuation, early suicide risk, switching and MAOI washouts, pregnancy pointer. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Antidepressant pharmacology is daily viva language across FRANZCP, MRCPsych and ABPN. Examiners want agent-level doses, monitoring, STAR*D step logic, Cipriani network ranks without marketing spin, and hard safety knowledge — serotonin toxicity, early treatment suicidality, hyponatraemia, washouts — not a brand list. This topic is the drug-class spine that major depression, anxiety, and emergency toxicology topics plug into.[1][6][15]
Definition and classification
An antidepressant is a medicine whose primary psychotropic use is reduction of depressive syndrome severity (and, for many agents, anxiety-spectrum disorders), acting principally through monoamine transporter inhibition, receptor modulation, or monoamine oxidase inhibition.[6][11]
Working exam taxonomy (use deliberately): Class maps by monoamine target organise exam answers better than marketing generations.[6][11]
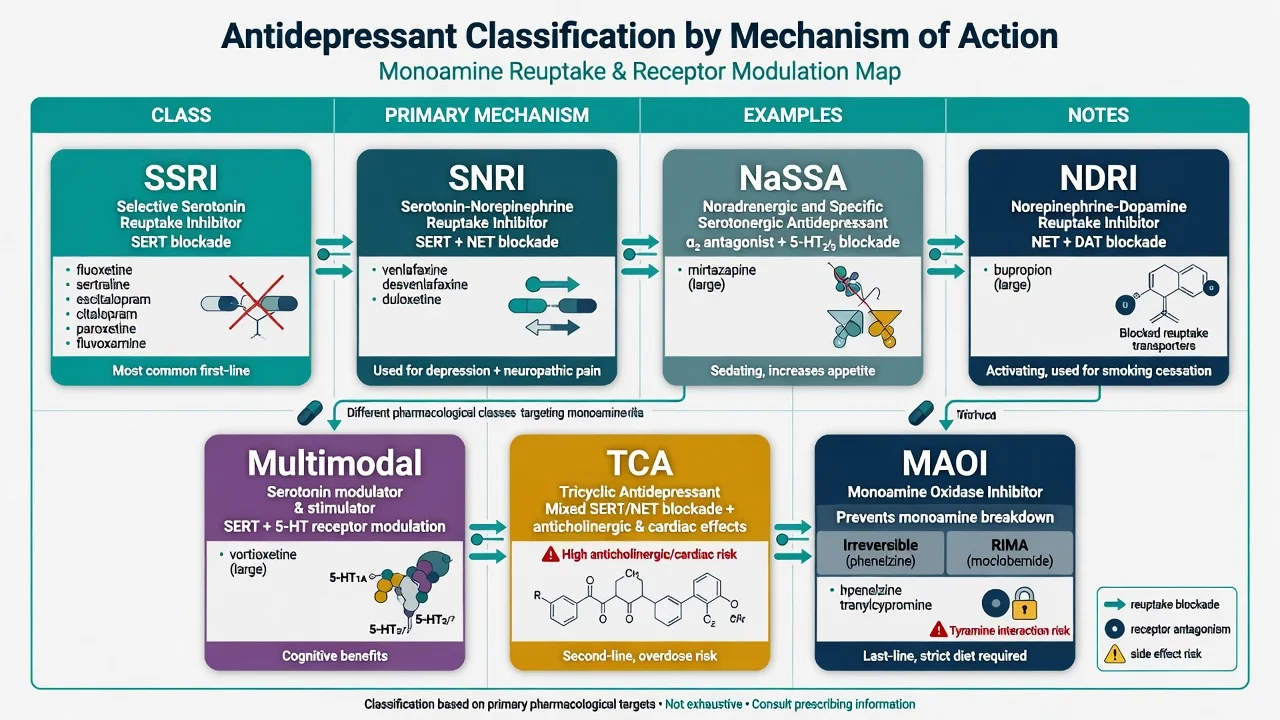
| Class | Core mechanism | Common agents (examples) | Exam emphasis |
|---|---|---|---|
| SSRI | SERT inhibition | Fluoxetine, sertraline, escitalopram, citalopram, paroxetine, fluvoxamine | First-line workhorses; sexual SE; hyponatraemia; QTc for citalopram/escitalopram |
| SNRI | SERT + NET | Venlafaxine, desvenlafaxine, duloxetine | Discontinuation (venlafaxine); BP; pain niche (duloxetine) |
| NaSSA | α2 antagonism; 5-HT2/3 block | Mirtazapine | Sedation, weight; relatively less sexual SE |
| NDRI | NET + DAT | Bupropion | Sexual sparing; seizure threshold; not anxiety-first |
| Multimodal | SERT + 5-HT receptor actions | Vortioxetine | Cognitive claims context; tolerability profile |
| TCA | Mixed monoamine + M1/H1/Na channel | Amitriptyline, nortriptyline, clomipramine | Overdose lethality; pain/OCD niches |
| MAOI | MAO inhibition | Phenelzine, tranylcypromine; moclobemide (RIMA) | Diet/interactions; washouts; late TRD pathway |
| Classification by transporter and receptor action beats “generation” marketing slogans in the exam room.[6][7][11] |
Mechanism — the viva core
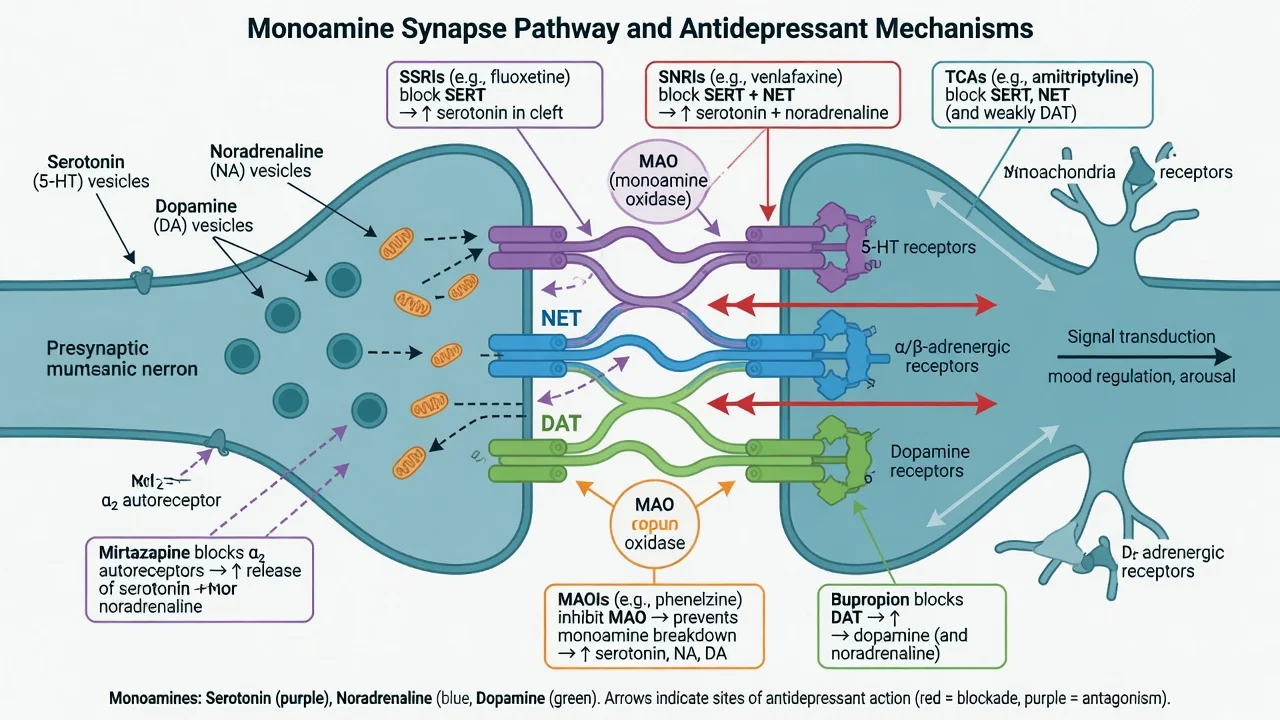
Exam scaffold. Acute transporter blockade raises synaptic monoamines; adaptive receptor and network changes over days to weeks track clinical improvement. Do not claim a single “chemical imbalance cured by one tablet” narrative — state monoamine modulation as a useful but incomplete model that still organises drug choice and toxicity.[6][12]
Class-specific hooks examiners reward:
- Mirtazapine: central α2 antagonism increases noradrenergic and serotonergic transmission; 5-HT2/3 antagonism contributes to lower sexual dysfunction and anti-nausea relative to many SSRIs, with H1-related sedation and appetite increase.[11]
- Bupropion: catecholaminergic reuptake profile; activating; lowers seizure threshold in a dose-dependent fashion; relatively sexual-function sparing in many patients.[3][20]
- Vortioxetine: SERT inhibition plus multiple 5-HT receptor actions (multimodal teaching label); place among newer options using efficacy–acceptability evidence rather than advertising slogans.[6]
- TCAs: monoamine reuptake plus anticholinergic, antihistamine and sodium-channel effects that drive cardiotoxicity in overdose.[11]
- MAOIs: block monoamine catabolism; irreversible nonselective agents create tyramine and drug-interaction constraints that make washout rules non-negotiable.[5][15]
Epidemiology and clinical context of use
Antidepressants are among the most prescribed psychotropics. Population use is high; the fellowship task is appropriate use — severity-matched, measurement-based, safety-aware — not maximal prescribing. Absolute suicide risk remains elevated in depressive illness; drug effects on suicidality are age- and time-dependent (see safety section).[12][17][18]
Sexual dysfunction and hyponatraemia are not rare curiosities: prospective multicentre data show high rates of treatment-emergent sexual dysfunction across many serotonergic agents, and case-control data link antidepressant use with hyponatraemia, especially relevant in older adults.[20][21]
When to start — stepped care, not automatic tablets
RANZCP mood disorder guidance and CANMAT pharmacological sections frame antidepressants within stepped care: mild depression often starts with psychological therapies and active monitoring; moderate-to-severe illness more often warrants medicine with or without psychotherapy; severe melancholic, psychotic, catatonic or highly suicidal presentations escalate biological intensity early (including ECT pathways covered in the MDD topic).[11][12][13]
Fournier’s patient-level meta-analysis found the average drug–placebo advantage increases with baseline severity — use this to answer “why not start an SSRI for everyone with low mood?” without nihilism about genuine moderate-severe MDD.[16]
Landmark evidence every candidate must own
Trials and analyses that change viva answers
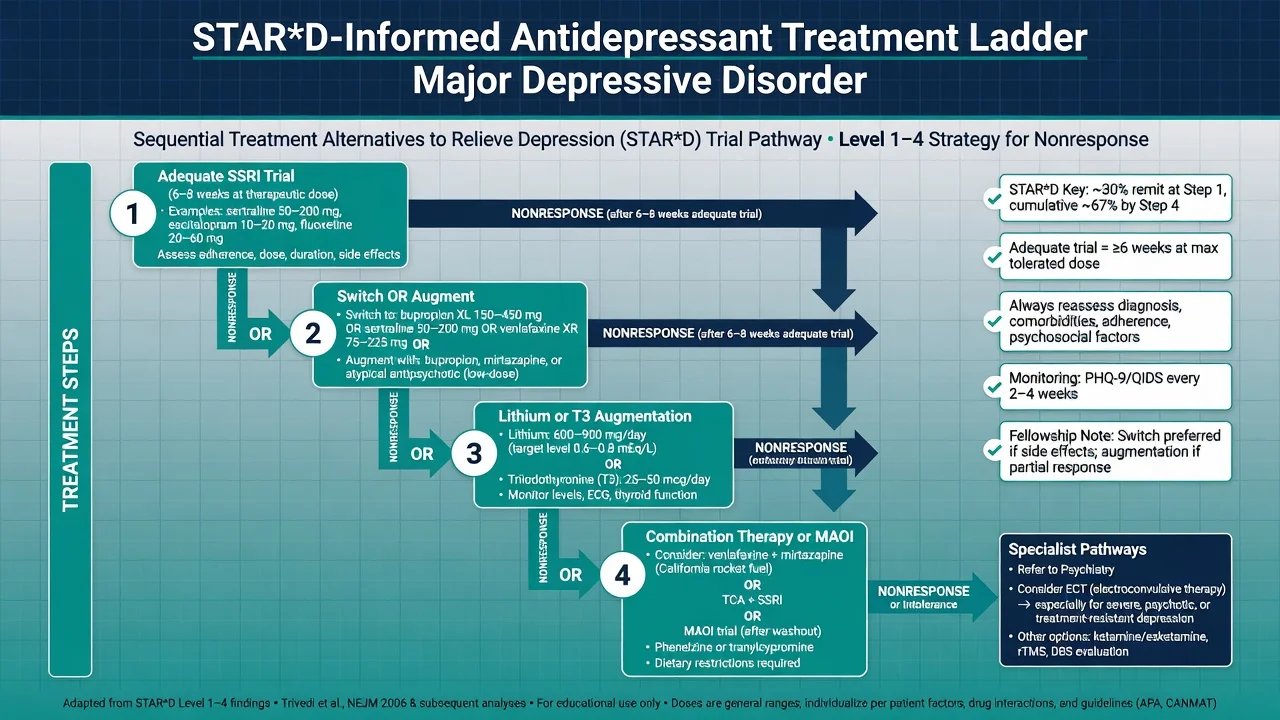
STAR*D. Level 1 measurement-based citalopram showed that structured dose optimisation matters; roughly three in ten remitted at step one in the acute report framing used in exams.[2] Overall multi-step outcomes show that many patients need more than one step and that cumulative remission falls as treatment resistance accumulates — plan for switch/augment, not endless hope on a subtherapeutic tablet.[1] After SSRI failure, switching to bupropion-SR, sertraline or venlafaxine-XR produced broadly similar remission rates — choose by side-effect profile and patient factors, not mythology of a single “strongest” switch.[3] Lithium and T3 were compared as augmentation after two failed medication treatments; both are examinable options with different monitoring burdens.[4] After three failed medication trials, tranylcypromine versus venlafaxine plus mirtazapine illustrated late-pathway difficulty and low remission — TRD is real and needs specialist intensity, not casual MAOI improvisation.[5]
Cipriani network meta-analyses. The 2009 multi-treatments analysis and the 2018 21-drug NMA show antidepressants as a class beat placebo in adults with MDD, with differences among agents in efficacy and acceptability that are real but often modest — use ranks to inform shared decisions, not to declare one universal first drug for all humans.[6][7]
Relapse prevention. Continuation antidepressant treatment after response substantially reduces relapse risk versus discontinuation in depressive disorders — maintenance is pharmacology, not optional aftercare.[8]
Augmentation meta-analyses. Lithium has randomised evidence for acceleration and augmentation of antidepressants.[10] Atypical antipsychotic augmentation improves response/remission versus placebo with metabolic and other tolerability costs that must be named.[9][23]
Clinical use and selection algorithm
Choosing a first agent (exam structure): shared decision; prior response/family history; anxiety comorbidity; sexual function priorities; sleep/appetite needs; medical comorbidity (seizure risk, hyponatraemia risk, cardiac/QTc); pregnancy potential; drug interactions (CYP); overdose risk in the home; local formulary. Typical adult oral starts (always check current product information and individualise; lower starts in older adults) are oriented by comparative efficacy–acceptability evidence and guideline pharmacological sections.[6][11][13]
| Agent | Typical adult oral pattern | Practical notes |
|---|---|---|
| Sertraline | 50 mg daily → 50–200 mg | Broad anxiety comorbidity utility |
| Escitalopram | 10 mg → 10–20 mg | Clean PK; QTc caution at higher dose |
| Citalopram | 20 mg → max often 40 mg adults (lower in elderly) | QTc warnings limit ceiling |
| Fluoxetine | 20 mg → 20–60 mg | Long half-life; fewer discontinuation jolts; long MAOI washout |
| Paroxetine | 20 mg → 20–50 mg | Anticholinergic; high discontinuation risk |
| Venlafaxine XR | 75 mg → 75–225 mg (higher specialist) | BP; short half-life discontinuation |
| Duloxetine | 30–60 mg → 60–120 mg | Pain/neuropathy niche |
| Mirtazapine | 15 mg nocte → 15–45 mg | Sedation/weight; sexual sparing relative |
| Bupropion XL | 150 mg → 150–300 mg | Seizure threshold; activating |
| Vortioxetine | 10 mg → 5–20 mg | Nausea early; multimodal profile |
| Nortriptyline | 25 mg → often 50–150 mg with levels in some settings | TCA; cardiac/anticholinergic |
| Phenelzine / tranylcypromine | Specialist start low | Diet, interactions, washouts |
| Ranges are orientation anchors for exams and guidelines teaching — product information and local protocols override memory tables.[6][11][13] |
Adequate trial. Therapeutic dose for typically 4–8 weeks (many guidelines operationalise ~6 weeks at an optimised dose) with adherence confirmed and measurement-based symptom tracking before declaring failure. Pseudo-resistance checks: wrong diagnosis (bipolar/mixed), substances, medical illness, trauma maintaining factors, under-dosing from side-effect avoidance, and non-adherence.[1][11][12]
After nonresponse: switch within or across class or augment if partial response and tolerability allows. Systematic review of switching after nonresponse supports the clinical practice of change when a true nonresponse is documented, without guaranteeing large incremental gains every time.[24][3]
Augmentation strategies
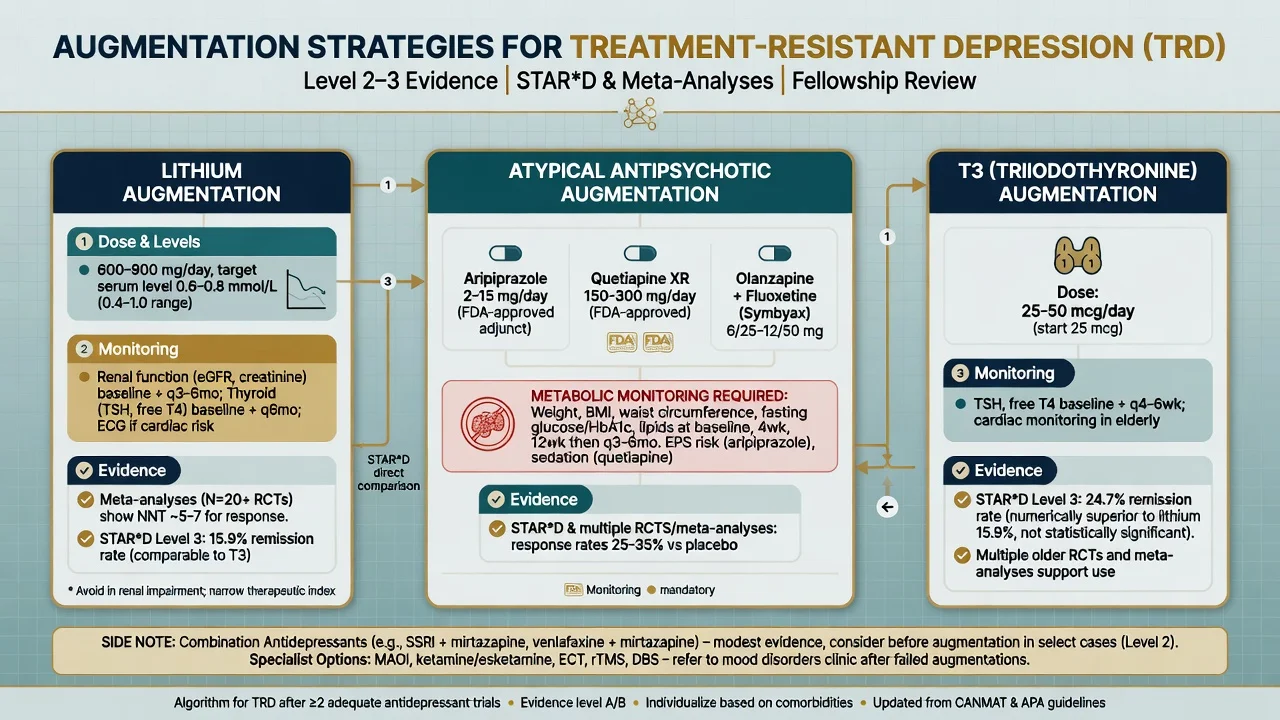
Lithium. Strongest classic pharmacological augmenter in many curricula; Crossley and Bauer meta-analyses support acceleration and augmentation effects. Target serum levels as for mood-disorder practice (commonly discussed in the 0.6–0.8 mmol/L teaching range for augmentation, individualised), with renal, thyroid, calcium, ECG and interaction vigilance.[10][4][12]
T3 (liothyronine). STAR*D compared T3 with lithium after two failed medication treatments; both are legitimate options. Typical teaching doses often 25–50 micrograms daily with thyroid monitoring and caution in cardiac disease — confirm local product guidance.[4]
Atypical antipsychotics. Meta-analysis shows efficacy as augmentation in MDD with clear tolerability costs (weight, metabolic, akathisia, sedation depending on agent). Common exam agents: aripiprazole (often start 2–5 mg), quetiapine XR (sedation/metabolic), olanzapine–fluoxetine combination in selected TRD contexts. Monitor metabolic parameters as for antipsychotic prescribing.[9][23]
Combinations. Venlafaxine plus mirtazapine appears in late STAR*D pathways; combination strategies need clear rationale and interaction review, not random polypharmacy.[5]
Switching and washouts
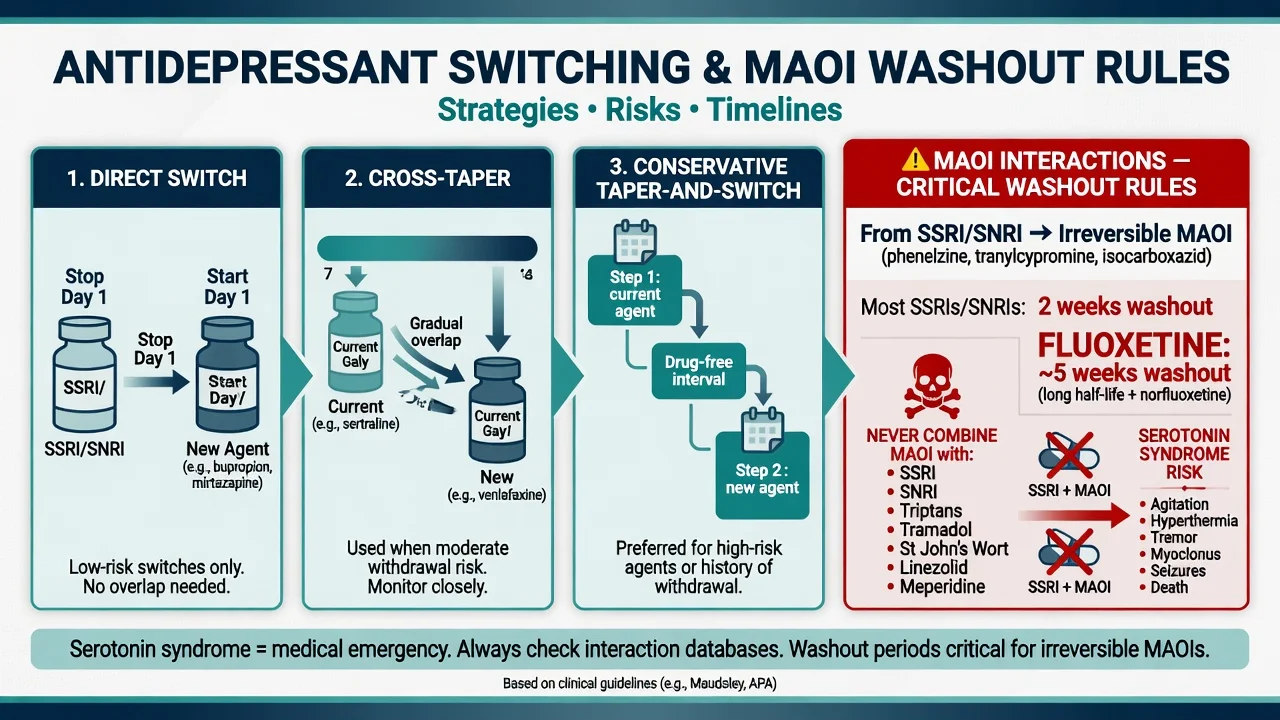
Strategies. Direct switch (similar class, stable patient), cross-taper (different profiles, withdrawal risk), or taper-stop-washout-start (mandatory thinking near MAOIs). Fluoxetine’s long half-life means prolonged serotonergic activity after cessation — critical before MAOI start.[24][15]
MAOI rules (exam red line). Do not combine irreversible MAOIs with SSRIs, SNRIs, many TCAs (especially clomipramine), tramadol, pethidine, dextromethorphan, linezolid context, or St John’s wort. Observe manufacturer and local protocol washouts (commonly 2 weeks from most serotonergic antidepressants to MAOI; about 5 weeks after fluoxetine). Reverse direction also needs washout from MAOI before starting SSRI/SNRI. RIMA (moclobemide) has different constraints but still demands interaction literacy.[5][15][11]
Monitoring
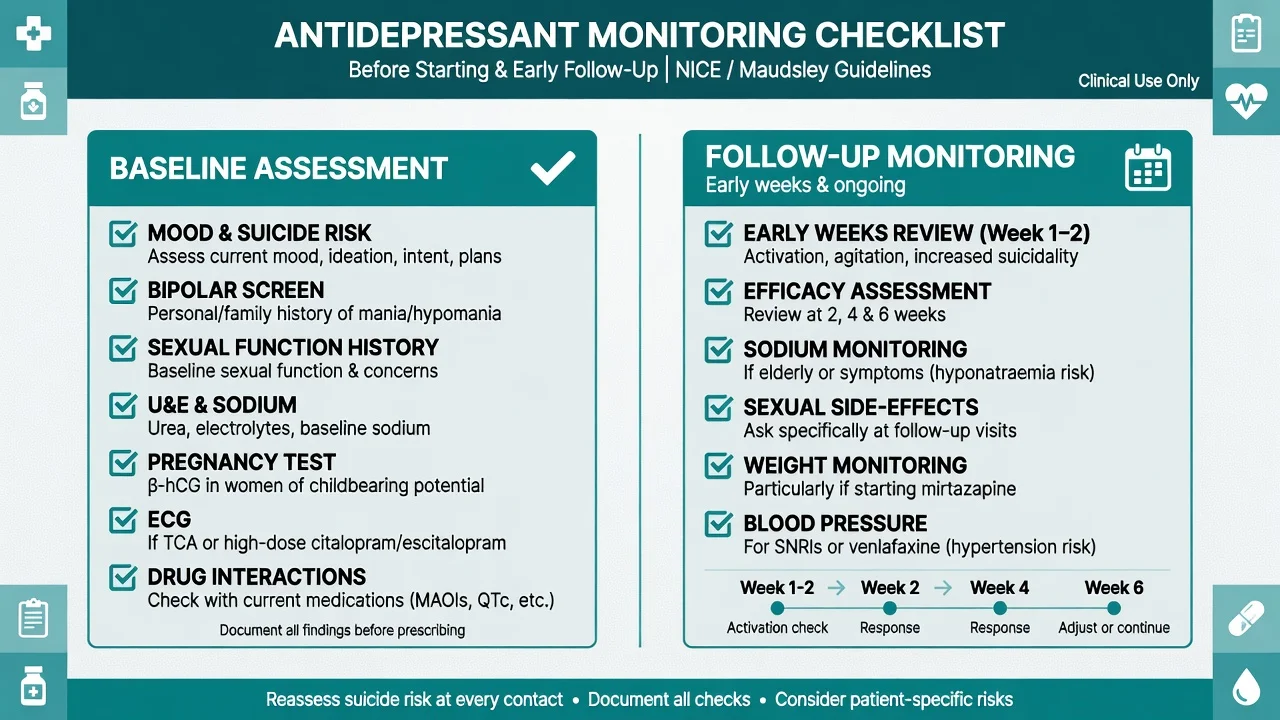
Before first dose (document): diagnosis and bipolar screen; suicide risk and means access; sexual function baseline; medical and substance history; concurrent serotonergic drugs; pregnancy potential; U&E (sodium); LFT if relevant; ECG when using TCAs or when QTc risk (citalopram/escitalopram ceilings, cardiac disease); blood pressure baseline for SNRIs.[11][12][21]
Early follow-up: review within days to 2 weeks for activation, akathisia, insomnia, and suicidality — especially under 25 and after dose increases — then efficacy and tolerability at 2–4–6 weeks with measurement-based care. Recheck sodium if older age, symptoms, or interacting drugs. Weight for mirtazapine/TCAs; BP for venlafaxine/duloxetine; metabolic labs if antipsychotic augmentation used.[17][18][2]
RANZCP 2020 mood guidelines anchor ANZ fellowship practice in formulation-based stepped care and careful antidepressant use. CANMAT 2016 and the 2023 update provide granular pharmacological line choices and augmentation ranks widely used in exams. NICE emphasises stepped care and review intensity. APA practice emphasises measurement-based care and shared decision. Thresholds and formulary differ; the exam constant is adequate trial logic plus safety monitoring, not a single global brand preference.[11][12][13]
Adverse effects and emergencies — map, not laundry list
Sexual dysfunction
- High with many SSRI/SNRI (Montejo prospective data)
- Discuss before prescribe
- Options: wait, dose reduce, switch, add bupropion where appropriate
- Mirtazapine/bupropion relatively sparing
Hyponatraemia
- SSRI/SNRI association (Movig case-control)
- Older adults, female sex, diuretics
- Confusion, falls, seizures
- Stop/switch; fluid/sodium management
Discontinuation
- Paroxetine, venlafaxine classic
- Dizziness, electric shocks, flu-like, irritability
- Taper; not 'addiction' framing
- Fluoxetine smoother stop
Toxic emergencies
- Serotonin toxicity — Hunter rules
- TCA overdose — Na channel / bicarb
- MAOI hypertensive crisis principles
- Never MAOI + SSRI improvisation
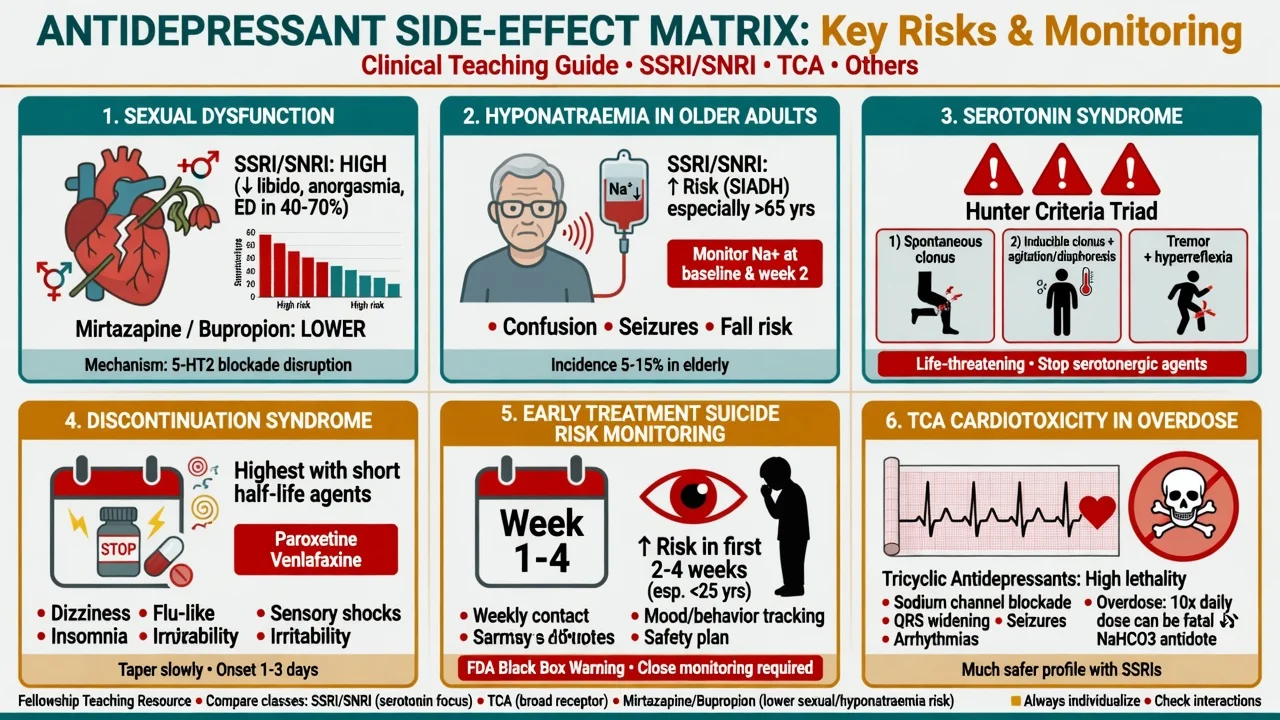
Sexual side-effects
Montejo’s prospective multicentre study of over a thousand outpatients documented high incidence of sexual dysfunction with many antidepressants — this is an adherence and quality-of-life crisis, not a delicate optional conversation. Screen at baseline and follow-up; offer management strategies rather than silence.[20]
Hyponatraemia
Case-control evidence associates antidepressant use with hyponatraemia. Highest clinical vigilance in older adults: check baseline sodium, recheck if unwell, and treat symptomatic hyponatraemia as a medical problem while revising the psychotropic plan.[21]
Serotonin syndrome (toxicity)
Clinical diagnosis. Boyer and Shannon describe the classic continuum of neuromuscular excitation, autonomic hyperactivity and altered mental status. Hunter Serotonin Toxicity Criteria improve diagnostic specificity in the presence of a serotonergic agent — spontaneous clonus; inducible clonus plus agitation or diaphoresis; ocular clonus plus agitation or diaphoresis; tremor plus hyperreflexia; or hypertonia plus temperature above 38°C plus ocular/inducible clonus (use the published decision rules precisely in exams).[14][15]
Management principles: stop serotonergic agents; ABC support; benzodiazepines for agitation; cooling; cyproheptadine considered in specialist protocols; ICU for severe hyperthermia and rigidity. Differentiate from NMS (dopamine blocker context, bradyreflexia/rigidity pattern).[15]
Discontinuation / withdrawal symptoms
Consensus recommendations describe a common, usually time-limited syndrome after abrupt stop or missed doses, worse with short half-life agents (paroxetine, venlafaxine). Educate, taper when stopping, and do not mislabel all symptoms as relapse — though true relapse also occurs and needs separate planning.[19]
Early treatment suicide risk
FDA analyses of paediatric trials found increased suicidality signal with antidepressants versus placebo in children and adolescents — the foundation of black-box warnings and close monitoring practice.[17] Adult trial meta-analysis shows age interaction: elevated suicidal behaviour/ideation signal in younger adults, with different patterns in middle and older age groups — never quote a single number as universal risk or universal protection.[18] Clinical translation: see patients more often early after start or dose increase; safety plan; involve family where appropriate; treat activation/akathisia actively.
TCA overdose
Wide-complex arrhythmia, seizures, coma — sodium bicarbonate for sodium-channel toxicity is the classic emergency medicine interface; prevent access to large TCA supplies in high-risk outpatients.[11]
Specific scenarios
Anxious depression / primary anxiety comorbidity. SSRIs and SNRIs cover both domains for many patients; start low if activation risk.[11][13]
Atypical features. Historical MAOI responsiveness remains examinable lore; modern practice still individualises, with MAOIs reserved for experienced pathways.[5][11]
Psychotic depression. Antidepressant alone is usually insufficient — antipsychotic combination and/or ECT pathways (see MDD topic).[12]
Pain. Duloxetine (and TCAs historically) for selected neuropathic/pain-depression overlap.[11]
Smoking cessation comorbidity. Bupropion dual utility where seizure risk acceptable.[3]
Bipolar depression. Antidepressant monotherapy in bipolar I is an exam fail; polarity-safe agents first (see bipolar topic).[12]
Special populations
Older adults. Start low, go slow; hyponatraemia and falls risk; drug interactions; avoid highly anticholinergic TCAs when possible.[21][12]
Youth. Elevated relative suicidality signal in paediatric analyses; fluoxetine has the strongest classic adolescent trial footprint (TADS context in MDD topic); mandatory close review and family engagement.[17]
Pregnancy and lactation. Individualised risk–benefit: untreated depression harms mother and fetus; large meta-analytic data on SSRI exposure and congenital malformations inform counselling without binary panic or denial. Prefer agents with more reproductive data when possible; coordinate perinatal psychiatry/obstetrics; never stop abruptly without a plan.[22][12]
Hepatic/renal impairment. Prefer agents with simpler kinetics; dose-adjust per product information (e.g. duloxetine hepatic caution).[11]
Prognosis and disposition
Response is typically ≥50% symptom reduction; remission is the goal because residual symptoms drive relapse. After a first episode, continue for months after remission; after recurrent illness, longer maintenance is often justified — Geddes-level evidence supports continuation pharmacology to prevent relapse.[8][1] Step up to crisis services, inpatient care, or ECT when severity, psychosis, catatonia, or suicide risk outstrip outpatient titration speed.[12]
Evidence, guidelines and controversies
Controversies to handle calmly: efficacy in mild depression (Fournier); how long to continue; when to abandon pharmacology for ECT/esketamine pathways; industry influence on ranking tables; withdrawal versus relapse framing. Answer with severity, patient values, and evidence tier — not fashion.[16][19][13]
Exam pearls
SAFE START before prescribing
SAFESTART
References
- [1]Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report Am J Psychiatry, 2006.PMID 17074942
- [2]Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice Am J Psychiatry, 2006.PMID 16390886
- [3]Rush AJ, Trivedi MH, Wisniewski SR, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression N Engl J Med, 2006.PMID 16554525
- [4]Nierenberg AA, Fava M, Trivedi MH, et al. A comparison of lithium and T(3) augmentation following two failed medication treatments for depression: a STAR*D report Am J Psychiatry, 2006.PMID 16946176
- [5]McGrath PJ, Stewart JW, Fava M, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report Am J Psychiatry, 2006.PMID 16946177
- [6]Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis Lancet, 2018.PMID 29477251
- [7]Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis Lancet, 2009.PMID 19185342
- [8]Geddes JR, Carney SM, Davies C, et al. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review Lancet, 2003.PMID 12606176
- [9]Nelson JC, Papakostas GI Atypical antipsychotic augmentation in major depressive disorder: a meta-analysis of placebo-controlled randomized trials Am J Psychiatry, 2009.PMID 19687129
- [10]Crossley NA, Bauer M Acceleration and augmentation of antidepressants with lithium for depressive disorders: two meta-analyses of randomized, placebo-controlled trials J Clin Psychiatry, 2007.PMID 17592920
- [11]Kennedy SH, Lam RW, McIntyre RS, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments Can J Psychiatry, 2016.PMID 27486148
- [12]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [13]Lam RW, Kennedy SH, Adams C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder Can J Psychiatry, 2024.PMID 38711351
- [14]Dunkley EJ, Isbister GK, Sibbritt D, et al. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity QJM, 2003.PMID 12925718
- [15]Boyer EW, Shannon M The serotonin syndrome N Engl J Med, 2005.PMID 15784664
- [16]Fournier JC, DeRubeis RJ, Hollon SD, et al. Antidepressant drug effects and depression severity: a patient-level meta-analysis JAMA, 2010.PMID 20051569
- [17]Hammad TA, Laughren T, Racoosin J Suicidality in pediatric patients treated with antidepressant drugs Arch Gen Psychiatry, 2006.PMID 16520440
- [18]Stone M, Laughren T, Jones ML, et al. Risk of suicidality in clinical trials of antidepressants in adults: analysis of proprietary data submitted to US Food and Drug Administration BMJ, 2009.PMID 19671933
- [19]Schatzberg AF, Blier P, Delgado PL, et al. Antidepressant discontinuation syndrome: consensus panel recommendations for clinical management and additional research J Clin Psychiatry, 2006.PMID 16683860
- [20]Montejo AL, Llorca G, Izquierdo JA, et al. Incidence of sexual dysfunction associated with antidepressant agents: a prospective multicenter study of 1022 outpatients J Clin Psychiatry, 2001.PMID 11229449
- [21]Movig KL, Leufkens HG, Lenderink AW, et al. Association between antidepressant drug use and hyponatraemia: a case-control study Br J Clin Pharmacol, 2002.PMID 11966666
- [22]Gao SY, Wu QJ, Sun C, et al. Selective serotonin reuptake inhibitor use during early pregnancy and congenital malformations: a systematic review and meta-analysis of cohort studies of more than 9 million births BMC Med, 2018.PMID 30415641
- [23]Zhou X, Keitner GI, Qin B, et al. Atypical Antipsychotic Augmentation for Treatment-Resistant Depression: A Systematic Review and Network Meta-Analysis Int J Neuropsychopharmacol, 2015.PMID 26012350
- [24]Bschor T, Kern H, Henssler J, et al. Switching the Antidepressant After Nonresponse in Adults With Major Depression: A Systematic Literature Search and Meta-Analysis J Clin Psychiatry, 2018.PMID 27929611