Psych · Psychopharmacology — antipsychotics
Antipsychotics
Also known as Neuroleptics · Atypical antipsychotics · Second-generation antipsychotics · Long-acting injectable antipsychotics · LAI · Dopamine antagonists
Exam-exhaustive fellowship pharmacology of antipsychotics — receptor maps, FGA vs SGA evidence (CATIE, CUtLASS, EUFEST, Leucht NMA), dosing, metabolic and EPS monitoring, LAIs, switching, TRRIP pathway to clozapine, acute adverse-effect emergencies. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Antipsychotic pharmacology is a daily viva language across FRANZCP, MRCPsych and ABPN. Examiners expect pathway maps, occupancy concepts, agent-level doses, monitoring schedules, landmark effectiveness trials, and the TRRIP door to clozapine — not brand slogans. This topic is the drug-class spine that schizophrenia, bipolar mania, agitation and clozapine topics plug into.[1][4][6]
Definition and classification
An antipsychotic is a medicine whose primary licensed psychotropic use is reduction of psychotic symptoms (and, for many agents, acute mania), acting principally through dopamine D2 receptor antagonism or partial agonism, often with additional serotonergic and other receptor effects.[7][11]
Working exam taxonomy (use deliberately): FGA (high D2 affinity pattern; EPS and prolactin more prominent — e.g. haloperidol, chlorpromazine, zuclopenthixol); SGA (5-HT2A–D2 and multi-receptor actions; metabolic liability often higher for several agents — e.g. olanzapine, quetiapine, risperidone, amisulpride, paliperidone); partial agonists (aripiprazole, brexpiprazole, cariprazine — D2 partial agonism with a different EPS/metabolic mix).[4][13]
Do not recite "atypicals are always better." CATIE and CUtLASS dismantled marketing mythology: effectiveness differences are smaller than advertised; side-effect profiles drive real-world choice.[1][2]
Mechanism — the viva core
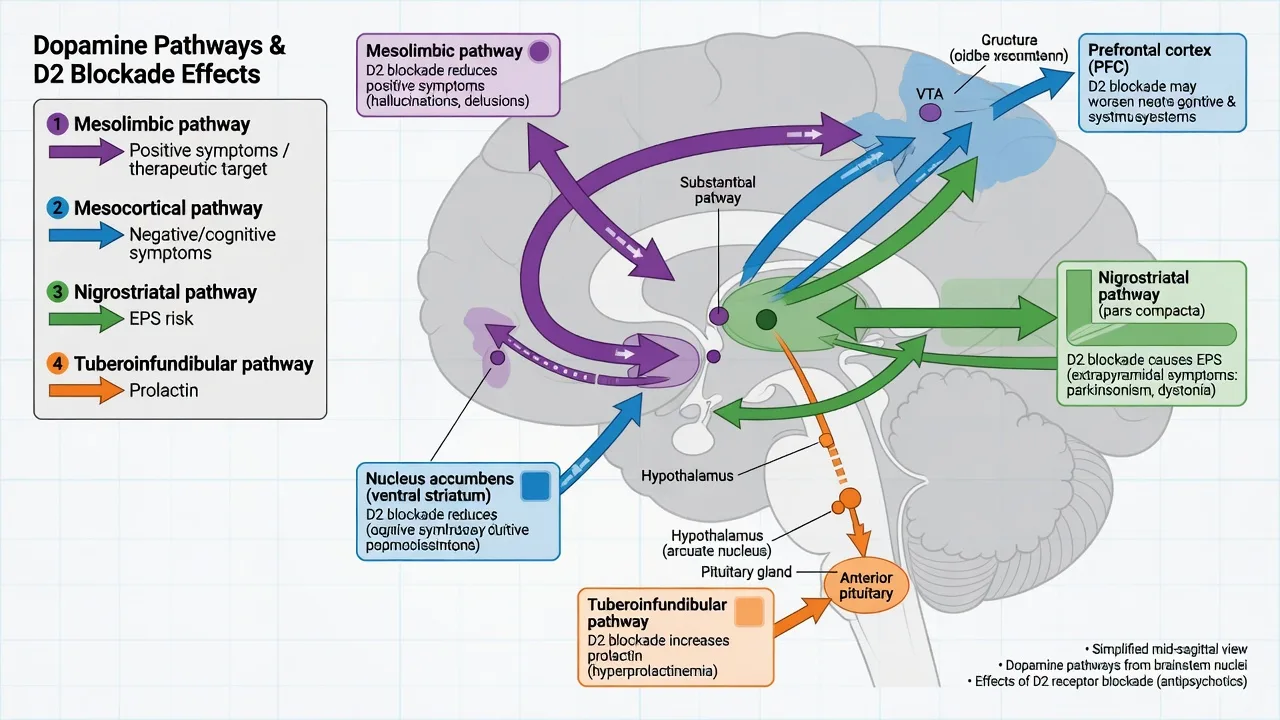
Dopamine hypothesis version III frames psychosis as convergent striatal dopamine dysregulation. Antipsychotic efficacy against positive symptoms tracks D2 occupancy in striatum; roughly 60–80% occupancy is the classic therapeutic window taught in exams, with EPS rising sharply as occupancy exceeds about 80% (agent and individual variability apply).[7]
| Pathway | Clinical correlate of D2 blockade |
|---|---|
| Mesolimbic | Therapeutic reduction of positive symptoms |
| Mesocortical | Excess blockade may worsen secondary negative/cognitive symptoms |
| Nigrostriatal | Dystonia, parkinsonism, akathisia, tardive dyskinesia risk |
| Tuberoinfundibular | Hyperprolactinaemia |
| Pathway mapping is the standard viva scaffold for efficacy versus neurological and endocrine harm.[7] |
Off-target receptors explain the rest of the table examiners love: H1 (sedation, weight), M1 (anticholinergic burden, cognitive dulling, constipation risk stacked with clozapine), alpha-1 (postural hypotension), 5-HT2C (metabolic signalling), cardiac ion channels (QTc).[4][7]
Landmark evidence every candidate must own
Trials that change viva answers
CATIE. In chronic schizophrenia, all-cause discontinuation was high across agents; olanzapine showed longer time to discontinuation for some comparisons but more weight and metabolic harm — the exam takeaway is effectiveness under real-world conditions, not pure efficacy.[1]
CUtLASS 1. Quality of life was not broadly superior for SGAs versus FGAs in people requiring a change of antipsychotic — another nail in "atypical supremacy."[2]
EUFEST. In first-episode psychosis, several SGAs had lower discontinuation than low-dose haloperidol; still, treat FEP as a special population with lower starting doses and early intervention systems, not just a drug choice.[3][8][15]
Leucht network meta-analysis. Clozapine ranks highest for efficacy among antipsychotics; other agents separate modestly on efficacy with larger separation on side-effects — use this when asked to justify choice beyond habit.[4]
Sixty years of placebo-controlled trials. Antipsychotics clearly beat placebo in acute schizophrenia; effect sizes and predictors inform realistic expectations and trial design literacy for critical appraisal stations.[11]
Mortality context. Population data (FIN11) associate long-term antipsychotic treatment, including clozapine, with lower mortality than no antipsychotic in schizophrenia cohorts — argue for treated illness, not therapeutic nihilism, while still attacking metabolic risk aggressively.[9]
Clinical use and selection algorithm
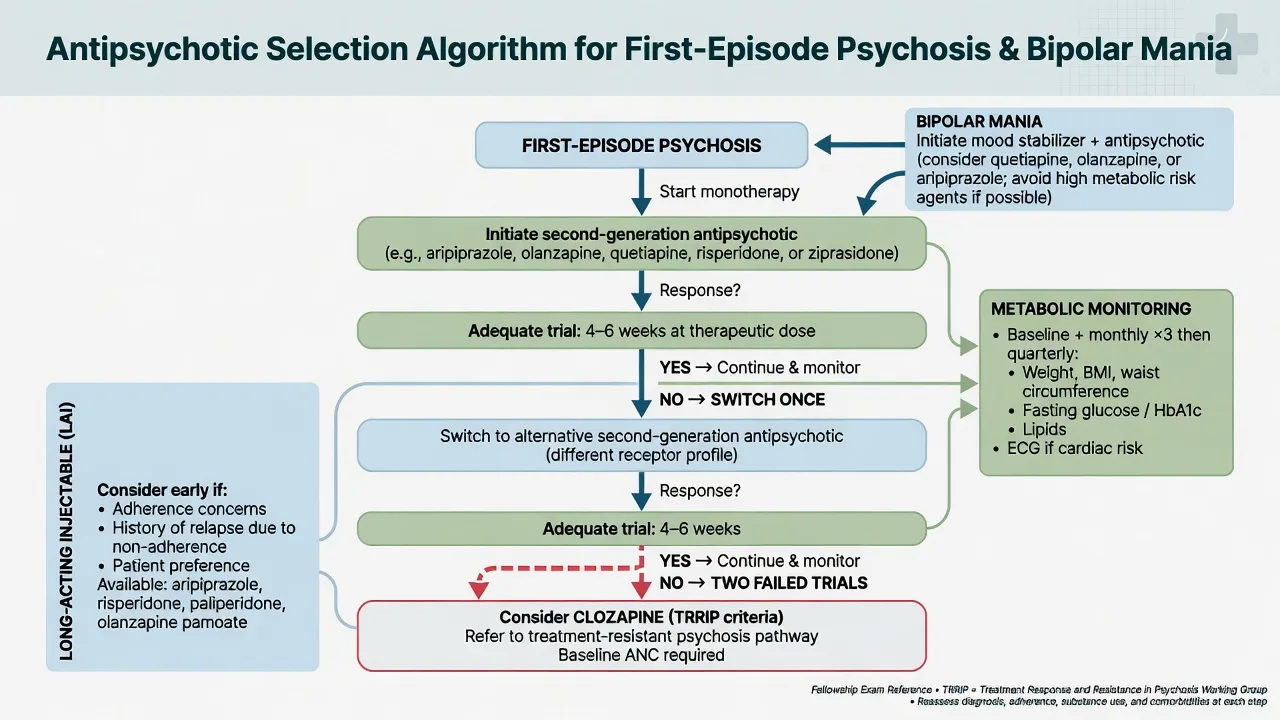
Indications you must separate: (1) schizophrenia spectrum / FEP — core indication, pair medicines with multi-element early intervention care; (2) acute mania for selected agents (e.g. olanzapine, quetiapine, risperidone, aripiprazole, asenapine — local labels differ); (3) adjunct in major depression for selected licensed agents (e.g. quetiapine XR, aripiprazole, brexpiprazole); (4) short-term behavioural disturbance only after de-escalation (see rapid tranquillisation topic).[8][14][15][4]
Choosing a first agent in FEP (exam structure): shared decision; prior response/family history; metabolic risk; EPS sensitivity; need for sedation; pregnancy potential; formulation (oral vs LAI readiness); drug–drug interactions; local formulary. Start low in FEP (e.g. aripiprazole 10 mg oral daily; risperidone 1–2 mg; olanzapine 5–10 mg) and titrate to an adequate dose for 4–6 weeks with adherence support before declaring failure. Individual product information always overrides a memory table.[3][4][8]
Adequate trial (TRRIP spirit): therapeutic dose range, sufficient duration, confirmed adherence (consider LAI or plasma level where available), and exclusion of pseudo-resistance (substance use, wrong diagnosis, intolerable under-dosing).[6]
After one failure: switch class/profile (e.g. metabolic-heavy to partial agonist or vice versa) with cross-taper planned for receptor differences. After two failures: assess for treatment-resistant schizophrenia and offer clozapine — response rates in meta-analysis support earlier, not later, use.[5][6][12]
Agent-level doses and practical notes (oral, adult)
Ranges are typical adult starting-to-usual targets; always individualise, check local product information, and use lower starts in older adults and many FEP patients.[4]
| Agent | Typical oral adult pattern | Exam monitoring emphasis |
|---|---|---|
| Haloperidol | 0.5–5 mg/day start; higher in acute settings with caution | EPS, QTc, NMS |
| Risperidone | 1–2 mg → 2–6 mg/day | Prolactin, EPS at higher doses |
| Paliperidone | Oral 3–12 mg; LAI widely used | Prolactin, renal dosing |
| Olanzapine | 5–10 mg → 10–20 mg/day | Weight, lipids, glucose; IM+BZD ban |
| Quetiapine | IR titration to 300–800 mg in psychosis/mania | Sedation, metabolic, orthostasis |
| Aripiprazole | 10–15 mg daily (FEP often 10 mg) | Akathisia; lower metabolic |
| Amisulpride | 400–800 mg/day (lower for negatives in some practice) | Prolactin, QTc |
| Clozapine | Slow titration; specialist monitoring | Neutrophils, myocarditis, constipation, seizures, levels |
| Typical adult oral ranges above are exam orientation anchors from comparative evidence and product-class teaching — always individualise and check local product information.[4][3] |
Clozapine remains the only agent with robust superiority in true TRS and has anti-suicide evidence in high-risk schizophrenia (InterSePT). Full protocol lives in the dedicated clozapine topic; do not improvise blood monitoring rules in an exam without the schedule.[5][10][12]
Long-acting injectables (LAIs)
LAIs reduce covert non-adherence and relapse risk for many patients. Exam points: discuss early (not as punishment), ensure oral tolerability first for most agents, know oral overlap requirements, injection interval, and post-injection observation rules where required (e.g. olanzapine pamoate in some jurisdictions). Offer LAI within a recovery plan that still includes psychosocial care.[8][16]
Monitoring
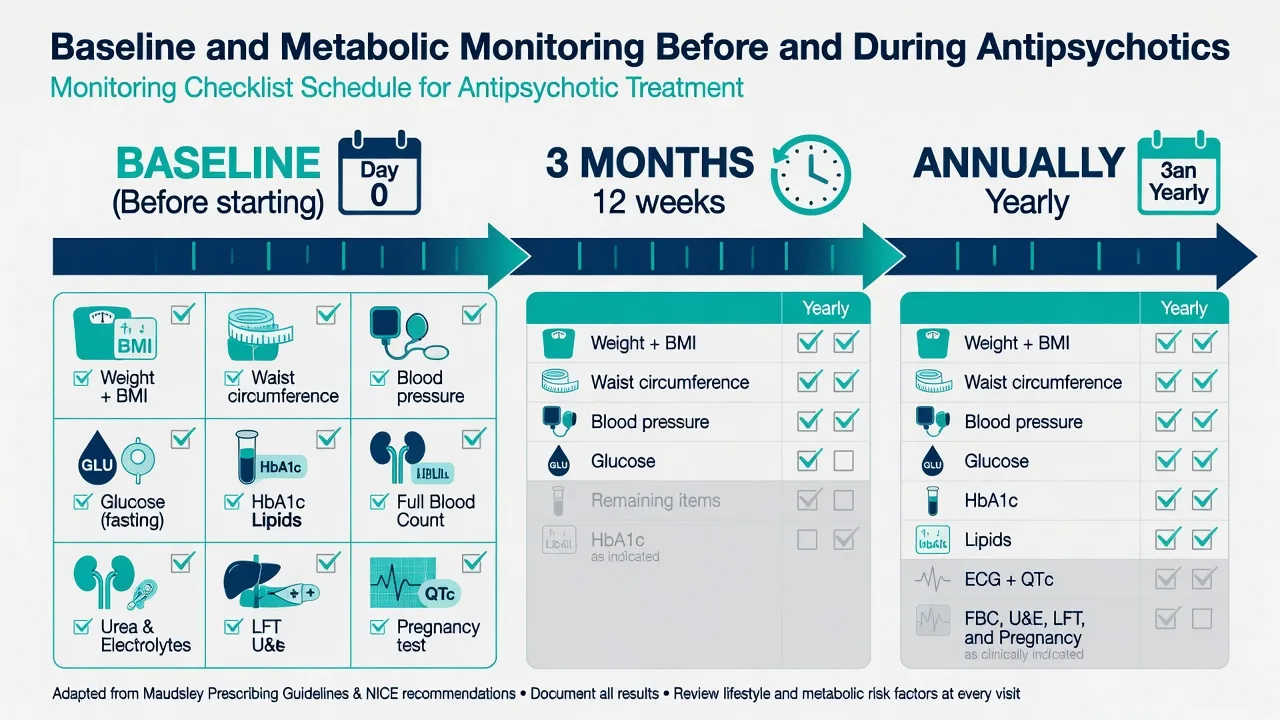
Before first dose (document): weight, BMI, waist, BP, fasting glucose or HbA1c, lipids, FBC, U&E, LFT, ECG with QTc when risk factors or high-risk agents, pregnancy test when relevant, smoking status, substance history.[4][9]
Early follow-up: review efficacy, adherence, EPS/akathisia, sedation, and weight within weeks; repeat metabolic panel at about 3 months then at least annually (sooner if rapid weight gain). Prolactin if symptoms (sexual dysfunction, amenorrhoea, galactorrhoea). Eye review historically for some low-potency agents; focus modern exams on metabolic, cardiac, neurological, and clozapine-specific harms.[1][4]
RANZCP-aligned practice emphasises cardiometabolic monitoring embedded in routine psychosis care. NICE similarly hard-wires physical health checks. APA practice emphasises measurement-based care and shared decision. Thresholds and forms differ; the exam constant is structured baseline and longitudinal physical health, not a single global lab slip.[4][9]
Adverse effects — map, not laundry list
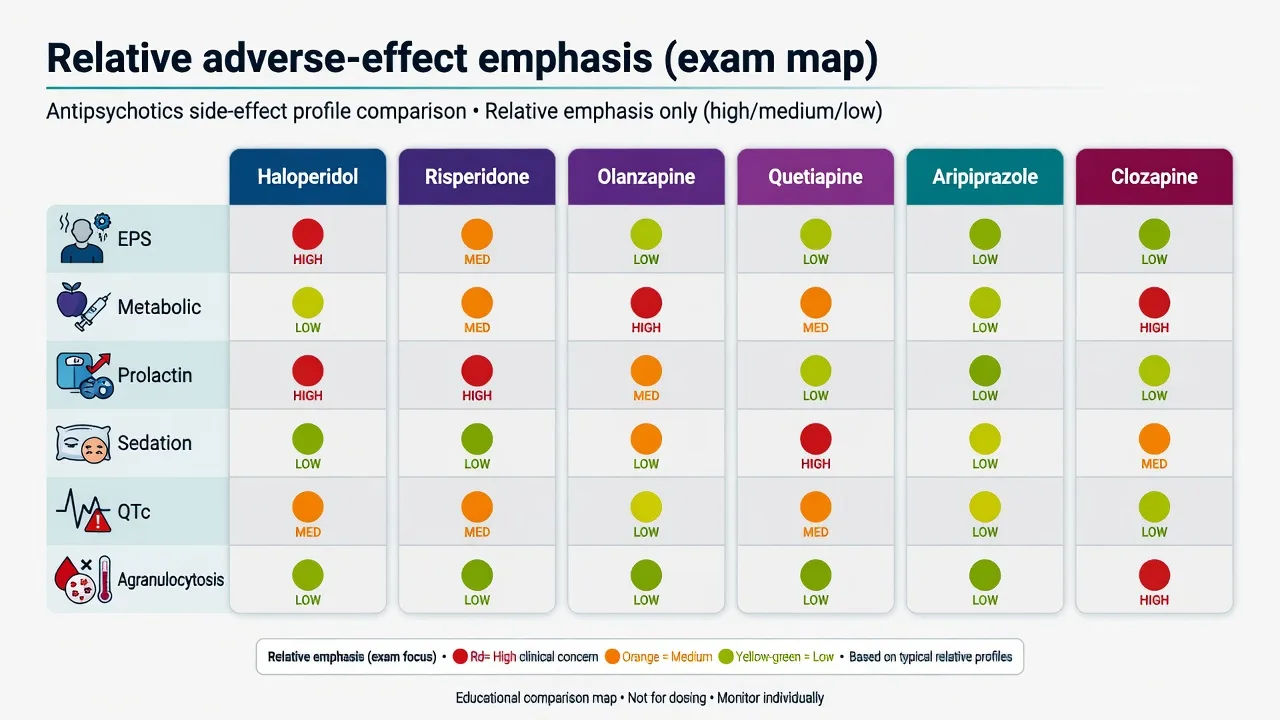
EPS / TD risk higher
- High-potency FGAs (haloperidol)
- Risperidone/paliperidone at higher doses
- Watch for acute dystonia early
- TD: late, potentially persistent
Metabolic risk higher
- Olanzapine, clozapine heavy
- Quetiapine meaningful
- Lifestyle + labs from day 0
- Switch if trajectory bad
Prolactin higher
- Risperidone, paliperidone, amisulpride, many FGAs
- Partial agonists often sparing
- Check symptoms, not only numbers
Special toxicities
- Clozapine: neutrophils, myocarditis, ileus, seizures
- QTc: ECG risk stratification
- NMS: any dopamine blocker
Acute neurological and systemic emergencies
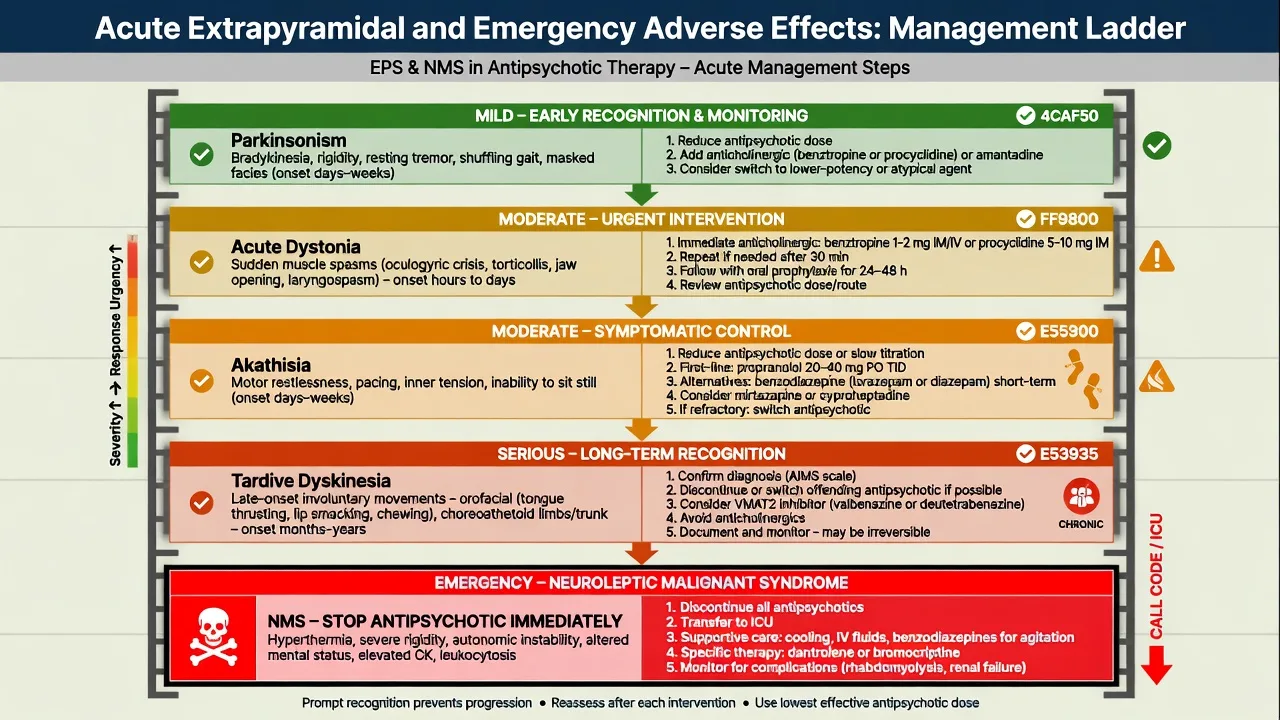
- Acute dystonia (including oculogyric crisis, laryngospasm risk): stop offending escalation; give parenteral anticholinergic (e.g. benztropine or procyclidine per local protocol); reassure; review ongoing antipsychotic.[4]
- Akathisia: reduce dose or switch; consider propranolol or short-term benzodiazepine where appropriate; do not mislabel as anxiety or agitation alone.[4]
- Parkinsonism: reduce dose, switch to lower-EPS agent, limited anticholinergic use (cognitive cost).
- Tardive dyskinesia: prevention by lowest effective dose and justified duration; review VMAT2 inhibitors where available/indicated; document AIMS-style surveillance in long-term care.
- NMS: rigidity, fever, autonomic instability, altered consciousness, raised CK — stop antipsychotic, supportive/ICU care, exclude infection and serotonin syndrome; specialist management.[4]
Special populations
Older adults. Start low, go slow; falls, QTc, anticholinergic burden, and stroke risk warnings in dementia-related psychosis demand extreme caution and non-drug strategies first.[4]
Pregnancy and lactation. Individualised risk–benefit; untreated psychosis also harms. Prefer agents with more reproductive data when possible; coordinate obstetric psychiatry. Detail sits with the pregnancy psychopharmacology topic.[4]
Parkinson disease psychosis. Avoid high-potency D2 blockers; quetiapine or clozapine are the classic exam answers when an antipsychotic is unavoidable, alongside reviewing precipitating meds.[4]
Youth. Lower starts, metabolic vigilance, family engagement, early intervention framing.[3][8]
Psychosocial care is not optional
Medicines without psychosocial intervention under-perform for relapse prevention. Family intervention, CBTp access, supported employment and adherence support belong in the same plan as the prescription — network meta-analysis supports multi-element psychosocial packages for relapse prevention.[16][14][15]
Switching, polypharmacy and deprescribing
Prefer monotherapy. Cross-taper when receptor profiles differ (especially when stopping clozapine or anticholinergic-heavy agents). Document target regimen and review date. After sustained remission in FEP, maintenance duration is shared decision with high relapse risk if stopped early; multi-episode illness usually needs longer prevention. Never strip clozapine casually.[6][11]
Evidence, guidelines and controversies
Controversies to handle calmly: when to start LAIs; how early to offer clozapine; antipsychotic use in dementia; polypharmacy for "residual negatives"; antidepressant co-prescription in schizophrenia. Answer with evidence tier, risk, and patient values — not fashion.[6][12]
Exam pearls
PREDICT harm domains
PREDICT
References
- [1]Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia N Engl J Med, 2005.PMID 16172203
- [2]Jones PB, Barnes TR, Davies L, et al. Randomized controlled trial of the effect on Quality of Life of second- vs first-generation antipsychotic drugs in schizophrenia: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1) Arch Gen Psychiatry, 2006.PMID 17015810
- [3]Kahn RS, Fleischhacker WW, Boter H, et al. Effectiveness of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: an open randomised clinical trial Lancet, 2008.PMID 18374841
- [4]Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis Lancet, 2013.PMID 23810019
- [5]Kane JM, Honigfeld G, Singer J, et al. Clozapine in treatment-resistant schizophrenics Psychopharmacol Bull, 1988.PMID 3290950
- [6]Howes OD, McCutcheon R, Agid O, et al. Treatment-Resistant Schizophrenia: Treatment Response and Resistance in Psychosis (TRRIP) Working Group Consensus Guidelines on Diagnosis and Terminology Am J Psychiatry, 2017.PMID 27919182
- [7]Howes OD, Kapur S The dopamine hypothesis of schizophrenia: version III--the final common pathway Schizophr Bull, 2009.PMID 19325164
- [8]Kane JM, Robinson DG, Schooler NR, et al. Comprehensive Versus Usual Community Care for First-Episode Psychosis: 2-Year Outcomes From the NIMH RAISE Early Treatment Program Am J Psychiatry, 2016.PMID 26481174
- [9]Tiihonen J, Lönnqvist J, Wahlbeck K, et al. 11-year follow-up of mortality in patients with schizophrenia: a population-based cohort study (FIN11 study) Lancet, 2009.PMID 19595447
- [10]Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT) Arch Gen Psychiatry, 2003.PMID 12511175
- [11]Leucht S, Leucht C, Huhn M, et al. Sixty Years of Placebo-Controlled Antipsychotic Drug Trials in Acute Schizophrenia: Systematic Review, Bayesian Meta-Analysis, and Meta-Regression of Efficacy Predictors Am J Psychiatry, 2017.PMID 28541090
- [12]Siskind D, Siskind V, Kisely S Clozapine Response Rates among People with Treatment-Resistant Schizophrenia: Data from a Systematic Review and Meta-Analysis Can J Psychiatry, 2017.PMID 28655284
- [13]Davis JM, Chen N, Glick ID A meta-analysis of the efficacy of second-generation antipsychotics Arch Gen Psychiatry, 2003.PMID 12796218
- [14]Bertelsen M, Jeppesen P, Petersen L, et al. Five-year follow-up of a randomized multicenter trial of intensive early intervention vs standard treatment for patients with a first episode of psychotic illness: the OPUS trial Arch Gen Psychiatry, 2008.PMID 18606949
- [15]Correll CU, Galling B, Pawar A, et al. Comparison of Early Intervention Services vs Treatment as Usual for Early-Phase Psychosis: A Systematic Review, Meta-analysis, and Meta-regression JAMA Psychiatry, 2018.PMID 29800949
- [16]Bighelli I, Rodolico A, García-Mieres H, et al. Psychosocial and psychological interventions for relapse prevention in schizophrenia: a systematic review and network meta-analysis Lancet Psychiatry, 2021.PMID 34653393