Psych · Psychopharmacology — anxiolytics and hypnotics
Anxiolytics and hypnotics
Also known as Benzodiazepines · Z-drugs · Sedative-hypnotics · Buspirone · Pregabalin anxiety · Hydroxyzine · Melatonin · Hypnotics · Anxiolytic pharmacology
Exam-exhaustive fellowship psychopharmacology of anxiolytics and hypnotics — benzodiazepines and Z-drugs (GABA-A PAM, half-life maps, short-term use only), buspirone, pregabalin, hydroxyzine, melatonin; dependence risk, structured taper principles, elderly falls and Beers criteria, opioid/alcohol interactions, guideline deltas (BAP, WFSBP, AASM, Canadian BRZA, EMPOWER). FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship viva language is concrete: half-life maps, agent-level doses, written exit plans, Beers-listed elderly harm, and when not to reach for alprazolam. Long-term anxiety control is SSRI/SNRI plus psychological therapy; GABAergic drugs are bridges, crisis tools, or specialised exceptions — not lifestyle maintenance.[13][14][5]
Definition and classification
An anxiolytic reduces pathological anxiety; a hypnotic promotes sleep onset or maintenance. Many GABA-A modulators do both in a dose-dependent way. Dependence-capable sedative-hypnotic-anxiolytic prescribing is a public-health and exam problem: high use, especially in older adults, with limited long-term benefit for primary insomnia.[5][26][7]
| Class | Core mechanism | Core agents (examples) | Exam emphasis |
|---|---|---|---|
| Benzodiazepines | GABA-A positive allosteric modulators (PAM) | Diazepam, lorazepam, oxazepam, temazepam, alprazolam, clonazepam | Half-life; short-term use; taper; LOT in liver disease |
| Z-drugs | GABA-A BZ-site agonists (hypnotic-biased teaching) | Zolpidem, zopiclone/eszopiclone, zaleplon | Still dependence-forming; elderly/driving risk |
| Buspirone | 5-HT1A partial agonist | Buspirone | Delayed onset; not BZD withdrawal cover |
| Pregabalin | α2δ voltage-gated Ca channel ligand | Pregabalin | GAD RCTs; dizziness/oedema; misuse vigilance |
| Hydroxyzine | H1 antagonist (plus other receptor actions) | Hydroxyzine | Non-GABAergic anxiolysis; anticholinergic/sedation load |
| Melatonin | MT1/MT2 agonists | Melatonin (and agonists elsewhere) | Modest sleep-onset effect; circadian niche |
| Class maps by mechanism organise exam answers better than marketing generations.[1][13][28] |
Classification by mechanism and half-life beats brand lists in the exam room.[1][13][28]
Mechanisms — viva core
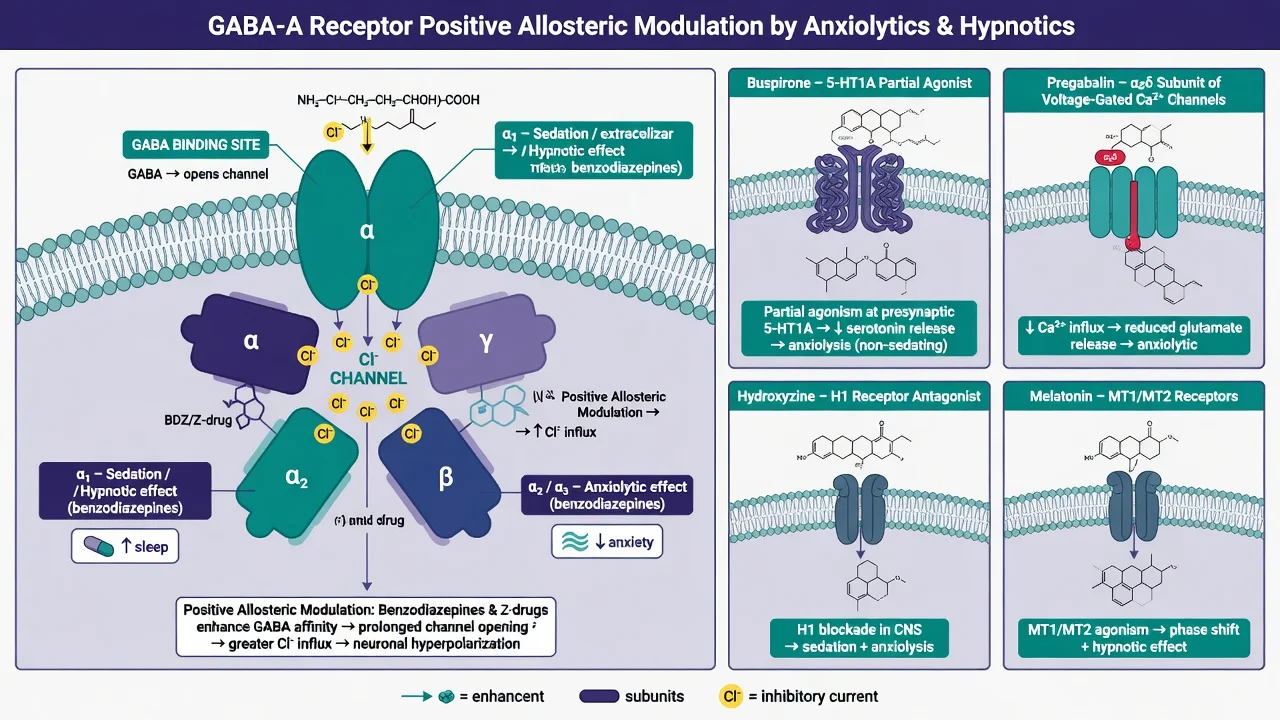
Benzodiazepines. Bind the interface of α/γ subunits of GABA-A receptors, increasing frequency of chloride channel opening when GABA is present — positive allosteric modulation, not direct agonists. Teaching model: α1-rich circuits lean sedation/amnesia/anticonvulsant effects; α2/3 lean anxiolysis; α5 relates to cognitive effects. Tolerance develops faster to sedation/hypnosis than to anxiolysis; withdrawal produces rebound hyperexcitability (anxiety, insomnia, autonomic arousal, seizures).[1][3][5]
Z-drugs. Chemically non-benzodiazepine but act at the BZ site of GABA-A receptors with relative α1 preference in teaching narratives. They are not free of dependence, complex sleep behaviours, falls, or driving impairment. Toxicological reviews emphasise residual CNS depression and performance risk.[28][7][1]
Buspirone. 5-HT1A partial agonism; anxiolytic effect is delayed (often framed as 2–4 weeks). No GABA-A PAM activity — cannot substitute for benzodiazepines in withdrawal. Cochrane azapirone evidence supports efficacy versus placebo in GAD with a different adverse-effect profile from benzodiazepines.[22][13]
Pregabalin. Binds α2δ subunit of voltage-gated calcium channels, reducing excitatory neurotransmitter release. Multiple placebo-controlled GAD trials (including comparisons with alprazolam) support anxiolytic efficacy; expect dizziness, somnolence, weight gain/oedema, and growing concern about misuse in vulnerable populations.[17][18][19]
Hydroxyzine. Histamine H1 antagonism produces sedation and anxiolysis without the classical benzodiazepine dependence pathway. A three-month double-blind GAD study and Cochrane review support a role, limited by anticholinergic burden and sedation — especially in older adults.[20][21]
Melatonin. MT1/MT2 agonism with modest effects on sleep latency and total sleep time in meta-analyses — useful circadian/insomnia adjunct framing, not a high-potency hypnotic substitute for CBT-I.[23][24][16]
Epidemiology and harm landscape
Benzodiazepine exposure is common in population datasets; US analyses show substantial use with concentration in older adults — exactly the group with the worst risk–benefit ratio for sedative-hypnotics.[26][6] Meta-analysis in older people with insomnia found sedative-hypnotics improve sleep modestly but increase adverse cognitive and psychomotor events, including falls risk framing used across geriatrics curricula.[7] Concurrent prescription opioids and benzodiazepines associate with overdose in large retrospective analyses — a non-negotiable interaction exam pearl.[25] Observational work also links anxiolytic/hypnotic prescriptions with mortality hazards; treat long-term automatic renewals as a quality and safety problem, not neutral maintenance.[5]
Half-life map and agent selection (benzodiazepines)
| Pattern | Examples | Clinical implication |
|---|---|---|
| Ultra-short / short onset | Midazolam, triazolam (context) | Procedural; rebound/withdrawal can be sharp |
| Short–intermediate | Alprazolam, lorazepam, oxazepam, temazepam | Alprazolam: high-potency, misuse and interdose anxiety risk |
| Long (+ active metabolites) | Diazepam, clonazepam, chlordiazepoxide | Smoother taper vehicle; accumulation in elderly/hepatic disease |
| Half-life drives withdrawal tempo and taper vehicle choice.[1][2][3] |
LOT teaching (hepatic impairment): prefer lorazepam, oxazepam, temazepam — conjugation pathways with fewer active oxidative metabolites — when liver disease is relevant.[2][1]
Typical adult oral orientation anchors (always check current product information; lower starts in older adults; individualise): dose ranges below are teaching scaffolds from clinical sources and guidelines, not a substitute for local product information.[2][13][15]
| Agent | Typical adult oral pattern | Notes |
|---|---|---|
| Diazepam | 2–5 mg as needed or divided; specialist higher in withdrawal protocols | Long; taper vehicle |
| Lorazepam | 0.5–1 mg PRN/scheduled short courses | Intermediate; useful in hepatic disease |
| Oxazepam | 7.5–15 mg short courses | Short–intermediate; LOT |
| Temazepam | 10 mg nocte short courses (some use 20 mg) | Hypnotic niche; LOT |
| Alprazolam | 0.25–0.5 mg short-term if used at all | High-potency short-acting — misuse and hard taper |
| Clonazepam | 0.25–0.5 mg (anxiety/seizure contexts) | Long; accumulation |
| Zolpidem | 5–10 mg nocte short-term (5 mg older adults) | Complex sleep behaviours; residual impairment |
| Zopiclone | 3.75–7.5 mg nocte short-term | Metallic taste; residual sedation |
| Buspirone | 5 mg two–three times daily → often 15–30 mg/day total in divided doses | Delayed onset; no withdrawal cover |
| Pregabalin | 75 mg twice daily → commonly 150–300 mg/day in divided doses (max per label/context) | Renal adjust; misuse vigilance |
| Hydroxyzine | 25–50 mg up to 3–4 times daily short-term anxiety contexts (label varies) | Anticholinergic/sedation |
| Melatonin | Often 2–5 mg nocte (formulations vary widely) | Modest effect size |
| Ranges are orientation anchors for exams — product information and local protocols override memory tables.[2][13][15][17][20] |
Dose tables are exam orientation, not a substitute for local product information.[2][13][15][17][20]
When short-term GABA cover is justified
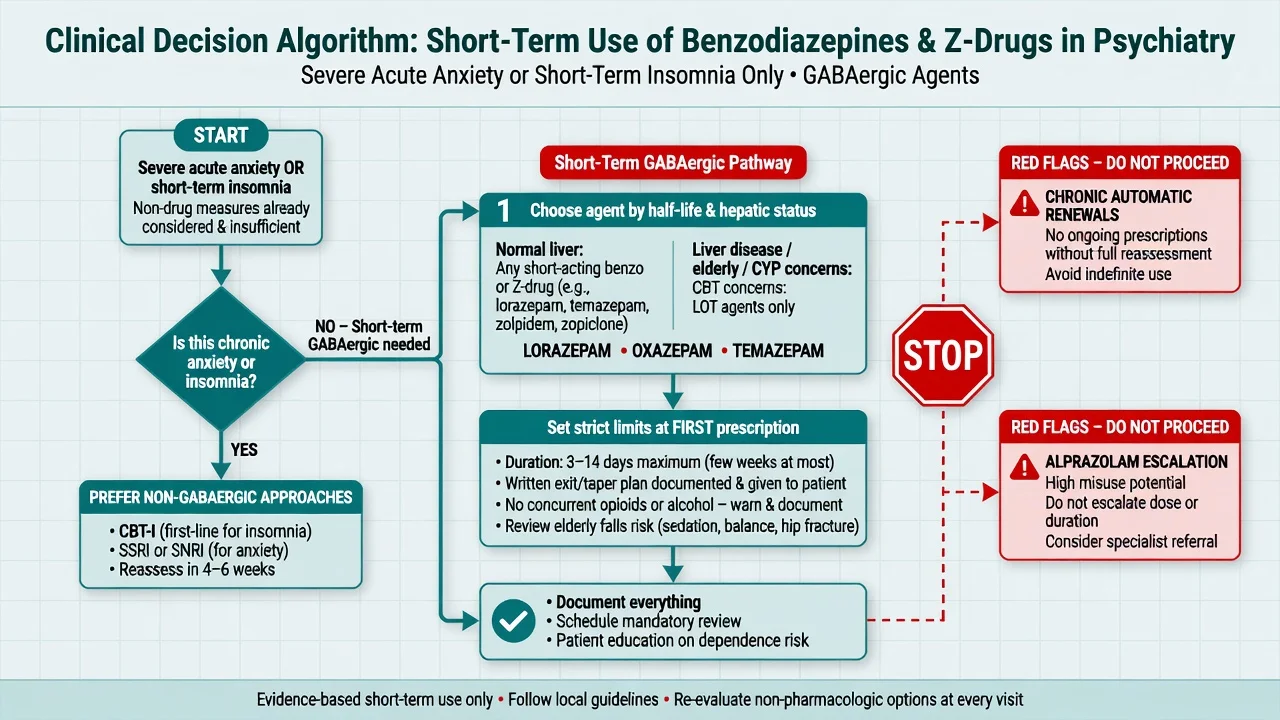
Legitimate short-term contexts (exam structure): severe acute anxiety or panic bridging while an SSRI/SNRI is started; time-limited severe insomnia after stimulus control/sleep hygiene and when CBT-I access is delayed; alcohol withdrawal protocols (owned by addiction topics); procedural sedation/agitation pathways (owned by emergency topics); selected specialist indications (e.g. catatonia adjunct — pointer). BAP anxiety guidance places SSRIs/SNRIs and psychological therapies as durable treatments; benzodiazepines are not the long-term default for GAD/panic.[13][14]
Insomnia: AASM pharmacologic guidelines and BAP sleep consensus prioritise behavioural treatment; hypnotic medicines, if used, are adjunctive and time-limited, not indefinite renewals.[15][16]
Non-GABAergic options for anxiety when tablets are needed without benzodiazepine dependence pathway (buspirone, pregabalin, hydroxyzine as examined alternatives to chronic GABA cover):
- Buspirone — GAD evidence as azapirone class; delayed onset; good for patients who cannot risk GABAergic dependence if they can wait weeks.[22]
- Pregabalin — multiple positive GAD RCTs including fixed-dose and alprazolam comparator designs.[17][18][19]
- Hydroxyzine — short-to-medium term symptomatic anxiolysis with H1 mechanism; Cochrane supports limited but real efficacy data.[20][21] Non-GABAergic choices still need indication, dose limits, and monitoring — they are not automatic free passes.[13][22][17]
Benzodiazepines
- Rapid anxiolysis/sedation
- Dependence and withdrawal seizures
- Falls, cognition, RTAs
- Short-term bridge only for primary anxiety
Z-drugs
- Hypnotic niche
- Still GABA-A BZ-site agonists
- Complex sleep behaviours; driving risk
- Beers-listed avoid in older adults
Buspirone / hydroxyzine
- No classic BZD withdrawal cover (buspirone)
- Delayed (buspirone) vs faster sedation (hydroxyzine)
- Anticholinergic load with hydroxyzine
- Useful non-GABAergic options
Pregabalin / melatonin
- Pregabalin: GAD RCT support
- Renal dosing; misuse vigilance
- Melatonin: modest sleep latency benefit
- Neither replaces CBT-I for chronic insomnia
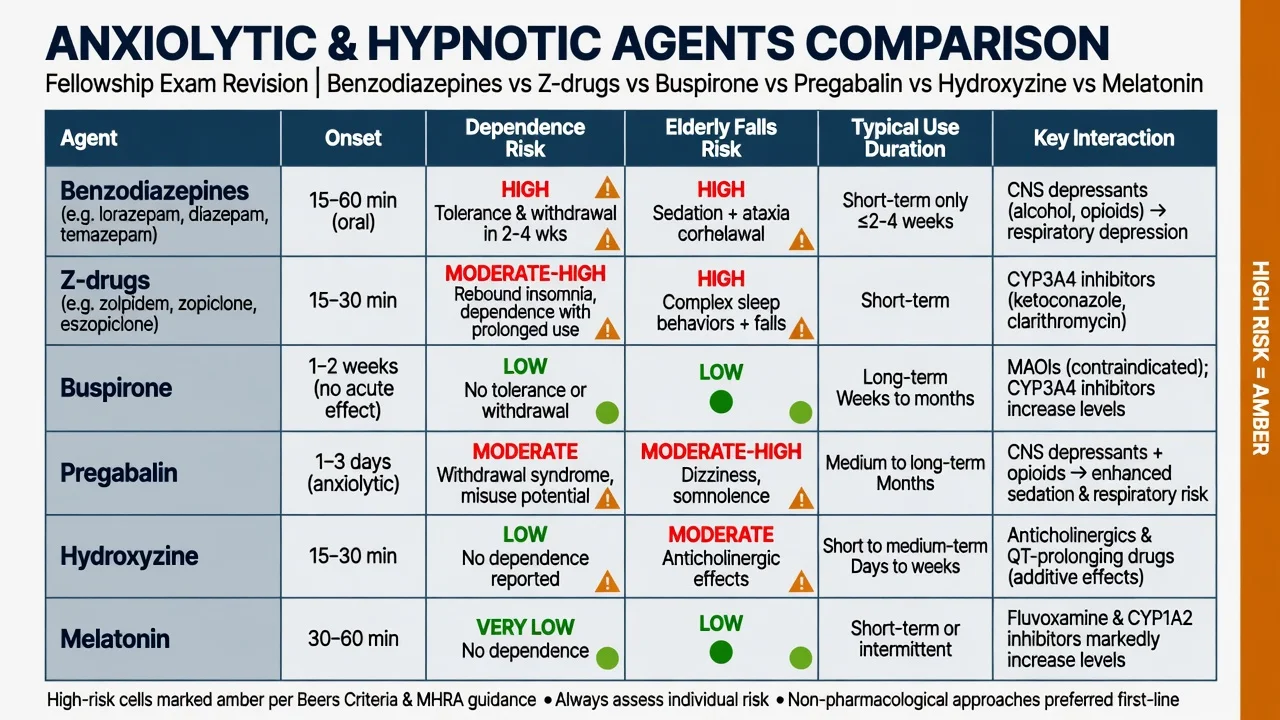
Class comparison for viva: mechanism, dependence risk, and elderly harm before brand preference.[1][7][13]
Dependence risk, taper, and deprescribing
Physiological dependence (tolerance + withdrawal) can occur with therapeutic doses after continuous use; sedative/hypnotic/anxiolytic use disorder is the full behavioural syndrome (covered in depth in the benzodiazepine-dependence topic). High-potency short-acting agents, higher doses, longer duration, prior substance use disorder, and multiple prescribers raise risk.[1][3][2]
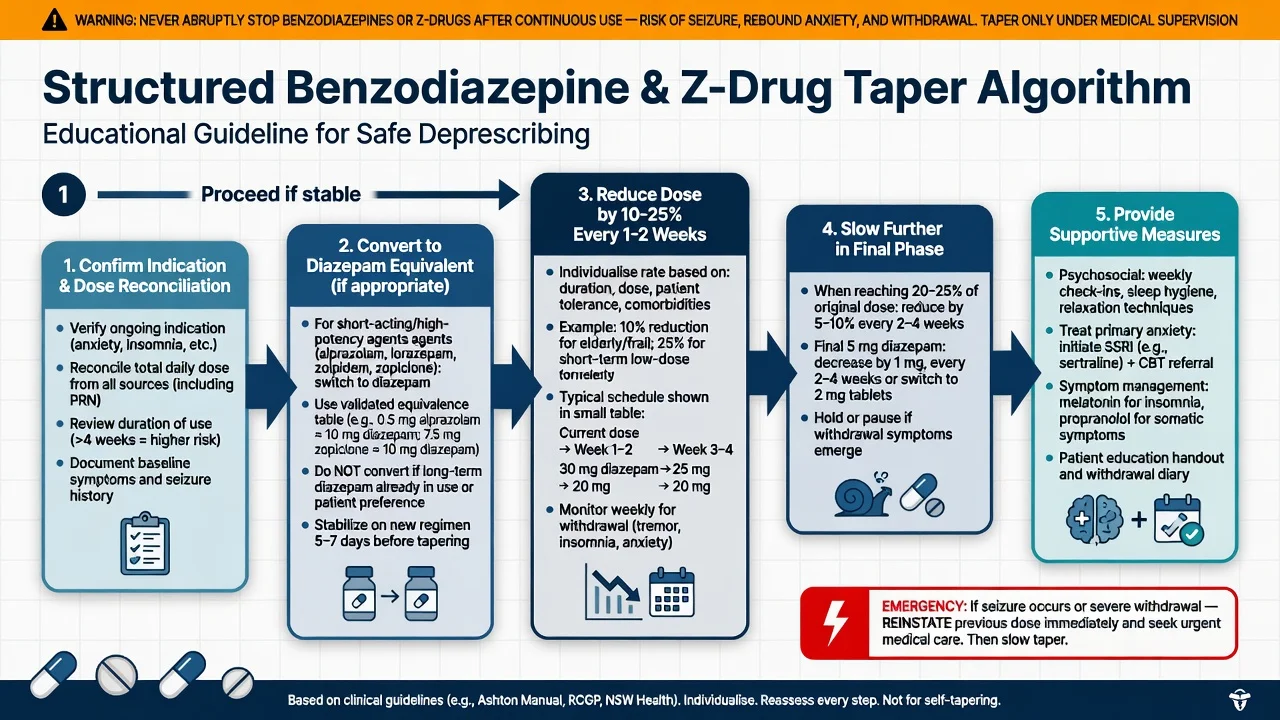
Taper principles (must-know):
- Confirm actual dose (prescribed vs taken), agent, duration, co-use of alcohol/opioids/gabapentinoids.
- Prefer gradual dose reduction; convert short-acting high-potency agents to a longer agent (often diazepam equivalents) when interdose withdrawal or complex polypharmacy confounds the taper.
- Common teaching scaffold: reduce by about 10–25% of the daily dose every 1–2 weeks (sometimes slower), with smaller steps in the final phase; symptom-triggered pauses beat macho schedules.
- If seizures or severe withdrawal emerge: reinstate adequate GABA cover, then restart a slower taper — medical emergency pathway as needed.
- Treat the underlying anxiety/insomnia with SSRI/SNRI, CBT/CBT-I, and sleep hygiene rather than endless GABA substitution.[1][3][4][12]
Meta-analysis supports structured discontinuation strategies over abrupt advice alone.[4] Psychosocial interventions help harmful use/dependence pathways; pharmacological adjuncts for discontinuation have mixed Cochrane support — do not invent a miracle taper pill.[10][11] EMPOWER showed direct patient education can reduce inappropriate long-term benzodiazepine use in older adults; Canadian BRZA deprescribing guidance operationalises shared decision and tapering in primary care-style settings.[8][9]
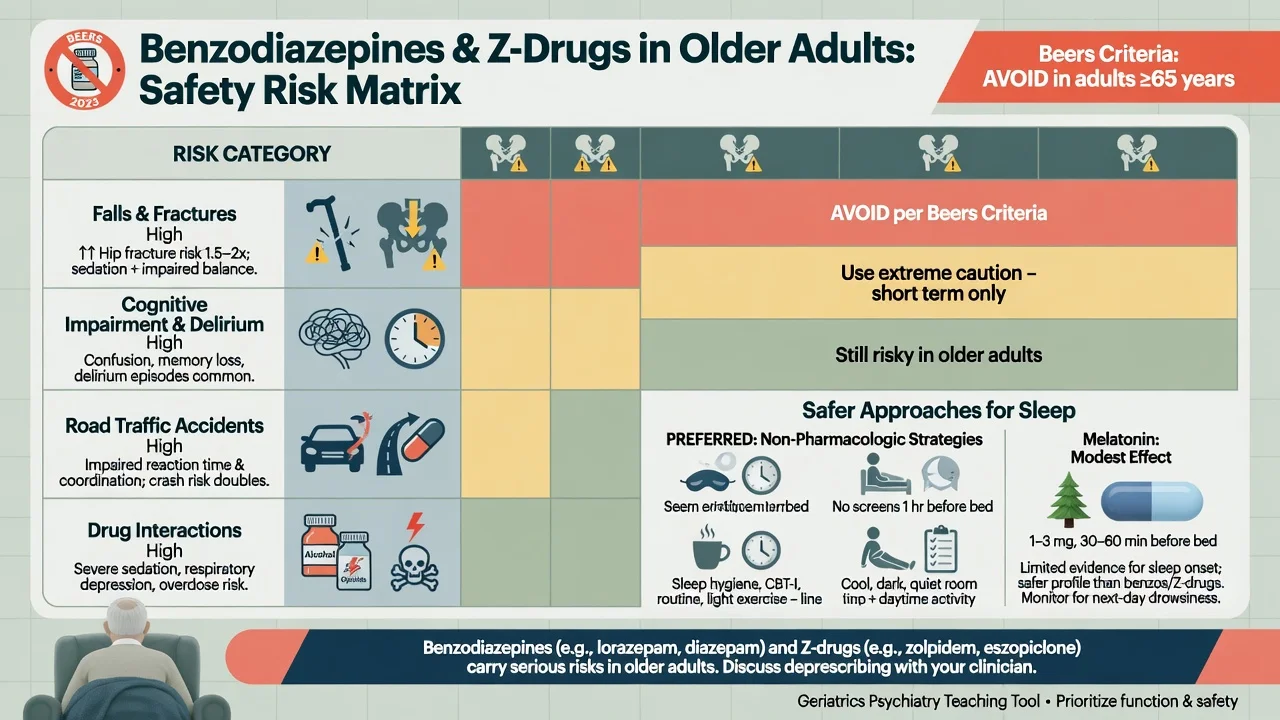
Elderly patients — falls, cognition, Beers
In older adults, benzodiazepines and Z-drugs associate with falls, fractures, cognitive impairment, delirium risk, and motor vehicle accidents. Glass meta-analysis quantified unfavourable risk–benefit for sedative-hypnotics in older people with insomnia; Markota reviews clinical dangers and alternatives; AGS Beers Criteria continue to list these agents as potentially inappropriate medications in older adults.[7][6][27] Prefer non-drug sleep strategies, treat depression/pain/nocturia causes of insomnia, and if medicine is unavoidable use the lowest dose for the shortest time with falls precautions — melatonin is a modest option, not a miracle.[23][16]
Interactions and overdose
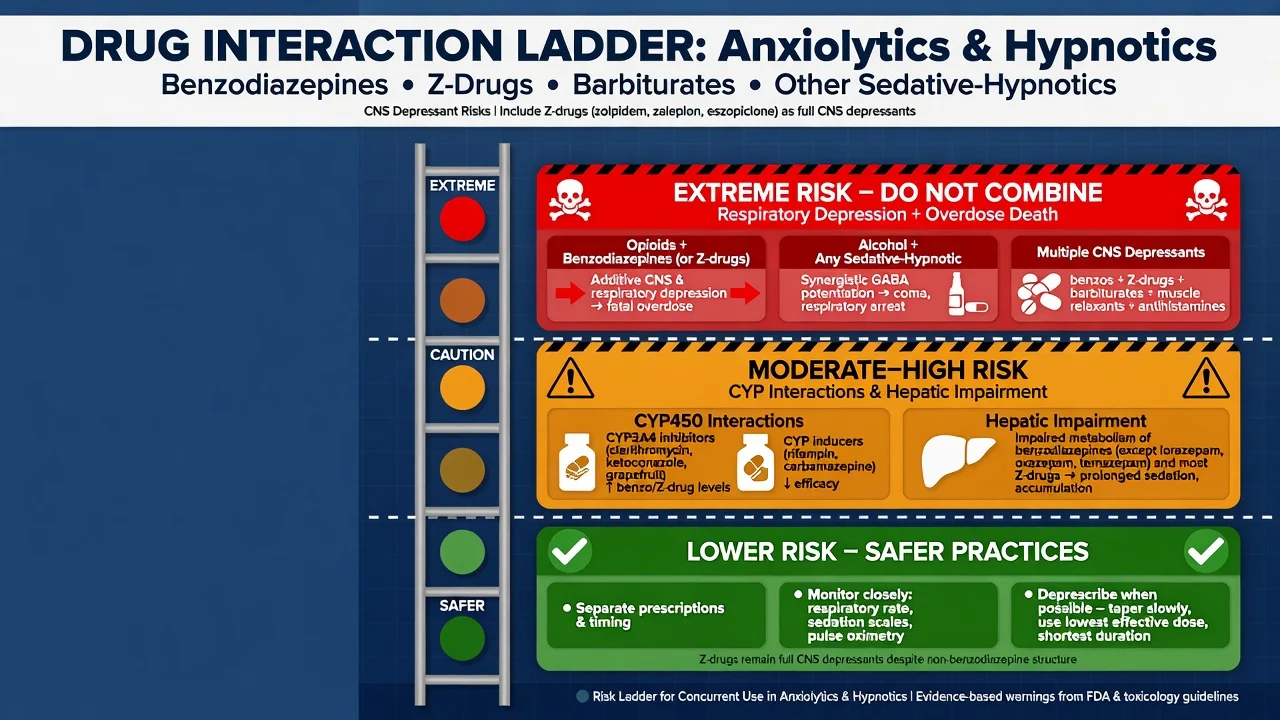
Critical combinations: opioids + benzodiazepines (overdose association in large data); alcohol + any sedative-hypnotic; stacked CNS depressants (antipsychotics, gabapentinoids, sedating antidepressants).[25][2][5]
Overdose management principles: airway and ventilation first; supportive care; flumazenil only in highly selected pure iatrogenic settings — can precipitate seizures in chronic users or mixed overdoses and is not a routine antidote. Naloxone for suspected opioid co-ingestion does not reverse benzodiazepine effects.[1][28]
Monitoring and shared decision
Before first GABAergic prescription: substance history; alcohol/opioid status; falls and driving risk; occupation (machinery); pregnancy potential; cognitive baseline; prior withdrawal seizures; pharmacy reconciliation; capacity and goals; written duration and exit plan.[2][5]
Early review: efficacy, sedation, falls, confusion, complex sleep behaviours (Z-drugs), dose escalation, multiple prescribers. If still needed beyond a short course, re-diagnose the maintaining problem rather than renew by default.[15][28]
Numbers that stick in viva
These anchors compress Glass, Sun, EMPOWER, and taper teaching into viva-ready fragments.[7][25][8][1][22]
Special populations
Pregnancy/lactation. Avoid routine benzodiazepines; if used near term, anticipate neonatal floppy infant and withdrawal syndromes — individualised risk–benefit with obstetric liaison. Prefer non-drug anxiety/insomnia care and pregnancy-compatible antidepressants when indicated for underlying disorders.[13]
Youth. Avoid chronic benzodiazepines for anxiety; first-line psychological therapies and SSRI pathways per anxiety guidance.[13][14]
Hepatic disease. LOT agents; avoid long-acting oxidative metabolites when possible.[2]
Renal impairment. Adjust pregabalin; sedation risk rises with accumulation of many CNS drugs.[17]
Dementia/delirium. Benzodiazepines often worsen confusion and falls — not first-line behavioural management (see delirium and BPSD topics).[6][27]
Regional guideline deltas
ANZ practice emphasises Australian Prescriber-style deprescribing literacy (Brett and Murnion) and short-term only culture for benzodiazepines outside withdrawal protocols. UK BAP anxiety (Baldwin 2014) and sleep (Wilson 2019) statements prioritise SSRI/SNRI and CBT-I over chronic GABAergic use. US AASM pharmacologic insomnia guidance is similarly cautious; AGS Beers Criteria drive geriatric avoid-lists. Canadian BRZA deprescribing CPG and EMPOWER give concrete tools for primary-care deprescribing. WFSBP 2023 anxiety guidance places durable anxiolytics (antidepressants) ahead of long-term benzodiazepines. Formulary names differ; the exam constant is short-term GABAergic use, interaction literacy, and planned taper.[2][13][15][9][14][27]
Complications and exam pitfalls
Prognosis and disposition
Most patients given a true short course and an exit plan avoid long-term dependence. Once continuous use is established, success rates improve with structured taper plus psychosocial support and treatment of primary anxiety/insomnia; high-dose use, seizure history, or unstable polysubstance use may need specialist addiction/inpatient pathways (see benzodiazepine-dependence topic).[1][4][10]
Exam pearls
- Short-term only for BZD/Z-drugs in primary anxiety/insomnia unless specialist exception.[13][15]
- Half-life dictates withdrawal tempo; alprazolam is a high-potency short-acting trap.[1][3]
- LOT in liver disease.[2]
- Z-drugs remain dependence-capable and Beers-listed in older adults.[28][27]
- Buspirone: delayed; no GABA withdrawal cover.[22]
- Pregabalin: GAD RCTs real; renal dose; misuse vigilance.[17][19]
- Opioid + BZD = overdose synergy.[25]
- Flumazenil is not default antidote in chronic users.[1]
- EMPOWER + Canadian BRZA = deprescribing evidence language.[8][9]
Related topics
Cross-link benzodiazepine dependence for deep use-disorder and detox detail; GAD and panic topics for durable SSRI/SNRI/CBT pathways; alcohol and opioid topics for cross-tolerance and lethal combinations; agitation/rapid tranquillisation for acute parenteral pathways.[1][13][25]
References
- [1]Soyka M Treatment of Benzodiazepine Dependence N Engl J Med, 2017.PMID 28328330
- [2]Brett J, Murnion B Management of benzodiazepine misuse and dependence Aust Prescr, 2015.PMID 26648651
- [3]Ashton H The diagnosis and management of benzodiazepine dependence Curr Opin Psychiatry, 2005.PMID 16639148
- [4]Voshaar RC, Couvée JE, van Balkom AJ, et al. Strategies for discontinuing long-term benzodiazepine use: meta-analysis Br J Psychiatry, 2006.PMID 16946355
- [5]Lader M Benzodiazepine harm: how can it be reduced? Br J Clin Pharmacol, 2014.PMID 22882333
- [6]Markota M, Rummans TA, Bostwick JM, et al. Benzodiazepine Use in Older Adults: Dangers, Management, and Alternative Therapies Mayo Clin Proc, 2016.PMID 27814838
- [7]Glass J, Lanctôt KL, Herrmann N, et al. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits BMJ, 2005.PMID 16284208
- [8]Tannenbaum C, Martin P, Tamblyn R, et al. Reduction of inappropriate benzodiazepine prescriptions among older adults through direct patient education: the EMPOWER cluster randomized trial JAMA Intern Med, 2014.PMID 24733354
- [9]Pottie K, Thompson W, Davies S, et al. Deprescribing benzodiazepine receptor agonists: Evidence-based clinical practice guideline Can Fam Physician, 2018.PMID 29760253
- [10]Darker CD, Sweeney BP, Barry JM, et al. Psychosocial interventions for benzodiazepine harmful use, abuse or dependence Cochrane Database Syst Rev, 2015.PMID 26106751
- [11]Baandrup L, Ebdrup BH, Rasmussen JØ, et al. Pharmacological interventions for benzodiazepine discontinuation in chronic benzodiazepine users Cochrane Database Syst Rev, 2018.PMID 29543325
- [12]Lader M, Kyriacou A Withdrawing Benzodiazepines in Patients With Anxiety Disorders Curr Psychiatry Rep, 2016.PMID 26733324
- [13]Baldwin DS, Anderson IM, Nutt DJ, et al. Evidence-based pharmacological treatment of anxiety disorders, post-traumatic stress disorder and obsessive-compulsive disorder: a revision of the 2005 guidelines from the British Association for Psychopharmacology J Psychopharmacol, 2014.PMID 24713617
- [14]Bandelow B, Allgulander C, Baldwin DS, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for treatment of anxiety, obsessive-compulsive and posttraumatic stress disorders - Version 3. Part I: Anxiety disorders World J Biol Psychiatry, 2023.PMID 35900217
- [15]Sateia MJ, Buysse DJ, Krystal AD, et al. Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline J Clin Sleep Med, 2017.PMID 27998379
- [16]Wilson S, Anderson K, Baldwin D, et al. British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders: An update J Psychopharmacol, 2019.PMID 31271339
- [17]Pande AC, Crockatt JG, Feltner DE, et al. Pregabalin in generalized anxiety disorder: a placebo-controlled trial Am J Psychiatry, 2003.PMID 12611835
- [18]Feltner DE, Crockatt JG, Dubovsky SJ, et al. A randomized, double-blind, placebo-controlled, fixed-dose, multicenter study of pregabalin in patients with generalized anxiety disorder J Clin Psychopharmacol, 2003.PMID 12826986
- [19]Rickels K, Pollack MH, Feltner DE, et al. Pregabalin for treatment of generalized anxiety disorder: a 4-week, multicenter, double-blind, placebo-controlled trial of pregabalin and alprazolam Arch Gen Psychiatry, 2005.PMID 16143734
- [20]Llorca PM, Spadone C, Sol O, et al. Efficacy and safety of hydroxyzine in the treatment of generalized anxiety disorder: a 3-month double-blind study J Clin Psychiatry, 2002.PMID 12444816
- [21]Guaiana G, Barbui C, Cipriani A Hydroxyzine for generalised anxiety disorder Cochrane Database Syst Rev, 2010.PMID 21154375
- [22]Chessick CA, Allen MH, Thase M, et al. Azapirones for generalized anxiety disorder Cochrane Database Syst Rev, 2006.PMID 16856115
- [23]Ferracioli-Oda E, Qawasmi A, Bloch MH Meta-analysis: melatonin for the treatment of primary sleep disorders PLoS One, 2013.PMID 23691095
- [24]Brzezinski A, Vangel MG, Wurtman RJ, et al. Effects of exogenous melatonin on sleep: a meta-analysis Sleep Med Rev, 2005.PMID 15649737
- [25]Sun EC, Dixit A, Humphreys K, et al. Association between concurrent use of prescription opioids and benzodiazepines and overdose: retrospective analysis BMJ, 2017.PMID 28292769
- [26]Olfson M, King M, Schoenbaum M Benzodiazepine use in the United States JAMA Psychiatry, 2015.PMID 25517224
- [27]By the 2023 American Geriatrics Society Beers Criteria Update Expert Panel American Geriatrics Society 2023 updated AGS Beers Criteria for potentially inappropriate medication use in older adults J Am Geriatr Soc, 2023.PMID 37139824
- [28]Gunja N The clinical and forensic toxicology of Z-drugs J Med Toxicol, 2013.PMID 23404347