Psych · Psychopharmacology — augmentation strategies
Augmentation strategies in mood and psychosis
Also known as Antidepressant augmentation · Lithium augmentation · Atypical antipsychotic augmentation · T3 augmentation · Treatment-resistant depression next steps · Clozapine augmentation · Clozapine-resistant schizophrenia · Combination antidepressants
Fellowship-depth atlas of structured augmentation in non-response — augment vs switch vs combination, pseudo-resistance exclusion, STAR*D and VAST-D logic, lithium/T3/atypical antipsychotic dosing and monitoring, combination antidepressants, specialist ketamine/esketamine and neuromodulation, OCD add-ons, and clozapine-era/CRS pathways including Petrides ECT and Wagner evidence tiers. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Augmentation is a high-yield fellowship topic because it tests decision architecture more than brand names: re-diagnose, define an adequate trial, choose switch versus augment versus combination versus neuromodulation, name doses and monitoring, and stop a failed add-on on measured outcomes. Examiners punish both premature polypharmacy and years of incomplete trials while suicide risk or metabolic harm accumulate.[1][8][9]
Definition and classification
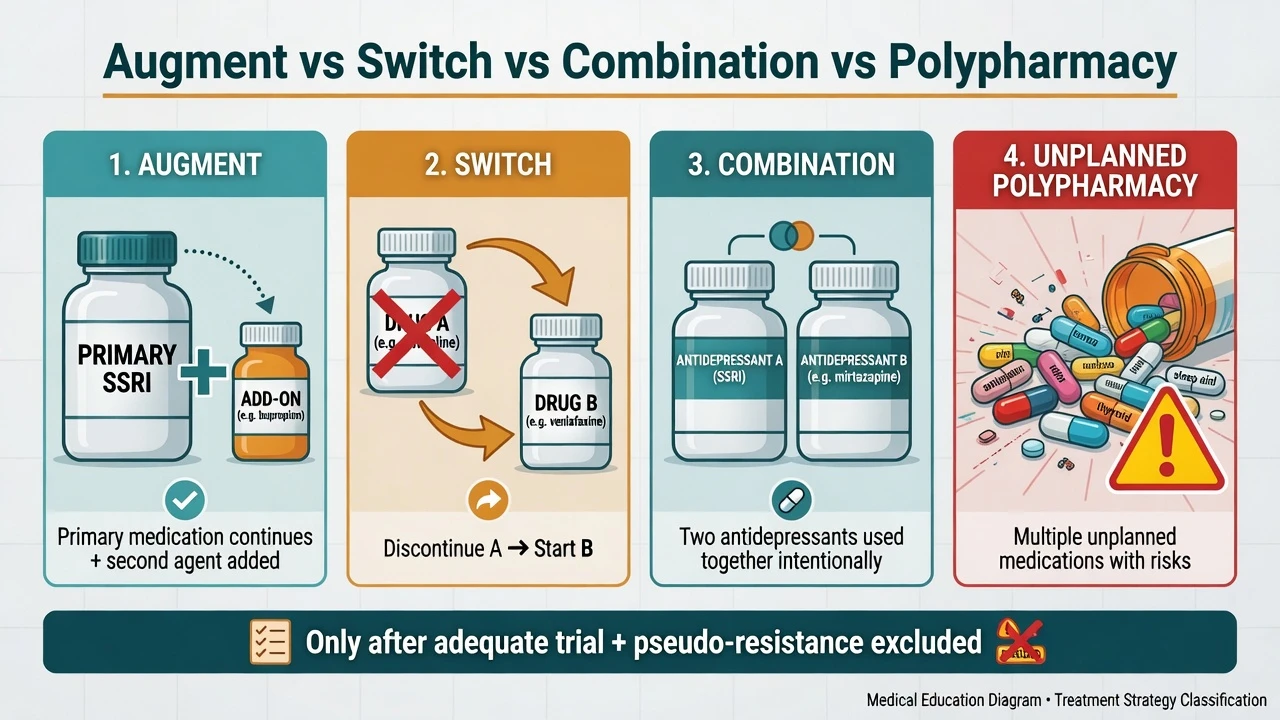
Augmentation is the intentional addition of a second agent (usually with a different primary mechanism) while continuing a partially effective or otherwise appropriate primary drug. It is not the same as switching (stop A, start B), combination therapy (two antidepressants used together by design, e.g. SNRI + mirtazapine), or unplanned polypharmacy (multiple agents without formulation, outcome plan, or stop rules).[1][8]
Outcomes language. Response commonly means about ≥50% reduction on a severity scale (PHQ-9, HAM-D, MADRS, or CGI framing); remission means near-absent symptoms plus function; partial response is meaningful improvement short of remission; non-response fails the response threshold after an adequate trial. Partial response is the classic clinical substrate for augmentation — the primary drug is not useless, so you keep it and add.[1][2][20]
Adequate primary trial (exam mantra). Correct diagnosis, right drug, therapeutic dose, about 4–6 weeks (sometimes longer if slow partial response), verified adherence, addressed substances and medical confounders, and measured outcome — before declaring non-response and reaching for an augmenter.[2][8]
| Strategy | Core idea | Typical use case |
|---|---|---|
| Augment | Keep primary + add different-mechanism agent | Partial response; want to preserve gains |
| Switch | Stop A → start B | Intolerance or near-zero benefit from A |
| Combination | Two antidepressants intentionally | Selected TRD steps (e.g. STAR*D level 4 combo arm) |
| Neuromodulation / ketamine class | Device or rapid-acting agent pathway | Severity, TRD steps, or psychosis urgency |
| Strategy labels above structure viva answers; do not use "polypharmacy" as a synonym for planned, monitored augmentation.[1][4][8] |
Epidemiology and why this matters
STAR*D under measurement-based care found that only about one-third of outpatients remitted at level 1 with citalopram, and cumulative remission fell as successive treatment steps accumulated — so partial response and sequential failure are the norm, not the exception, in real clinics.[1][2]
That epidemiology drives everyday use of lithium, T3, and atypical antipsychotic augmentation, and later specialist options. In psychosis, a substantial minority meet treatment-resistant schizophrenia (TRS) criteria after two adequate antipsychotic trials; among those offered clozapine, incomplete response creates clozapine-resistant / ultra-treatment-resistant pathways where augmentation (including ECT) becomes the exam conversation — not another random dual oral pair without formulation.[12][17][18]
Anchors examiners expect
Pathophysiology and mechanistic rationales
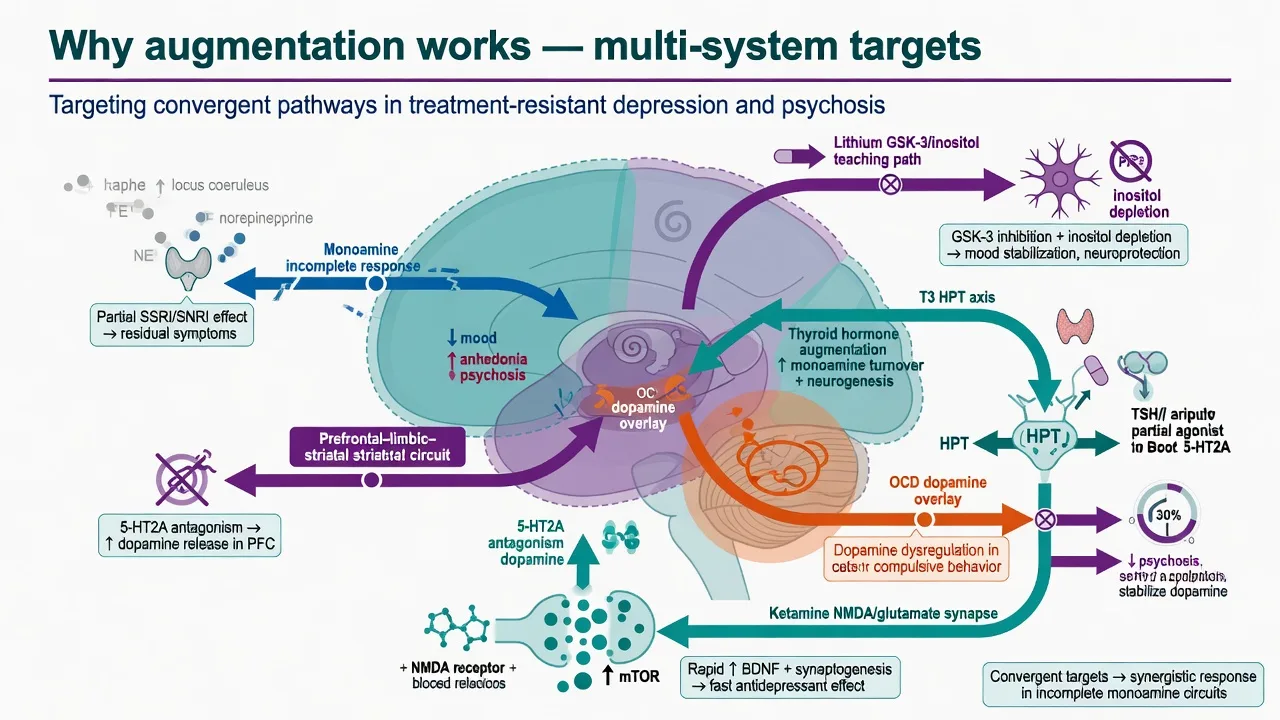
Do not invent a single "augmentation receptor." Teaching models map add-ons to residual pathway gaps after monoamine optimisation: lithium (intracellular signalling / GSK-3 and inositol pathway models; anti-suicide relevance in mood disorders), T3 (HPT axis and monoamine facilitation teaching), second-generation antipsychotics (D2 partial agonism or 5-HT2A / multi-receptor profiles depending on agent), and ketamine/esketamine (NMDA/glutamate–synaptic plasticity). In OCD, low-dose antipsychotic add-on targets residual compulsive drive after high-dose SRI. In clozapine-resistant schizophrenia, residual positive symptoms after adequate D2 and clozapine exposure motivate ECT and carefully selected pharmacological add-ons with thinner evidence tiers.[5][6][10][11][13]
Clinical presentation of the "augmenter candidate"
Typical mood picture: improved sleep or mood range but residual anhedonia, anxiety, cognitive fog, or incomplete functional recovery on a therapeutic antidepressant. Typical psychosis picture after two antipsychotics: ongoing hallucinations or delusions with or without negative/cognitive burden — if TRRIP criteria are met, the next structured step is clozapine, not improvisational dual AP as default "augmentation."[1][12][18]
Intolerance is not non-response. If the patient never reached a therapeutic dose because of side effects, optimise, switch for tolerability, or treat the side effect — do not stack drugs on a failed exposure.[2][8]
Differential — exclude pseudo-resistance first
Pseudo-resistance
- Wrong diagnosis (bipolar, mixed, medical)
- Subtherapeutic dose or too-short trial
- Non-adherence / pharmacy gaps
- Substances, OSA, thyroid, B12
True non-response substrate
- Confirmed diagnosis
- ≥1 adequate failed trial (or ≥2 for TRD label)
- Adherence verified
- Measured outcome
Mood traps
- Covert bipolar spectrum
- Anxious distress / PTSD driving scores
- Personality disorder residual distress
- Psychotic depression needing ECT
Psychosis traps
- Oral non-adherence → use LAI before TRS stamp
- Substance-induced psychosis
- Organic psychosis
- Clozapine never offered
Bedside assessment and investigations before you add
History scaffold: drug, dose, duration at dose, adherence method, response, side-effects, prior steps (ATHF-quality treatment history). Bipolar screen. Substances. Trauma. Medical and perinatal. Suicide risk and care intensity.[1][8]
Measurement: PHQ-9 or equivalent for depression (serial), CGI; in psychosis use structured clinical global impression and local positive-symptom tracking; Y-BOCS if OCD augment context.[2][20]
Pre-lithium labs: U&E/creatinine/eGFR, TFT, calcium, weight, pregnancy test when relevant, ECG if cardiac risk/older adult. Plan 12-hour trough TDM culture.[6][9]
Pre-atypical antipsychotic: weight/BMI, BP, fasting glucose or HbA1c, lipids; ECG if QT risk or high-risk combinations. Consent for metabolic and movement effects.[5][8]
Pre-T3: exclude hyperthyroidism; baseline TFT; plan follow-up thyroid tests and symptom review for iatrogenic thyrotoxic features.[3]
Clozapine-era: confirm FBC monitoring infrastructure, plasma level when available, constipation and myocarditis education before any CRS augmenter discussion.[17][18][19]
Acute and emergency priorities (do not "augment through" these)
- Suicide risk / severe self-neglect — raise care intensity; means restriction; consider admission; ECT when indicated for severe depression with risk or psychosis.[9][15]
- Psychotic depression, catatonia, life-threatening poor intake — ECT is a first-line pathway, not a distant last resort after five oral add-ons.[9][15]
- Toxicity emergencies — lithium toxicity, NMS, serotonin syndrome: stop offenders, medical resuscitation pathways.[6][9]
- Ketamine/esketamine pathway — only with monitoring for blood pressure, dissociation, and misuse risk; not a casual outpatient "boost."[13]
Definitive management — mood pathway
Decision tree
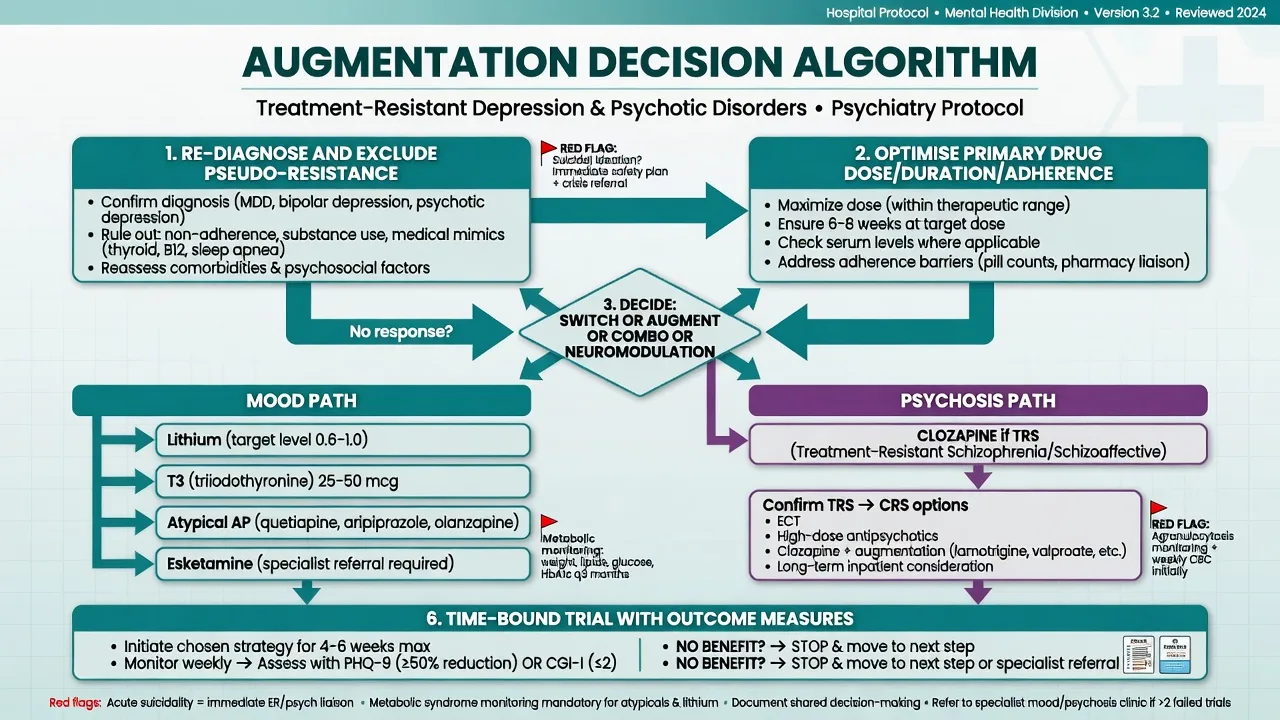
- Re-diagnose and exclude pseudo-resistance.[1][8]
- Optimise the primary agent (dose, duration, adherence).[2]
- Choose switch (intolerance / zero benefit), augment (partial response), combination, or neuromodulation / rapid-acting pathway based on severity, preference, comorbidity, and access.[1][7][8]
- Set a time-bound trial with a scale and a stop rule.[2][20]
STAR*D level-2 switching among bupropion-SR, sertraline, and venlafaxine-XR after SSRI failure showed broadly similar remission — the exam pearl is that several reasonable switches can be equivalent under measurement-based care, so do not fetishise one brand.[14]
VAST-D randomised veterans unresponsive to an antidepressant to switch to bupropion, augment with bupropion, or augment with aripiprazole — a modern real-world comparison of switch versus augment strategies examiners may set against STAR*D.[7]
Lithium augmentation (examiner gold)
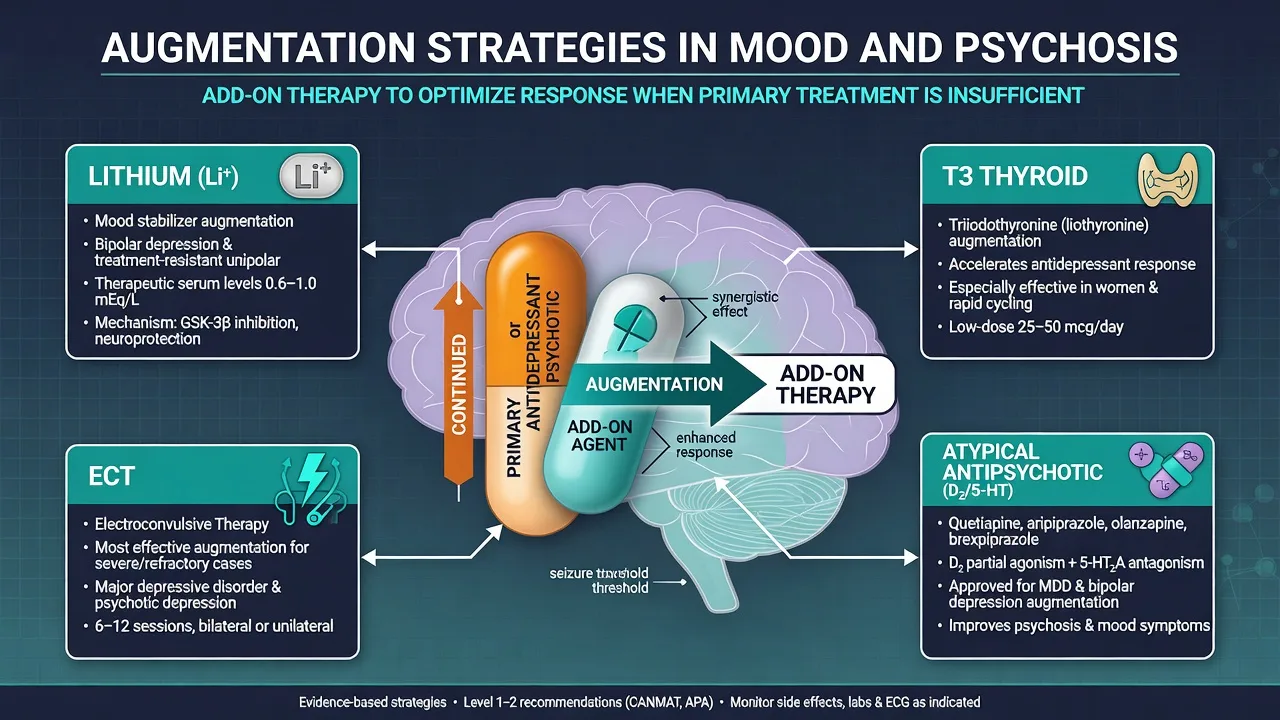
Crossley and Bauer meta-analysed randomised placebo-controlled trials: lithium both accelerates and augments antidepressant response in depressive disorders — still the classic board answer for pharmacological augmentation of antidepressants.[6]
Exam dosing scaffold (individualise; product-dependent): start lithium carbonate often at 250–500 mg/day oral (or local IR/SR equivalent), titrate using clinical response and 12-hour trough levels. For depression augmentation, many services target lower-to-mid maintenance bands (commonly taught around 0.4–0.8 mmol/L depending on age, tolerability, and local guidance — state the principle and local protocol rather than inventing a universal single number). Monitor eGFR/TFT/calcium and educate on NSAIDs, ACEI/ARB, thiazides, and dehydration.[6][9]
T3 (liothyronine) augmentation
STAR*D compared lithium and T3 after two failed medication treatments: remission rates were similar with different side-effect profiles (lithium more often discontinued for adverse effects in that report) — so T3 is a legitimate examiner alternative when lithium is unsuitable, not a folk remedy.[3]
Exam dosing orientation: liothyronine commonly taught in the order of about 25–50 micrograms oral daily (start low, especially older adults), with thyroid monitoring and vigilance for palpitations, tremor, anxiety, and bone/cardiac risk with longer use — confirm product information and endocrine collaboration for extended courses.[3][8]
Atypical antipsychotic augmentation
Nelson and Papakostas meta-analysed placebo-controlled RCTs: atypical antipsychotic augmentation improves response/remission in MDD non-response and increases adverse effects (weight, sedation, EPS risk depending on agent).[5]
High-yield agents in exams: aripiprazole (often start 2–5 mg oral daily, titrate toward common trial ranges around 5–15 mg daily as tolerated), quetiapine XR (sleep/anxiety residual patterns; metabolic and sedation load; titrate per product information — often low-to-moderate antidepressant-augment doses rather than full antipsychotic mania doses), and olanzapine–fluoxetine combination contexts in selected severe/psychotic-leaning depression pathways. Metabolic monitoring is non-negotiable.[5][7][8]
Combination antidepressants
STAR*D level 4 compared tranylcypromine with venlafaxine plus mirtazapine after multiple failures — both difficult pathways with modest remission and important safety teaching (MAOI diet/interaction rules; serotonin risk when combining poorly). Combination is a deliberate strategy, not accidental stacking.[4]
Specialist next steps when oral augmentation fails or severity is high
- ECT remains the most effective rapid somatic treatment for severe major depression in meta-analytic evidence; use early for psychotic/melancholic high-risk presentations.[15]
- rTMS (high-frequency left DLPFC programmes as classic framing) has multisite RCT support for acute treatment of depression with a different risk profile from ECT.[16]
- Esketamine nasal spray with a newly initiated oral antidepressant improved TRD outcomes in pivotal programmes (Popova); requires supervised administration and monitoring — access and product labels are jurisdiction-specific.[13]
Definitive management — psychosis pathway
Do not call dual oral antipsychotics "augmentation" as a way to avoid clozapine. After two adequate antipsychotic failures with adherence addressed (LAI when oral adherence is doubtful), TRRIP terminology and clinical guidance direct candidates toward clozapine — the only agent with robust superiority for treatment-resistant schizophrenia since Kane 1988.[12][17][18][19]
Clozapine-resistant schizophrenia (CRS). Before adding anything: confirm adequate dose, duration, adherence, and plasma level where available. Then evidence-tier options carefully.[11][18]
ECT augmentation of clozapine. Petrides and colleagues showed that ECT added to clozapine outperformed clozapine continuation alone for residual positive symptoms in clozapine-resistant schizophrenia — the modern board answer when clozapine is optimised and positives persist.[10]
Pharmacological clozapine augmentation. Wagner and colleagues' meta-review of clozapine resistance options shows heterogeneous and often limited-quality evidence for many add-ons (second antipsychotic, mood stabilisers, others) — answer with evidence tiers and harm monitoring, not a shopping list presented as equivalent RCTs.[11]
OCD and other special augment contexts
For OCD after high-dose SSRI (and ERP where available), low-dose antipsychotic augmentation (e.g. risperidone or aripiprazole) is a classic exam move for residual Y-BOCS burden, with metabolic/EPS monitoring and preference for ERP co-treatment when accessible. Glutamatergic experiments exist but are not first-line fellowship defaults.[5][8]
Bipolar depression: do not import unipolar multi-antidepressant stacking. Mood-stabiliser backbone (lithium, lamotrigine, quetiapine, lurasidone, etc. per guideline region) first; antidepressant add-on is cautious and short when used at all.[9]
Special populations
Older adults: lower lithium targets and closer renal/thyroid surveillance; higher sensitivity to SGA metabolic and extrapyramidal effects; ECT often favourable in severe late-life depression.[6][9][15]
Pregnancy: risk–benefit of untreated severe illness versus agents; specialist perinatal pathways; ECT may be preferred in life-threatening depression.[9][15]
Adolescents: limited trial evidence for many adult TRD augmenters; specialist CAMHS care; therapy plus carefully chosen primary agents first.[8][9]
Intellectual disability / autism: formulation-first; treat diagnosed mental illness, not behaviour alone with cascading polypharmacy.[19]
Complications and pitfalls
- Labelling pseudo-resistance as TRD and stacking drugs.[1]
- Metabolic syndrome from SGA augmenters without monitoring.[5]
- Lithium organ neglect and interaction blindness (NSAIDs).[6]
- Missed bipolarity and antidepressant-only escalation.[9]
- Dual antipsychotics for years without clozapine discussion.[12][18]
- Declaring clozapine failure without level/duration.[11][18]
- No stop rule — permanent polypharmacy after a failed 2-week "try."[2]
Prognosis and disposition
STAR*D teaches diminishing returns with successive failed steps — aim for remission, not chronic partial response that still disables or kills. Disposition spans GP shared care with measurement, community mental health, mood disorder clinics, clozapine clinics, ECT suites, and neuromodulation services. After late remission, continue the effective regimen and plan maintenance (including continuation ECT or maintenance rTMS/esketamine pathways where used).[1][9][13][15]
Evidence, guidelines, regional deltas
Landmark pillars: STAR*D multi-step outcomes and measurement-based care;[1][2] level-2 switch equivalence;[14] lithium vs T3;[3] level-4 MAOI/combo;[4] Crossley lithium meta-analysis;[6] Nelson atypical AP meta-analysis;[5] VAST-D;[7] Popova esketamine;[13] UK ECT Review Group;[15] O'Reardon rTMS;[16] Kane clozapine;[17] TRRIP;[12] Petrides ECT for CRS;[10] Wagner clozapine augmentation review;[11] CANMAT pharmacological section;[8] RANZCP mood 2020;[9] RANZCP schizophrenia.[19]
RANZCP mood guidelines embed measurement-based sequencing, lithium and antipsychotic monitoring culture, and early somatic therapies for severe illness.[9] CANMAT provides explicit first-/second-line pharmacological tables for MDD including augmentation choices.[8] NICE pathways emphasise stepped care and evidence-based psychological therapies alongside medicines. APA schizophrenia guidance prioritises clozapine for TRS and structured physical-health monitoring when antipsychotics (including augmenters) are used. Access to esketamine, rTMS, and VMAT2-class agents differs by jurisdiction — state clinical indication and evidence, then local formulary, rather than inventing funding rules.
Controversies to handle calmly: early atypical antipsychotic versus lithium given metabolic cost; early neuromodulation/ketamine versus traditional oral augmentation; quality of evidence for many clozapine add-ons; dual antipsychotics without clozapine. Answer with measurement, patient values, risk, and named trials.[5][7][11]
Exam pearls
PASS for augmentation clinics
PASS
References
- [1]Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report Am J Psychiatry, 2006.PMID 17074942
- [2]Trivedi MH, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D, Ritz L, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice Am J Psychiatry, 2006.PMID 16390886
- [3]Nierenberg AA, Fava M, Trivedi MH, Wisniewski SR, Thase ME, McGrath PJ, et al. A comparison of lithium and T(3) augmentation following two failed medication treatments for depression: a STAR*D report Am J Psychiatry, 2006.PMID 16946176
- [4]McGrath PJ, Stewart JW, Fava M, Trivedi MH, Wisniewski SR, Nierenberg AA, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report Am J Psychiatry, 2006.PMID 16946177
- [5]Nelson JC, Papakostas GI Atypical antipsychotic augmentation in major depressive disorder: a meta-analysis of placebo-controlled randomized trials Am J Psychiatry, 2009.PMID 19687129
- [6]Crossley NA, Bauer M Acceleration and augmentation of antidepressants with lithium for depressive disorders: two meta-analyses of randomized, placebo-controlled trials J Clin Psychiatry, 2007.PMID 17592920
- [7]Mohamed S, Johnson GR, Chen P, Hicks PB, Davis LL, Yoon J, et al. Effect of Antidepressant Switching vs Augmentation on Remission Among Patients With Major Depressive Disorder Unresponsive to Antidepressant Treatment: The VAST-D Randomized Clinical Trial JAMA, 2017.PMID 28697253
- [8]Kennedy SH, Lam RW, McIntyre RS, Tourjman SV, Bhat V, Blier P, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments Can J Psychiatry, 2016.PMID 27486148
- [9]Malhi GS, Bell E, Bassett D, Boyce P, Bryant R, Hazell P, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [10]Petrides G, Malur C, Braga RJ, et al. Electroconvulsive therapy augmentation in clozapine-resistant schizophrenia: a prospective, randomized study Am J Psychiatry, 2015.PMID 25157964
- [11]Wagner E, Löhrs L, Siskind D, et al. Clozapine augmentation strategies - a systematic meta-review of available evidence. Treatment options for clozapine resistance J Psychopharmacol, 2019.PMID 30696332
- [12]Howes OD, McCutcheon R, Agid O, et al. Treatment-Resistant Schizophrenia: Treatment Response and Resistance in Psychosis (TRRIP) Working Group Consensus Guidelines on Diagnosis and Terminology Am J Psychiatry, 2017.PMID 27919182
- [13]Popova V, Daly EJ, Trivedi M, Cooper K, Lane R, Lim P, et al. Efficacy and Safety of Flexibly Dosed Esketamine Nasal Spray Combined With a Newly Initiated Oral Antidepressant in Treatment-Resistant Depression: A Randomized Double-Blind Active-Controlled Study Am J Psychiatry, 2019.PMID 31109201
- [14]Rush AJ, Trivedi MH, Wisniewski SR, Stewart JW, Nierenberg AA, Thase ME, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression N Engl J Med, 2006.PMID 16554525
- [15]UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis Lancet, 2003.PMID 12642045
- [16]O'Reardon JP, Solvason HB, Janicak PG, Sampson S, Isenberg KE, Nahas Z, et al. Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: a multisite randomized controlled trial Biol Psychiatry, 2007.PMID 17573044
- [17]Kane J, Honigfeld G, Singer J, et al. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry, 1988.PMID 3046553
- [18]Kane JM, Agid O, Baldwin ML, et al. Clinical Guidance on the Identification and Management of Treatment-Resistant Schizophrenia J Clin Psychiatry, 2019.PMID 30840788
- [19]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681
- [20]Kroenke K, Spitzer RL, Williams JB The PHQ-9: validity of a brief depression severity measure J Gen Intern Med, 2001.PMID 11556941