Psych · Psychopharmacology — benzodiazepine prescribing and tapering
Benzodiazepine prescribing and tapering
Also known as Benzodiazepine taper · BZD deprescribing · Diazepam substitution · Benzodiazepine withdrawal management · Alprazolam taper · Benzodiazepine initiation · Sedative-hypnotic prescribing
Exam-exhaustive fellowship psychopharmacology of benzodiazepine initiation and structured tapering — half-life and equipotency maps, short-term-only rules, adult oral dose anchors, diazepam substitution, 10–25% taper scaffolds, EMPOWER and Canadian BRZA deprescribing, elderly Beers harm, opioid synergy, pregnancy cautions, and flumazenil pitfalls. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
2 MCQs with explanations
Target exams
Red flags
This leaf is prescribing craft and taper craft. Full use-disorder nosology and dual-diagnosis depth sit in the benzodiazepine-dependence topic; the wider non-GABAergic class map (buspirone, pregabalin, Z-drugs, melatonin) sits in anxiolytics and hypnotics. Examiners still expect you to initiate safely, convert equipotently, deprescribe with evidence language, and avoid the classic traps (alprazolam defaults, automatic renewals, flumazenil bravado, elderly Beers violations).[1][8][15]
Definition and classification
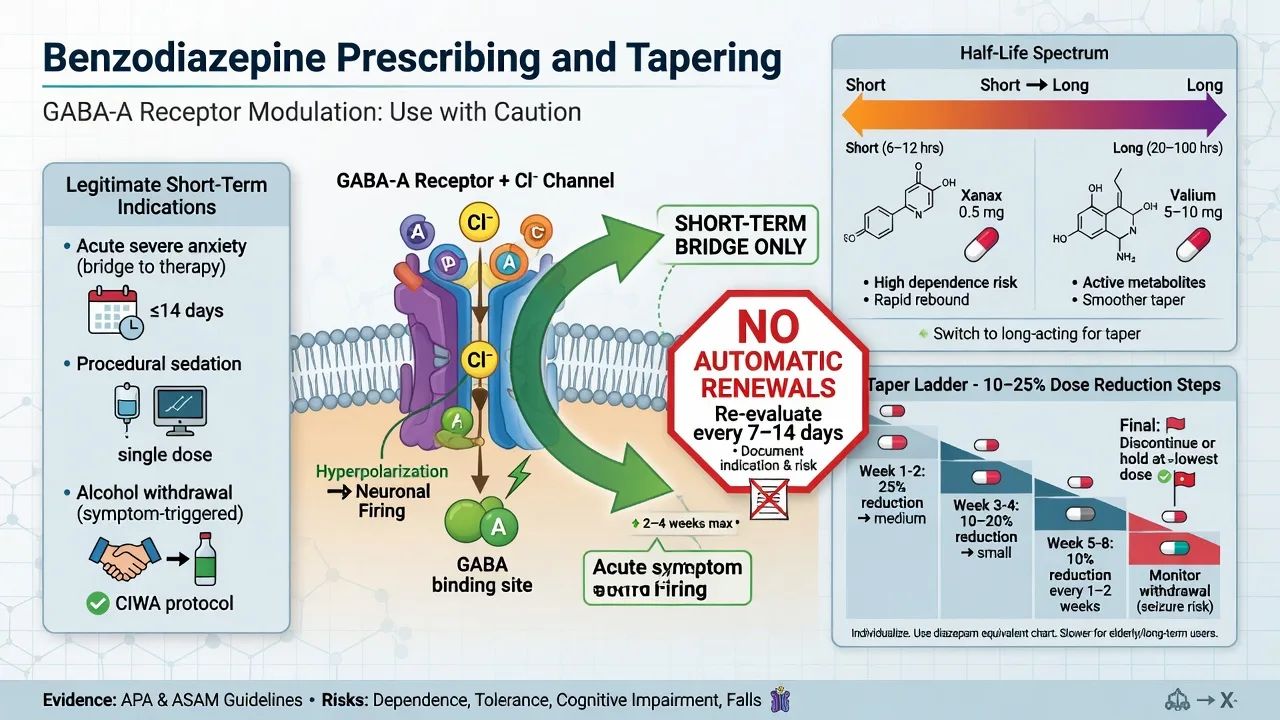
Benzodiazepines are GABA-A positive allosteric modulators (PAMs). They increase the frequency of chloride-channel opening when GABA is present — they are not direct agonists. Clinical effects are dose- and circuit-dependent: anxiolysis, sedation/hypnosis, anticonvulsant action, anterograde amnesia, and muscle relaxation.[1][3][15]
| Pattern | Examples | Prescribing implication |
|---|---|---|
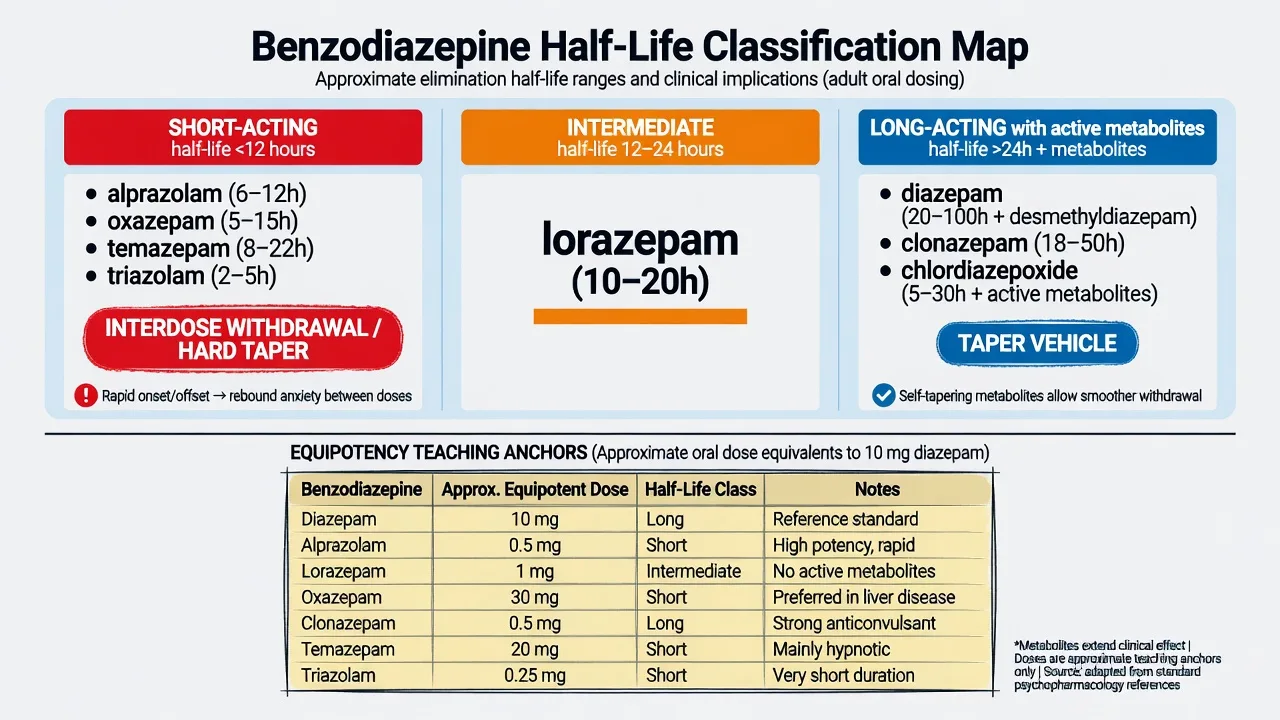
| Ultra-short / very short | Midazolam, triazolam (context) | Procedural; sharp offset/rebound |
| Short–intermediate | Alprazolam, lorazepam, oxazepam, temazepam | Alprazolam: high-potency, interdose anxiety, hard taper |
| Long (+ active metabolites) | Diazepam, clonazepam, chlordiazepoxide | Smoother taper vehicle; accumulation in elderly/hepatic disease |
| Half-life and active metabolites drive withdrawal tempo and choice of taper vehicle.[1][2][3] |
Z-drugs (zolpidem, zopiclone/eszopiclone, zaleplon) act at the benzodiazepine site of GABA-A receptors. They are not free of dependence, complex sleep behaviours, falls, or residual impairment — do not market them as safe long-term hypnotics, especially in older adults.[10][19][20]
Epidemiology and harm landscape
Population data show substantial benzodiazepine exposure, with older adults over-represented relative to their risk–benefit ratio.[18][9] Long-term use associates with falls, fractures, cognitive impairment, road traffic risk, dependence, and — in observational cohorts — dementia signals that remain confounded but examinable.[10][11][16] Concurrent prescription opioids and benzodiazepines associate with overdose death in large retrospective analyses — a non-negotiable interaction pearl.[17] Harm-reduction framing for fellowship is practical: reduce inappropriate starts, stop automatic renewals, and deprescribe with structure rather than moral panic alone.[8][12][13]
Mechanisms — viva core
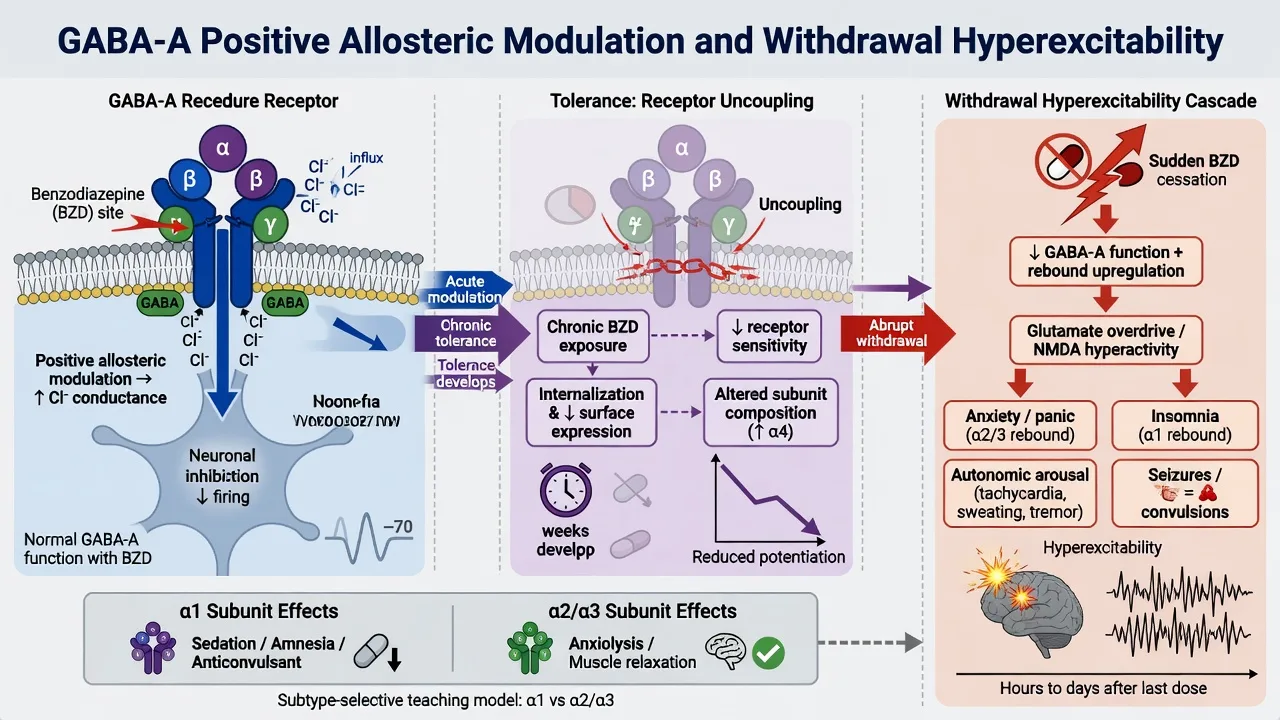
Acute pharmacology. Benzodiazepines bind the α/γ interface of GABA-A receptors and potentiate GABA. Teaching subunit model: α1-rich circuits lean sedation, amnesia, and anticonvulsant effects; α2/3 lean anxiolysis; α5 relates to cognitive effects in teaching narratives.[1][3][15]
Tolerance and dependence physiology. Continuous exposure uncouples allosteric efficacy and shifts receptor adaptation. Physiological dependence (tolerance + withdrawal) can occur at therapeutic doses after weeks of continuous use — you do not need recreational misuse for a hard taper.[1][3][7]
Withdrawal hyperexcitability. Anxiety, insomnia, tremor, sweating, tachycardia, sensory hyperacusis, depersonalisation, seizures, and rarely delirium. Short-acting high-potency agents tend to produce earlier, more intense interdose and withdrawal symptoms; long-acting agents (and active metabolites) delay and smooth the curve — hence diazepam substitution teaching.[1][2][3]
Protracted symptoms. Weeks to months of fluctuating anxiety, insomnia, and sensory symptoms can follow cessation. Tempo relative to the last dose reduction discriminates withdrawal rebound from primary anxiety relapse — wrong labelling drives dose escalation.[3][7]
When initiation is justified
Legitimate short-term contexts (exam structure): severe acute anxiety or panic as a bridge while SSRI/SNRI and psychological therapy start; time-limited severe insomnia after sleep hygiene/stimulus control when CBT-I is delayed (not indefinite nocte scripts); alcohol withdrawal protocols (owned in detail by addiction topics); procedural or acute agitation pathways (owned by emergency topics); and selected specialist niches (e.g. catatonia adjunct — pointer only).[1][7][15][20]
For primary chronic GAD, panic, and insomnia, durable care is psychological therapy and/or SSRI/SNRI pathways — benzodiazepines are not the long-term default.[7][15][20]
Initiation checklist (must document): indication; agent and half-life rationale; dose and route; stop/review date; co-prescribed opioids/alcohol risk; falls and driving counselling; pregnancy potential; pharmacy reconciliation; plan for non-GABAergic treatment of the maintaining problem.[2][8][14]
Agent selection and adult oral dose anchors
Ranges below are exam orientation scaffolds from clinical reviews and deprescribing literature — always check current product information and local protocols; use lower starts in older adults.[2][12][15]
| Agent | Typical adult oral pattern | Exam notes |
|---|---|---|
| Diazepam | 2–5 mg as needed or divided short courses; specialist higher in withdrawal protocols | Long; preferred taper vehicle |
| Lorazepam | 0.5–1 mg PRN/scheduled short courses | Intermediate; useful in hepatic disease (LOT) |
| Oxazepam | 7.5–15 mg short courses | Short–intermediate; LOT |
| Temazepam | 10 mg nocte short courses (some use 20 mg) | Hypnotic niche; LOT |
| Alprazolam | 0.25–0.5 mg short-term if used at all | High-potency short-acting — avoid as default chronic anxiolytic |
| Clonazepam | 0.25–0.5 mg (anxiety/seizure contexts) | Long; accumulation risk |
| Dose tables are teaching anchors, not a licence to invent chronic high-dose scripts.[2][1][15] |
LOT teaching (hepatic impairment): prefer lorazepam, oxazepam, temazepam — conjugation-dominant pathways with fewer long-acting oxidative metabolites — when liver disease is relevant.[2][1]
Equipotency teaching anchors (approximate oral equivalents to diazepam 10 mg; local conversion tables override memory): alprazolam about 0.5 mg; lorazepam about 1 mg; clonazepam about 0.5 mg; oxazepam about 15–30 mg depending on table; temazepam about 20 mg. Use conversions to stabilise on a long-acting agent before stepwise reduction when interdose withdrawal or poly-agent chaos confounds the taper.[1][2][3][14]
Assessment before prescribe or taper
Structure the history: agent(s), prescribed versus actual intake (pill counts, early refills), duration, PRN versus scheduled, prior withdrawal seizures, alcohol and opioid co-use, gabapentinoids, online/illicit supply, multiple prescribers, falls, driving/occupation, pregnancy intent, cognitive baseline, suicide risk, and capacity for a collaborative plan.[2][1][14] Physical exam targets vitals, tremor, gait, nystagmus, and sequelae of falls or seizures. Urine drug screens miss many benzodiazepines on immunoassay — history and pharmacy data first; no routine serum levels for outpatient taper craft.[2][1]
Structured taper algorithm
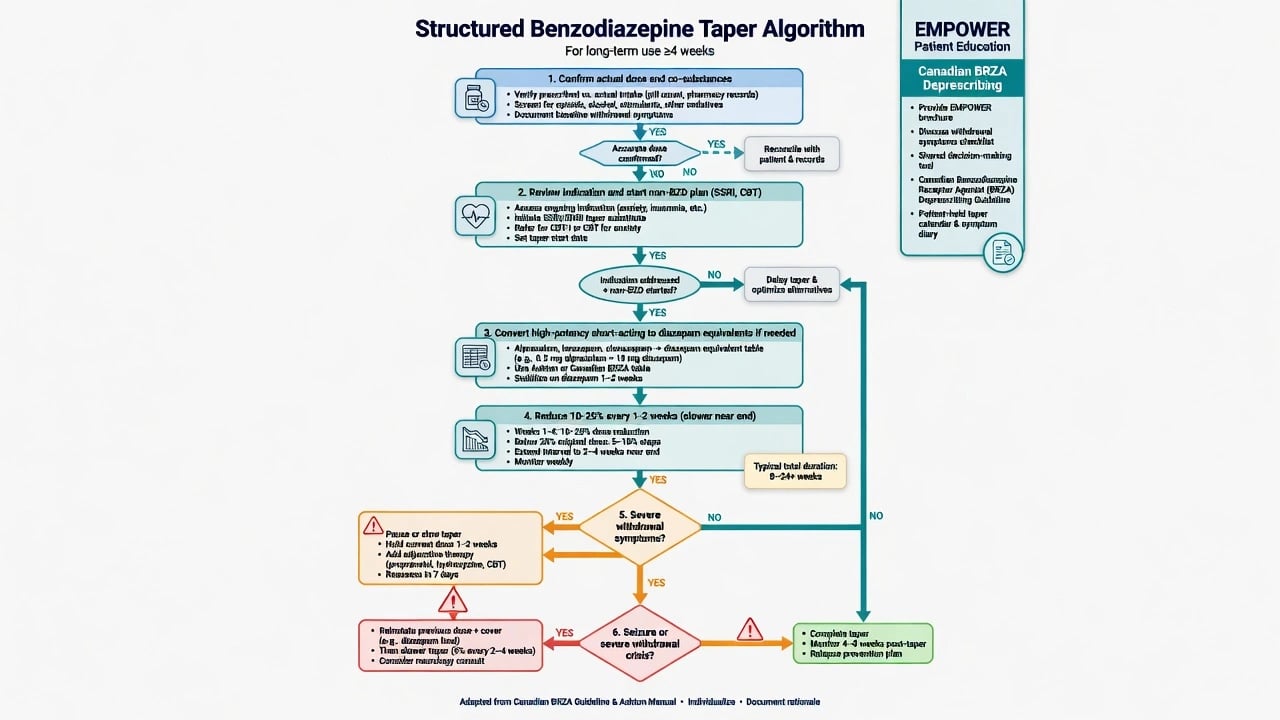
Core steps (must-know):
- Confirm actual dose and co-substances; reconcile pharmacy records.
- Review indication — stop if no ongoing evidence-based role; start or optimise SSRI/SNRI, CBT/CBT-I, sleep hygiene.
- Convert high-potency short-acting agents to a longer vehicle (often diazepam) when needed; stabilise briefly if chaotic use.
- Reduce about 10–25% of the current daily dose every 1–2 weeks (sometimes slower), with smaller steps in the final phase.
- Pause or slow for severe withdrawal symptoms rather than powering through.
- If seizure or severe crisis: reinstate adequate GABA cover, medical emergency pathway as needed, then restart a slower taper — do not leave a dependent patient off all cover.[1][2][3][14]
Meta-analysis supports structured discontinuation strategies over abrupt advice alone.[4] Psychosocial interventions improve outcomes in harmful use/dependence pathways; pharmacological adjuncts for discontinuation have mixed Cochrane support — do not invent a miracle taper pill.[5][6] EMPOWER showed direct patient education can reduce inappropriate long-term benzodiazepine prescriptions in older adults; Canadian BRZA deprescribing guidance and joint tapering CPGs operationalise shared decision-making and stepwise reduction when risks outweigh benefits.[13][12][14]
Short-term initiation
- Named indication and stop date
- Lowest effective oral dose
- Parallel SSRI/CBT plan
- Avoid automatic renewals
Outpatient taper
- Confirm actual dose
- Diazepam substitution if needed
- 10–25% every 1–2+ weeks
- EMPOWER-style education
High-risk / complex
- Seizure history
- High-dose or polysubstance
- Failed outpatient taper
- Consider specialist/inpatient cover
Never-do traps
- Abrupt stop after continuous use
- Opioid + BZD stacking
- Flumazenil as default
- Alprazolam as chronic default
Prescribing craft is as much about what you refuse as what you start.[1][14][17]
Acute toxicity and emergency withdrawal
Overdose: airway and ventilation first; supportive care. Flumazenil is only for highly selected pure iatrogenic settings — it can precipitate seizures in chronic users or mixed overdoses and is not a routine antidote.[1][2] Naloxone treats the opioid component of mixed overdose; it does not reverse benzodiazepine effects.[17]
Withdrawal seizure or delirium: ABC, terminate seizure per emergency protocol, reinstate long-acting benzodiazepine cover, exclude other causes, then plan controlled taper. Combined alcohol–benzodiazepine withdrawal is higher acuity and needs protocolised medical management.[1][2][3]
Elderly patients — Beers, falls, cognition
In older adults, benzodiazepines and Z-drugs associate with falls, fractures, cognitive impairment, delirium risk, and motor vehicle accidents. Glass meta-analysis found unfavourable risk–benefit for sedative-hypnotics in older people with insomnia; Markota reviews clinical dangers and alternatives; AGS Beers Criteria list these agents as potentially inappropriate medications in older adults.[10][9][19] Prefer non-drug sleep strategies, treat depression/pain/nocturia causes of insomnia, and if medicine is unavoidable use the lowest dose for the shortest time with falls precautions. EMPOWER-style education is an evidence-based deprescribing lever in this group.[13][12]
Special populations
Pregnancy and lactation. Avoid routine benzodiazepines. If exposure continues near term, anticipate neonatal floppy infant syndrome and withdrawal — individualised risk–benefit with obstetric liaison; prefer non-drug anxiety/insomnia care and pregnancy-compatible treatment of underlying disorders when indicated.[15][2]
Youth. Avoid chronic benzodiazepines for anxiety; first-line psychological therapies and SSRI pathways.[15][7]
Hepatic disease. LOT agents; avoid accumulation of long-acting oxidative metabolites when possible.[2]
Dementia and delirium. Benzodiazepines often worsen confusion and falls — not first-line behavioural management outside specific withdrawal or seizure contexts.[9][19]
Regional guideline deltas
ANZ practice emphasises Australian Prescriber-style deprescribing literacy (Brett and Murnion) and short-term-only culture outside withdrawal protocols. UK BAP sleep consensus prioritises behavioural treatment over chronic hypnotics. US practice increasingly cites joint tapering guidance when risks outweigh benefits and AGS Beers avoid-lists in geriatrics. Canadian BRZA deprescribing CPG and EMPOWER give concrete primary-care tools. Formulary names differ; the exam constant is short-term GABAergic use, interaction literacy, equipotent conversion, and planned taper.[2][20][14][12][13][19]
Monitoring and disposition
During any course or taper: efficacy, sedation, falls, confusion, dose escalation, multiple prescribers, mood and suicidality, alcohol/opioid substitution, driving advice, and prescription monitoring where available.[2][14] Most true short courses succeed if the exit is set at initiation. Established continuous users need a deprescribing pathway with psychosocial support; high-dose use, seizure history, or unstable polysubstance use may need specialist addiction or inpatient pathways (see benzodiazepine-dependence topic).[1][4][5]
Numbers that stick in viva
These anchors compress equipotency, taper craft, opioid synergy, and deprescribing evidence into viva-ready fragments.[2][1][17][13]
Complications and exam pitfalls
Exam pearls
- Exit plan on day one — indication, dose, duration, review date.[8][14]
- Half-life dictates withdrawal tempo; alprazolam is a high-potency short-acting trap.[1][3]
- LOT in liver disease.[2]
- 10–25% every 1–2 weeks is a scaffold, not dogma — slower near the end.[1][12][14]
- Diazepam substitution for chaotic short-acting high-potency use.[2][3]
- Opioid + BZD = overdose synergy.[17]
- Flumazenil is not default in chronic users.[1]
- EMPOWER + Canadian BRZA + joint tapering CPG = deprescribing viva language.[13][12][14]
- Beers 2023: avoid benzodiazepines and Z-drugs in older adults when possible.[19]
Related topics
Cross-link benzodiazepine dependence for use-disorder and complex detox detail; anxiolytics and hypnotics for non-GABAergic alternatives and Z-drug depth; GAD/panic for durable SSRI/SNRI/CBT pathways; alcohol withdrawal for protocolised BZD treatment of alcohol; opioids for lethal combinations; older-adult prescribing and perinatal psychopharmacology for special-population depth.[1][15][17]
References
- [1]Soyka M Treatment of Benzodiazepine Dependence N Engl J Med, 2017.PMID 28614686
- [2]Brett J, Murnion B Management of benzodiazepine misuse and dependence Aust Prescr, 2015.PMID 26648651
- [3]Ashton H The diagnosis and management of benzodiazepine dependence Curr Opin Psychiatry, 2005.PMID 16639148
- [4]Voshaar RC, Couvée JE, van Balkom AJ, et al. Strategies for discontinuing long-term benzodiazepine use: meta-analysis Br J Psychiatry, 2006.PMID 16946355
- [5]Darker CD, Sweeney BP, Barry JM, et al. Psychosocial interventions for benzodiazepine harmful use, abuse or dependence Cochrane Database Syst Rev, 2015.PMID 26106751
- [6]Baandrup L, Ebdrup BH, Rasmussen JØ, et al. Pharmacological interventions for benzodiazepine discontinuation in chronic benzodiazepine users Cochrane Database Syst Rev, 2018.PMID 29543325
- [7]Lader M, Kyriacou A Withdrawing Benzodiazepines in Patients With Anxiety Disorders Curr Psychiatry Rep, 2016.PMID 26733324
- [8]Lader M Benzodiazepine harm: how can it be reduced? Br J Clin Pharmacol, 2014.PMID 22882333
- [9]Markota M, Rummans TA, Bostwick JM, et al. Benzodiazepine Use in Older Adults: Dangers, Management, and Alternative Therapies Mayo Clin Proc, 2016.PMID 27814838
- [10]Glass J, Lanctôt KL, Herrmann N, et al. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits BMJ, 2005.PMID 16284208
- [11]Barker MJ, Greenwood KM, Jackson M, et al. Cognitive effects of long-term benzodiazepine use: a meta-analysis CNS Drugs, 2004.PMID 14731058
- [12]Pottie K, Thompson W, Davies S, et al. Deprescribing benzodiazepine receptor agonists: Evidence-based clinical practice guideline Can Fam Physician, 2018.PMID 29760253
- [13]Tannenbaum C, Martin P, Tamblyn R, et al. Reduction of inappropriate benzodiazepine prescriptions among older adults through direct patient education: the EMPOWER cluster randomized trial JAMA Intern Med, 2014.PMID 24733354
- [14]Brunner E, Chen CA, Klein T, et al. Joint Clinical Practice Guideline on Benzodiazepine Tapering: Considerations When Risks Outweigh Benefits J Gen Intern Med, 2025.PMID 40526204
- [15]Guina J, Merrill B Benzodiazepines I: Upping the Care on Downers: The Evidence of Risks, Benefits and Alternatives J Clin Med, 2018.PMID 29385731
- [16]Billioti de Gage S, Bégaud B, Bazin F, et al. Benzodiazepine use and risk of dementia: prospective population based study BMJ, 2012.PMID 23045258
- [17]Sun EC, Dixit A, Humphreys K, et al. Association between concurrent use of prescription opioids and benzodiazepines and overdose: retrospective analysis BMJ, 2017.PMID 28292769
- [18]Olfson M, King M, Schoenbaum M Benzodiazepine use in the United States JAMA Psychiatry, 2015.PMID 25517224
- [19]By the 2023 American Geriatrics Society Beers Criteria Update Expert Panel American Geriatrics Society 2023 updated AGS Beers Criteria for potentially inappropriate medication use in older adults J Am Geriatr Soc, 2023.PMID 37139824
- [20]Wilson S, Anderson K, Baldwin D, et al. British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders: An update J Psychopharmacol, 2019.PMID 31271339