Psych · Psychopharmacology — carbamazepine and oxcarbazepine
Carbamazepine and oxcarbazepine
Also known as Tegretol · Carbamazepine ERC · Equetro · Oxcarbazepine · Trileptal · CBZ · OXC · MHD licarbazepine
Exam-exhaustive fellowship psychopharmacology of carbamazepine and oxcarbazepine — Weisler ERC-CBZ mania RCTs, autoinduction and CYP3A4 induction (oral contraceptives), HLA-B1502 and HLA-A3101 severe cutaneous reaction risk, trough levels, OXC hyponatraemia, Wagner negative youth OXC trial, pregnancy hierarchy versus valproate, and CANMAT/ISBD placement. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
5 MCQs with explanations
Target exams
Red flags
Carbamazepine (CBZ) and oxcarbazepine (OXC) are medium-weight fellowship psychopharmacology because examiners stack mania trial literacy, autoinduction, contraceptive failure, pharmacogenetic rash screening, hyponatraemia, and honest evidence limits for OXC into one station. This leaf deepens the mood-stabiliser spine into a dual-agent monograph you can teach from cold.[1][3][12]
Definition and place in treatment
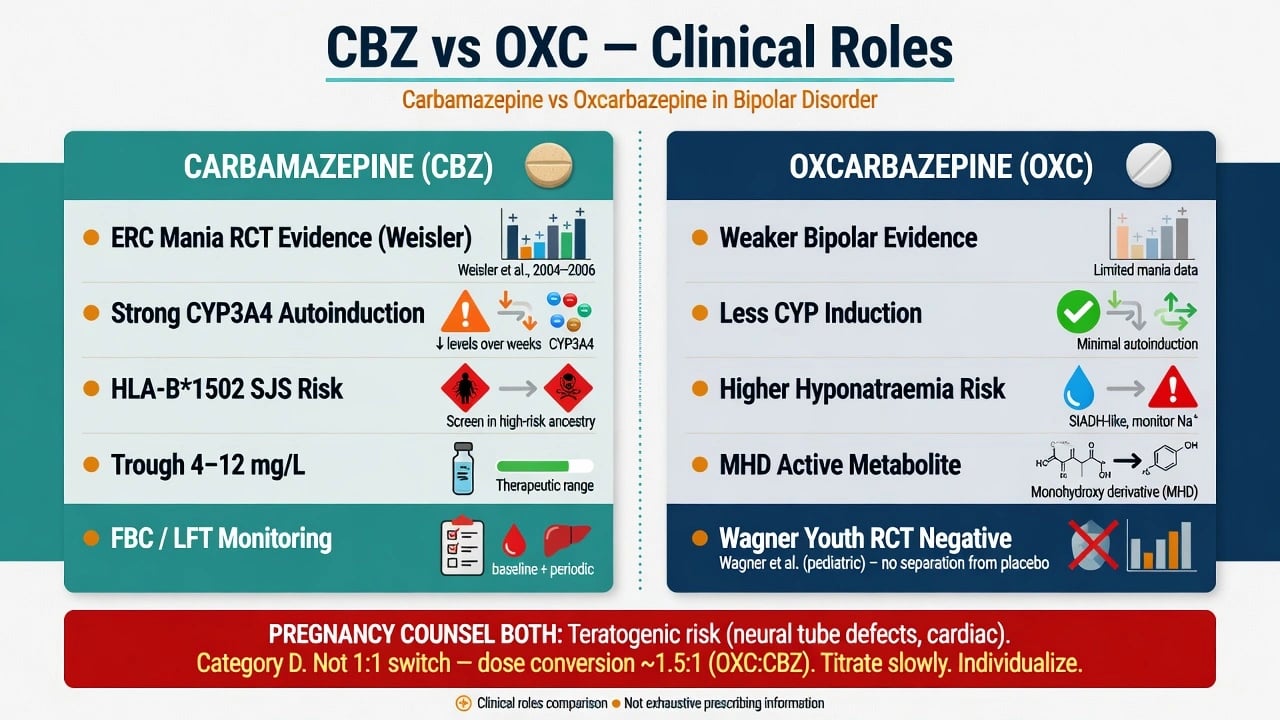
Carbamazepine is a dibenzazepine anticonvulsant used as a mood stabiliser. Immediate-release and extended/controlled-release products exist; extended-release carbamazepine capsules (ERC-CBZ) have the pivotal modern bipolar mania RCT programme examiners name (Weisler). Brand teaching (e.g. Tegretol, Equetro) is secondary to formulation kinetics and local product information.[1][2][3]
Oxcarbazepine is a 10-keto structural relative converted to the monohydroxy derivative (MHD, licarbazepine). It is not milligram-for-milligram interchangeable with CBZ, has a different induction and hyponatraemia profile, and has a weaker bipolar evidence base than CBZ ERC mania trials.[9][10][12]
| Use case | Exam stance |
|---|---|
| Acute mania / mixed (CBZ ERC) | Supported by Weisler placebo-controlled RCTs; still often second-line after lithium/valproate/SGA algorithms |
| CBZ maintenance | Thinner dedicated bipolar maintenance RCT portfolio than lithium; individualise if clear prior response |
| OXC for bipolar | Lower-tier / off-label in many algorithms; do not oversell |
| Youth bipolar OXC | Wagner 2006 negative vs placebo — do not invent first-line efficacy |
| People who can become pregnant | Prefer alternatives; CBZ MCM risk intermediate among ASMs (below valproate, not zero) |
| CBZ is a tool with interaction and SCAR overhead; OXC is not automatic rescue.[1][9][12][14] |
Mechanisms — viva depth without fluff
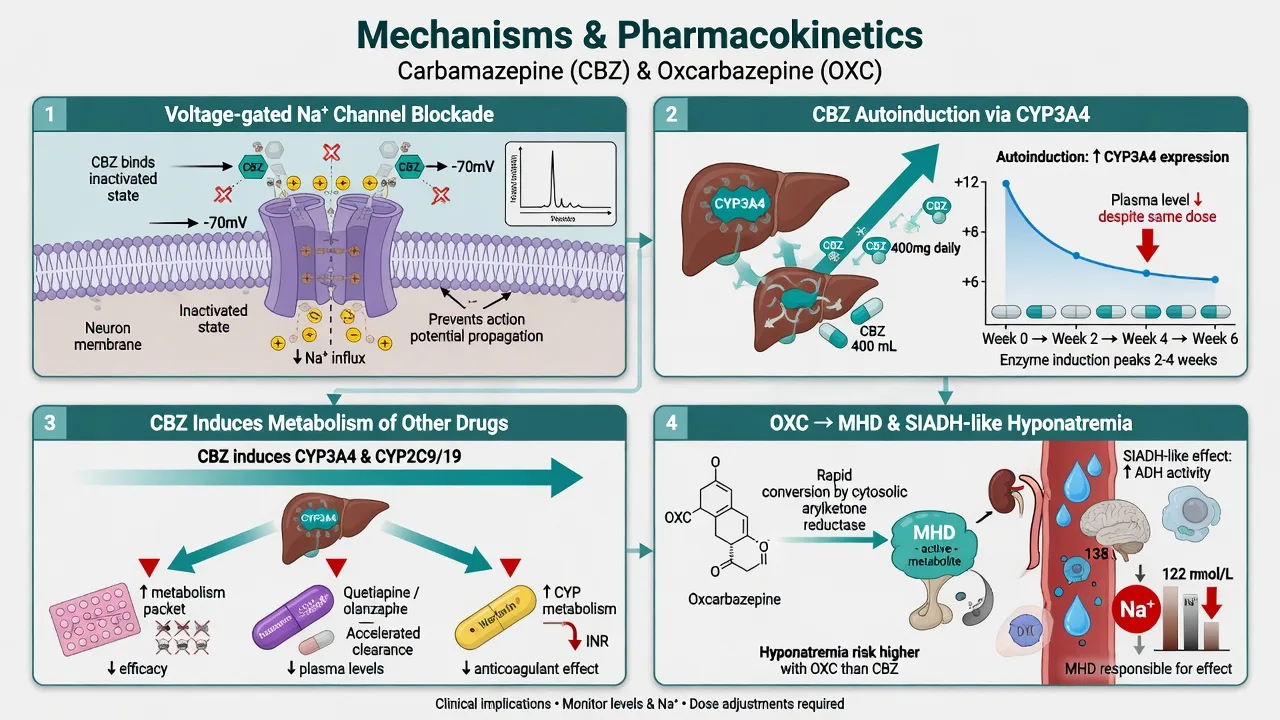
Voltage-gated sodium channel blockade. Use-dependent Na channel effects are the shared antiseizure and antimanic teaching core for both agents.[1][4]
CBZ metabolism and autoinduction. CBZ is oxidised to an active 10,11-epoxide and is a classic autoinducer of CYP3A4: clearance rises over the first weeks, so plasma levels often fall at a constant dose. Recheck trough after induction settles and after any interacting drug change — this is a standard viva trap for late “loss of effect.”[1][12]
Strong enzyme induction (CBZ). CBZ induces metabolism of combined hormonal contraceptives, many antipsychotics and antidepressants, warfarin and numerous other substrates. Counsel contraceptive failure risk and dual contraception when pregnancy prevention matters; review every co-medication list before start and at dose changes.[12]
OXC kinetics. Cytosolic reduction to MHD; weaker CYP3A4 induction than CBZ (still not zero for high-dose hormonal contraception teaching in some labels), with a greater propensity for hyponatraemia than CBZ in comparative neurology data.[10]
Severe cutaneous adverse reactions. HLA-restricted T-cell mechanisms link HLA-B*1502 to CBZ-related SJS/TEN in many Han Chinese and other East/South-East Asian groups (Chung; Chen screening), and HLA-A*3101 to a broader hypersensitivity spectrum in European ancestry (McCormack).[6][7][8]
Landmark evidence every candidate must own
Trials and genetics that change viva answers
Historical lineage. Ballenger and Post established early systematic interest in CBZ for manic-depressive illness; Okuma’s double-blind comparison with chlorpromazine embedded CBZ in antimanic teaching decades before modern ERC trials.[4][5]
Weisler ERC-CBZ mania programme. Multicentre randomised double-blind placebo-controlled trials showed extended-release carbamazepine capsules superior to placebo as monotherapy for bipolar I manic or mixed episodes; pooled analyses reinforced the antimanic signal. Name Weisler when asked for modern CBZ bipolar RCT evidence — not only epilepsy lore.[1][2][3]
Network context. Cipriani’s acute mania network meta-analysis frames comparative antimanic efficacy and acceptability across agents; CBZ appears in the field but is not the universal first pick over lithium, valproate or several SGAs in many algorithms — own the hierarchy honestly.[11][12]
Pharmacogenetics. Chung linked HLA-B1502 to CBZ-related SJS/TEN; Chen’s prospective Taiwan screening programme showed that avoiding CBZ in allele carriers can prevent CBZ-SJS/TEN. McCormack associated HLA-A3101 with CBZ hypersensitivity reactions in Europeans. These are named papers, not vague “genetic risk.”[6][7][8]
OXC youth trial. Wagner and colleagues found oxcarbazepine not superior to placebo in a double-blind RCT for bipolar disorder in children and adolescents — kill any casual first-line paediatric OXC claim.[9]
Hyponatraemia. Dong and colleagues quantified hyponatraemia with both agents and emphasised greater risk signals with oxcarbazepine relative to carbamazepine in their series — sodium monitoring is not optional decoration on OXC.[10]
Clinical selection algorithm
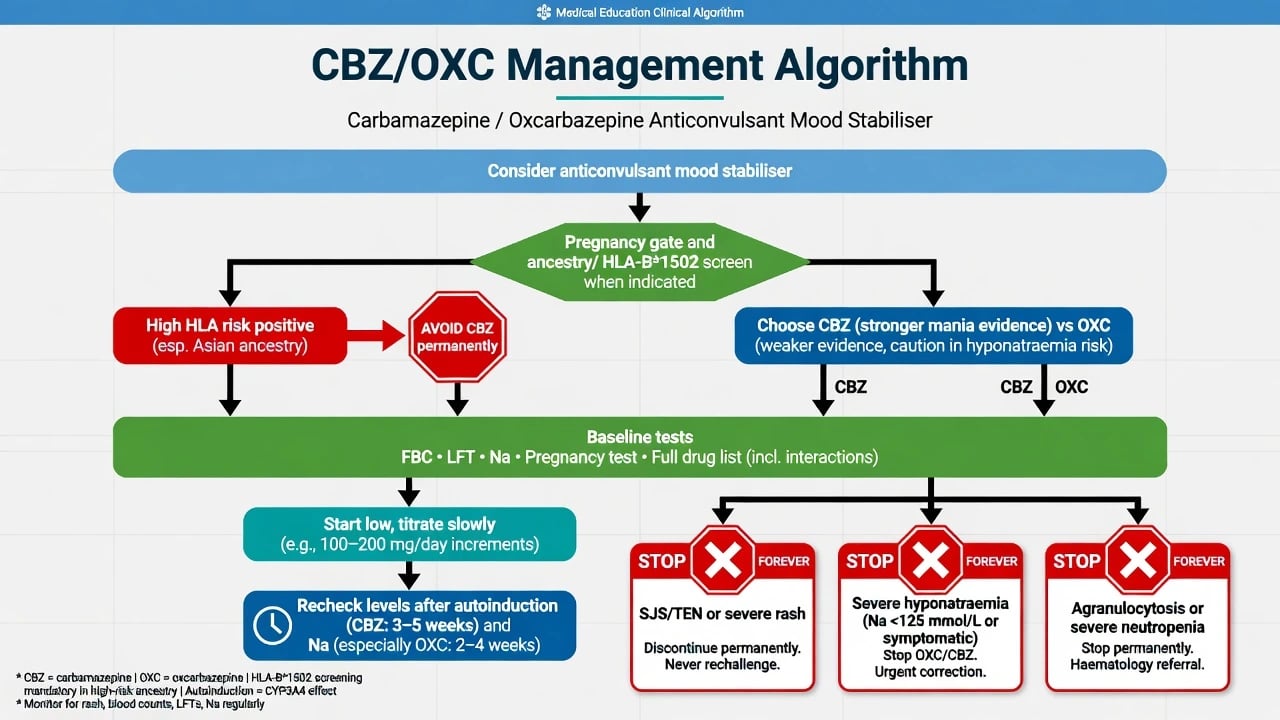
Prefer CBZ for acute mania when: lithium/valproate unsuitable or previously failed/intolerable, prior clear CBZ response, ERC formulation available, interaction list manageable, HLA-B*1502 screening completed when indicated, and pregnancy potential is managed with effective non-enzyme-vulnerable contraception planning.[1][2][7][12]
Prefer alternatives when: high HLA-B*1502 prevalence ancestry without timely screening; heavy CYP3A4-substrate polypharmacy (e.g. complex antipsychotic regimens, warfarin); OXC proposed as youth first-line; depression-pole maintenance better suited to lamotrigine/lithium strategies; inability to monitor FBC/LFT/Na or counsel SCAR risk.[7][9][12]
OXC niche. Selected adults who need an anticonvulsant-class option, cannot tolerate CBZ induction burden, accept weaker efficacy certainty, and can be monitored for hyponatraemia — not a default “safer CBZ clone.” Cross-reactivity for severe rash is possible; do not rechallenge with OXC after CBZ SJS/TEN.[9][10][12]
Dosing, levels and autoinduction
Teaching scaffolds always yield to local product information and hospital protocols.[12]
CBZ adult initiation (scaffold). Start low to reduce early neurotoxicity and rash risk — common teaching starts around 200 mg twice daily immediate-release (or product-specific ERC starts), titrating every few days by response and tolerability. Many adult psychiatric total daily doses land roughly 400–1600 mg/day, individualised to trough and side effects (diplopia, ataxia, sedation, nausea).[1][2][12]
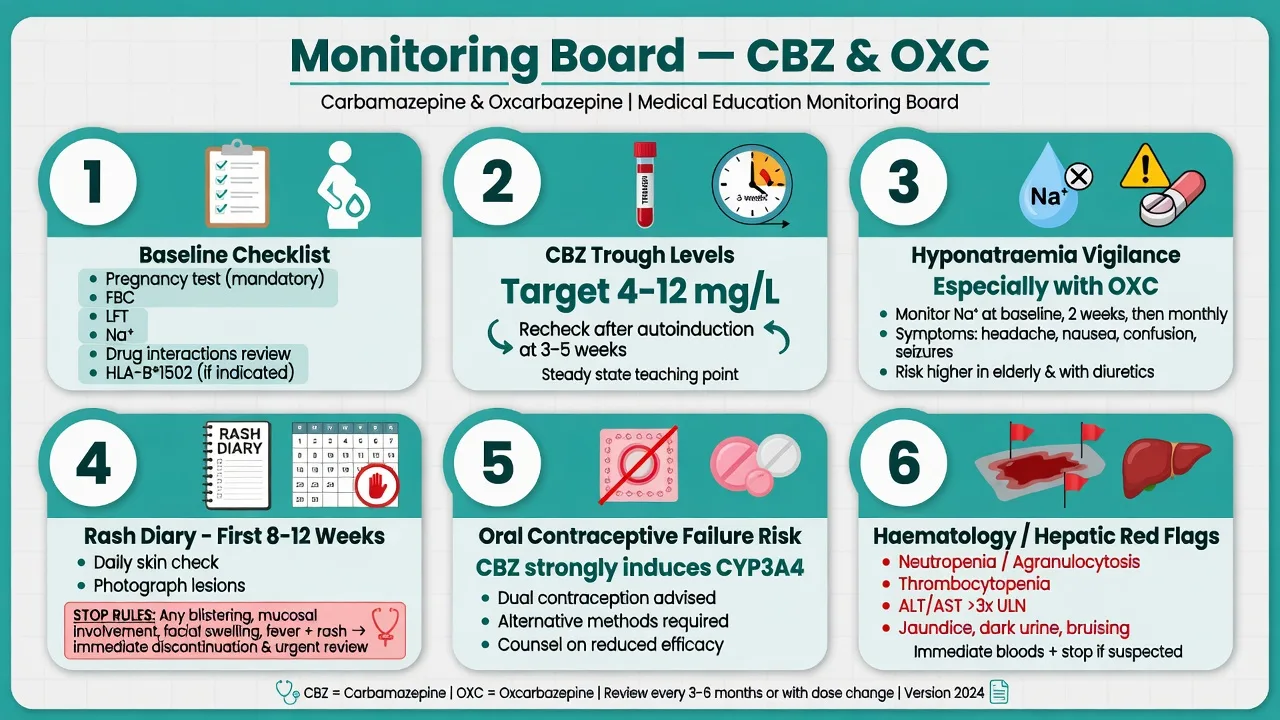
Serum levels. Draw trough samples. Class teaching therapeutic windows often cite about 4–12 mg/L (µg/mL). Recheck after autoinduction (commonly around 3–5 weeks of continuous therapy) and after interacting drug starts/stops; do not interpret a week-1 level as a lifelong set-point.[1][12]
OXC adult scaffold. Teaching starts often around 300 mg twice daily, titrating; bipolar use is typically off-label relative to epilepsy licensing. Monitor sodium closely during titration and after dose increases; levels of MHD are less routinely used in psychiatry than CBZ troughs but may appear in specialist settings.[9][10][12]
Pre-start assessment and monitoring
Baseline before first dose: ancestry and HLA-B*1502 when indicated/available; pregnancy test when relevant; contraception method (enzyme-induction risk for CBZ); FBC; LFT; electrolytes including sodium; full drug interaction list; capacity for early rash review and bloods; SCAR counselling with stop rules.[6][7][10][12]
Ongoing: clinical neurotoxicity and mood response; rash vigilance in the first weeks to months; serial Na especially on OXC and in older adults; periodic FBC/LFT for CBZ culture; trough CBZ after autoinduction and when non-response/toxicity/adherence/interaction issues arise.[7][8][10]
HLA screening and severe cutaneous reactions — highest exam stakes
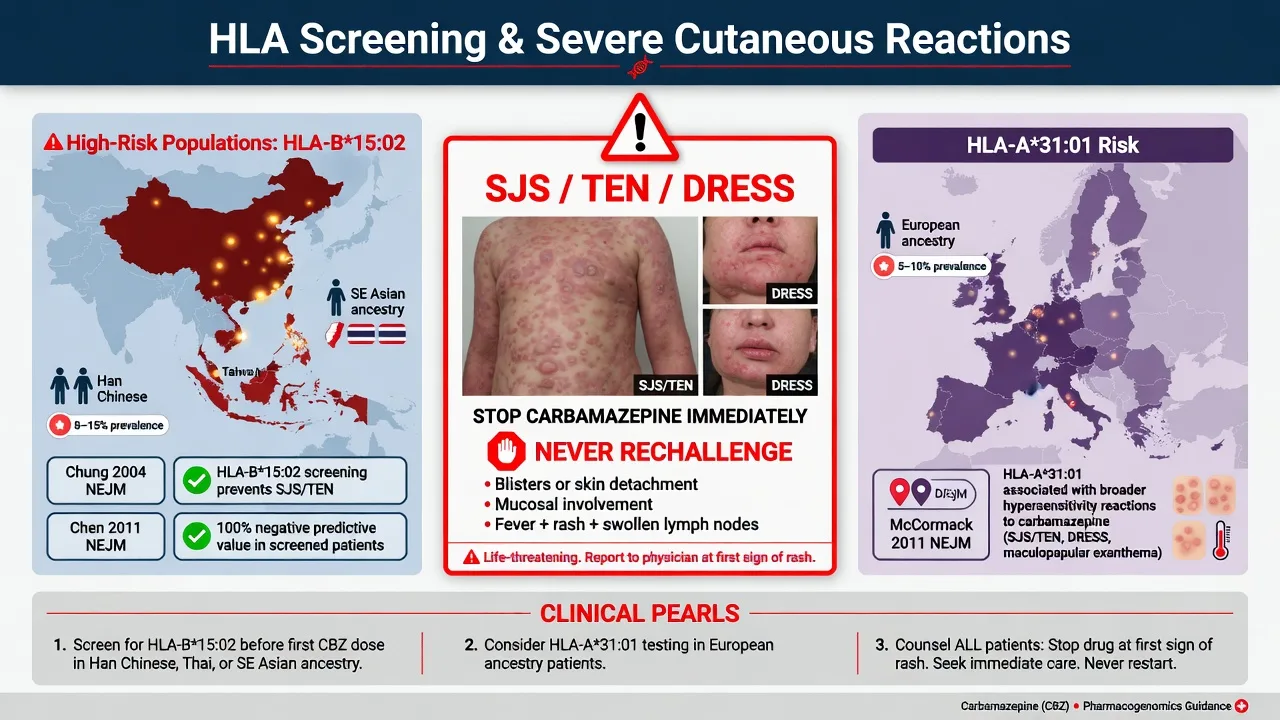
HLA-B*1502. Strong association with CBZ-induced SJS/TEN in Han Chinese and other at-risk Asian populations (Chung). Prospective screening with CBZ avoidance in carriers can prevent CBZ-SJS/TEN (Chen). Regulatory culture (FDA-style boxed warnings; local Asian screening standards) makes this examinable in ANZ with culturally diverse populations — ask ancestry and arrange testing before first dose when risk is material.[6][7]
HLA-A*3101. Associated with CBZ hypersensitivity spectrum (including milder rash through severe reactions) in European ancestry (McCormack). Screening practice is less uniformly mandated than B*1502 in many systems, but risk counselling still matters.[8]
Stop rules. Any suspected SJS/TEN (mucosal involvement, blistering, skin detachment, systemic toxicity) or DRESS (fever, lymphadenopathy, organ involvement, facial oedema): stop immediately, escalate dermatology/ICU pathways, never rechallenge. Benign early morbilliform rashes still warrant urgent clinical review — when in doubt, hold and escalate rather than “watch for a week.”[6][7][8]
Hyponatraemia
OXC carries a higher hyponatraemia burden than CBZ in comparative data; both can lower sodium via SIADH-like mechanisms. Risk rises in older adults, with diuretics, and at higher doses. Check baseline Na, recheck during titration, and urgently if confusion, seizures, falls or headache appear. Severe symptomatic hyponatraemia: hold the drug and correct sodium under medical protocols.[10]
Pregnancy and teratogenicity
Do not treat CBZ as pregnancy-safe. EURAP analyses show dose-related and comparative major congenital malformation risk across antiseizure medicines; valproate ranks higher, but CBZ is not risk-free and requires specialist perinatal planning, folic acid per local guidance, and preferably preconception switch when bipolar allows. OXC data are thinner for psychiatry-focused counselling — still specialist territory. Enzyme-inducing CBZ additionally threatens contraceptive efficacy — a double hit for unplanned pregnancy.[12][13][14]
Other complications and pitfalls
| Problem | First move |
|---|---|
| Diplopia, ataxia, sedation | Level check, dose reduce, formulation review |
| Early rash | Urgent review; stop if SCAR features |
| Hyponatraemia | Na check, hold if severe/symptomatic |
| Cytopenia / fever / sore throat | Urgent FBC; stop if marrow failure suspected |
| Hepatic injury | Stop, LFTs, synthetic function |
| OC failure risk | Dual contraception counselling; non-enzyme plan |
| Late loss of CBZ effect | Recheck trough after autoinduction |
| Common traps for viva speed.[1][7][10][12] |
Pitfalls that fail stations: starting CBZ without HLA-B*1502 when indicated; selling OXC as proven paediatric bipolar therapy; ignoring contraceptive induction; worshipping a day-3 level after autoinduction; rechallenge after SJS; treating OXC as interaction-free; missing sodium on OXC; equating CBZ with valproate pregnancy risk (wrong direction) or with zero risk (also wrong).[7][9][10][14]
Special populations
Ancestry and pharmacogenetics. Highest priority safety gate for CBZ — B1502 workflow in at-risk groups; A3101 awareness in European ancestry.[6][7][8]
People who can become pregnant. Prefer non-inducing alternatives when feasible; counsel MCM risk and contraceptive failure on CBZ; specialist perinatal if continuing.[12][13][14]
Older adults. Lower starts, falls from ataxia/sedation, hyponatraemia, polypharmacy induction chaos.[10][12]
Youth. Wagner negative OXC RCT; specialist only for any off-label use; do not default to OXC for paediatric bipolar.[9]
Hepatic disease / complex CL polypharmacy. Caution with CBZ induction and hepatotoxicity monitoring; often prefer agents with cleaner interaction profiles.[12]
Prognosis and disposition
Acute mania often improves over 1–3 weeks once sleep and agitation are controlled and CBZ levels are adequate post-titration. Long-term: continue only with clear benefit, manageable interactions, and monitoring capacity. Admit for severe mania risk, SCAR, severe hyponatraemia, or marrow/hepatic catastrophes.[1][2][7][10]
Evidence, guidelines and regional differences
| Source | Exam take-home |
|---|---|
| Weisler 2004/2005/2006 | ERC-CBZ antimanic RCT evidence |
| Ballenger–Post / Okuma | Historical CBZ bipolar lineage |
| Chung / Chen / McCormack | HLA-B1502 and HLA-A3101 SCAR genetics |
| Wagner 2006 | OXC youth bipolar RCT negative |
| Dong 2005 | Hyponatraemia OXC more than CBZ signal |
| Cipriani 2011 | Antimanic network field |
| EURAP Tomson | Comparative MCM risk (CBZ less than VPA) |
| CANMAT/ISBD 2018 | Algorithmic bipolar placement with safety gates |
| Landmark synthesis for viva speed.[1][2][6][7][8][9][10][11][12][14] |
ANZ: Diverse ancestry makes HLA-B1502 screening relevant in many clinics; RANZCP-aligned bipolar care still privileges lithium/valproate/SGA pathways with CBZ as alternative antimanic. UK: NICE bipolar pathways and MHRA-style product warnings for serious skin reactions and interactions. US: FDA-approved ERC-CBZ for acute manic/mixed bipolar I; boxed warning culture for HLA-B1502 and serious dermatologic reactions. East Asia: Chen-style prospective B*1502 screening is standard-of-care culture. Exact forms differ — the clinical hierarchy of screen, counsel, and stop does not.[1][7][12]
Exam pearls
CBZ strengths
- Weisler ERC mania RCTs
- Okuma/Ballenger lineage
- Option when Li/VPA fail
- Trough-guided titration
CBZ costs
- CYP3A4 autoinduction
- OC and co-med failure
- HLA-linked SJS/TEN
- FBC/LFT culture
OXC profile
- Less enzyme induction
- More hyponatraemia
- Weaker bipolar evidence
- Wagner youth negative
Shared gates
- Rash stop rules
- Pregnancy counselling
- Na monitoring
- Not 1:1 interchangeable
References
- [1]Weisler RH, Kalali AH, Ketter TA, et al. A multicenter, randomized, double-blind, placebo-controlled trial of extended-release carbamazepine capsules as monotherapy for bipolar disorder patients with manic or mixed episodes J Clin Psychiatry, 2004.PMID 15119909
- [2]Weisler RH, Keck PE Jr, Swann AC, et al. Extended-release carbamazepine capsules as monotherapy for acute mania in bipolar disorder: a multicenter, randomized, double-blind, placebo-controlled trial J Clin Psychiatry, 2005.PMID 15766298
- [3]Weisler RH, Hirschfeld R, Cutler AJ, et al. Extended-release carbamazepine capsules as monotherapy in bipolar disorder: pooled results from two randomised, double-blind, placebo-controlled trials CNS Drugs, 2006.PMID 16529527
- [4]Ballenger JC, Post RM Carbamazepine in manic-depressive illness: a new treatment Am J Psychiatry, 1980.PMID 7386656
- [5]Okuma T, Inanaga K, Otsuki S, et al. Comparison of the antimanic efficacy of carbamazepine and chlorpromazine: a double-blind controlled study Psychopharmacology (Berl), 1979.PMID 119267
- [6]Chung WH, Hung SI, Hong HS, et al. Medical genetics: a marker for Stevens-Johnson syndrome Nature, 2004.PMID 15057820
- [7]Chen P, Lin JJ, Lu CS, et al. Carbamazepine-induced toxic effects and HLA-B*1502 screening in Taiwan N Engl J Med, 2011.PMID 21428768
- [8]McCormack M, Alfirevic A, Bourgeois S, et al. HLA-A*3101 and carbamazepine-induced hypersensitivity reactions in Europeans N Engl J Med, 2011.PMID 21428769
- [9]Wagner KD, Kowatch RA, Emslie GJ, et al. A double-blind, randomized, placebo-controlled trial of oxcarbazepine in the treatment of bipolar disorder in children and adolescents Am J Psychiatry, 2006.PMID 16816222
- [10]Dong X, Leppik IE, White J, Rarick J Hyponatremia from oxcarbazepine and carbamazepine Neurology, 2005.PMID 16380624
- [11]Cipriani A, Barbui C, Salanti G, et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis Lancet, 2011.PMID 21851976
- [12]Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder Bipolar Disord, 2018.PMID 29536616
- [13]Tomson T, Battino D, Bonizzoni E, et al. Dose-dependent risk of malformations with antiepileptic drugs: an analysis of data from the EURAP epilepsy and pregnancy registry Lancet Neurol, 2011.PMID 21652013
- [14]Tomson T, Battino D, Bonizzoni E, et al. Comparative risk of major congenital malformations with eight different antiepileptic drugs: a prospective cohort study of the EURAP registry Lancet Neurol, 2018.PMID 29680205