Psych · Psychopharmacology — clozapine
Clozapine
Also known as Clozaril · Clopine · Treatment-resistant schizophrenia clozapine · Clozapine monitoring · TRS clozapine
Exam-exhaustive fellowship reference on clozapine — TRRIP entry, titration, plasma levels, region-aware haematology principles, myocarditis and cardiomyopathy, constipation/ileus, seizures, hypersalivation, metabolic risk, smoking/CYP1A2, InterSePT, Siskind response rates, rechallenge, elderly slow titration. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Clozapine is a high-stakes, high-yield fellowship topic because examiners test indication discipline, protocol literacy, and lethal adverse-effect recognition in the same station. Kane established superiority in treatment resistance; modern meta-analysis confirms meaningful response rates; InterSePT supports an anti-suicide role; monitoring systems exist because agranulocytosis, myocarditis and ileus kill when protocols fail.[1][3][4][5][8][10][13]
Definition and place in treatment
Clozapine is a dibenzodiazepine multi-receptor antipsychotic (low D2 occupancy relative to many FGAs, strong 5-HT2A and other receptor actions) reserved for treatment-resistant schizophrenia (TRS) and selected high-risk scenarios, not as a casual first-line tablet. Network meta-analysis places it at the top of antipsychotic efficacy rankings; that ranking is not a licence to skip monitoring.[6][24]
Core indications examiners expect you to name: (1) schizophrenia spectrum illness meeting TRS criteria after two adequate failed antipsychotic trials; (2) high suicide risk in schizophrenia/schizoaffective disorder where clozapine is indicated (InterSePT context); (3) specialist niches (historically Parkinson disease psychosis) only with extreme caution and modern alternatives considered.[1][2][3][24]
TRRIP entry criteria — when clozapine becomes the answer
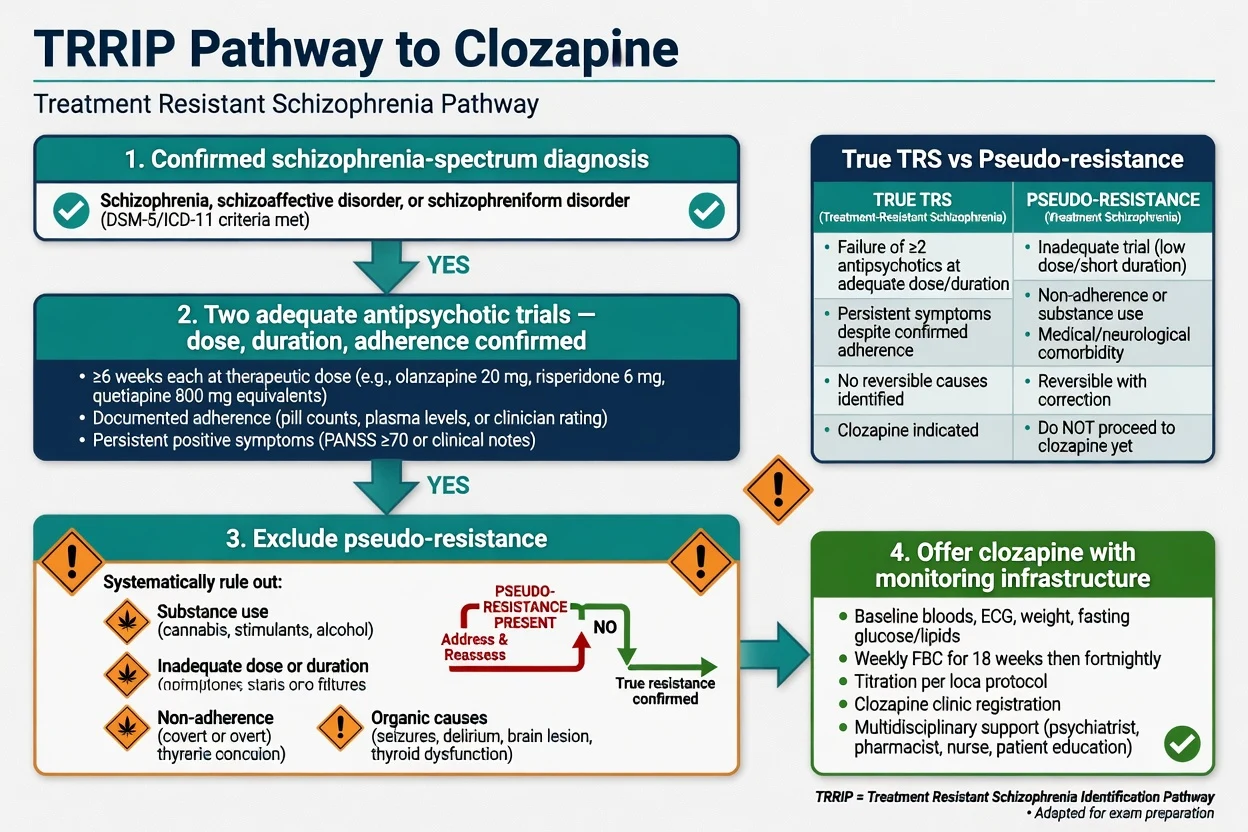
The TRRIP (Treatment Response and Resistance in Psychosis) consensus defines treatment-resistant schizophrenia for research and clinical clarity: confirmed schizophrenia-spectrum diagnosis, inadequate response to at least two different antipsychotics given at an adequate dose and duration with adherence confirmed, and exclusion of pseudo-resistance.[2]
| Construct | Exam meaning |
|---|---|
| Adequate trial | Therapeutic dose range, typically around 6 weeks at target dose (document local practice), adherence verified |
| True TRS | Persistent symptoms despite two adequate adherent trials |
| Pseudo-resistance | Wrong diagnosis, substance use, non-adherence, under-dosing, organic contributors |
| Clozapine offer | Not optional theatre after years of polypharmacy — offer when TRS criteria are met if monitoring is available |
| TRRIP is the language that turns "try another SGA" into a defensible decision pathway.[2] |
Kane 1988 remains the foundational TRS trial: clozapine outperformed chlorpromazine in rigorously defined treatment-resistant schizophrenia. That principle still structures every modern guideline conversation about delayed clozapine.[1]
Epidemiology, under-use and the mortality paradox
Response rates. Siskind and colleagues' systematic review and meta-analysis show that a substantial proportion of people with TRS respond when clozapine is used properly — the exam message is offer earlier, not later, because delayed clozapine is a system failure, not a virtue of caution.[4][5]
Under-utilisation is global: fear of monitoring, service gaps, clinician inertia ("clozaphobia"), and patient/family fear after incomplete counselling. Examiners reward candidates who can consent to risks and state the cost of untreated TRS (relapse, suicide, institutionalisation).[4][24]
Mortality paradox. FIN11-style population data associate antipsychotic treatment, including clozapine, with lower mortality than no antipsychotic in schizophrenia cohorts — argue for treated illness while still attacking drug-specific lethal risks (neutropenia, myocarditis, ileus, metabolic disease).[7][8][10][13]
Numbers every candidate must own
Landmark anchors above are exam orientation numbers from Kane, TRRIP, InterSePT, Siskind, concentration–response teaching and myocarditis series — always individualise levels and monitoring to the patient and local protocol.[1][2][3][4][11][18]
Pathophysiology and receptor map
Clozapine's clinical fingerprint is multi-receptor: dopamine D2 (loose binding / relatively low occupancy explaining low EPS), 5-HT2A, H1 (sedation, weight), M1 (anticholinergic gut and cognition effects), alpha-1 (orthostasis), and other targets. Low EPS is real; constipation risk is the anticholinergic price you must prevent actively.[6][13][24]
Metabolism. Primary pathway is CYP1A2 to norclozapine; smoking polycyclic aromatic hydrocarbons induce CYP1A2 and lower levels; smoking cessation or potent CYP1A2 inhibitors (classically fluvoxamine) raise levels and toxicity risk. Age, sex, and dose also shape concentration — predictive models exist for teaching adjustment logic.[16][17]
Agranulocytosis is idiosyncratic, highest risk early in treatment historically, and the reason mandatory haematology registries exist; incidence estimates from early US experience underpin modern monitoring culture even as absolute rates are managed by systems.[8]
Myocarditis presents as an early inflammatory/hypersensitivity pattern; rapid titration and concomitant sodium valproate are documented risk amplifiers in case-control work.[10][11][12]
CIGH (clozapine-induced gastrointestinal hypomotility) is anticholinergic gut paralysis on a spectrum from constipation to toxic megacolon and death — pharmacovigilance series make this a board-level red flag, not a nursing afterthought.[13][14][15]
Clinical effects and time course
Expect positive symptom improvement over weeks; judge response with documented dose and plasma level context, not after three under-dosed days. Partial response still matters. Some patients need months at an adequate level before you declare clozapine failure and escalate to augmentation strategies for ultra-resistant illness.[4][18][19][24]
Common tolerability issues: sedation, tachycardia, orthostatic hypotension, hypersalivation, weight gain, nocturnal enuresis, constipation, metabolic disturbance. Each is manageable if anticipated; each is examinable as a pitfall if ignored.[22][24]
Differentials that save lives
| Presentation on clozapine | Prefer | Do not miss |
|---|---|---|
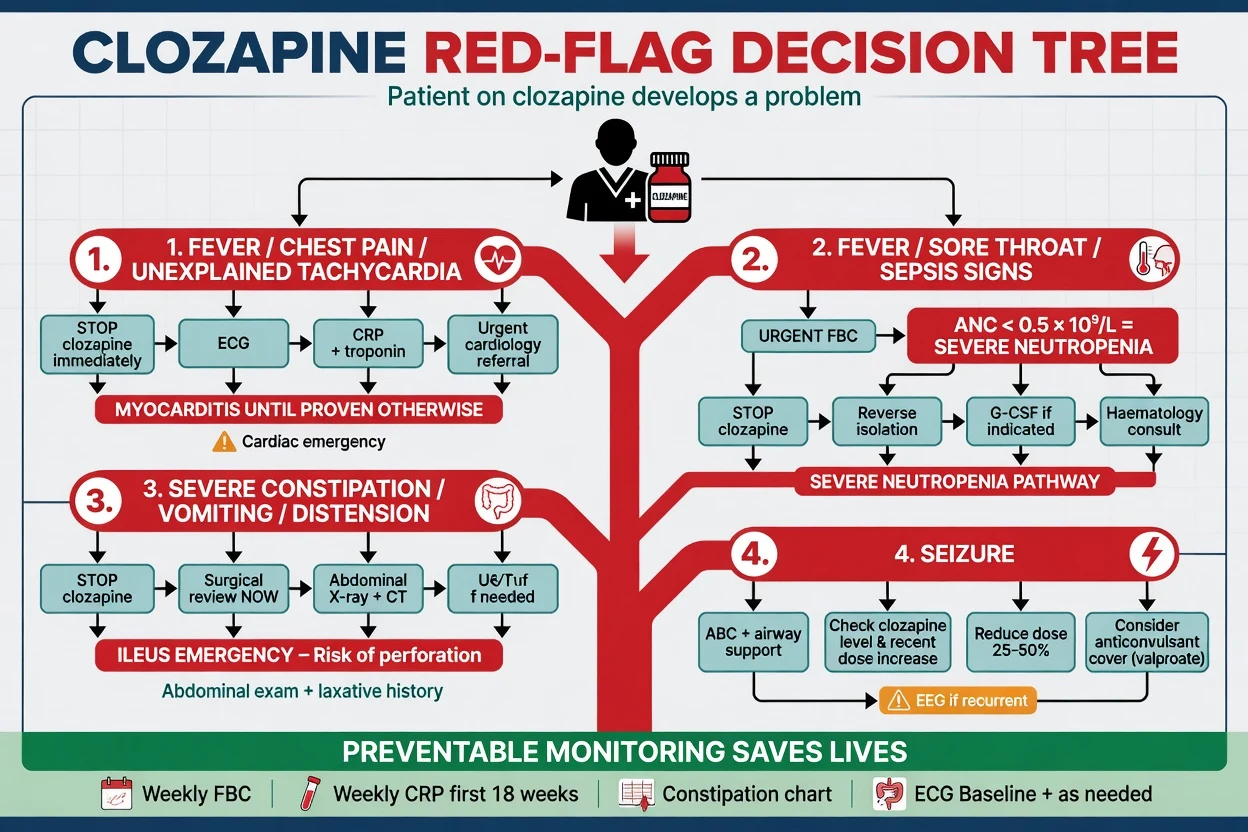
| Early fever + tachycardia ± chest pain | Myocarditis work-up; stop clozapine | "Just a virus" without CRP/troponin/ECG |
| Fever + sore throat + unwell | Neutropenia until FBC proves otherwise | Discharging without bloods |
| Abdominal pain, vomiting, no flatus/stool | Ileus/obstruction surgical pathway | Another stimulant laxative and hope |
| Worsening psychosis | Levels, smoking change, non-adherence, substances | Blind dose escalation without levels |
| Rigidity + fever + autonomic instability | NMS spectrum (any dopamine blocker) | Assuming only myocarditis |
| Fever on clozapine is a protocol, not a guess.[11][13][22] |
Pre-start assessment and service readiness
Before first dose, document: TRRIP-eligible indication; capacity/consent or legal framework; baseline FBC with ANC; metabolic panel (glucose/HbA1c, lipids, weight/BMI/waist); ECG; CRP ± troponin as per local myocarditis protocol; bowel history and laxative plan; smoking status and nicotine products; full medication list (fluvoxamine, carbamazepine, other bone-marrow toxins, anticholinergics); pregnancy status when relevant; and whether the service can actually deliver protocol bloods and act on red results.[2][20][22][24]
If monitoring infrastructure is absent, do not start. Clozapine without bloods is not courage — it is negligence framed as advocacy.[8][24]
Investigations and monitoring principles
Haematology (region-aware)
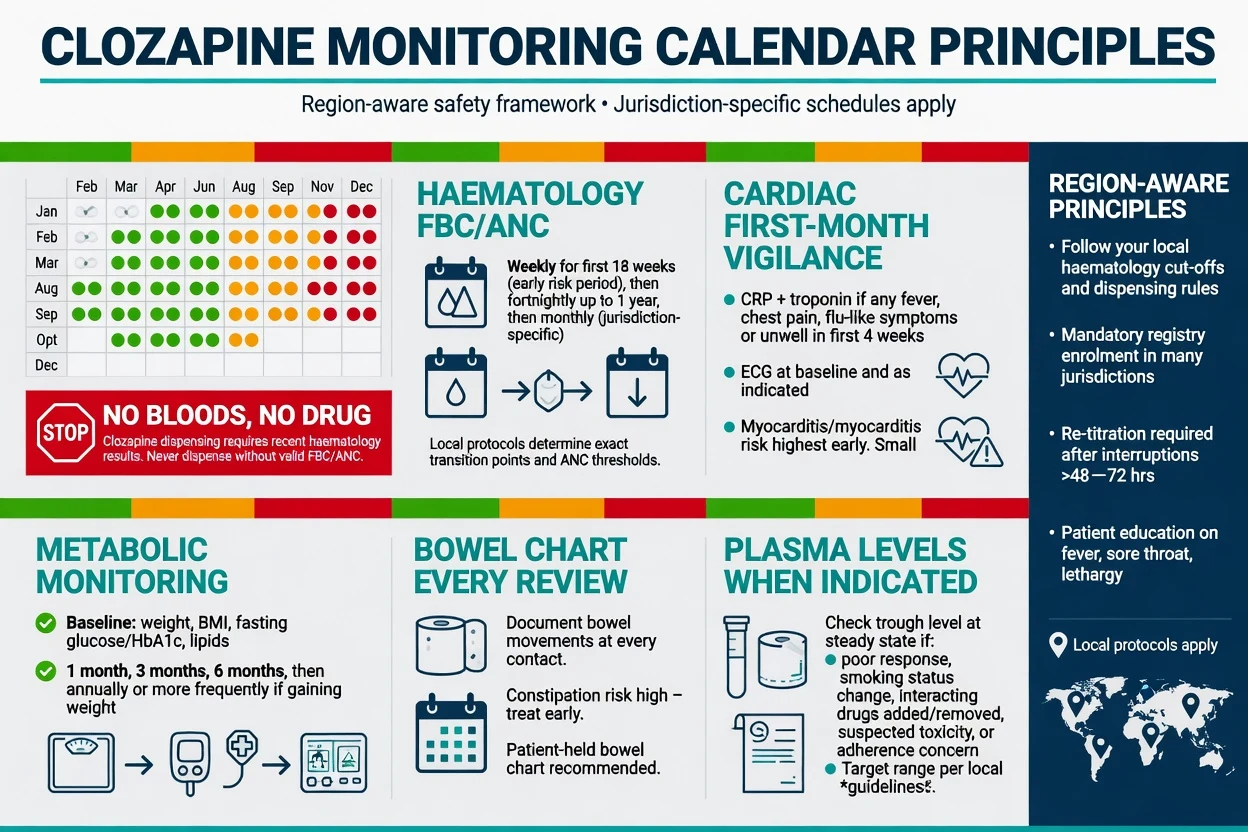
Mandatory neutrophil monitoring is non-negotiable. Exact schedules, green/amber/red bands, and dispensing locks are jurisdiction-specific (Australian/NZ patient monitoring systems, UK CPMS-style programmes, US REMS). Exam-safe principles: more frequent bloods early (commonly weekly for the first months), then less frequent if stable (fortnightly then monthly patterns in many systems); never dispense without a valid result; act immediately on severe neutropenia.[8][24]
Do not invent one country's exact ANC cut-offs as universal law in a viva. State principles, name that local product information and registry rules govern thresholds, and show you would look them up and follow them.[24]
Cardiac and "beyond WBC"
First-month vigilance for myocarditis is as important as blood counts. Cohen and colleagues argued for broader early-phase screening beyond white cells alone. Kilian and Ronaldson series define the clinical picture: fever, tachycardia, chest pain, flu-like illness, raised CRP and troponin, often within the first weeks.[10][11][22]
Plasma levels
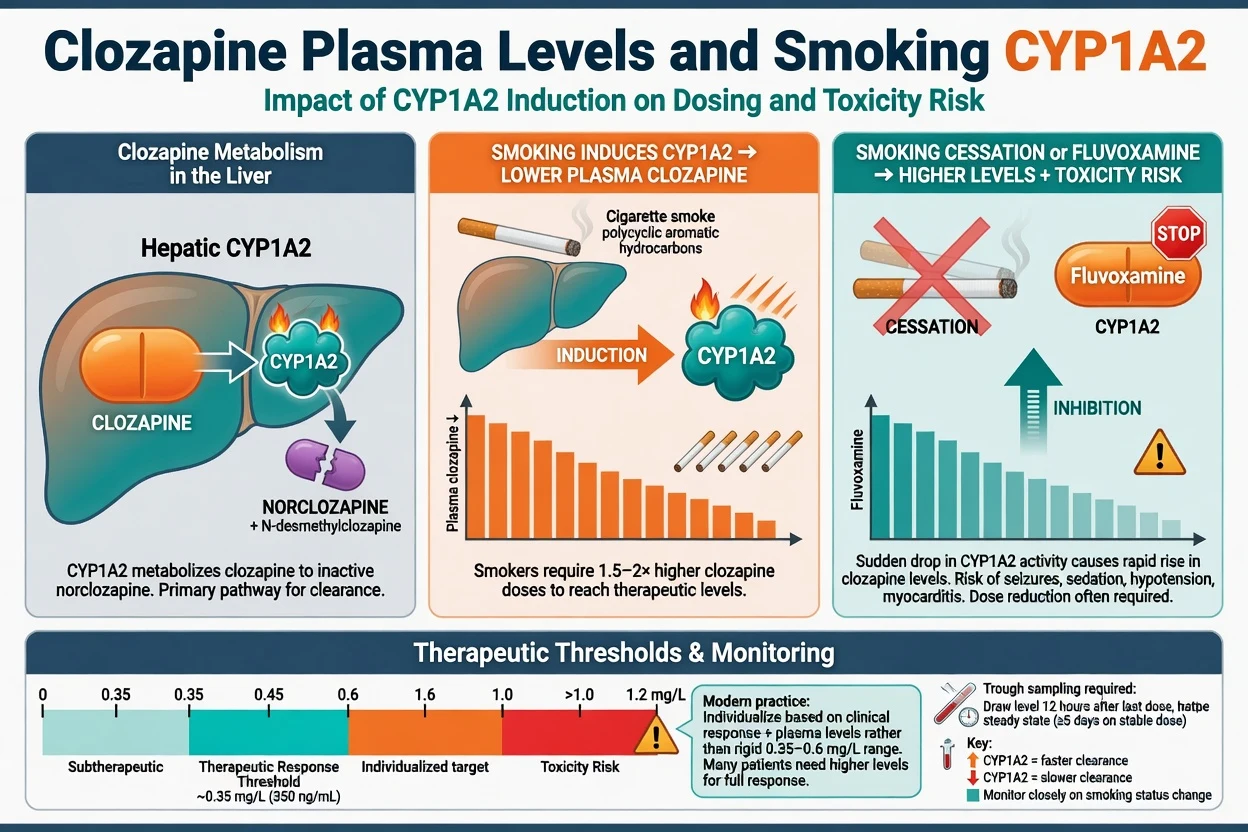
Classic teaching uses a response threshold around 0.35 mg/L (350 ng/mL) trough clozapine from early concentration–response work; modern individual-patient data analyses refine optimisation and remind you that response is individual, toxicity rises with high levels, and sampling should be trough at steady state.[18][19][23]
AGNP-style TDM consensus supports therapeutic drug monitoring as a tool for non-response, adherence questions, interaction management, and toxicity — not as a substitute for clinical judgement.[23]
Initiation and titration
Slow titration principles follow safer international guidance and myocarditis risk data — product information remains the local authority for exact schedules.[12][20]
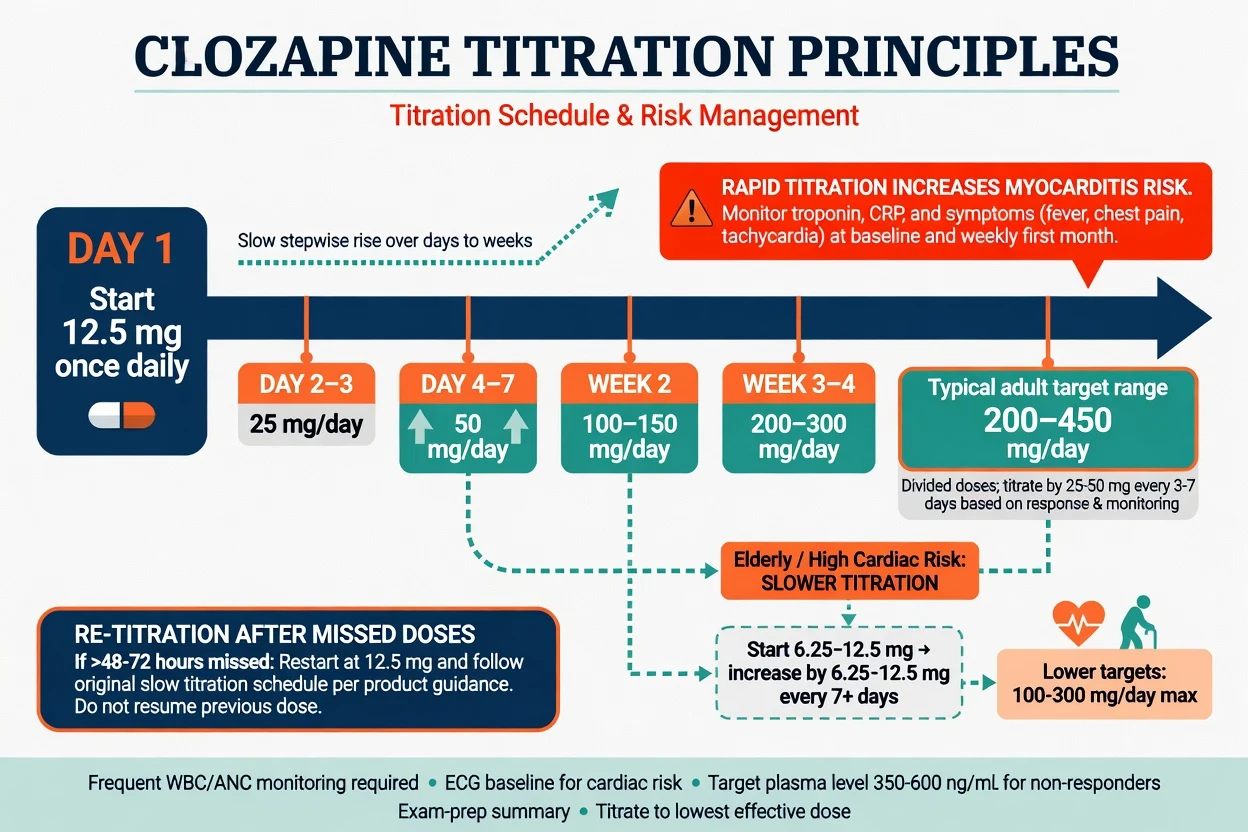
Typical adult pattern (teaching scaffold — always check local product information): start 12.5 mg, rise slowly over days to weeks, many adults land in a 200–450 mg/day range divided doses, individualised by tolerability and levels. de Leon and colleagues' international titration guideline emphasises safer, ancestry-informed slower schedules with CRP and level-informed care — the spirit is personalised slow titration, not macho dose racing.[12][20][24]
Elderly and high cardiac risk: much slower titration, lower targets often, falls and orthostasis vigilance, constipation risk amplified. Rapid titration and valproate co-prescription increase myocarditis risk in case-control data — if valproate is needed for seizures or mood, document the trade-off and monitor harder, do not pretend the interaction is theoretical.[12][20]
Missed doses: multi-day interruptions generally require re-titration from a low dose per product guidance (commonly taught around 48–72 hours thresholds — follow the local SmPC exactly). Never slam back to the previous maintenance dose after a prolonged gap.[20][24]
Emergency management of life-threatening adverse effects
Severe neutropenia / agranulocytosis
Stop clozapine immediately. Urgent FBC confirmation, infection work-up, isolation as indicated, hospitalise, involve haematology, G-CSF when appropriate. Do not restart without a specialist rechallenge pathway. Historical incidence data justify the entire monitoring industry around this drug.[8][21][24]
Myocarditis
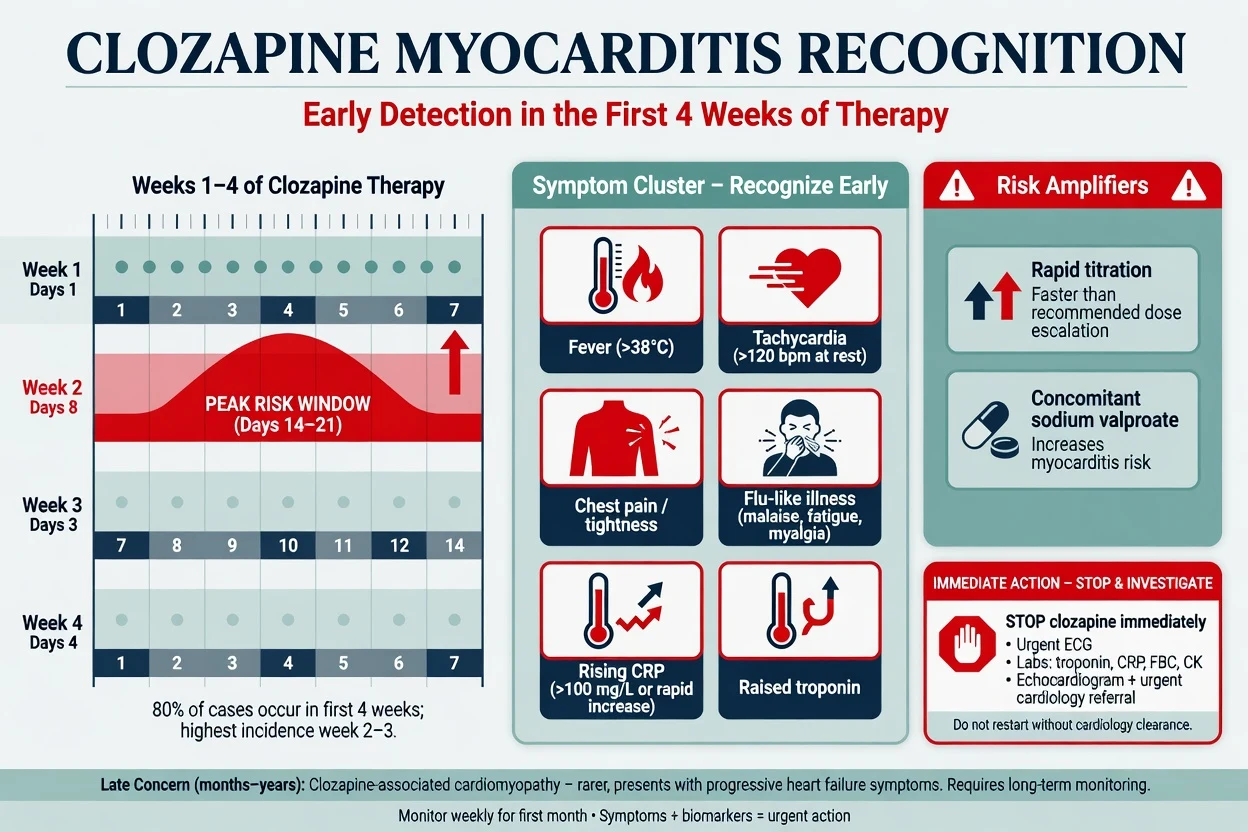
Stop clozapine. ECG, CRP, troponin, cardiology/echo. Do not push the dose while "observing." Late cardiomyopathy is a separate, rarer concern with progressive heart-failure phenotype — still examine and investigate when the story fits.[10][11][12]
Constipation, CIGH and ileus
Prevent from day one with a proactive laxative protocol, bowel chart, and review at every contact. Serious CIGH presents with constipation, abdominal pain, vomiting, distension; mortality is real in pharmacovigilance series. Emergency: stop clozapine and other anticholinergics, surgical review, imaging — this is not "wait and see."[13][14][15]
Seizures
Dose- and level-related risk rises at higher exposures; large series quantify clozapine-related seizures. Manage ABC, check recent dose changes, levels, smoking cessation, and interacting drugs. Dose reduction and/or anticonvulsant cover (valproate commonly discussed — monitor levels and myocarditis risk trade-offs) may allow continuation when benefit is clear; do not casually abandon a life-changing response without a plan.[9][12][24]
Definitive management beyond the emergency
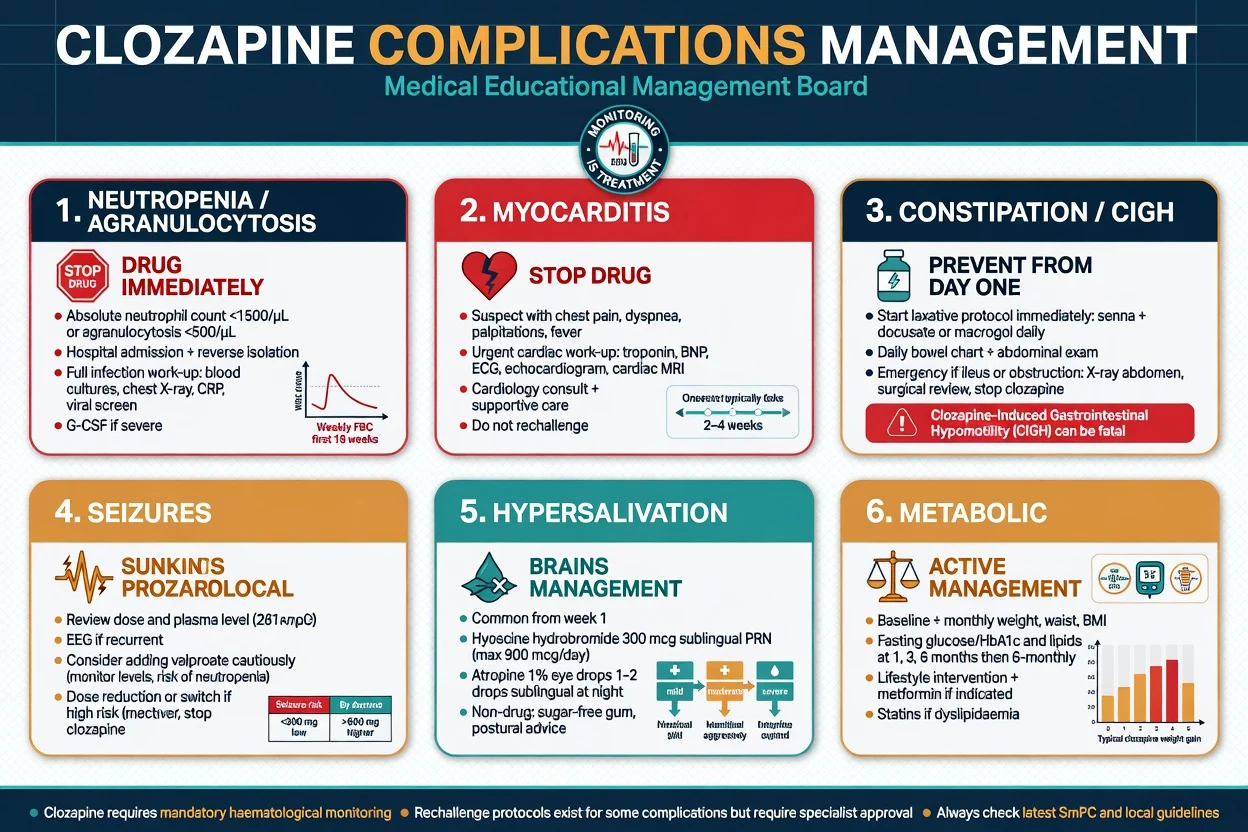
Hypersalivation. Common and socially disabling; options include hyoscine hydrobromide, sublingual atropine drop protocols in specialist practice, postural advice, and dental care — balance anticholinergic load against gut risk.[24]
Metabolic. Clozapine is metabolically heavy. Baseline and longitudinal weight, glucose/HbA1c, lipids; lifestyle intervention; metformin and cardiometabolic pathways as indicated; do not celebrate psychiatric improvement while ignoring diabetes trajectory.[7][22][24]
Smoking changes. Document cigarettes/day and any vaping/nicotine replacement. Smoking induces CYP1A2 and lowers clozapine levels; cessation raises levels — pre-empt dose reduction and level checks when patients stop smoking in hospital.[16][17]
Key interactions (exam favourites): fluvoxamine (marked level rise); smoking cessation (level rise); carbamazepine (avoid — marrow risk and enzyme induction); other bone-marrow toxic agents; stacked anticholinergics worsening CIGH.[16][17][24]
Clozapine-resistant (ultra-resistant) schizophrenia. Confirm adherence and adequate level first. Augmentation strategies are specialist (selected antipsychotics, ECT in appropriate cases, psychosocial intensification) — evidence hierarchy over polypharmacy chaos.[4][5][24]
Rechallenge principles
Rechallenge after major adverse effects is not automatic. Manu and colleagues synthesised case series into clinical guidelines: risk differs by reaction type (neutropenia vs myocarditis vs other). Neutropenia rechallenge may be considered in highly selected cases with intensive monitoring and haematology partnership; myocarditis rechallenge is far more cautious and often avoided. Ileus survivors need gut protocols before any discussion of restart. Document multidisciplinary decision and informed consent.[21]
Special populations
Older adults. Slow titration, lower targets, fall and cardiac risk, constipation, anticholinergic delirium risk, shared decision with physical health services.[20][24]
Youth / early TRS. Do not wait a decade of failed polypharmacy; engage family, metabolic intensity, education about monitoring burden.[2][4]
Pregnancy and lactation. Specialist perinatal psychiatry; untreated psychosis harms mother and fetus; individualised risk–benefit with obstetric partners — no casual online dosing.[24]
Intellectual disability / autism with psychosis. Capacity, communication, constipation risk, and sensory issues amplify monitoring complexity.[24]
Cultural and access barriers. Smoking prevalence, transport to blood tests, and trust shape real-world clozapine success — exam answers that ignore access fail community psychiatry stations.[24]
Prognosis and disposition
A meaningful fraction of TRS patients respond to clozapine; partial responders still gain function and suicide-risk reduction for some. Continuation needs indefinite monitoring discipline. Shared care with GPs works when roles, blood schedules, and red-flag pathways are written down. Super-refractory illness belongs in tertiary clozapine clinics, not endless unsupported community polypharmacy.[3][4][7][24]
Evidence, guidelines and regional differences
| Source | Exam take-home |
|---|---|
| Kane 1988 | Clozapine superior in TRS vs chlorpromazine |
| TRRIP 2017 | Operational TRS; two adequate trials |
| Siskind 2016/2017 | Efficacy vs other APs; response-rate magnitude |
| InterSePT 2003 | Suicidal behaviour reduction vs olanzapine |
| Leucht NMA 2013 | Highest efficacy rank among antipsychotics |
| FIN11 2009 | Treated illness mortality context |
| Ronaldson/Kilian | Myocarditis recognition and risk amplifiers |
| Palmer/Every-Palmer | CIGH is lethal and preventable |
| de Leon 2022 | Safer personalised titration |
| Northwood 2023 | Level optimisation with modern IPD methods |
| Landmark synthesis for viva speed.[1][2][3][4][5][6][7][10][11][13][14][19][20] |
ANZ: product-linked patient monitoring systems and cardiometabolic standards in psychosis care; myocarditis awareness is high after Australian case series. UK: NICE-aligned TRS pathway with clozapine after non-response; CPMS-style monitoring. US: FDA REMS framework for clozapine; APA TRS recommendations. Europe: AGNP TDM culture stronger in some centres. Exact ANC thresholds and dispensing rules are local law and product rules — principles travel; numbers may not.[2][11][23][24]
Exam pearls
CLOZAPINE non-negotiables
CLOZAPINE
References
- [1]Kane J, Honigfeld G, Singer J, et al. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry, 1988.PMID 3046553
- [2]Howes OD, McCutcheon R, Agid O, et al. Treatment-Resistant Schizophrenia: Treatment Response and Resistance in Psychosis (TRRIP) Working Group Consensus Guidelines on Diagnosis and Terminology Am J Psychiatry, 2017.PMID 27919182
- [3]Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT) Arch Gen Psychiatry, 2003.PMID 12511175
- [4]Siskind D, Siskind V, Kisely S Clozapine Response Rates among People with Treatment-Resistant Schizophrenia: Data from a Systematic Review and Meta-Analysis Can J Psychiatry, 2017.PMID 28655284
- [5]Siskind D, McCartney L, Goldschlager R, et al. Clozapine v. first- and second-generation antipsychotics in treatment-refractory schizophrenia: systematic review and meta-analysis Br J Psychiatry, 2016.PMID 27388573
- [6]Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis Lancet, 2013.PMID 23810019
- [7]Tiihonen J, Lönnqvist J, Wahlbeck K, et al. 11-year follow-up of mortality in patients with schizophrenia: a population-based cohort study (FIN11 study) Lancet, 2009.PMID 19595447
- [8]Alvir JM, Lieberman JA, Safferman AZ, et al. Clozapine-induced agranulocytosis. Incidence and risk factors in the United States. N Engl J Med, 1993.PMID 8515788
- [9]Pacia SV, Devinsky O Clozapine-related seizures: experience with 5,629 patients. Neurology, 1994.PMID 7991106
- [10]Kilian JG, Kerr K, Lawrence C, et al. Myocarditis and cardiomyopathy associated with clozapine. Lancet, 1999.PMID 10584719
- [11]Ronaldson KJ, Taylor AJ, Fitzgerald PB, et al. Diagnostic characteristics of clozapine-induced myocarditis identified by an analysis of 38 cases and 47 controls. J Clin Psychiatry, 2010.PMID 20361910
- [12]Ronaldson KJ, Fitzgerald PB, Taylor AJ, et al. Rapid clozapine dose titration and concomitant sodium valproate increase the risk of myocarditis with clozapine: a case-control study. Schizophr Res, 2012.PMID 23010488
- [13]Palmer SE, McLean RM, Ellis PM, et al. Life-threatening clozapine-induced gastrointestinal hypomotility: an analysis of 102 cases. J Clin Psychiatry, 2008.PMID 18452342
- [14]Every-Palmer S, Ellis PM Clozapine-Induced Gastrointestinal Hypomotility: A 22-Year Bi-National Pharmacovigilance Study of Serious or Fatal 'Slow Gut' Reactions, and Comparison with International Drug Safety Advice. CNS Drugs, 2017.PMID 28623627
- [15]Handley SA, Every-Palmer S, Ismail A, et al. Clozapine-induced gastrointestinal hypomotility: presenting features and outcomes, UK pharmacovigilance reports, 1992-2017. Br J Psychiatry, 2022.PMID 35164895
- [16]Rostami-Hodjegan A, Amin AM, Spencer EP, et al. Influence of dose, cigarette smoking, age, sex, and metabolic activity on plasma clozapine concentrations: a predictive model and nomograms to aid clozapine dose adjustment and to assess compliance in individual patients. J Clin Psychopharmacol, 2004.PMID 14709950
- [17]Haslemo T, Eikeseth PH, Tanum L, et al. The effect of variable cigarette consumption on the interaction with clozapine and olanzapine. Eur J Clin Pharmacol, 2006.PMID 17089108
- [18]Perry PJ, Miller DD, Arndt SV, et al. Clozapine and norclozapine plasma concentrations and clinical response of treatment-refractory schizophrenic patients. Am J Psychiatry, 1991.PMID 1670979
- [19]Northwood K, Pearson E, Arnautovska U, et al. Optimising plasma clozapine levels to improve treatment response: an individual patient data meta-analysis and receiver operating characteristic curve analysis. Br J Psychiatry, 2023.PMID 36994656
- [20]de Leon J, Schoretsanitis G, Smith RL, et al. An International Adult Guideline for Making Clozapine Titration Safer by Using Six Ancestry-Based Personalized Dosing Titrations, CRP, and Clozapine Levels. Pharmacopsychiatry, 2022.PMID 34911124
- [21]Manu P, Lapitskaya Y, Shaikh A, et al. Clozapine Rechallenge After Major Adverse Effects: Clinical Guidelines Based on 259 Cases. Am J Ther, 2018.PMID 29505490
- [22]Cohen D, Bogers JP, van Dijk D, et al. Beyond white blood cell monitoring: screening in the initial phase of clozapine therapy. J Clin Psychiatry, 2012.PMID 23140648
- [23]Hiemke C, Bergemann N, Clement HW, et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017. Pharmacopsychiatry, 2018.PMID 29390205
- [24]Flanagan RJ, Lally J, Gee S, et al. Clozapine in the treatment of refractory schizophrenia: a practical guide for healthcare professionals. Br Med Bull, 2020.PMID 32885238