Psych · Psychopharmacology — cognitive enhancers
Cognitive enhancers (cholinesterase inhibitors and memantine)
Also known as Cholinesterase inhibitors · AChEI · Donepezil · Rivastigmine · Galantamine · Memantine · Anti-dementia drugs · Cognitive enhancers dementia
Exam-exhaustive fellowship monograph on cholinesterase inhibitors and memantine — mechanisms, severity- and subtype-linked indications (AD, DLB, PDD, MCI caveats), adult oral and patch doses with titration and monitoring, DOMINO-AD continuation, combination therapy, AD2000 appraisal, cardiac/GI safety, deprescribing, and BAP/APA/NICE-style regional framing. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Definition and class map
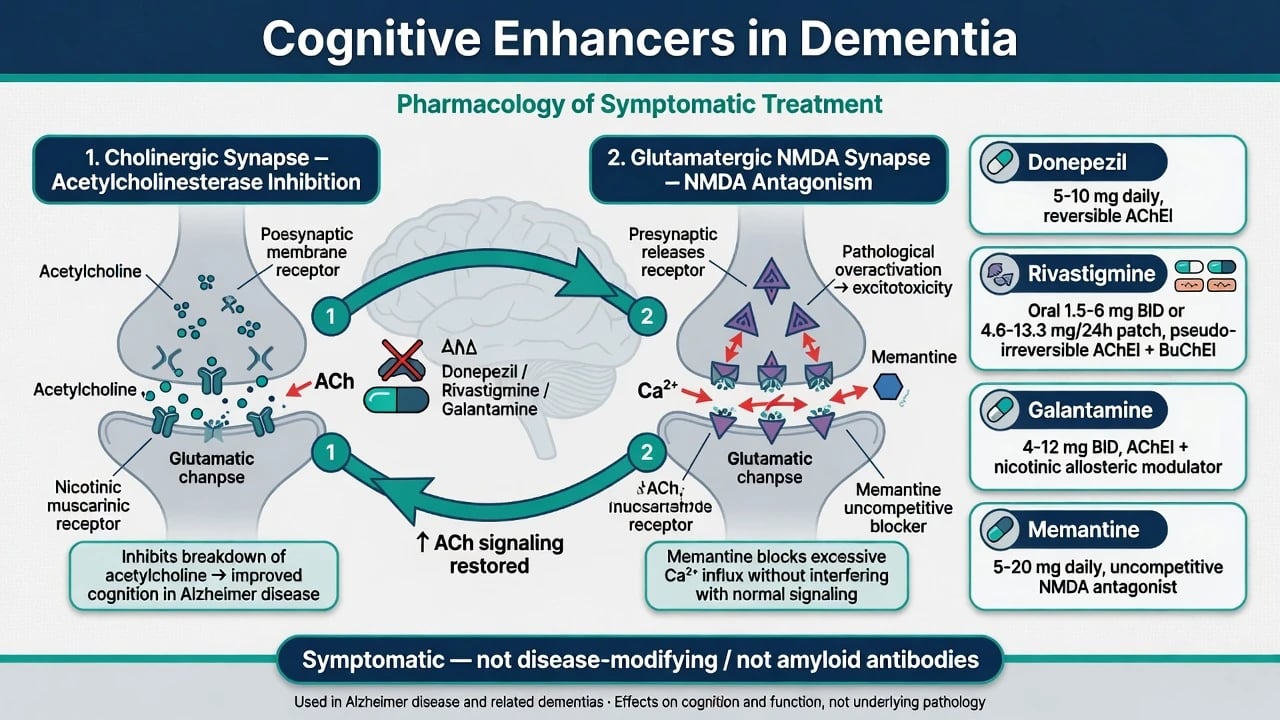
Cognitive enhancers (anti-dementia drugs) in fellowship psychopharmacology means the licensed cholinesterase inhibitors (AChEIs) and memantine. They improve or slow decline in cognitive, global, and sometimes functional measures on average by modest effect sizes. They are not disease-modifying anti-amyloid monoclonals, not stimulants for healthy cognition, and not a substitute for diagnosis, carer support, or capacity-aware care planning.[13][17][18]
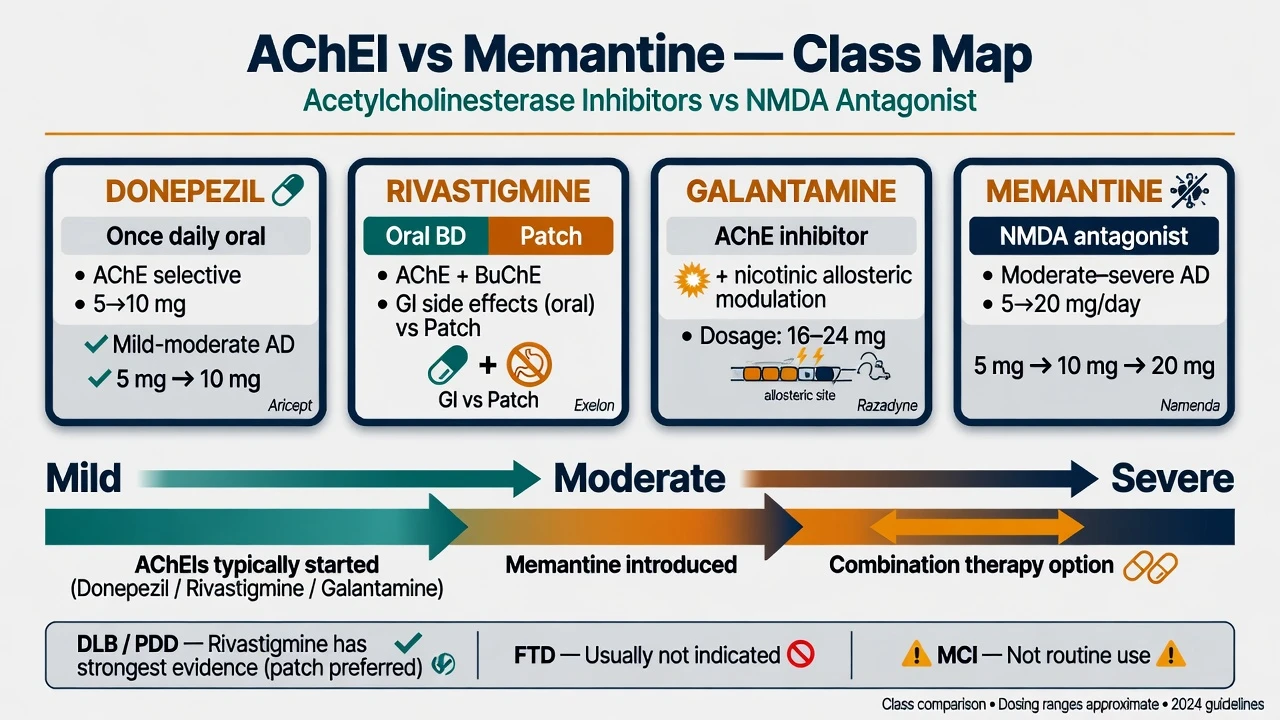
AChEIs: donepezil (selective AChE inhibition, once-daily oral), rivastigmine (AChE and butyrylcholinesterase; oral or transdermal patch), galantamine (AChE inhibition plus allosteric nicotinic receptor modulation teaching). Memantine: uncompetitive NMDA-receptor antagonist used primarily in moderate–severe AD, alone or added to an AChEI.[5][6][16]
Epidemiology and clinical context
These agents are among the most prescribed medicines in old-age psychiatry and memory clinics. Cochrane syntheses confirm small average benefits of donepezil and rivastigmine in AD dementia and of memantine in moderate–severe disease, with adverse events (especially GI for AChEIs) driving discontinuation.[13][14][15] Raina and colleagues summarised that benefits are measurable but clinically modest across the evidence base used for guideline development.[17] National reimbursement rules (for example PBS or NICE-style pathways) often shape real-world initiation and continuation as much as pure efficacy data.[18][19]
Pathophysiology — why these drugs exist
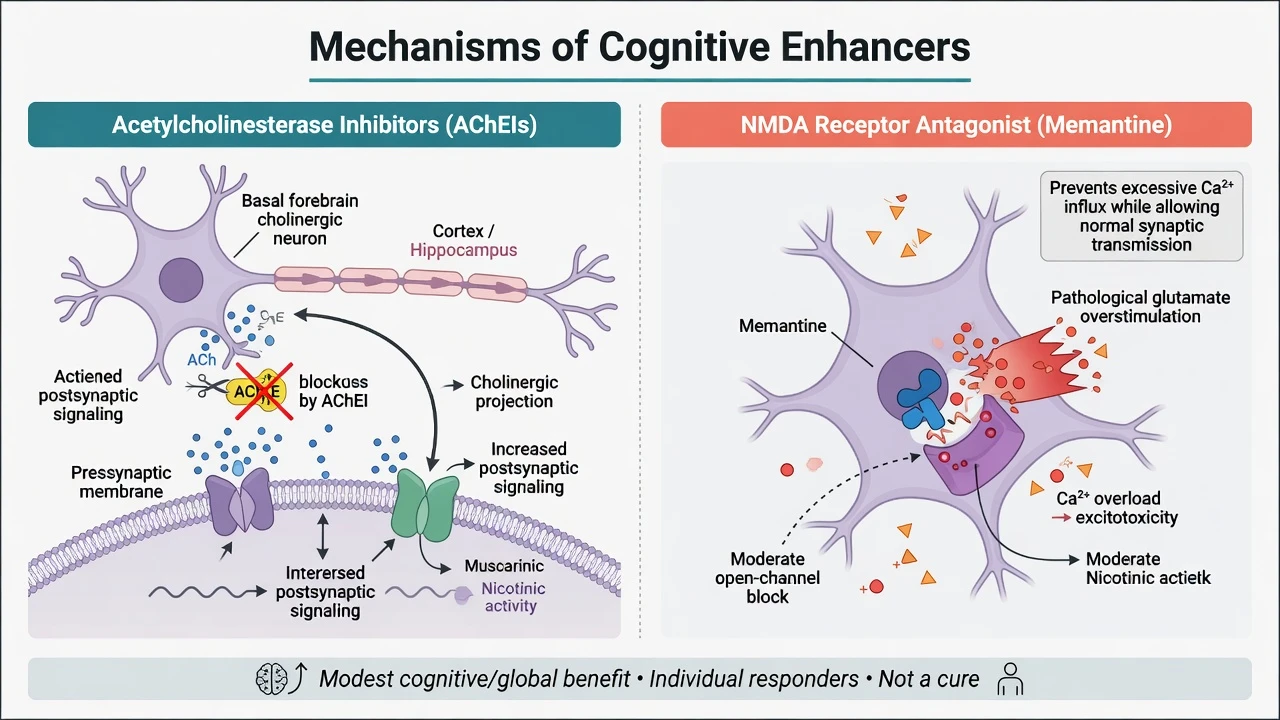
AD and related cortical dementias feature basal forebrain cholinergic degeneration. Raising synaptic acetylcholine by inhibiting acetylcholinesterase (and for rivastigmine also BuChE) underpins AChEI symptomatic benefit.[1][13] Pathological glutamatergic overactivation at NMDA receptors is the teaching rationale for memantine’s moderate open-channel block without abolishing normal synaptic transmission.[5][15] Lewy-body spectrum dementias are often relatively cholinergically depleted, which helps explain stronger clinical interest in rivastigmine for DLB and Parkinson disease dementia (PDD).[9][10]
Indications by subtype and severity
Alzheimer disease
Mild–moderate AD dementia: AChEI first-line pharmacological option after shared decision and baseline safety checks. Landmark RCTs established donepezil (Rogers; Feldman in moderate–severe strata), rivastigmine (Rösler), and galantamine (Tariot USA-10) efficacy on cognition and global measures versus placebo.[1][2][3][4]
Moderate–severe AD: Continue AChEI if tolerated and still serving goals (DOMINO-AD); memantine has standalone evidence (Reisberg) and add-on evidence to donepezil (Tariot).[5][6][7] Cochrane memantine review supports benefit mainly in moderate–severe dementia, with less clear benefit in mild disease.[15]
Dementia with Lewy bodies and Parkinson disease dementia
McKeith 2000: rivastigmine improved neuropsychiatric and cognitive outcomes versus placebo in DLB — a classic exam trial.[9] EXPRESS (Emre 2004): rivastigmine benefited cognition and global status in PDD versus placebo.[10] Donepezil and galantamine are also used clinically in Lewy-body spectrum disease depending on formulary and tolerability; rivastigmine carries the cleanest named-trial footprint for exams.[9][10][18]
Vascular cognitive impairment and FTD
Mixed AD–vascular pathology is common; pure vascular cognitive impairment has a weaker, more heterogeneous AChEI signal — individualise rather than auto-prescribe.[17][18] Behavioural-variant FTD is generally a poor AChEI target and not a routine indication — do not treat “dementia tablet” as pan-subtype.[18][19]
Mild cognitive impairment
Petersen 2005: donepezil delayed progression to AD at 12 months but not at 36 months, with more adverse events; vitamin E was ineffective.[11] Tricco meta-analysis: cognitive enhancers in MCI show limited efficacy signals with increased GI and other harms — not routine long-term disease-modifying therapy for pure MCI.[12]
Adult doses and titration (exam scaffolds)
Always confirm current product information and local formulary; start lower in frail older adults. Teaching scaffolds used in fellowship answers follow the major RCT dose programmes and product titration culture.[1][3][5][16]
| Agent | Typical adult start | Titration / target teaching | Key cautions |
|---|---|---|---|
| Donepezil oral | 5 mg once daily | Increase to 10 mg after at least 4 weeks if tolerated | Bradycardia, GI, vivid dreams (evening dose lore) |
| Rivastigmine oral | 1.5 mg twice daily | Stepwise every ≥2 weeks toward 3–6 mg twice daily as tolerated | High oral GI burden |
| Rivastigmine patch | 4.6 mg/24 h | To 9.5 mg/24 h then 13.3 mg/24 h if indicated | Application site reactions; lower peak GI vs oral (IDEAL) |
| Galantamine | Low start (product-dependent IR/ER) | Toward 16–24 mg/day total | Hepatic caution; GI |
| Memantine | 5 mg once daily | Weekly +5 mg to 10 mg twice daily (20 mg/day); ER 28 mg daily where available | Renal dose adjust; dizziness, confusion, headache |
| Teaching sources for these scaffolds: donepezil and rivastigmine RCTs, galantamine USA-10, memantine Reisberg/Tariot, and IDEAL patch programmes.[1][3][4][5][6][16] |
Donepezil RCT programmes used 5–10 mg ranges; rivastigmine oral and patch programmes define the titration culture still examined today; memantine titration to 20 mg/day underpins Reisberg/Tariot practice.[1][3][5][6][16]
IDEAL (Winblad): rivastigmine patch showed efficacy with a more favourable GI profile than high-dose capsules — use patch language when oral rivastigmine is not tolerated.[16]
Assessment, investigations, and monitoring
Before start: confirm dementia (not untreated delirium), approximate subtype and severity, goals of care, carer involvement, and capacity for consent.[18][19] Baseline pulse; ECG when bradycardia, conduction disease, syncope history, or interacting negative chronotropes are present. Weight and nutrition (GI loss risk). eGFR/creatinine before memantine. Review and deprescribe unnecessary anticholinergics that oppose AChEI benefit. Asthma/COPD, peptic ulcer disease, urinary obstruction, and seizure history inform risk counselling.[13][18]
After start: early contact for GI symptoms and falls/syncope; structured review at about 3 months then typically 6-monthly for cognition, function, behaviour, carer impression, adherence, and adverse effects. Same cognitive instrument over time aids interpretation; absolute score change is only one part of the global clinical decision.[18][19]
Landmark evidence every candidate must own
Cognitive enhancer trials that change viva answers
Donepezil RCTs. Rogers established 24-week efficacy in mild–moderate AD; Feldman extended benefit into moderate–severe AD strata.[1][2] Birks Cochrane supports small cognitive and global benefits across severities in trial windows.[13]
Rivastigmine and galantamine. Rösler international RCT and Birks rivastigmine Cochrane for AD; Tariot USA-10 for galantamine; IDEAL for patch delivery.[3][4][14][16]
Memantine. Reisberg: memantine versus placebo in moderate–severe AD. Tariot: memantine added to stable donepezil superior to donepezil plus placebo on key outcomes. McShane Cochrane: benefit concentrated in moderate–severe disease.[5][6][15]
DOMINO-AD (Howard 2012). In community-living patients with moderate–severe AD already on donepezil, continuing donepezil improved cognition and function versus stopping; memantine had smaller or mixed effects depending on outcome; combination was not clearly superior to continued donepezil alone on primary cognitive/functional pair in the way candidates sometimes overclaim. Exam pearl: do not automatically stop donepezil merely because the patient has become moderately to severely impaired if it is still tolerated and goals support continuation.[7]
AD2000 (Courtney 2004). UK pragmatic trial that found limited benefits of donepezil on progression to disability and institutionalisation and fuelled funding debates. Exam-safe appraisal: high attrition, controversial endpoints, and method debates mean it does not license a one-liner that “donepezil never works” against the broader RCT and Cochrane corpus.[8][13]
BPSD signal. Holmes and colleagues showed donepezil effects on neuropsychiatric symptoms in AD in a withdrawal design context — enhancers can help some behavioural domains but are not a substitute for non-drug BPSD care or for cautious antipsychotic decision-making when risk is high.[20]
Adverse effects and acute problems
AChEI class: nausea, vomiting, diarrhoea, anorexia, weight loss, abdominal pain; bradycardia, syncope, heart block risk; insomnia or vivid dreams (donepezil); muscle cramps; urinary incontinence exacerbation; rarely seizures. Management: take with food where advised, slow titration, dose reduce or switch agent/route (patch), hold for severe bradycardia/syncope pending ECG and medical review.[13][14][16]
Memantine: dizziness, headache, constipation, confusion, hypertension teaching points; accumulation in renal impairment — adjust or avoid per product rules.[15]
AChEI risks
- GI intolerance and weight loss
- Bradycardia / syncope / block
- Vivid dreams (donepezil lore)
- Opposing anticholinergic polypharmacy
Memantine risks
- Dizziness and confusion
- Renal dose adjustment
- Less GI than AChEI classically
- Main benefit mod–severe AD
When to stop
- Intolerable harm
- No meaningful benefit after trial
- Goals of care end-stage comfort
- Not auto-stop solely on severity
Subtype pearls
- DLB/PDD: rivastigmine trials
- MCI: not routine enhancer
- FTD: usually avoid AChEI
- Mixed vascular: individualise
Prescribing algorithm
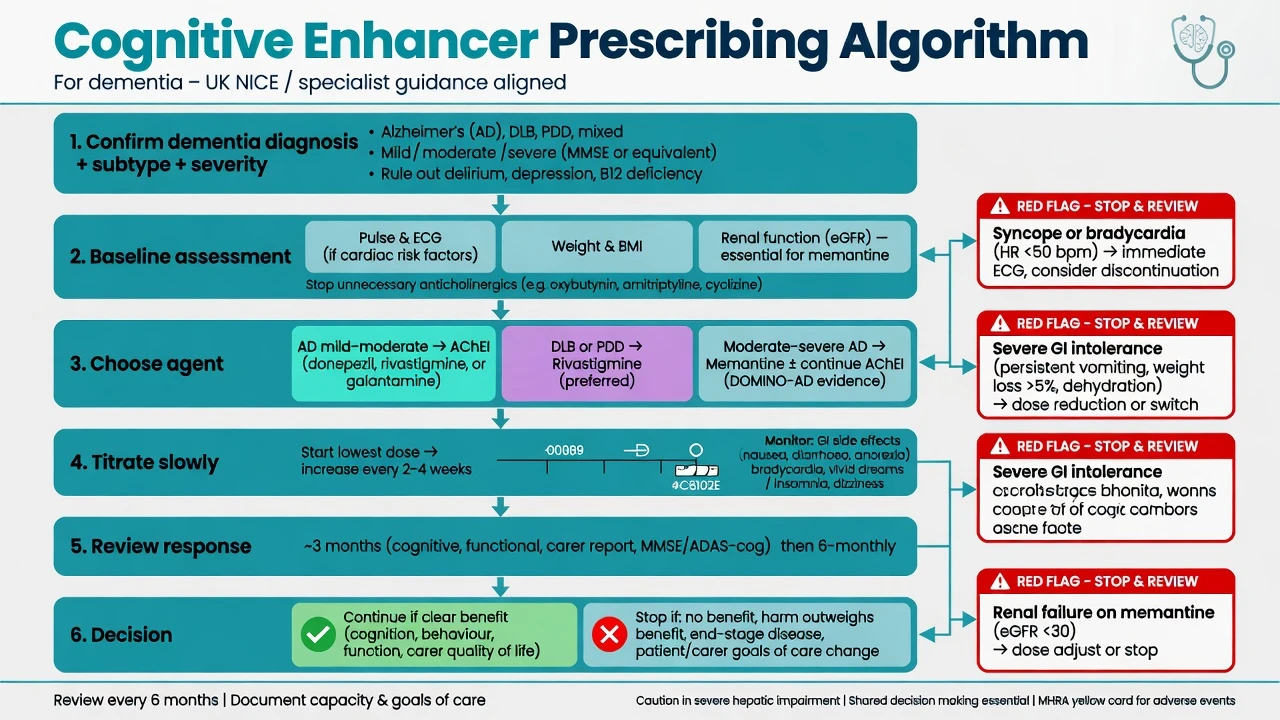
- Confirm major NCD/dementia diagnosis and likely subtype; treat delirium and reversible contributors first.[18][19]
- Baseline safety: pulse ± ECG, weight, renal function if memantine, drug review.[13][18]
- Choose: mild–moderate AD → AChEI; DLB/PDD → prefer rivastigmine evidence base; moderate–severe AD → memantine ± continued AChEI (DOMINO/Tariot logic).[7][9][10]
- Titrate slowly; educate carer on GI and cardiac red flags.
- Review response and tolerability; continue, switch, add memantine, or stop based on goals — not a single score threshold alone.[7][18]
Special populations
Frail older adults: start low, watch weight, falls, and bradycardia; simplify regimens (donepezil once daily or patch).[13][16] Renal impairment: memantine dose reduction is mandatory teaching. Hepatic impairment: galantamine and rivastigmine product constraints. Young-onset dementia and intellectual disability: specialist pathways; do not copy-paste late-life defaults. Pregnancy: rare; specialist advice.
Regional guideline deltas
ANZ. Memory-clinic and PBS-style authority frameworks often govern AChEI and memantine initiation and continuation criteria — state principles (confirmed AD or approved indication, baseline and review scores, specialist involvement) without inventing a single national number as eternal law. UK. NICE-aligned stepped pathways historically restricted AChEI to mild–moderate AD and memantine to moderate–severe or AChEI-intolerant moderate disease; BAP third consensus (O'Brien 2017) gives examinable anti-dementia drug practice statements including subtype nuances.[18] US. APA Alzheimer guideline supports cholinesterase inhibitors and memantine within comprehensive dementia care; FDA labels drive dose ceilings and warnings.[19] Exam constant: modest efficacy, monitoring, realistic counselling — formulary details vary by region.
Prognosis, deprescribing, and disposition
Average benefits are modest; some patients and carers report clear stabilisation of function or behaviour. Plan review intervals and document what “benefit” means for this person. Deprescribe when harm outweighs benefit, end-stage goals favour comfort only, or there was never a meaningful response after an adequate trial — but do not equate rising severity alone with mandatory AChEI cessation contrary to DOMINO-AD.[7][15][18] Link disposition to care planning, driving/safety, BPSD non-drug first-line care, and capacity law (see Alzheimer disease and BPSD topics).
Exam pearls
ENHANCE checklist before first script
ENHANCE
References
- [1]Rogers SL, Farlow MR, Doody RS, et al. A 24-week, double-blind, placebo-controlled trial of donepezil in patients with Alzheimer's disease Neurology, 1998.PMID 9443470
- [2]Feldman H, Gauthier S, Hecker J, et al. A 24-week, randomized, double-blind study of donepezil in moderate to severe Alzheimer's disease Neurology, 2001.PMID 11524468
- [3]Rösler M, Anand R, Cicin-Sain A, et al. Efficacy and safety of rivastigmine in patients with Alzheimer's disease: international randomised controlled trial BMJ, 1999.PMID 10066203
- [4]Tariot PN, Solomon PR, Morris JC, et al. A 5-month, randomized, placebo-controlled trial of galantamine in AD. The Galantamine USA-10 Study Group Neurology, 2000.PMID 10881251
- [5]Reisberg B, Doody R, Stöffler A, et al. Memantine in moderate-to-severe Alzheimer's disease N Engl J Med, 2003.PMID 12672860
- [6]Tariot PN, Farlow MR, Grossberg GT, et al. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: a randomized controlled trial JAMA, 2004.PMID 14734594
- [7]Howard R, McShane R, Lindesay J, et al. Donepezil and memantine for moderate-to-severe Alzheimer's disease N Engl J Med, 2012.PMID 22397651
- [8]Courtney C, Farrell D, Gray R, et al. Long-term donepezil treatment in 565 patients with Alzheimer's disease (AD2000): randomised double-blind trial Lancet, 2004.PMID 15220031
- [9]McKeith I, Del Ser T, Spano P, et al. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study Lancet, 2000.PMID 11145488
- [10]Emre M, Aarsland D, Albanese A, et al. Rivastigmine for dementia associated with Parkinson's disease N Engl J Med, 2004.PMID 15590953
- [11]Petersen RC, Thomas RG, Grundman M, et al. Vitamin E and donepezil for the treatment of mild cognitive impairment N Engl J Med, 2005.PMID 15829527
- [12]Tricco AC, Soobiah C, Berliner S, et al. Efficacy and safety of cognitive enhancers for patients with mild cognitive impairment: a systematic review and meta-analysis CMAJ, 2013.PMID 24043661
- [13]Birks JS, Harvey RJ Donepezil for dementia due to Alzheimer's disease Cochrane Database Syst Rev, 2018.PMID 29923184
- [14]Birks JS, Chong LY, Grimley Evans J Rivastigmine for Alzheimer's disease Cochrane Database Syst Rev, 2015.PMID 26393402
- [15]McShane R, Westby MJ, Roberts E, et al. Memantine for dementia Cochrane Database Syst Rev, 2019.PMID 30891742
- [16]Winblad B, Cummings J, Andreasen N, et al. IDEAL: a 6-month, double-blind, placebo-controlled study of the first skin patch for Alzheimer disease Neurology, 2007.PMID 17646619
- [17]Raina P, Santaguida P, Ismaila A, et al. Effectiveness of cholinesterase inhibitors and memantine for treating dementia: evidence review for a clinical practice guideline Ann Intern Med, 2008.PMID 18316756
- [18]O'Brien JT, Holmes C, Jones M, et al. Clinical practice with anti-dementia drugs: A revised (third) consensus statement from the British Association for Psychopharmacology J Psychopharmacol, 2017.PMID 28103749
- [19]APA Work Group on Alzheimer's Disease and other Dementias, Rabins PV, Blacker D, et al. American Psychiatric Association practice guideline for the treatment of patients with Alzheimer's disease and other dementias. Second edition Am J Psychiatry, 2007.PMID 18340692
- [20]Holmes C, Wilkinson D, Dean C, et al. The efficacy of donepezil in the treatment of neuropsychiatric symptoms in Alzheimer disease Neurology, 2004.PMID 15277611