Psych · Psychopharmacology — drug interactions and QTc
Drug interactions and QTc
Also known as QTc prolongation psychotropics · Drug-induced long QT · Torsades de pointes psychiatry · CYP interactions antipsychotics · Smoking clozapine CYP1A2 · Psychotropic polypharmacy interactions
Exam-exhaustive fellowship reference on psychotropic drug–drug interactions and QTc risk — PK vs PD framework, CYP1A2/2D6/3A4 maps, smoking–clozapine, fluvoxamine, QTc measurement and thresholds, TdP, high-risk agents, ECG monitoring, polypharmacy, and special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Psychiatrists own two quiet killers of viva candidates: missed CYP interactions that turn a stable dose into toxicity or relapse, and missed QTc risk stacking that ends in syncope or torsades de pointes (TdP). This topic is the cross-cutting safety spine for antipsychotics, antidepressants, mood stabilisers, methadone, and rapid tranquillisation — not a side note to pharmacology tables.[1][2][6][14]
Overview and definition
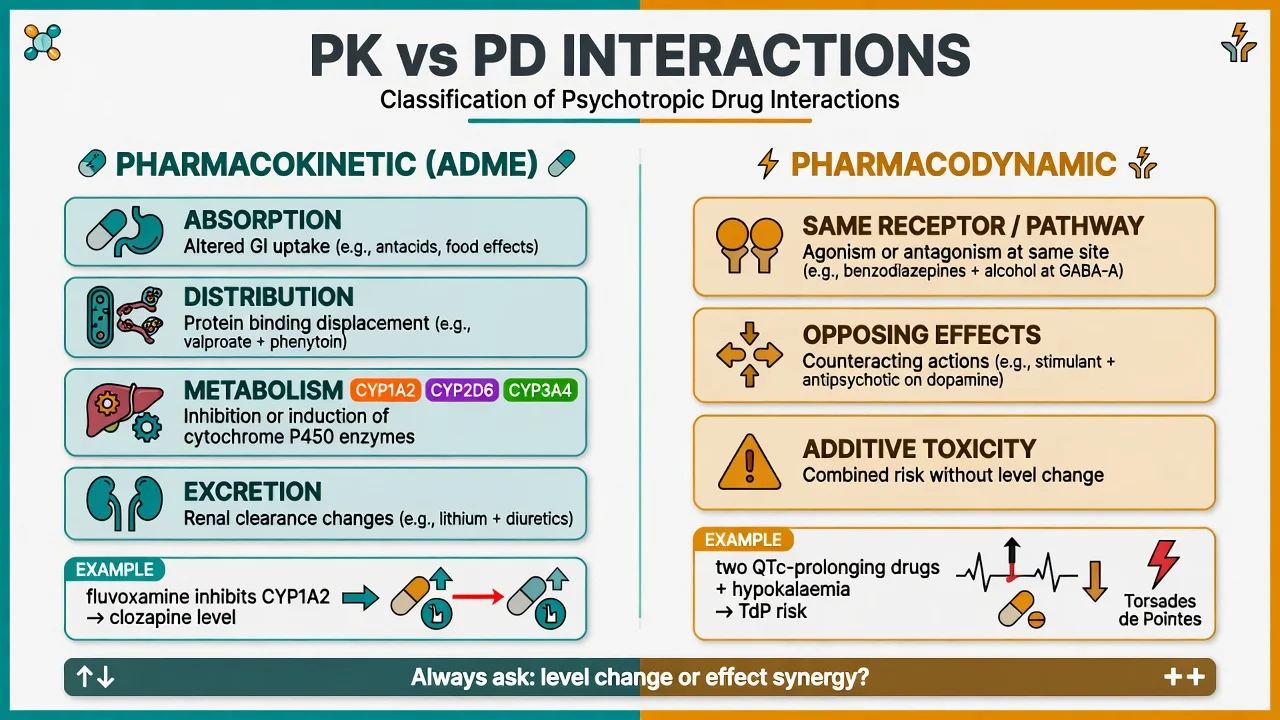
A drug–drug interaction is a clinically meaningful change in effect or safety when two or more substances are combined — including prescription drugs, OTC agents, herbals, and smoking. Pharmacokinetic (PK) interactions change exposure (absorption, distribution, metabolism, excretion). Pharmacodynamic (PD) interactions change effect at the same exposure (same pathway, opposing actions, or additive toxicity such as QTc prolongation).[13][14]
QTc is the heart-rate–corrected QT interval on the ECG, a bedside surrogate for ventricular repolarisation time. Prolongation increases the risk of early afterdepolarisations and polymorphic ventricular tachycardia of the TdP type. Drug-induced (acquired) long QT is far more common in psychiatric practice than congenital long QT syndrome, but the two share the same final common pathway of reduced repolarisation reserve.[4][19]
Classification — PK, PD, and QTc liability
Pharmacokinetic classes examiners expect
| Layer | Exam meaning | Psychiatry examples |
|---|---|---|
| Absorption | pH, chelation, gut motility | Antacids with some agents; less often the viva headline |
| Distribution | Protein binding displacement (rarely sole cause of disaster) | Mostly exam trivia unless free levels matter |
| Metabolism | CYP and UGT inhibition/induction | CYP1A2, 2D6, 3A4 dominate psychiatry stems |
| Excretion | Renal clearance of active drug/metabolites | Lithium is the classic renal interaction (see lithium topic) |
| Metabolic interactions with antipsychotics and antidepressants are the bread-and-butter of fellowship interaction questions.[13][14] |
Pharmacodynamic classes
- Same pathway / additive toxicity: two QTc-prolonging drugs; SSRI + MAOI → serotonin syndrome; multiple anticholinergics → delirium/constipation.
- Opposing effects: dopamine agonists undoing antipsychotics; stimulants vs sedatives in poorly planned polypharmacy.
- Disease–drug synergy: hypokalaemia + QT drug; bradycardia + QT drug; heart failure + QT drug.[4][6]
Relative QTc liability (teaching ladder, not a statute)
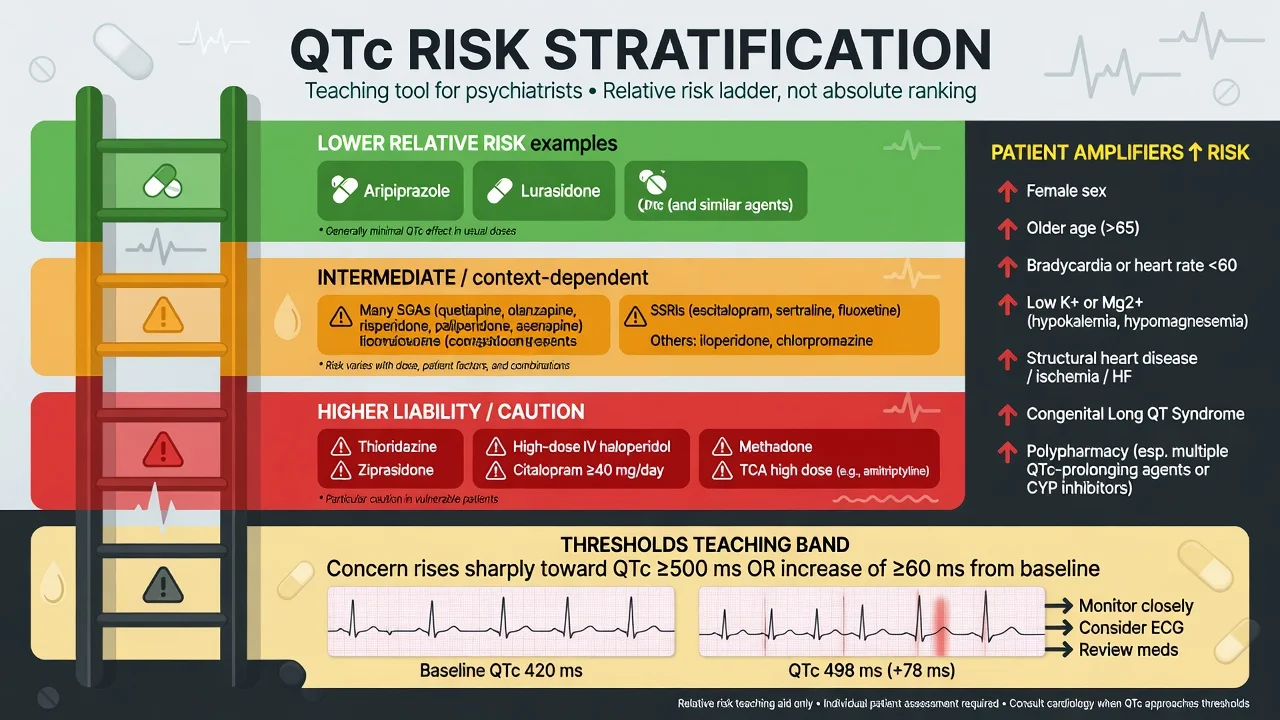
Classic teaching places thioridazine, high-dose IV haloperidol, and ziprasidone toward higher liability; many oral SGAs and SSRIs in a middle, context-dependent band; and agents such as aripiprazole toward lower mean QTc effect in comparative work. Individual patients still surprise you — reduced repolarisation reserve turns a "low-risk" drug dangerous.[1][5][6][10]
Epidemiology and risk
Sudden cardiac death signals associate with both typical and atypical antipsychotics. Ray and colleagues showed dose-related sudden cardiac death risk with atypical antipsychotics comparable in magnitude to typical agents in a large cohort — dismantling the myth that "atypicals are cardiac-safe by default."[2] Earlier work had already linked typical antipsychotics to elevated SCD risk.[1]
In psychiatric patients, QTc abnormalities cluster with specific agents and combinations (thioridazine, droperidol historical context, high-dose antipsychotics, TCAs) rather than diagnosis alone.[3] Inpatient ECG screening programmes (for example Girardin ESOP teaching) show that drug-induced long QT is detectable when you look systematically, especially under polypharmacy.[6][10]
Antidepressant signals are real but heterogeneous: EHR data link citalopram (and some other agents) to longer QTc than sertraline-class comparisons, aligning with SSRI ranking reviews and FDA-era citalopram dose caps that examiners still test.[8][9][10] Nationwide case-time-control work associates some antidepressants with out-of-hospital cardiac arrest risk gradients by agent class.[6]
Patient amplifiers (memorise): female sex, older age, bradycardia, hypokalaemia, hypomagnesaemia, structural heart disease/ischaemia, congenital LQTS or family sudden death, high drug concentrations (overdose, inhibition, poor metaboliser), and multiple concurrent QT drugs.[4][16][17]
Pathophysiology — from hERG to TdP
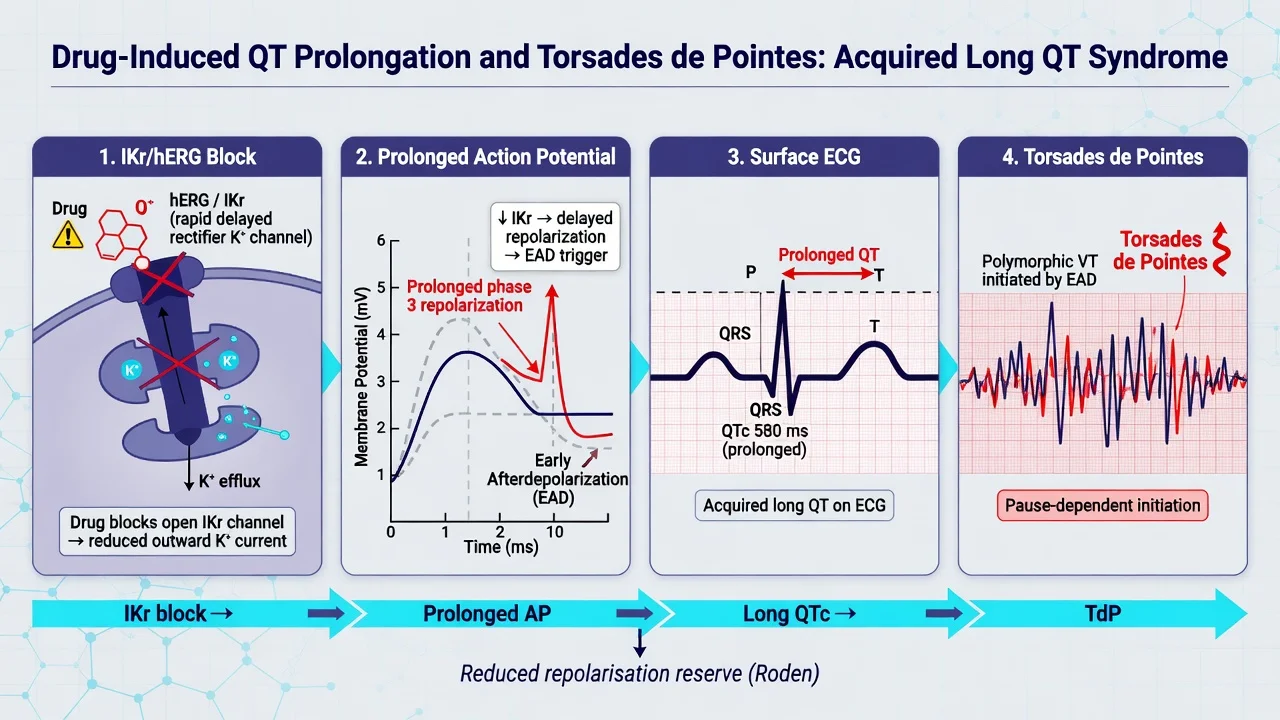
Most QT-prolonging drugs block the rapid delayed rectifier potassium current (IKr) mediated by the hERG channel, slowing phase-3 repolarisation. Prolonged action potentials favour early afterdepolarisations, which can trigger polymorphic VT with the twisting QRS morphology of TdP, which may self-terminate or degenerate to VF.[4][19]
Roden's reduced repolarisation reserve concept is the viva frame: a single modest hit rarely causes TdP; multiple hits (drug + low K+ + female sex + bradycardia + second QT drug) do.[4]
Rate correction matters. Raw QT lengthens as heart rate falls. Bazett (QTc = QT/√RR) is ubiquitous on machines but overcorrects at high rates and undercorrects at low rates; Fridericia (QT/RR⅓) is often preferred for serial monitoring teaching. Always inspect the tracing — automated values fail with wide QRS, U waves, paced rhythms, and artefact.[20][16]
PK interactions feed the same pathway by raising free drug at the channel without any change in the written dose — the reason a new inhibitor can convert a stable QTc into a dangerous one overnight.[13][5]
Clinical presentation
Most prolonged QTc is silent until monitoring or until syncope. Red presentations include palpitations, presyncope, syncope or seizure-mimic during polymorphic VT; cardiac arrest from TdP/VF; clozapine toxicity after smoking cessation or fluvoxamine start (sedation, hypersalivation, myoclonus/seizure, rising plasma level); loss of efficacy after enzyme induction (smoking restart; carbamazepine with 3A4 substrates); and methadone patients stacked with additional QT drugs — a dual-diagnosis exam favourite.[11][12][15][18][4][6]
Differential diagnosis
| Problem | Discriminators |
|---|---|
| Syncope on psychotropics | Arrhythmic (brief, no prodrome, injury) vs vasovagal vs orthostasis (alpha-1 block) vs seizure vs psychogenic |
| Polymorphic VT | Pause-dependent TdP after long–short sequence vs ischaemic VT vs artefact |
| Long QTc causes | Drugs vs electrolytes vs ischaemia vs intracranial event vs congenital LQTS vs measurement error |
| Rising clozapine level | Smoking stop, infection/inflammation (CYP1A2 downregulation teaching), fluvoxamine/ciprofloxacin, overdose, lab trough timing |
| Do not label every collapse "conversion" until ECG, electrolytes, and drug chart are clean.[4][6][11] |
Bedside assessment and medication reconciliation
Before starting or escalating a QTc-risk regimen, document cardiac history (syncope, familial sudden death, known LQTS, heart failure, ischaemia); full drug list including psychotropics, antiarrhythmics, macrolides, quinolones, azole antifungals, antiemetics (ondansetron), methadone, diuretics, St John's wort and grapefruit; smoking/vaping status (cigarettes induce CYP1A2 via polycyclic aromatic hydrocarbons; nicotine replacement does not fully recreate that induction); baseline vitals with attention to bradycardia; and ECG indications (high-liability agent, IV antipsychotics, methadone, QT polypharmacy, older adult, electrolyte risk, overdose, family history, prior prolonged QTc, or unexplained syncope).[15][11][6][7][22]
Investigations
Numbers every registrar must own
ECG: measure QT in a clear lead (often II or V5), correct for rate, document QRS width. Teaching bands used widely in hospital protocols: concern rises as QTc approaches 450 ms (men) / 460–470 ms (women); action threshold commonly taught at ≥500 ms or an increase of about 60 ms from baseline — local protocols vary; state them as bands, not universal law.[6][7][16][22]
Bloods: U&E with K+ and Mg2+, calcium, glucose; consider TSH. Aim potassium toward the higher normal range in QT risk states per cardiology prevention teaching.[16]
Tisdale QT risk score (hospitalised patients) combines age, sex, loop diuretics, K+, admission QTc, acute MI, sepsis, heart failure, and number of QT drugs — useful stratification language in liaison/inpatient settings.[17]
Therapeutic drug monitoring: clozapine (and selected other agents) levels guide interaction management when smoking status changes or inhibitors are added; AGNP consensus provides level interpretation principles.[21][11]
Management — resuscitation (TdP and critical QTc)
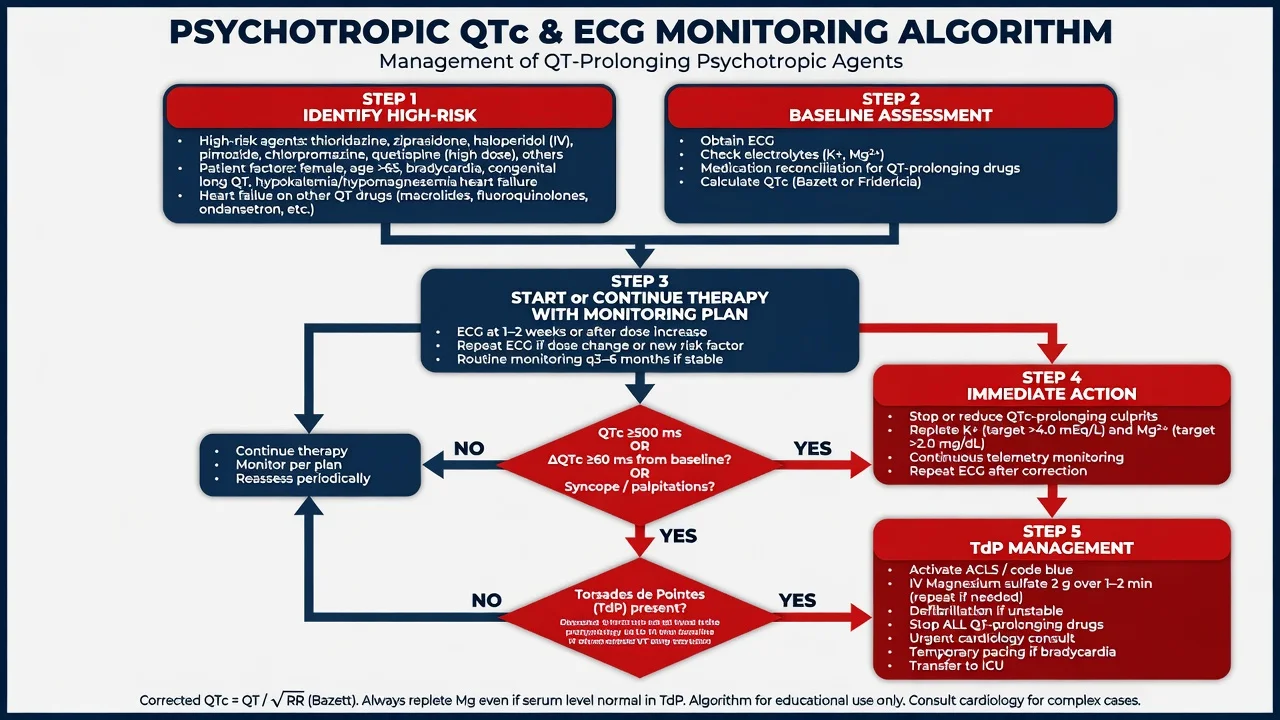
Unstable TdP / cardiac arrest: defibrillation and standard ACLS. Give IV magnesium sulfate as first-line anti-torsadogenic therapy even when the serum magnesium is within the reference range. Correct potassium aggressively toward high-normal. Stop all QT-prolonging agents. Temporary overdrive pacing or isoprenaline may be used in selected pause-dependent TdP under specialist care.[16][19][4]
Critical QTc without TdP: continuous monitoring, strip culprits, replete electrolytes, avoid further QT drugs and bradycardic insults, cardiology liaison. Do not treat empirically with class Ia/III agents that further prolong QT.[16][22]
Clozapine toxicity from interaction: hold or reduce dose, check trough level, seizure precautions, reverse the precipitant carefully (do not restart full smoking-era dose the day after cessation counselling fails).[11][12][21]
Management — definitive interaction practice
The four-question prescription check
Before signing, ask: is the new drug a substrate of a CYP that something else inhibits or induces; is it a strong inhibitor/inducer that will change a psychotropic already on board; is there PD overlap (QTc, serotonin, anticholinergic, CNS depression, bleeding with SSRI plus NSAID or anticoagulant); and what is the monitoring plan (ECG, electrolytes, plasma level, clinical toxicity check) with a named owner for follow-up?[13][14][6]
High-yield CYP map
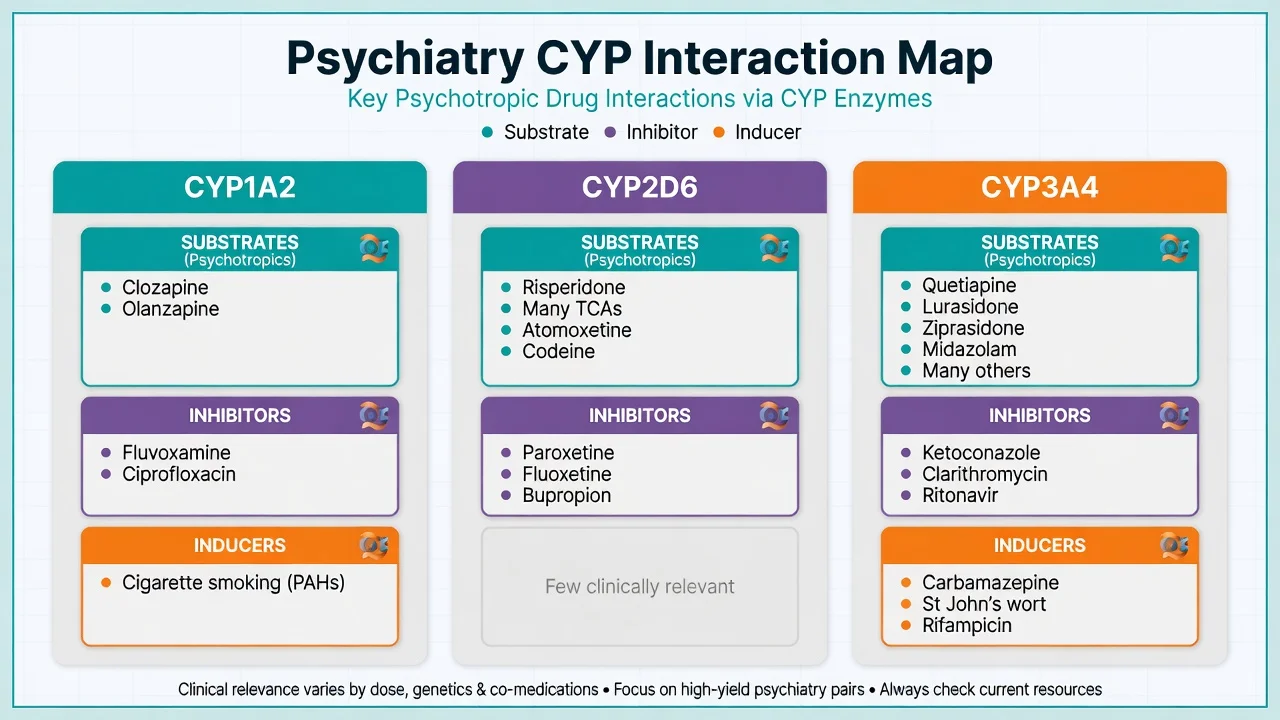
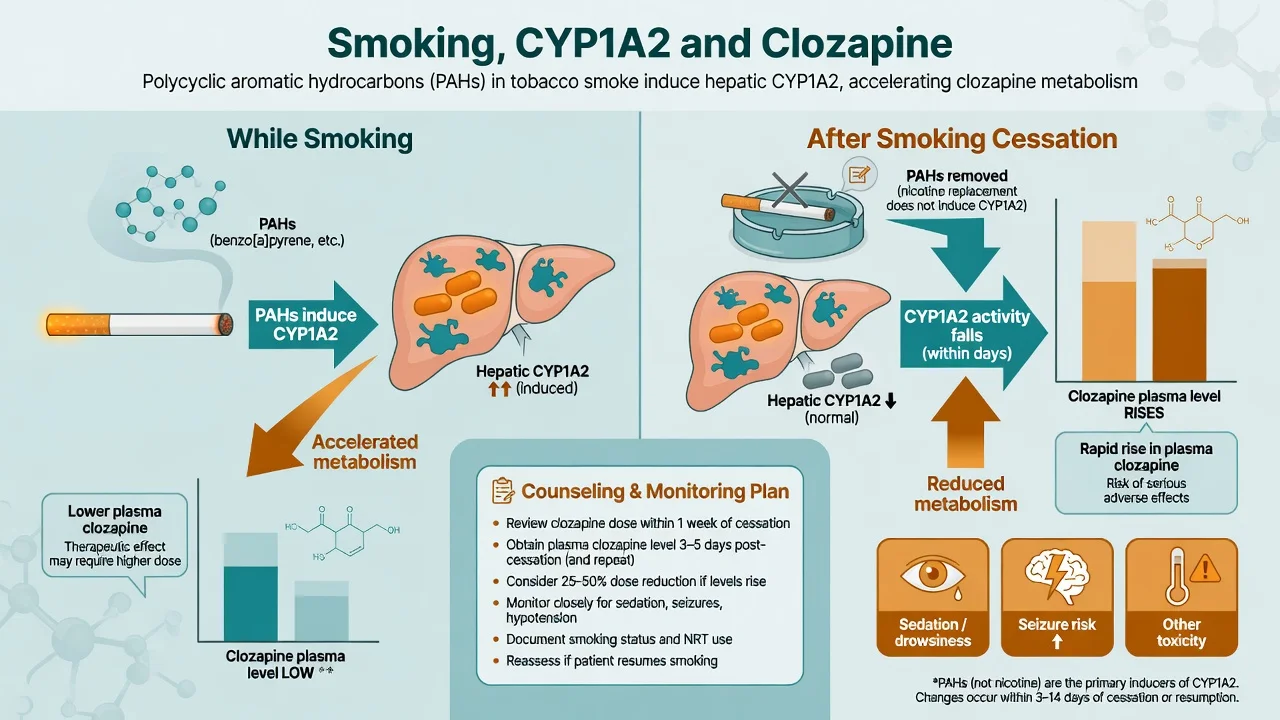
CYP1A2. Substrates: clozapine, olanzapine (and theophylline outside psychiatry). Inhibitors: fluvoxamine (potent), ciprofloxacin. Inducers: cigarette smoking (PAHs). Smoking cessation can substantially raise clozapine levels; models and clinical nomograms support dose individualisation with levels.[11][12][15][13]
CYP2D6. Substrates: risperidone, many TCAs, atomoxetine, codeine/tramadol activation pathways. Strong inhibitors: paroxetine, fluoxetine, bupropion. Poor metaboliser genetics amplify inhibitor effects — viva depth without ordering a genotype for every patient.[13][14]
CYP3A4. Substrates: quetiapine, lurasidone, ziprasidone, many benzodiazepines, carbamazepine (also inducer). Strong inhibitors: ketoconazole, clarithromycin, ritonavir-boosted regimens. Inducers: carbamazepine, rifampicin, St John's wort. Grapefruit can inhibit intestinal 3A4.[13][14]
High-risk combination matrix
Classic PK bombs
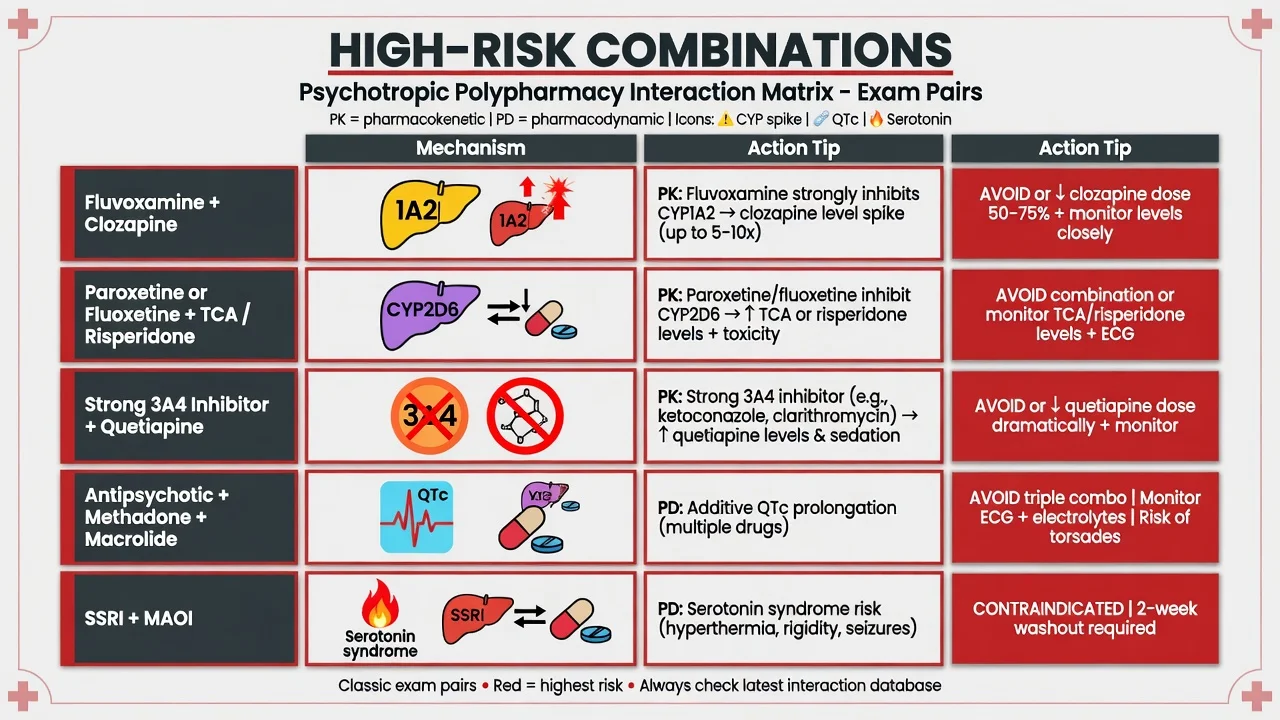
- Fluvoxamine + clozapine → level spike
- Smoking stop on clozapine → toxicity
- Strong 2D6 inhibitor + TCA/risperidone
- Strong 3A4 inhibitor + quetiapine/lurasidone
Classic PD bombs
- Two+ QT drugs + low K/Mg
- SSRI/SNRI + MAOI → serotonin syndrome
- Multiple anticholinergics
- CNS depressant stack (BZD + opioid + sedating AP)
Safer habits
- Reconcile meds every admission
- One change at a time
- ECG when risk stacks
- Deprescribe orphan psychotropics
Methadone interface
- Baseline and follow-up ECG principles
- Avoid extra QT drugs if possible
- Dose and interaction vigilance
- Coordinate with OAT service
QTc-specific prescribing rules
- Prefer lower-liability agents when cardiac risk is high and efficacy allows (shared decision; do not sacrifice necessary clozapine for a theoretical QTc fear without measurement).[6][7][10]
- Respect citalopram/escitalopram dose maxima in product information; avoid casual combination with other QT drugs; ECG if risk factors or higher doses historically used.[8][9][10]
- IV/high-dose haloperidol and multi-drug rapid tranquillisation: ECG as soon as practicable, lowest effective dose, electrolyte attention.[1][5][22]
- Methadone: follow ECG screening consensus principles (baseline, follow-up when dose high or risk factors, extra caution with other QT drugs).[18]
- After any new strong inhibitor or smoking cessation on a narrow-index substrate: early clinical review ± level ± ECG.[11][21]
Product information dose caps (citalopram/escitalopram), local formulary interaction checkers, and pharmacy alerts differ by region, but the exam constants are identical: CYP maps, reduced repolarisation reserve, QTc action bands, magnesium for TdP, and smoking–clozapine. RANZCP-aligned physical health monitoring, NICE physical health standards, and APA QTc resource documents all push structured risk assessment rather than panic or neglect.[7][22]
Specific scenarios
1. Clozapine smoker stops overnight in hospital. Expect rising levels over days; pre-emptive dose reduction plan, symptom watch, trough level, counsel that NRT ≠ full CYP1A2 induction replacement.[11][15]
2. GP starts fluvoxamine for OCD on stable clozapine. Potent 1A2 inhibition can multiply clozapine exposure — avoid or use only with specialist level-guided micro-adjustment; many services treat as relative contraindication without intensive TDM.[12][13]
3. Older woman on citalopram + thiazide + clarithromycin for pneumonia. Female sex + diuretic electrolyte risk + macrolide QT effect + SSRI — stop or switch one or more, replete K/Mg, ECG.[8][16][17]
4. Methadone OAT + new antipsychotic. Choose lower QTc liability if possible; ECG per Krantz-style principles; avoid further QT drugs.[18][6]
5. Congenital LQTS needing antipsychotic. Cardiology co-management; minimise QT drugs and bradycardia; correct electrolytes meticulously; document shared risk.[4][16]
6. TCA or citalopram overdose. Wide QRS/QTc, sodium bicarbonate algorithms for TCA (see toxicology pathways), continuous monitoring, psychiatry after medical clearance.[10][19]
Complications and pitfalls
- Trusting automated QTc only when U waves or wide QRS distort the interval.[20]
- Stacking three "borderline" QT drugs because each alone "looked fine."
- Treating TdP with amiodarone/sotalol without recognising QT mechanism.[16]
- Assuming nicotine patches preserve smoking-level CYP1A2 induction.[15]
- Ignoring non-psychotropic culprits on the drug chart (macrolide, quinolone, antifungal, antiemetic).
- Endless polypharmacy after unexplained syncope without ECG review.
Prognosis and disposition
Most drug-induced QTc prolongation improves after withdrawal and electrolyte repair. TdP that reaches hospital has substantial mortality if unrecognised. Admit/telemetry when QTc is critically prolonged, TdP occurred, overdose is recent, or electrolytes cannot be corrected safely as an outpatient. Document the culprit list for GP and pharmacy; avoid silent rechallenge.[16][22]
Special populations
Women have longer baseline QTc and higher TdP susceptibility in acquired LQTS teaching.[4][16] Older adults accumulate polypharmacy, reduced clearance, and diuretic use — start low, reconcile often. Pregnancy needs risk–benefit for necessary psychotropics without casual QT stacking. Youth have less high-quality comparative QTc data for some agents — still apply the same amplifier logic. Hepatic impairment magnifies inhibitor interactions. Intellectual disability may present syncope equivalents as unexplained falls — get collateral and ECGs.
Evidence, guidelines and controversies
Controversies: exact ranking tables differ by study design and dose; absolute TdP incidence is low so number-needed-to-harm estimates are noisy; how aggressively to ECG every SSRI starter remains debated — risk-stratified ECG is the defensible fellowship answer, not universal daily ECGs or never-ECG nihilism.[6][7][22]
Exam pearls
QTc SAFE script
- CYP1A2 + smoking + clozapine is the highest-yield single interaction stem in FRANZCP psychopharmacology.[11][15]
- Fluvoxamine is a potent CYP1A2 inhibitor — classic clozapine level explosion.[12]
- Magnesium first in TdP even if Mg is "normal."[16]
- Bazett lies at extremes of heart rate — know Fridericia exists.[20]
- Thioridazine / IV haloperidol / ziprasidone / high-dose citalopram / methadone / TCAs — know why each is on the caution list.[1][5][10][18]
- Polypharmacy QTc risk is multiplicative with patient factors, not a simple drug count.[4]
References
- [1]Glassman AH, Bigger JT Jr Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death Am J Psychiatry, 2001.PMID 11691681
- [2]Ray WA, Chung CP, Murray KT, et al. Atypical antipsychotic drugs and the risk of sudden cardiac death N Engl J Med, 2009.PMID 19144938
- [3]Reilly JG, Ayis SA, Ferrier IN, et al. QTc-interval abnormalities and psychotropic drug therapy in psychiatric patients Lancet, 2000.PMID 10744090
- [4]Roden DM Drug-induced prolongation of the QT interval N Engl J Med, 2004.PMID 14999113
- [5]Harrigan EP, Miceli JJ, Anziano R, et al. A randomized evaluation of the effects of six antipsychotic agents on QTc, in the absence and presence of metabolic inhibition J Clin Psychopharmacol, 2004.PMID 14709949
- [6]Beach SR, Celano CM, Noseworthy PA, et al. QTc prolongation, torsades de pointes, and psychotropic medications Psychosomatics, 2013.PMID 23295003
- [7]Funk MC, Beach SR, Bostwick JR, et al. QTc Prolongation and Psychotropic Medications Am J Psychiatry, 2020.PMID 32114782
- [8]Castro VM, Clements CC, Murphy SN, et al. QT interval and antidepressant use: a cross sectional study of electronic health records BMJ, 2013.PMID 23360890
- [9]Funk KA, Bostwick JR A comparison of the risk of QT prolongation among SSRIs Ann Pharmacother, 2013.PMID 24259697
- [10]Hasnain M, Vieweg WV QTc interval prolongation and torsade de pointes associated with second-generation antipsychotics and antidepressants: a comprehensive review CNS Drugs, 2014.PMID 25168784
- [11]Rostami-Hodjegan A, Amin AM, Spencer EP, et al. Influence of dose, cigarette smoking, age, sex, and metabolic activity on plasma clozapine concentrations: a predictive model and nomograms to aid clozapine dose adjustment and to assess compliance in individual patients J Clin Psychopharmacol, 2004.PMID 14709950
- [12]Hiemke C, Weigmann H, Härtter S, et al. Elevated levels of clozapine in serum after addition of fluvoxamine J Clin Psychopharmacol, 1994.PMID 7962687
- [13]Spina E, de Leon J Metabolic drug interactions with newer antipsychotics: a comparative review Basic Clin Pharmacol Toxicol, 2007.PMID 17214606
- [14]Spina E, Trifirò G, Caraci F Clinically significant drug interactions with newer antidepressants CNS Drugs, 2012.PMID 22171584
- [15]Kroon LA Drug interactions with smoking Am J Health Syst Pharm, 2007.PMID 17823102
- [16]Drew BJ, Ackerman MJ, Funk M, et al. Prevention of torsade de pointes in hospital settings: a scientific statement from the American Heart Association and the American College of Cardiology Foundation Circulation, 2010.PMID 20142454
- [17]Tisdale JE, Jaynes HA, Kingery JR, et al. Development and validation of a risk score to predict QT interval prolongation in hospitalized patients Crit Care Med, 2013.PMID 23716032
- [18]Krantz MJ, Martin J, Stimmel B, et al. QTc interval screening in methadone treatment Ann Intern Med, 2009.PMID 19153406
- [19]Yap YG, Camm AJ Drug induced QT prolongation and torsades de pointes Heart, 2003.PMID 14594906
- [20]Vandenberk B, Vandael E, Robyns T, et al. Which QT Correction Formulae to Use for QT Monitoring? J Am Heart Assoc, 2016.PMID 27317349
- [21]Hiemke C, Bergemann N, Clement HW, et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017 Pharmacopsychiatry, 2018.PMID 29390205
- [22]Fanoe S, Kristensen D, Fink-Jensen A, et al. Risk of arrhythmia induced by psychotropic medications: a proposal for clinical management Eur Heart J, 2014.PMID 24644307