Psych · Psychopharmacology — ECT and neurostimulation
ECT and neurostimulation
Also known as Electroconvulsive therapy · ECT · rTMS · iTBS · theta burst stimulation · tDCS · vagus nerve stimulation · VNS · deep brain stimulation depression · neurostimulation psychiatry · continuation ECT · maintenance ECT
Exam-exhaustive fellowship reference on ECT and neurostimulation — indications (depression, mania, catatonia, clozapine-resistant schizophrenia), consent and capacity, electrode placement and stimulus dosing, anaesthesia essentials for psychiatrists, cognitive adverse effects, continuation and maintenance, plus evidence-tiered rTMS/iTBS, tDCS, VNS and DBS. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
12 MCQs with explanations
Target exams
Red flags
ECT remains the most effective acute somatic treatment for severe major depression and a life-saving intervention in catatonia and high-risk affective illness. Fellowship examiners test whether you can indicate it correctly, consent without stigma theatre, choose placement and dose deliberately, partner with anaesthesia safely, monitor cognition honestly, and prevent relapse after remission. Non-ECT neurostimulation (rTMS/iTBS, tDCS, VNS, DBS) sits on a separate evidence ladder — know where each belongs.[1][5][6][15][21]
Overview and definition
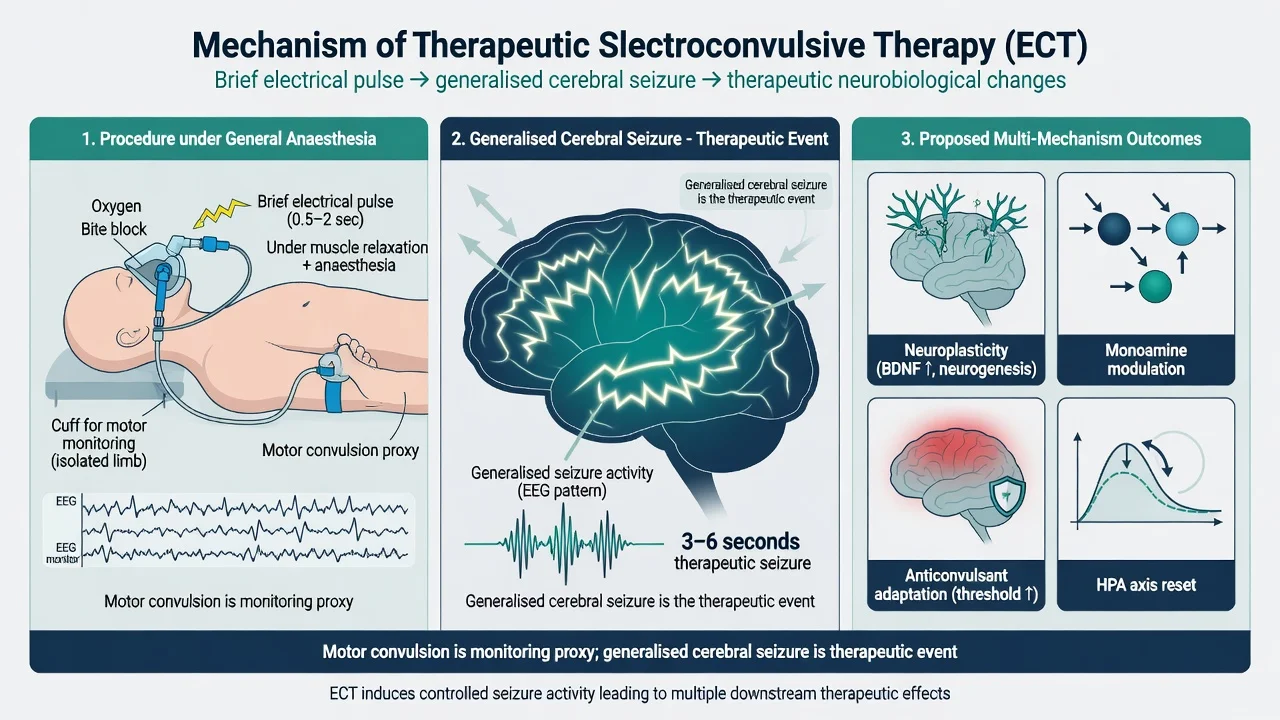
Electroconvulsive therapy (ECT) delivers a controlled electrical stimulus to the scalp under general anaesthesia and muscle relaxation to induce a generalised cerebral seizure. The motor convulsion is a monitoring proxy (classically with a limb cuff isolating a limb from the relaxant); the therapeutic event is the cerebral seizure itself.[5][6]
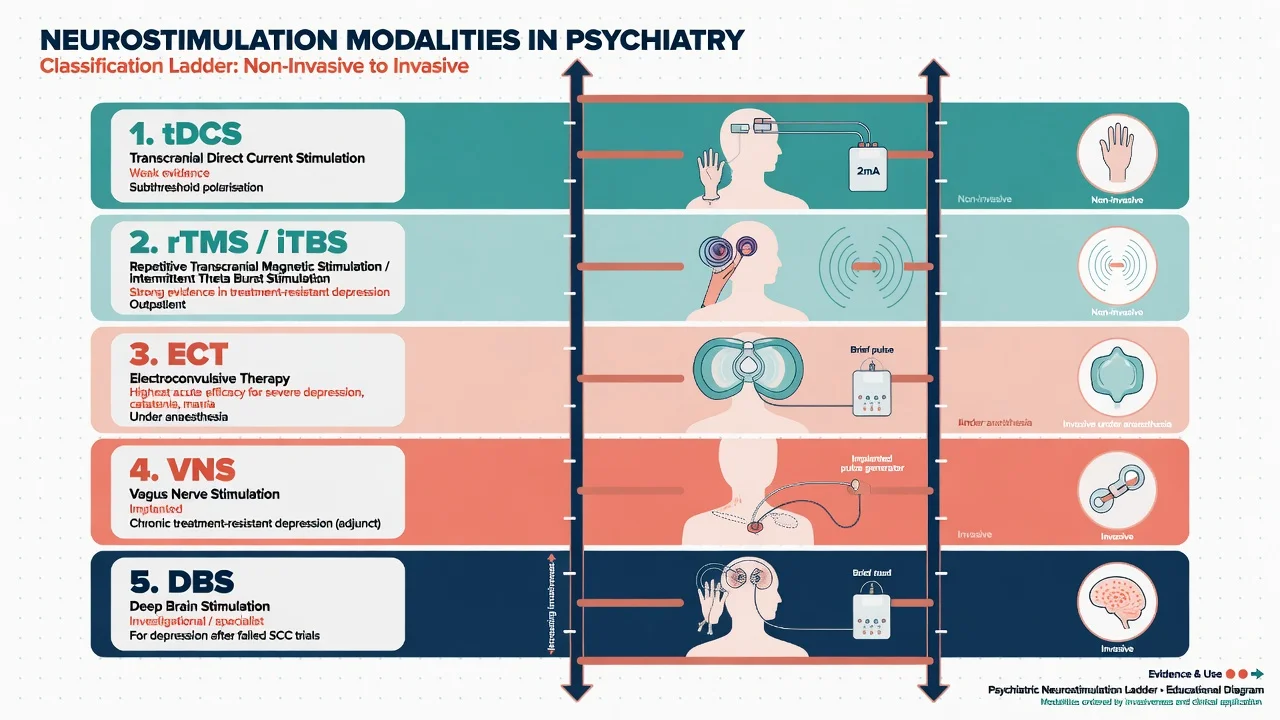
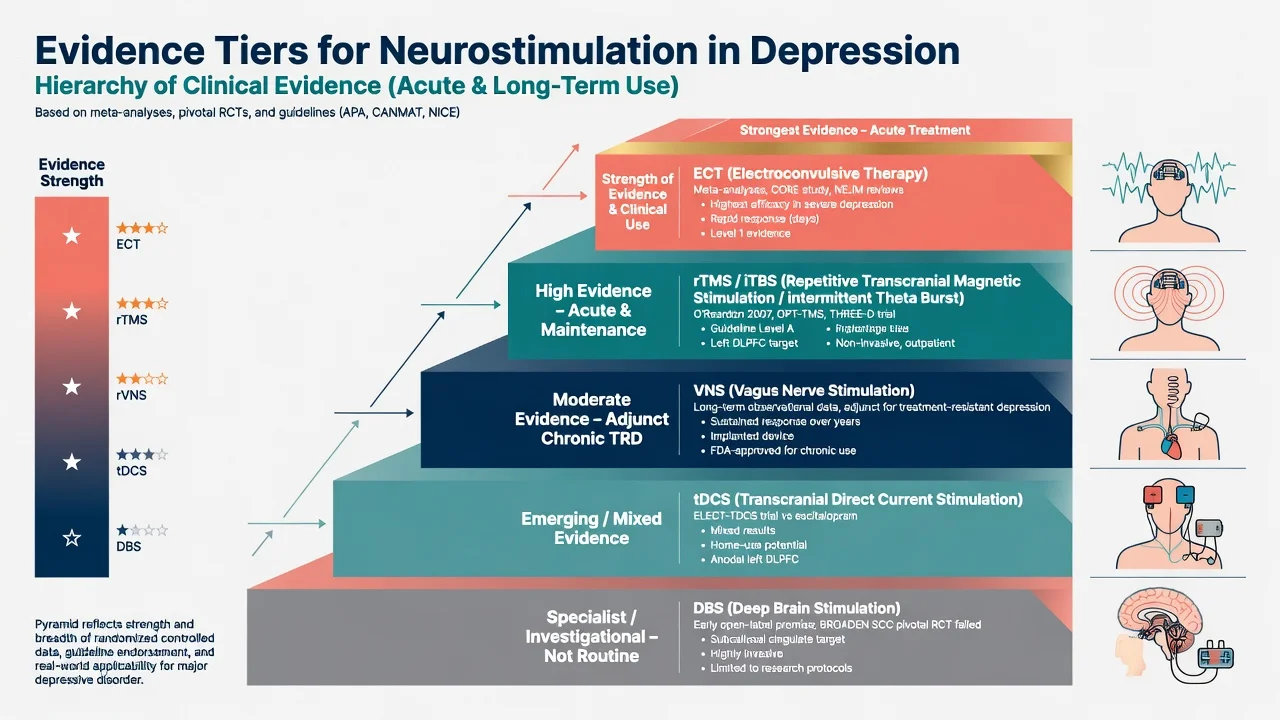
Neurostimulation in psychiatry is the broader family of device-based brain-modulating treatments. For exam purposes, order them by typical clinical use and evidence: ECT (highest acute efficacy for severe illness), rTMS/iTBS (outpatient TRD with solid sham-controlled data), tDCS (weaker/mixed), implanted VNS (chronic TRD adjunct), and DBS (highly specialised; pivotal SCC depression data failed).[16][17][20][21][25]
Classification of modalities and courses
| Construct | Exam meaning |
|---|---|
| Index ECT | Acute course aimed at remission of the current episode |
| Continuation ECT | Relapse prevention in the months after response (often taught as roughly the first 6 months) |
| Maintenance ECT | Longer-term prevention of new episodes after continuation |
| RUL / BT (BL) / BF | Right unilateral, bitemporal/bilateral, bifrontal electrode placements |
| Brief vs ultrabrief pulse | Pulse-width strategies that trade cognitive burden against dosing needs |
| Course labels are somewhat arbitrary but examiners still use them; the clinical point is active relapse prevention after successful acute treatment.[2][6][28] |
Epidemiology and clinical impact
The UK ECT Review Group meta-analysis established that real ECT is more effective than sham for depression, bilateral is moderately more effective than unilateral on average, and ECT is often more effective than pharmacotherapy in the short term for depressive disorders.[1]
CORE data show rapid response trajectories in major depression treated with ECT — clinically meaningful improvement can appear within the first week for many patients, a speed advantage examiners contrast with sequential oral antidepressants.[3]
Relapse without a plan is the hidden epidemic. CORE continuation work showed substantial relapse risk after index remission; both continuation ECT and robust pharmacotherapy (classic nortriptyline plus lithium pathway in that trial) outperform historical untreated trajectories. Leaving hospital after "six good ECTs" without continuation strategy is a systems error.[2][28]
Modern mortality with anaesthetic standards is low relative to the mortality of untreated severe depression, catatonia, and starvation — but cardiovascular, aspiration, and anaesthetic risks still drive pre-assessment.[5][6][15]
Numbers and anchors examiners reward
These anchors orient fellowship answers; individualise course length, placement and dose to the patient in front of you.[1][2][3][11][12][26]
Pathophysiology and mechanism
No single molecular pathway explains ECT. Viva-safe framing:
- Seizure necessity — a generalised cerebral seizure of adequate quality is required; very brief or aborted seizures may be ineffective.[5][6]
- Anticonvulsant adaptation — seizure threshold often rises over a course; this tracks treatment physiology and dosing decisions.[5][6]
- Neuroplastic and network effects — neurotrophic signalling, monoamine modulation, and HPA-axis recalibration are proposed contributors; do not overclaim one "ECT molecule".[5][6]
- Dose–placement interaction — efficacy is not "any shock will do". Unilateral treatments generally need substantially suprathreshold dosing for efficacy comparable to bilateral approaches delivered closer to threshold; ultrabrief pulse width reduces cognitive cost for many patients but may require more aggressive relative dosing or more sessions in some series.[7][9][10]
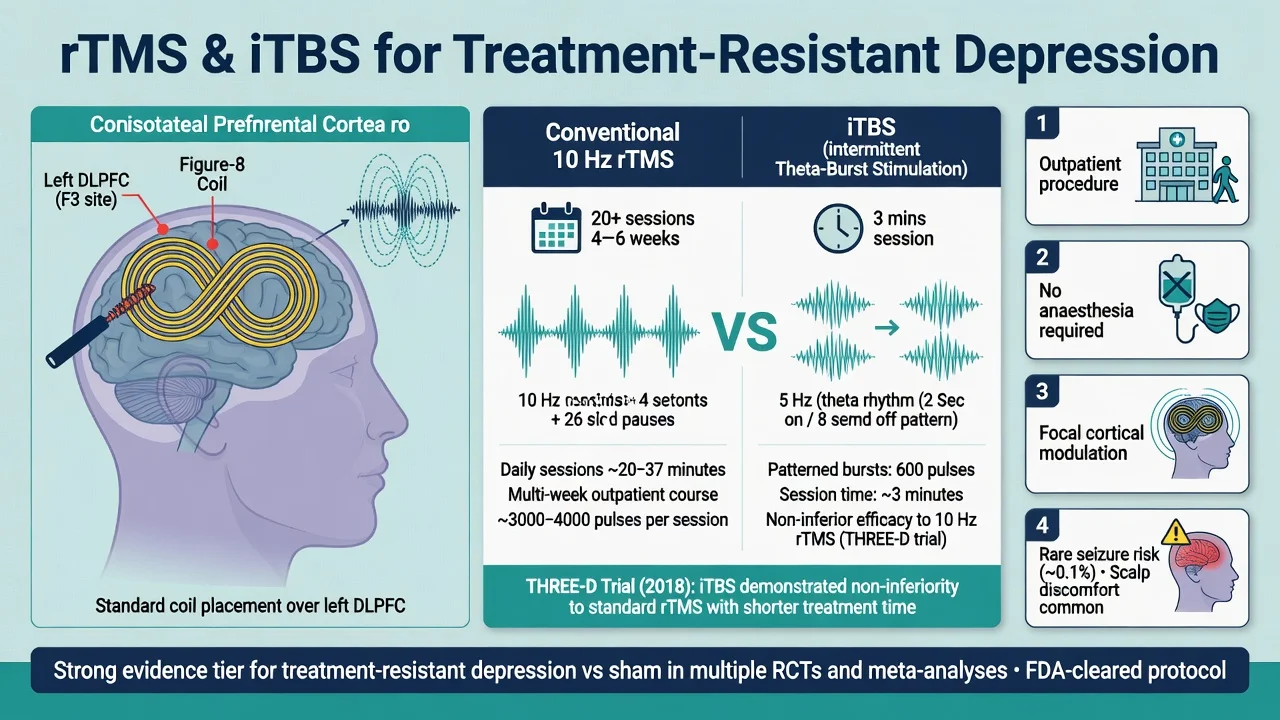
rTMS/iTBS modulates cortical excitability focally (classically left DLPFC for depression) without inducing a therapeutic seizure. tDCS applies weak direct current for subthreshold polarisation. VNS modulates afferent vagal pathways via an implanted generator. DBS stimulates deep circuit nodes (for example subcallosal cingulate in early depression work) with continuous or programmed stimulation.[16][17][20][22][24]
Clinical indications and presentation cues
Depression
Primary indication: severe major depression, especially with melancholic or psychotic features, high suicide risk, food or fluid refusal, or treatment resistance after adequate trials. Medication resistance reduces but does not abolish ECT response — Prudic showed attenuated yet still clinically meaningful response in more resistant patients.[1][4][5][6]
Mania and mixed states
ECT is effective in severe or treatment-refractory mania and mixed states, and when medical urgency or pregnancy contraindicates aggressive polypharmacy. Speed of affective response can be rapid; bipolar depression also responds, with historical CORE-related work noting trajectory differences versus unipolar illness.[6][27]
Catatonia
Catatonia (across mood, psychotic, and medical contexts) is a high-yield ECT indication. Use the Bush–Francis Catatonia Rating Scale (BFCRS) structure for examination and tracking. Benzodiazepines (often high-dose lorazepam) and ECT are complementary — malignant catatonia with autonomic instability is a medical emergency where ECT should not wait for weeks of failed oral trials.[6][14][15]
Schizophrenia and clozapine resistance
ECT has a role in schizophrenia, particularly with catatonic features or as augmentation in clozapine-resistant schizophrenia. Petrides and colleagues showed ECT augmentation superior to clozapine continuation alone in clozapine-resistant illness — this is the modern board answer when clozapine has been optimised and residual symptoms dominate.[12][13]
Differential diagnosis and decision boundaries
| Scenario | Prefer | Pitfall |
|---|---|---|
| Severe melancholic depression, not eating | ECT pathway + medical support | Another low-dose SSRI trial while BMI falls |
| Catatonic stupor | BFCRS, lorazepam challenge, ECT readiness | Labelling as "voluntary mutism" without exam |
| Fever, rigidity, autonomic instability on antipsychotics | NMS pathway (stop antipsychotics, cool, support) | Calling everything catatonia and giving more dopamine blockers |
| Outpatient TRD, mobile, no urgent risk | Consider rTMS/iTBS | Offering only ECT or only another SSRI |
| Chronic multi-year TRD after ECT/rTMS | Specialist VNS discussion | Selling DBS as proven community care |
| Non-response mid-ECT course | Check seizure quality, benzos/anticonvulsants, threshold rise | Declaring "ECT failed" after three under-dosed sessions |
| Distinguish pseudo-non-response (inadequate seizures, high anticonvulsant load, early stop) from true resistance.[4][6][14][15][21] |
Assessment, capacity and consent
Fellowship answers always include:
- Indication clarity and alternatives discussed honestly (medications, psychotherapy intensity, rTMS when appropriate).[15][21]
- Medical history — cardiac, respiratory, neurological, GORD/aspiration risk, pregnancy, dental, implanted devices.[6][15]
- Medication review — anticonvulsants and benzodiazepines raise seizure threshold; lithium requires anaesthetic caution peri-procedure; theophylline historically linked to prolonged seizures; document hypoglycaemic agents and MAOIs with anaesthetic team.[6][15]
- Baseline cognition and mood ratings where feasible (and BFCRS in catatonia).[8][14]
- Capacity is decision-specific and time-specific. Severe depression can impair appreciation of benefit without abolishing all understanding — reassess. If capacity is lacking and treatment is needed, use jurisdiction-specific mental health legislation (do not invent section numbers for all countries; name that ANZ, UK, US, and Indian statutes differ).[15]
- Informed consent elements — nature of procedure, anaesthesia, expected course length and frequency, common effects (headache, myalgia, temporary confusion), serious rare risks, cognitive risks including autobiographical memory, and the risk of not treating.[8][15]
Investigations
There is no single global mandatory panel, but fellowship practice commonly includes FBC, electrolytes, renal function, glucose; ECG in adults especially with cardiac risk; and further tests driven by history/exam (CXR, echocardiogram, neuroimaging for focal signs or atypical late catatonia). Imaging is not a universal prerequisite for every depression ECT course. Pregnancy testing when relevant. Coordinate device interrogation plans for pacemakers/ICDs with cardiology/anaesthesia.[6][15]
Acute pathway and anaesthesia essentials for the psychiatrist
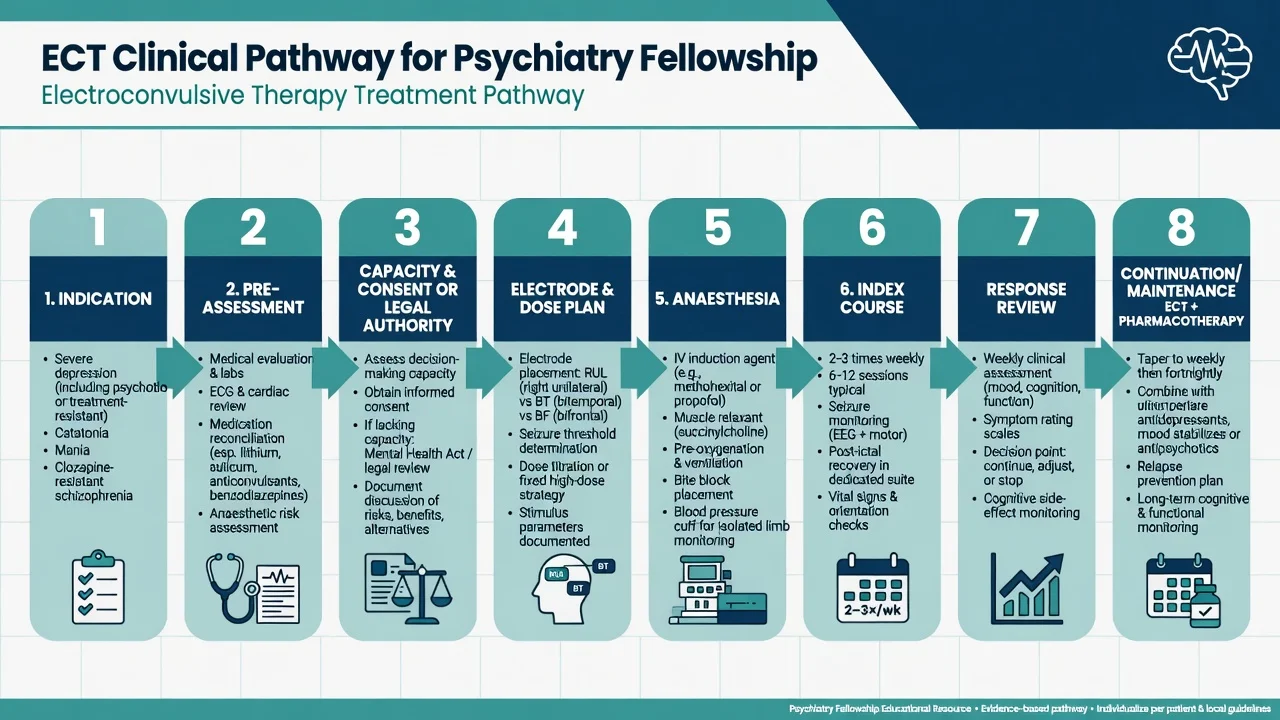
You are not the anaesthetist, but examiners expect operational literacy: short-acting induction agent (often propofol; services may use alternatives such as thiopentone or etomidate when seizure quality is poor — local protocol); muscle relaxant (classically suxamethonium) to reduce musculoskeletal injury; pre-oxygenation, airway support, bite block, continuous monitoring; cuff technique on a limb to observe motor seizure duration despite paralysis; EEG monitoring where available as adjunct to clinical seizure assessment. Psychiatrist roles: confirm indication and legal status that day, electrode placement and stimulus dose plan, medication holds/adjustments, seizure quality review, recovery cognitive check, and series planning.[6][15]
Electrode placement and stimulus dosing
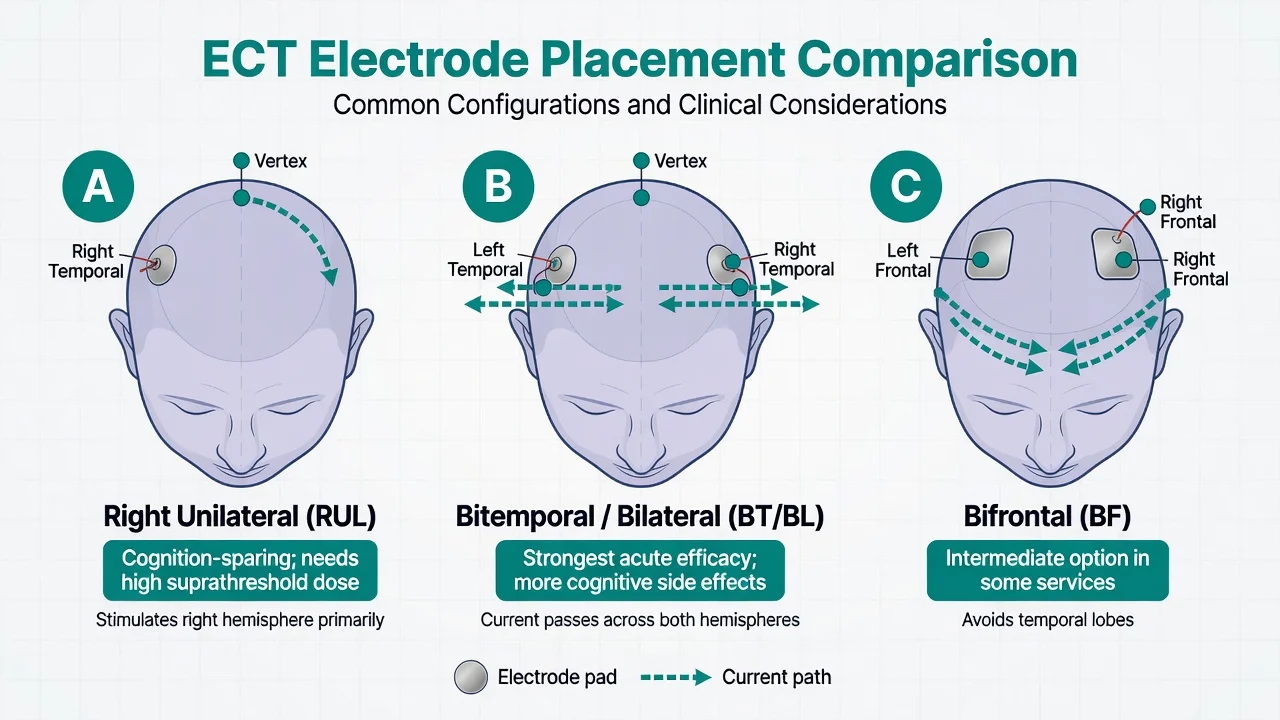
- Often preferred when cognition is priority
- Needs high suprathreshold dosing for efficacy
- Ultrabrief pulse width further reduces cognitive burden for many
- PRIDE supports RUL ultrabrief with venlafaxine in older adults
- Strong acute efficacy; UK Review Group: BL moderately > UL on average
- More cognitive adverse effects on average
- Chosen for urgency, severity, or RUL non-response
- EFFECT-Dep: high-dose unilateral can approach BT efficacy in pragmatic design
- Used in some services as intermediate option
- May spare temporal lobes relative to BT
- Local expertise and protocol driven
- Not a free lunch — still needs proper dosing and monitoring
Stimulus dosing concepts: seizure threshold (ST) is the minimum charge that elicits an adequate seizure and rises over a course and with age/anticonvulsants; titration methods vs formula/age-based methods differ by service but share the principle of relating dose to threshold; RUL is commonly dosed at high multiples of ST while bilateral is often effective at lower multiples; ultrabrief RUL improves cognitive profile in Sackeim work if dosing is competent; frequency is typically two to three treatments weekly for index courses; number is often about 6–12 for depression, stopping for plateau/remission or futility. Sackeim's pulse-width and placement work, Semkovska cognition analyses, EFFECT-Dep, and PRIDE Phase 1 are the modern evidence scaffold for these trade-offs.[7][9][10][11]
Continuation and maintenance
After index remission, plan: (1) optimised pharmacotherapy (for unipolar depression, lithium-containing strategies have classic post-ECT evidence pedigree; individualise to polarity and comorbidity); (2) continuation ECT on a tapering schedule for high relapse risk, prior rapid relapse after ECT, or medication intolerance — CORE C-ECT was a viable strategy versus C-Pharm; (3) combined approaches common in real services; (4) maintenance ECT for highly recurrent illness when benefits outweigh cumulative cognitive and logistical burdens, with quality-of-life data in older adults supporting continuation for selected patients.[2][28][30]
REPLAN
Cognitive adverse effects
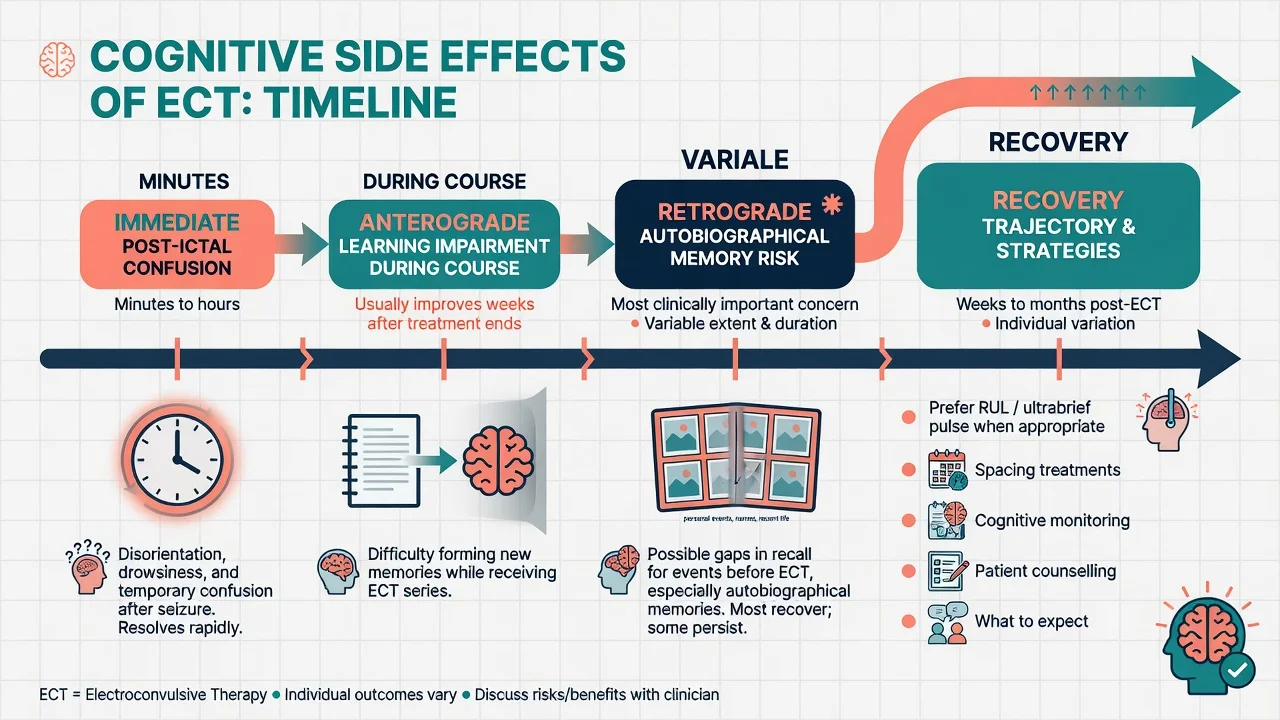
Community and research data (Sackeim community study; Semkovska work) support a nuanced message: post-ictal confusion lasts minutes to hours and is longer in older adults and after bilateral treatments; anterograde learning impairment during the course usually improves in the weeks after; retrograde autobiographical memory loss is the most clinically and medicolegally important risk — variable, sometimes persistent for personal memories around the treatment period; mitigation includes preferring RUL/ultrabrief when clinically appropriate, avoiding unnecessary bilateral dosing, spacing treatments, treating concurrent delirium risks, counselling before consent, and monitoring subjectively and with brief objective screens when possible. Do not gaslight patients who report memory problems. Do not refuse indicated ECT solely for fear of memory change when illness is lethal — balance explicitly.[7][8][9]
Other neurostimulation — evidence tiers
rTMS and iTBS
High-frequency left DLPFC rTMS has positive multisite sham-controlled evidence (O'Reardon Neuronetics trial; George OPT-TMS) and guideline support (Lefaucheur evidence-based guidelines; CANMAT neurostimulation section). Meta-analysis quantifies response and remission rates above sham with acceptable drop-out.[16][17][18][19][21][29]
THREE-D showed intermittent theta-burst stimulation (iTBS) was non-inferior to standard 10 Hz rTMS for depression with substantially shorter session duration — a service-capacity game changer examiners like.[26]
rTMS is outpatient, no anaesthesia, focal, and generally well tolerated (scalp discomfort, headache; seizure rare). It is not a substitute for urgent ECT in malignant catatonia or near-terminal melancholia.[18][21]
tDCS
ELECT-TDCS compared direct-current therapy with escitalopram and placebo contexts in depression — useful trial literacy, but tDCS remains a lower-tier option with more mixed real-world uptake than rTMS/ECT. Position it as investigational/selected adjunct rather than first-line for severe illness.[20][21]
VNS
Implanted vagus nerve stimulation is an adjunct for chronic treatment-resistant depression. Naturalistic and long-term observational data (including Aaronson five-year VNS vs treatment-as-usual comparisons) show gradual response trajectories and possible benefits on suicidality metrics — slower than ECT, different use-case (chronicity, not acute rescue).[22][23][21]
DBS
Mayberg and colleagues' early open-label subcallosal cingulate DBS work generated enthusiasm. The BROADEN multisite sham-controlled trial of SCC DBS for TRD did not meet its primary endpoint — temper any viva claim that DBS is established depression care. Refer only via specialist centres/trials; do not market it as failed-ECT standard of care in community services.[24][25]
RANZCP professional practice guidelines for ECT administration (Weiss et al.) set process standards for ANZ services — training, consent, facilities, monitoring, and quality. Use them as the local professional backbone alongside broader mood-disorder guidance.[15]
CANMAT neurostimulation section ranks ECT highly for efficacy in MDD and positions rTMS as an evidence-supported option for TRD. NICE (UK) and APA materials shape MRCPsych/ABPN framing; always name the guideline when you quote thresholds or pathways.[21][6]
Special populations
Older adults. PRIDE Phase 1 supports right unilateral ultrabrief ECT combined with venlafaxine in geriatric depression with strong remission rates; cognitive monitoring and medical optimisation are mandatory.[11][30]
Pregnancy. When maternal illness is severe (psychosis, catatonia, food refusal, high suicide risk), ECT is often safer than untreated illness or polypharmacy — coordinate obstetric and anaesthetic care, left lateral tilt considerations, and fetal monitoring as indicated.[6][15]
Youth. Specialist pathways, higher consent/assent bar, careful capacity assessment, and second opinions as local policy requires.[15]
Intellectual disability / limited capacity. Syndrome-targeted treatment (especially catatonia) can be transformative; legal substitute decision-making is jurisdiction-specific.[14][15]
Devices and medical comorbidity. Pacemakers, ICDs, cochlear implants, and existing DBS hardware need device-team planning. Unstable cardiac disease raises anaesthetic risk — do not ignore, do not automatically refuse life-saving ECT without cardiology input.[6][15]
Prognosis and disposition
Acute remission rates for severe depression with ECT are high relative to many multi-step medication algorithms, especially with psychotic features. Speed is a clinical advantage.[1][3][5]
Disposition checklist: medical stability, cognitive recovery adequate for safety, suicide risk re-scored, continuation plan booked, carers informed, crisis contacts, and documented electrode/dose recipe for future relapse.[2][15][28]
Escalate from rTMS to ECT when urgency rises, psychosis/catatonia emerges, or non-response is clear. Consider VNS referral for chronic multi-modal TRD in specialised pathways. DBS remains trial/specialist territory after negative pivotal SCC data.[21][23][25]
Evidence, guidelines and controversies
| Landmark / source | Exam take-home |
|---|---|
| UK ECT Review Group 2003 | ECT effective; BL moderately > UL; often > drugs short-term |
| CORE speed + continuation | Fast response; plan relapse prevention (C-ECT vs C-Pharm) |
| Sackeim pulse width/placement | Ultrabrief and placement drive cognition–efficacy trade-off |
| EFFECT-Dep | High-dose unilateral pragmatic non-inferiority framing vs BT |
| PRIDE Phase 1 | RUL ultrabrief + venlafaxine works in older adults |
| Petrides 2015 | ECT augments clozapine-resistant schizophrenia |
| O'Reardon / OPT-TMS / THREE-D / Lefaucheur | rTMS evidence base; iTBS efficiency |
| ELECT-TDCS | tDCS trial literacy; not ECT-equivalent |
| Aaronson VNS 5-year | Long-horizon chronic TRD device data |
| Mayberg open-label vs BROADEN | DBS hope vs failed pivotal SCC RCT |
| Controversies worth owning: autobiographical memory risk communication; involuntary ECT ethics; whether ultrabrief RUL underperforms in the most severe illness if under-dosed; service access inequity; and over-marketing of novel devices ahead of evidence.[1][2][7][10][11][12][16][17][20][23][25][26] |
Exam pearls
SHOCKED
- Generalised cerebral seizure is therapeutic; motor seizure is the bedside proxy.[5][6]
- RUL needs high suprathreshold dose; bilateral is more efficient at lower multiples but costlier cognitively.[7][1]
- Do not delay ECT in malignant catatonia or near-terminal melancholia.[14][6]
- Clozapine-resistant schizophrenia: think ECT augmentation (Petrides), not endless non-clozapine polypharmacy only.[12]
- iTBS ≈ 10 Hz efficacy, shorter sessions (THREE-D).[26]
- DBS for depression is not routine after BROADEN.[25]
- RANZCP PPG (Weiss) is the ANZ process standard for ECT administration.[15]
Viva self-test: why might 'ECT failed' be false?
Check: were seizures adequate in duration/quality? Was RUL under-dosed relative to threshold? Were benzodiazepines or anticonvulsants blocking seizures? Was the course stopped at session 3–4 during a still-rising trajectory? Was the diagnosis catatonia/NMS/encephalitis rather than simple MDD? Was adherence to continuation zero after a good index response, producing rapid relapse mislabelled as non-response?[4][6][7][14]
References
- [1]UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis Lancet, 2003.PMID 12642045
- [2]Kellner CH, Knapp RG, Petrides G, et al. Continuation electroconvulsive therapy vs pharmacotherapy for relapse prevention in major depression: a multisite study from the Consortium for Research in Electroconvulsive Therapy (CORE) Arch Gen Psychiatry, 2006.PMID 17146008
- [3]Husain MM, Rush AJ, Fink M, et al. Speed of response and remission in major depressive disorder with acute electroconvulsive therapy (ECT): a Consortium for Research in ECT (CORE) report J Clin Psychiatry, 2004.PMID 15119910
- [4]Prudic J, Haskett RF, Mulsant B, et al. Resistance to antidepressant medications and short-term clinical response to ECT Am J Psychiatry, 1996.PMID 8678194
- [5]Lisanby SH Electroconvulsive therapy for depression N Engl J Med, 2007.PMID 17989386
- [6]Espinoza RT, Kellner CH Electroconvulsive Therapy N Engl J Med, 2022.PMID 35172057
- [7]Sackeim HA, Prudic J, Nobler MS, et al. Effects of pulse width and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy Brain Stimul, 2008.PMID 19756236
- [8]Sackeim HA, Prudic J, Fuller R, et al. The cognitive effects of electroconvulsive therapy in community settings Neuropsychopharmacology, 2007.PMID 16936712
- [9]Semkovska M, Keane D, Babalola O, et al. Unilateral brief-pulse electroconvulsive therapy and cognition: effects of electrode placement, stimulus dosage and time J Psychiatr Res, 2011.PMID 21109254
- [10]Semkovska M, Landau S, Dunne R, et al. Bitemporal Versus High-Dose Unilateral Twice-Weekly Electroconvulsive Therapy for Depression (EFFECT-Dep): A Pragmatic, Randomized, Non-Inferiority Trial Am J Psychiatry, 2016.PMID 26892939
- [11]Kellner CH, Husain MM, Knapp RG, et al. Right Unilateral Ultrabrief Pulse ECT in Geriatric Depression: Phase 1 of the PRIDE Study Am J Psychiatry, 2016.PMID 27418379
- [12]Petrides G, Malur C, Braga RJ, et al. Electroconvulsive therapy augmentation in clozapine-resistant schizophrenia: a prospective, randomized study Am J Psychiatry, 2015.PMID 25157964
- [13]Tharyan P, Adams CE Electroconvulsive therapy for schizophrenia Cochrane Database Syst Rev, 2005.PMID 15846598
- [14]Bush G, Fink M, Petrides G, et al. Catatonia. I. Rating scale and standardized examination Acta Psychiatr Scand, 1996.PMID 8686483
- [15]Weiss A, Hussain S, Ng B, et al. Royal Australian and New Zealand College of Psychiatrists professional practice guidelines for the administration of electroconvulsive therapy Aust N Z J Psychiatry, 2019.PMID 30966782
- [16]O'Reardon JP, Solvason HB, Janicak PG, et al. Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: a multisite randomized controlled trial Biol Psychiatry, 2007.PMID 17573044
- [17]George MS, Lisanby SH, Avery D, et al. Daily left prefrontal transcranial magnetic stimulation therapy for major depressive disorder: a sham-controlled randomized trial Arch Gen Psychiatry, 2010.PMID 20439832
- [18]Lefaucheur JP, Aleman A, Baeken C, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014-2018) Clin Neurophysiol, 2020.PMID 31901449
- [19]Berlim MT, van den Eynde F, Tovar-Perdomo S, et al. Response, remission and drop-out rates following high-frequency repetitive transcranial magnetic stimulation (rTMS) for treating major depression: a systematic review and meta-analysis of randomized, double-blind and sham-controlled trials Psychol Med, 2014.PMID 23507264
- [20]Brunoni AR, Moffa AH, Sampaio-Junior B, et al. Trial of Electrical Direct-Current Therapy versus Escitalopram for Depression N Engl J Med, 2017.PMID 28657871
- [21]Milev RV, Giacobbe P, Kennedy SH, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 4. Neurostimulation Treatments Can J Psychiatry, 2016.PMID 27486154
- [22]Rush AJ, Marangell LB, Sackeim HA, et al. Effects of 12 months of vagus nerve stimulation in treatment-resistant depression: a naturalistic study Biol Psychiatry, 2005.PMID 16139581
- [23]Aaronson ST, Sears P, Ruvuna F, et al. A 5-Year Observational Study of Patients With Treatment-Resistant Depression Treated With Vagus Nerve Stimulation or Treatment as Usual: Comparison of Response, Remission, and Suicidality Am J Psychiatry, 2017.PMID 28359201
- [24]Mayberg HS, Lozano AM, Voon V, et al. Deep brain stimulation for treatment-resistant depression Neuron, 2005.PMID 15748841
- [25]Holtzheimer PE, Husain MM, Lisanby SH, et al. Subcallosal cingulate deep brain stimulation for treatment-resistant depression: a multisite, randomised, sham-controlled trial Lancet Psychiatry, 2017.PMID 28988904
- [26]Blumberger DM, Vila-Rodriguez F, Thorpe KE, et al. Effectiveness of theta burst versus high-frequency repetitive transcranial magnetic stimulation in patients with depression (THREE-D): a randomised non-inferiority trial Lancet, 2018.PMID 29726344
- [27]Daly JJ, Prudic J, Devanand DP, et al. ECT in bipolar and unipolar depression: differences in speed of response Bipolar Disord, 2001.PMID 11333069
- [28]Prudic J, Haskett RF, McCall WV, et al. Pharmacological strategies in the prevention of relapse after electroconvulsive therapy J ECT, 2013.PMID 23303417
- [29]Lefaucheur JP, André-Obadia N, Antal A, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS) Clin Neurophysiol, 2014.PMID 25034472
- [30]McCall WV, Lisanby SH, Rosenquist PB, et al. Effects of continuation electroconvulsive therapy on quality of life in elderly depressed patients: A randomized clinical trial J Psychiatr Res, 2018.PMID 29195125