Psych · Psychopharmacology — EPS and tardive dyskinesia
Extrapyramidal side effects and tardive dyskinesia
Also known as EPS · Drug-induced movement disorders · Acute dystonia · Akathisia · Drug-induced parkinsonism · Tardive dyskinesia · VMAT2 inhibitors · Valbenazine · Deutetrabenazine
Fellowship-depth atlas of antipsychotic-related extrapyramidal syndromes — acute dystonia (including laryngeal), akathisia (Barnes scale), drug-induced parkinsonism, tardive dyskinesia (Schooler–Kane, AIMS, Carbon/Solmi epidemiology), and VMAT2 inhibitor evidence (KINECT 3, ARM-TD, AIM-TD). FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Extrapyramidal side effects and tardive dyskinesia sit at the centre of everyday antipsychotic safety vivas. Examiners want tempo taxonomy, discriminators (especially drug-induced parkinsonism versus TD), named scales (Barnes, AIMS), acute rescue doses, prevention culture, and the modern VMAT2 evidence base — not a laundry list of brand names.[2][13][22]
Definition and classification
Extrapyramidal side effects (EPS) are drug-induced movement disorders arising principally from nigrostriatal dopamine D2 pathway disruption. Antipsychotics are the classic cause; other D2 antagonists (metoclopramide, prochlorperazine, some calcium-channel agents historically) matter in medical and surgical wards.[13][23]
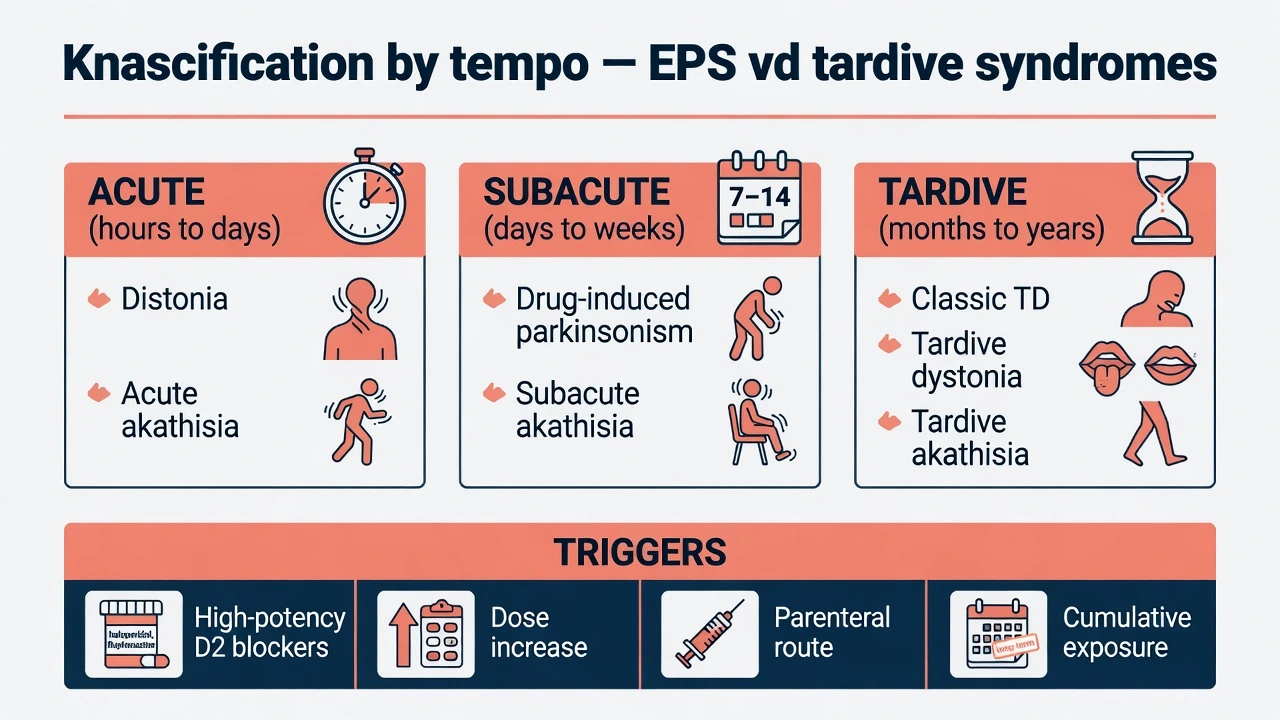
Tempo is the exam scaffold. Acute (hours to days): dystonia and acute akathisia. Subacute (days to weeks): drug-induced parkinsonism and subacute akathisia. Tardive (months to years of cumulative exposure; shorter windows possible in older adults): classic TD, tardive dystonia, and tardive akathisia.[1][13][23]
| Tempo | Typical window | Core syndromes |
|---|---|---|
| Acute | Hours to a few days after start, increase, or parenteral dose | Acute dystonia; acute akathisia |
| Subacute | Days to weeks | Drug-induced parkinsonism; subacute akathisia |
| Tardive | Months to years of cumulative exposure (shorter possible in older adults) | Classic TD; tardive dystonia; tardive akathisia |
| Tempo taxonomy above is the standard exam scaffold for EPS and tardive syndromes.[13][23] |
DSM-5-TR and ICD-11 frame these as medication-induced movement disorders / adverse effects, not primary psychiatric diagnoses. Do not collapse all tardive syndromes into one entity: classic orobuccolingual TD, tardive dystonia, and tardive akathisia have different disability profiles and treatment nuances.[1][13][22]
Schooler–Kane research diagnoses for TD remain the historical exam reference: characteristic choreiform/athetoid movements after sufficient cumulative neuroleptic exposure (commonly taught as about three months in younger adults, with shorter thresholds considered in older people), with exclusion of alternative causes. Use the criteria to structure research thinking and documentation even when everyday practice is clinical-probability based.[1]
Epidemiology and risk
TD was not abolished by second-generation antipsychotics. Carbon and colleagues meta-analysed prevalence in the SGA era and found substantial residual burden — order of about one in five in many treated samples depending on methodology and population — so "atypical means safe from TD" is an exam fail.[9]
In comparative randomised evidence, FGA exposure carries higher TD risk than SGA exposure, but absolute SGA risk is not zero; agent selection, dose, duration, and host factors still matter.[15][18]
Solmi risk factors to recite under pressure: older age, female sex (especially orofacial patterns), longer cumulative exposure, higher cumulative dose, early EPS, substance use, mood-disorder indications in some series, and medical brain vulnerability (e.g. diabetes, prior brain injury) in parts of the literature. Acute dystonia clusters in young males after high-potency FGAs, rapid escalation, or parenteral dosing.[8][11][23]
Akathisia remains common with high-potency FGAs and is clinically important with several SGAs, notably aripiprazole-class partial agonists and higher-dose risperidone/haloperidol patterns — and is systematically under-recognised.[14][18]
Numbers examiners expect you to contextualise
Pathophysiology
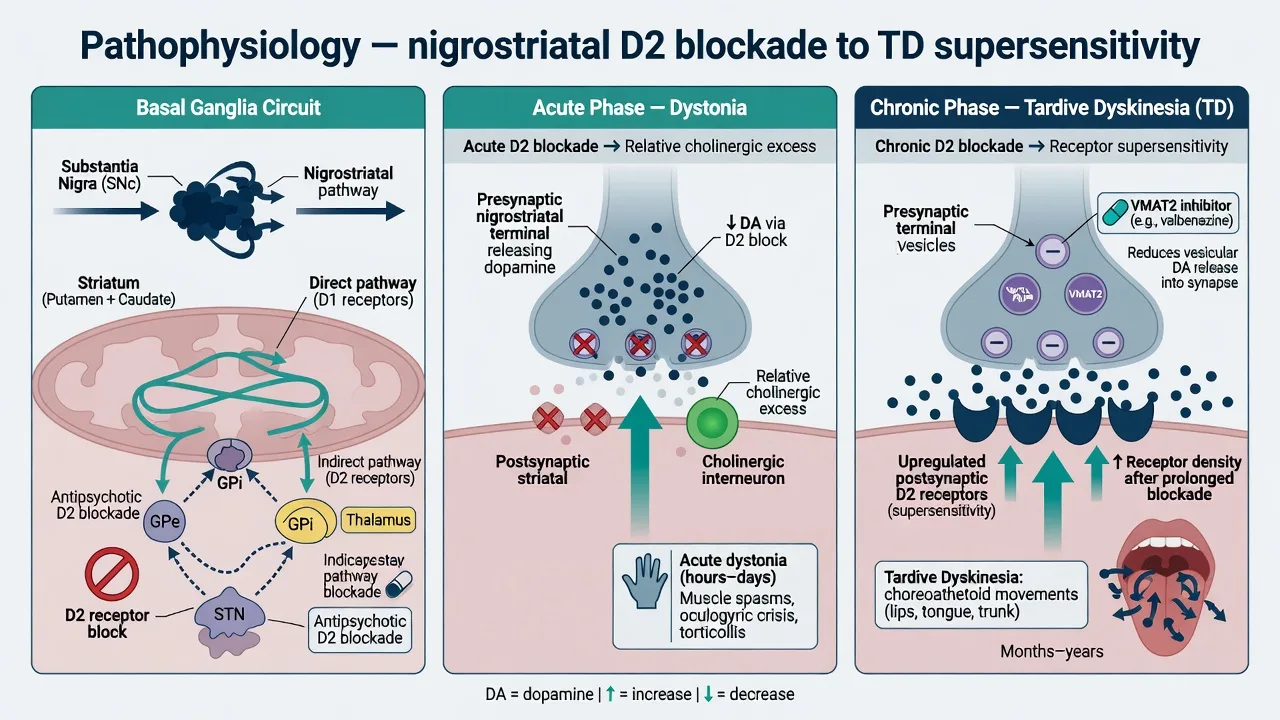
Map every side-effect to a pathway before inventing mechanisms. Nigrostriatal D2 blockade unbalances basal ganglia direct and indirect pathways. Acute dystonia reflects sudden D2 blockade with relative cholinergic excess — the pharmacological rationale for anticholinergic rescue.[11][23]
Akathisia is not "pure anxiety": mesocortical and ventral striatal dopamine disruption, with noradrenergic and serotonergic contributions, produce the subjective urge to move plus motor restlessness.[14]
Tardive dyskinesia is conceptualised as maladaptive plasticity after chronic D2 blockade, including postsynaptic dopamine receptor supersensitivity. That model explains why VMAT2 inhibitors (which reduce vesicular packaging and synaptic dopamine availability) can reduce dyskinetic movements even while an antipsychotic continues, and why abrupt antipsychotic withdrawal can transiently unmask or worsen TD before any later improvement.[3][10][22]
Clinical presentation
Acute dystonia
Onset typically within hours to days of starting or increasing a dopamine antagonist, or after parenteral dosing. Phenotypes: torticollis, trismus, tongue protrusion, oculogyric crisis, opisthotonus. Laryngeal dystonia presents with stridor, dyspnoea, or choking sensation and is an airway emergency — not "functional" until proven otherwise.[11][13][23]
Drug-induced parkinsonism (DIP)
Bradykinesia, rigidity, tremor, shuffling gait — often more bilateral and temporally linked to drug exposure than idiopathic Parkinson disease. Distinguish carefully from TD: management is opposite in key respects (anticholinergics may help DIP and worsen classic TD).[10]
Akathisia
Subjective sense of inner restlessness plus objective fidgeting, rocking, pacing, or inability to remain seated. Use the Barnes Akathisia Rating Scale structure: objective items, subjective awareness, distress, and global clinical assessment. Severe akathisia is associated with agitation and elevated self-harm risk if misread as worsening psychosis and treated with more dopamine blockade.[2][14]
Tardive dyskinesia
Classic pattern: oro-bucco-lingual movements (chewing, lip smacking, tongue darting, grimacing) with or without limb/trunk choreoathetosis. Movements often suppress briefly on command, worsen with distraction, and diminish in sleep. Tardive dystonia produces sustained postures and can be highly disabling, sometimes in younger patients.[1][22][24]

Differential diagnosis — discriminators, not lists
DIP vs TD
- DIP: bradykinesia/rigidity/tremor
- TD: hyperkinetic choreiform/orofacial
- Anticholinergics: help DIP, risk worsening TD
- Onset windows often differ
Akathisia vs agitation
- Akathisia: urge to move + distress
- Psychosis agitation: thought content drives behaviour
- More antipsychotic worsens akathisia
- Ask specifically about restlessness
TD mimics
- Edentulous dyskinesia
- Huntington / other chorea
- Hyperthyroidism
- Spontaneous elderly orofacial movements
- Functional movement disorder
Systemic traps
- NMS: fever, rigidity, autonomic storm
- Serotonin toxicity: clonus/hyperreflexia
- Not pure EPS algorithms
- Stop offenders, escalate medical care
Assessment and scales
History: full dopamine-antagonist timeline (oral, LAI, antiemetics), dose changes, adherence, substances, prior EPS, mood versus schizophrenia indication.[13][24]
Bedside exam: observe at rest, with activation manoeuvres used in AIMS (finger tapping, distraction), gait, tone, eye movements, speech. Document subjective restlessness for akathisia even if objective signs are subtle.[2][21]
AIMS (Abnormal Involuntary Movement Scale): structured observation of facial/oral, extremity, and trunk movements plus global severity/incapacitation/awareness. Track serial totals. Stacy and colleagues characterised minimal clinically important difference concepts for AIMS change in TD trials — roughly a two-point range is discussed as clinically meaningful context, not a rigid cut-off for every patient.[21][22]
Barnes scale for akathisia; Simpson–Angus for parkinsonism when quantifying DIP. Delphi consensus work emphasises systematic screening rather than waiting for complaint in chronic antipsychotic users.[2][24]
Investigations are mainly for atypical or progressive cases (thyroid, copper studies in young dystonia, imaging if red flags) and for NMS work-up if systemic features appear. There is no confirmatory blood test for TD.[13][22]
Acute and emergency management
Acute dystonia
- Secure airway if laryngeal involvement; call for emergency help early.[11][13]
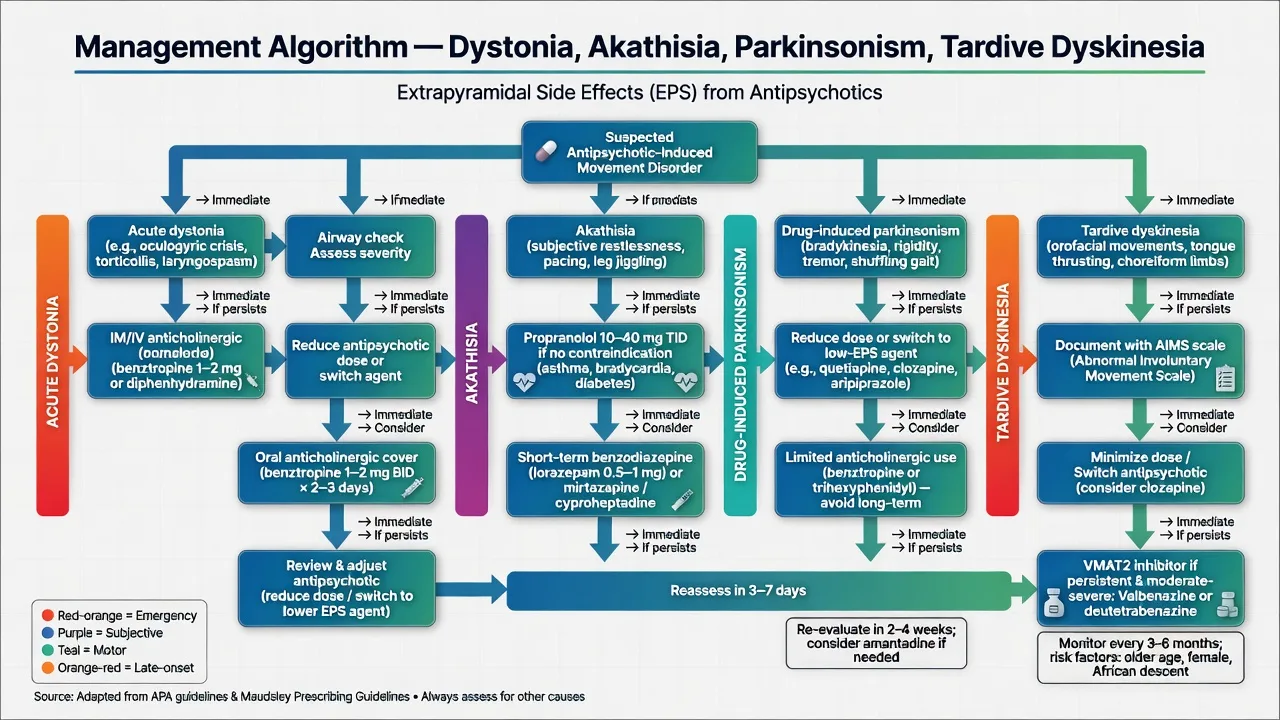
- Give parenteral anticholinergic: benztropine 1–2 mg IM or IV is a standard exam regimen (or diphenhydramine where local protocols use it); repeat if incomplete response per protocol.[11][13][23]
- Offer short oral anticholinergic cover for 1–3 days after a severe episode (e.g. benztropine 1–2 mg oral one to two times daily short-term — individualise and check local product information).[11][13]
- Review the antipsychotic: reduce dose, switch potency, avoid unnecessary parenteral high-potency agents.[11][13][23]
Severe akathisia
Do not escalate antipsychotic for "agitation." Reduce dose or switch to a lower-akathisia agent. Propranolol is the classic adjunct when no contraindication (asthma, significant bradycardia/heart block, uncontrolled heart failure): exam-style starting ranges often 10–20 mg two to three times daily, titrating toward 20–40 mg two to three times daily as tolerated under monitoring — always check local product information and medical comorbidity.[14][17]
Short-term benzodiazepines, and other agents (e.g. low-dose mirtazapine, cyproheptadine in some pathways) appear in network meta-analytic rankings; anticholinergics are more reliable for dystonia/parkinsonism than for pure akathisia.[17]
DIP
Reduce dose or switch toward lower-EPS agents (e.g. quetiapine, clozapine when indicated, or carefully chosen partial agonists depending on context). Limit duration of anticholinergic therapy because of cognitive harm and TD concerns with chronic use.[10][18]
Definitive management of tardive dyskinesia
Prevention first: lowest effective antipsychotic dose, justified duration, avoid unnecessary polypharmacy and high-potency escalation, screen longitudinally, educate patients and carers.[8][12][24]
When TD appears, use a structured pathway rather than reassurance alone.[16][22][24]
- Document AIMS and functional impact; confirm drug association and exclude mimics.[21][22]
- Re-evaluate whether the antipsychotic is still essential; if yes, minimise dose and consider switch to a lower-TD-risk option. Clozapine has a long clinical tradition as a switch target when ongoing antipsychotic treatment is required and TD is significant (specialist monitoring applies).[6][16]
- Avoid chronic anticholinergics for classic TD — they do not treat the hyperkinetic movements and may worsen them.[6][10]
- Offer a VMAT2 inhibitor when TD is moderate–severe or functionally impairing and available/indicated.[3][4][5][16]
VMAT2 inhibitors — name the trials
| Agent | Landmark trials | Exam dosing orientation | Notes |
|---|---|---|---|
| Valbenazine | KINECT 3 (Hauser 2017); long-term open-label extensions | Once daily; trial programmes used 40 mg and 80 mg daily regimens — follow current product information for start, titration, hepatic adjustment | AIMS improved vs placebo; monitor for somnolence, parkinsonism, QT/depression warnings per label |
| Deutetrabenazine | ARM-TD (Fernandez 2017); AIM-TD (Anderson 2017) | Twice-daily titration schedules with food per label — do not invent a single fixed "always" dose | AIMS benefit vs placebo across programmes; depression/suicidality class concerns historically for tetrabenazine family |
| Valbenazine once-daily regimens in KINECT 3 used 40 mg and 80 mg daily arms; deutetrabenazine uses twice-daily titration with food per product information and the ARM-TD/AIM-TD programmes — always confirm current local labels before prescribing.[3][4][5][20] |
KINECT 3 demonstrated clinically meaningful AIMS reduction with once-daily valbenazine versus placebo in adults with TD.[3] ARM-TD and AIM-TD established deutetrabenazine efficacy in randomised designs with different dose strategies and endpoints.[4][5] Long-term open-label data support durability of benefit for many patients who continue therapy, with expected return of movements if stopped.[20]
AAN 2013 guidance on tardive syndromes pre-dated full VMAT2 labelling for TD; Bhidayasiri 2018 updated algorithms incorporating newer evidence. Canadian recommendations (Ricciardi 2019) and Delphi screening consensus (Caroff 2020) reinforce measurement-based diagnosis and structured treatment pathways.[6][7][16][24]
Older options (tetrabenazine, amantadine, clonazepam, Ginkgo in selected older literature, vitamin E debates) appear in historical AAN discussions with weaker or mixed evidence compared with modern VMAT2 RCTs — answer with evidence tiers, not nostalgia.[6][7]
Special populations and scenarios
Older adults: higher TD risk at lower cumulative exposures; avoid antipsychotics for dementia-related behavioural symptoms unless last-line after non-drug strategies and clear risk–benefit documentation.[8][12]
Youth: dystonia-prone; start low; counsel families about early restlessness versus agitation.[14][23]
Parkinson disease / DLB: extreme sensitivity to D2 blockade — prefer avoiding high-potency agents; if psychosis treatment is essential, specialist pathways favour low-D2-burden options.[10]
Intellectual disability / autism: stereotypies can mimic TD; akathisia may present as irritability or self-injury — collateral history and serial observation are essential.[22]
Medical antiemetics: metoclopramide-associated TD is a classic non-psychiatric trap; stop the offender and apply the same TD principles.[13]
APA schizophrenia guidance embeds physical-health and adverse-effect monitoring, including neurological side-effects, into routine care.[12] NICE and RANZCP-aligned practice similarly expect structured side-effect enquiry, metabolic monitoring, and shared decision when TD appears. VMAT2 access, brand availability, and subsidy differ by jurisdiction — state the clinical indication and evidence, then name local formulary pathways rather than inventing funding rules. US product labels for valbenazine and deutetrabenazine drive dosing details in ABPN-style items; ANZ candidates should know trial names and class effects even when access is specialist-only.
Prognosis and disposition
Acute dystonia usually responds dramatically to anticholinergic rescue if the airway is protected. DIP often improves over weeks after dose reduction or switch. Akathisia generally improves with adjustment but chronic/tardive forms are harder. TD may persist for years; some improve slowly after drug change; VMAT2 can reduce severity while continued; movements commonly re-emerge on VMAT2 withdrawal.[3][10][20]
Disposition: medical emergency pathways for laryngeal dystonia and NMS-spectrum presentations; same-day senior review for severe akathisia with risk; outpatient AIMS-based follow-up for chronic antipsychotic clinics.[12][24]
Evidence, guidelines, controversies
Controversies to handle calmly: how early to start VMAT2 versus switch-first strategies; whether mild TD always warrants drug change when psychosis is fragile; duration of anticholinergic prophylaxis after dystonia; ranking of non-propranolol akathisia agents. Answer with measurement, patient values, relapse risk, and evidence tier.[7][16][17]
CATIE and related effectiveness literature remind candidates that real-world antipsychotic choice is a tolerability trade-off — neurological and metabolic harms both drive discontinuation.[18][19]
Exam pearls
DAPT for EPS clinics
DAPT
References
- [1]Schooler NR, Kane JM Research diagnoses for tardive dyskinesia Arch Gen Psychiatry, 1982.PMID 6121550
- [2]Barnes TR A rating scale for drug-induced akathisia Br J Psychiatry, 1989.PMID 2574607
- [3]Hauser RA, Factor SA, Marder SR, et al. KINECT 3: A Phase 3 Randomized, Double-Blind, Placebo-Controlled Trial of Valbenazine for Tardive Dyskinesia Am J Psychiatry, 2017.PMID 28320223
- [4]Anderson KE, Stamler D, Davis MD, et al. Deutetrabenazine for treatment of involuntary movements in patients with tardive dyskinesia (AIM-TD): a double-blind, randomised, placebo-controlled, phase 3 trial Lancet Psychiatry, 2017.PMID 28668671
- [5]Fernandez HH, Factor SA, Hauser RA, et al. Randomized controlled trial of deutetrabenazine for tardive dyskinesia: The ARM-TD study Neurology, 2017.PMID 28446646
- [6]Bhidayasiri R, Fahn S, Weiner WJ, et al. Evidence-based guideline: treatment of tardive syndromes: report of the Guideline Development Subcommittee of the American Academy of Neurology Neurology, 2013.PMID 23897874
- [7]Bhidayasiri R, Jitkritsadakul O, Friedman JH, Fahn S Updating the recommendations for treatment of tardive syndromes: A systematic review of new evidence and practical treatment algorithm J Neurol Sci, 2018.PMID 29454493
- [8]Solmi M, Pigato G, Kane JM, Correll CU Clinical risk factors for the development of tardive dyskinesia J Neurol Sci, 2018.PMID 29439776
- [9]Carbon M, Hsieh CH, Kane JM, Correll CU Tardive Dyskinesia Prevalence in the Period of Second-Generation Antipsychotic Use: A Meta-Analysis J Clin Psychiatry, 2017.PMID 28146614
- [10]Ward KM, Citrome L Antipsychotic-Related Movement Disorders: Drug-Induced Parkinsonism vs. Tardive Dyskinesia-Key Differences in Pathophysiology and Clinical Management Neurol Ther, 2018.PMID 30027457
- [11]Rupniak NM, Jenner P, Marsden CD Acute dystonia induced by neuroleptic drugs Psychopharmacology (Berl), 1986.PMID 2871578
- [12]Keepers GA, Fochtmann LJ, Anzia JM, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia Am J Psychiatry, 2020.PMID 32867516
- [13]Haddad PM, Dursun SM Neurological complications of psychiatric drugs: clinical features and management Hum Psychopharmacol, 2008.PMID 18098217
- [14]Kumar R, Sachdev PS Akathisia and second-generation antipsychotic drugs Curr Opin Psychiatry, 2009.PMID 19378382
- [15]Carbon M, Kane JM, Leucht S, Correll CU Tardive dyskinesia risk with first- and second-generation antipsychotics in comparative randomized controlled trials: a meta-analysis World Psychiatry, 2018.PMID 30192088
- [16]Ricciardi L, Pringsheim T, Barnes TRE, et al. Treatment Recommendations for Tardive Dyskinesia Can J Psychiatry, 2019.PMID 30791698
- [17]Gerolymos C, Barazer R, Yon DK, et al. Drug Efficacy in the Treatment of Antipsychotic-Induced Akathisia: A Systematic Review and Network Meta-Analysis JAMA Netw Open, 2024.PMID 38451521
- [18]Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis Lancet, 2013.PMID 23810019
- [19]Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia N Engl J Med, 2005.PMID 16172203
- [20]Lindenmayer JP, Verghese C, Marder SR, et al. A long-term, open-label study of valbenazine for tardive dyskinesia CNS Spectr, 2021.PMID 32419679
- [21]Stacy M, Sajatovic M, Kane JM, et al. Abnormal involuntary movement scale in tardive dyskinesia: Minimal clinically important difference Mov Disord, 2019.PMID 31234240
- [22]Correll CU, Citrome L Diagnostic and Treatment Fundamentals for Tardive Dyskinesia J Clin Psychiatry, 2021.PMID 34644461
- [23]Casey DE Motor and mental aspects of acute extrapyramidal syndromes Acta Psychiatr Scand Suppl, 1994.PMID 7914042
- [24]Caroff SN, Citrome L, Meyer J, et al. A Modified Delphi Consensus Study of the Screening, Diagnosis, and Treatment of Tardive Dyskinesia J Clin Psychiatry, 2020.PMID 31995677