Psych · Psychopharmacology — ketamine and esketamine
Ketamine and esketamine
Also known as Spravato · Esketamine nasal spray · Racemic ketamine depression · IV ketamine TRD · NMDA antagonist antidepressant
Exam-exhaustive fellowship reference on ketamine and esketamine for treatment-resistant depression — pharmacology, 0.5 mg/kg IV protocols, IN esketamine dosing and supervised observation, TRANSFORM/SUSTAIN/ASPIRE evidence, ELEKT-D vs ECT, dissociation and BP monitoring, abuse and bladder cautions, special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
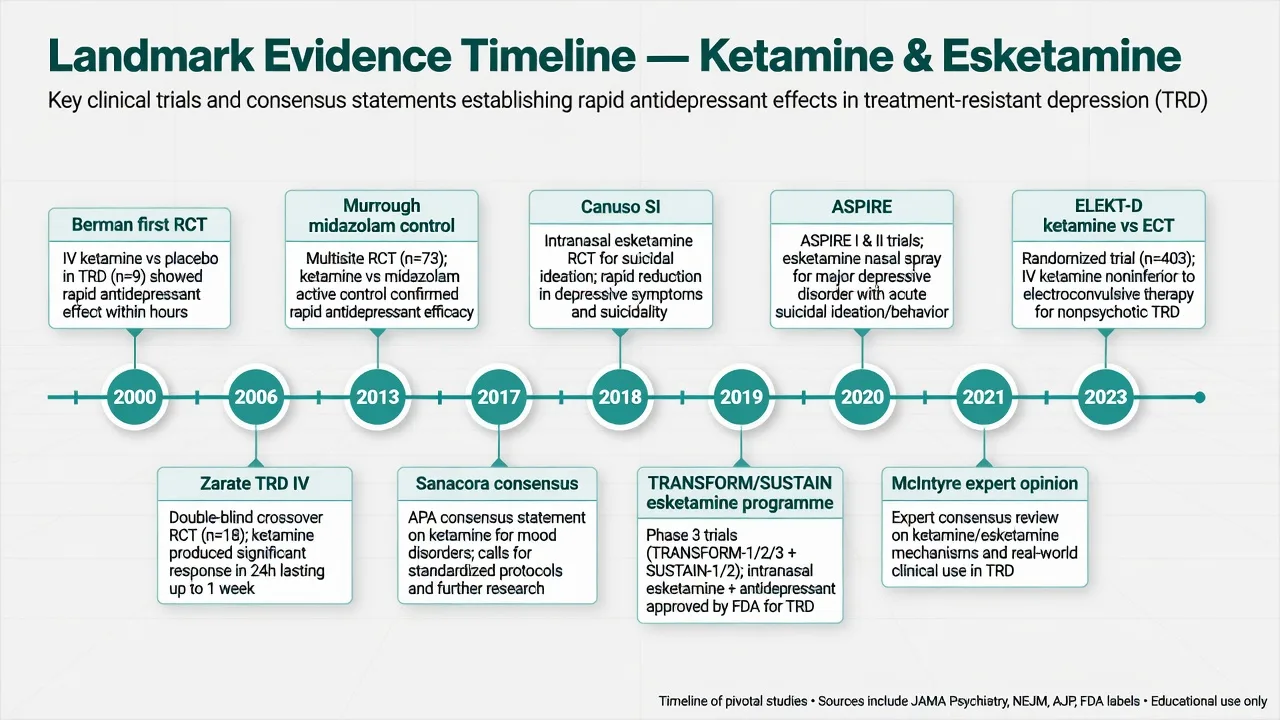
Ketamine and esketamine are high-yield fellowship topics because examiners test indication discipline, protocol literacy, safety monitoring, and honest reading of trial programmes in the same station. Berman opened the RCT door; Zarate and Murrough established sub-anaesthetic IV racemic ketamine in TRD; the esketamine phase 3 programme (TRANSFORM, SUSTAIN, ASPIRE) created a labelled pathway; Sanacora and McIntyre set implementation standards; ELEKT-D reframed the ECT conversation for nonpsychotic TRD.[1][2][3][9][13][15][21][23]

Definition and place in treatment
Racemic ketamine is a 1:1 mixture of R- and S-enantiomers, long used as a dissociative anaesthetic, now used at sub-anaesthetic doses for rapid antidepressant effect (largely off-label for depression outside research or local governance frameworks). Esketamine is the S-enantiomer formulated as a supervised nasal spray with regulatory pathways for treatment-resistant depression (TRD) in combination with an oral antidepressant, and — in jurisdictions where approved — for depressive symptoms in MDD with active suicidal ideation with intent, still under structured care.[4][8][9][13][21]
These agents sit in stepped care after failed monoaminergic trials, not as casual first-line tablets. They do not replace formulation, psychotherapy access, social interventions, or suicide risk management. International expert opinion synthesises implementation standards: diagnosis confirmed, monitoring infrastructure present, informed consent explicit about benefits, limits, and unknowns.[9][21]
Classification, entry criteria and pseudo-resistance
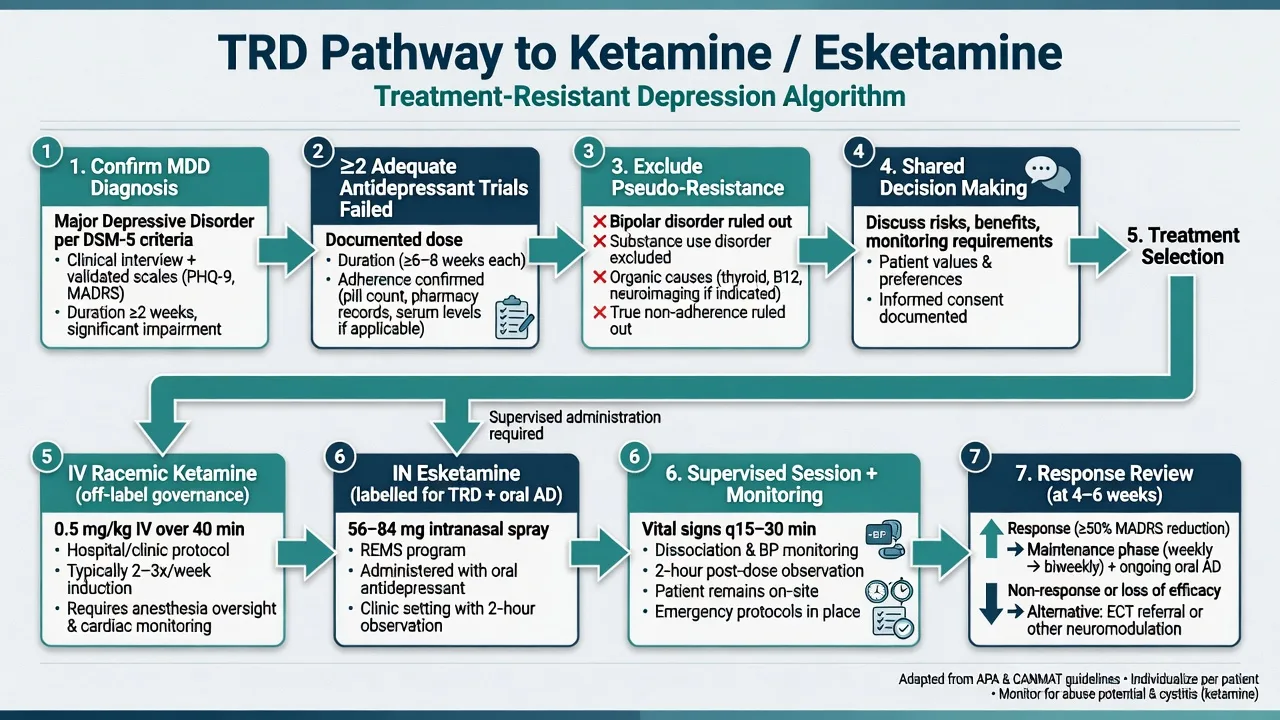
TRD teaching scaffold for exams: major depressive episode with inadequate response to at least two adequate antidepressant trials (dose, duration, adherence documented). Always exclude pseudo-resistance: wrong diagnosis (bipolar spectrum), substance-induced mood disorder, organic contributors, non-adherence, under-dosing, and inadequate psychotherapy exposure when relevant.[4][21]
| Construct | Exam meaning |
|---|---|
| Adequate AD trial | Therapeutic dose range, sufficient duration (commonly several weeks at target), adherence verified |
| True TRD | Persistent depressive syndrome after two adequate failed trials |
| Pseudo-resistance | Wrong diagnosis, substances, non-adherence, organic depression, under-dosing |
| Labelled esketamine TRD | Supervised IN esketamine plus oral antidepressant in pivotal designs |
| Off-label IV ketamine | Local governance, consent, monitoring — not informal DIY infusion |
| Pivotal esketamine TRD trials used a newly initiated or optimised oral antidepressant alongside nasal spray — do not describe labelled TRD use as free-standing monotherapy in exam answers unless discussing specific research contexts.[13][14][21] |
Epidemiology and clinical need
TRD carries outsized disability, hospitalisation, and suicide risk relative to treatment-responsive depression. Rapid-acting options matter because classical antidepressants take weeks and leave a lethal window for some patients. Meta-analytic and trial syntheses show ketamine-class agents can produce large short-term antidepressant effects relative to control conditions, with the durability problem solved only partly by repeated dosing and maintenance strategies.[4][5][16][21]
Abuse and diversion context is part of epidemiology for service design: ketamine has non-medical use; clinics must control supply, observe dosing, and screen for substance-use comorbidity. Chronic high-dose recreational use is linked to ulcerative cystitis and other urinary pathology — counsel and watch chronic exposure patterns.[9][10][22]
Pathophysiology and mechanism
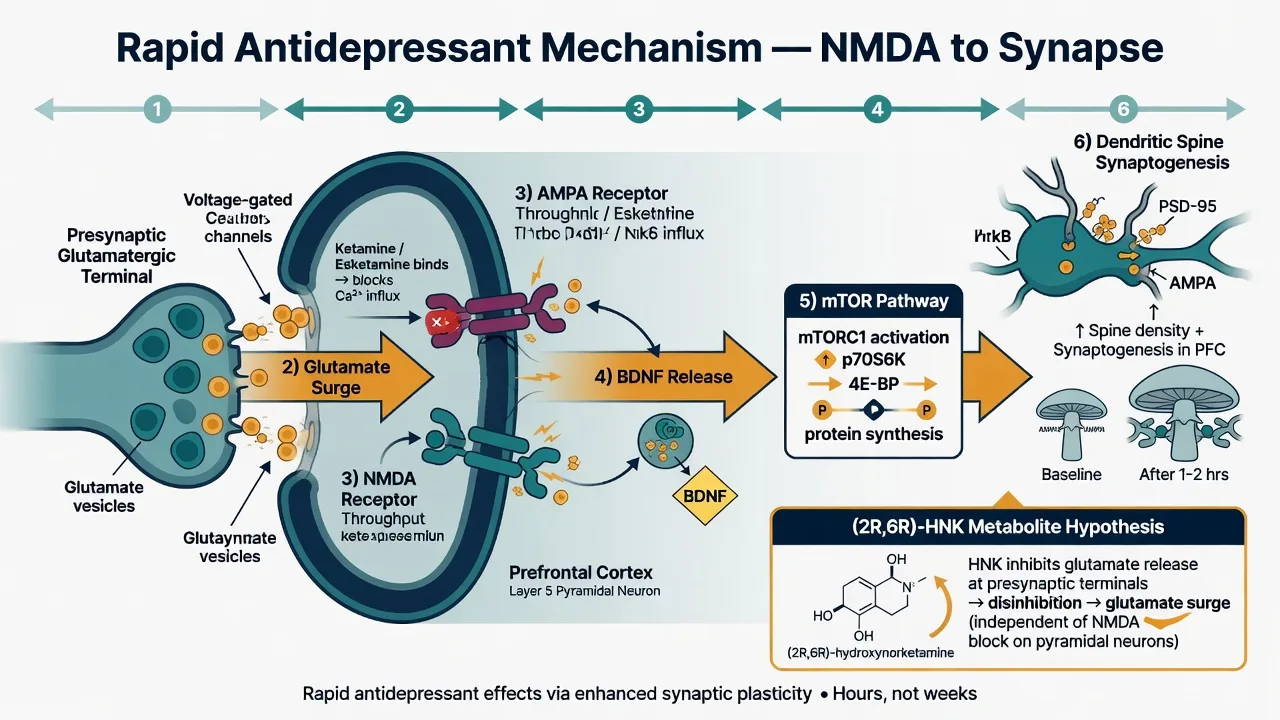
The dominant teaching model: NMDA receptor antagonism → glutamate surge and AMPA throughput → BDNF signalling → mTOR-dependent dendritic spine formation and synaptogenesis in mood-relevant circuits (prefrontal cortex emphasis in preclinical work).[6][4]
Metabolite science. Zanos and colleagues showed that the ketamine metabolite (2R,6R)-hydroxynorketamine can exert antidepressant-like effects in models with reduced sensory-side-effect burden, partially independent of direct NMDAR inhibition — viva-ready nuance, not a licence to ignore parent-drug cardiovascular and dissociative effects in clinic.[7]
Cardiovascular and dissociative effects map to sympathetic activation and perceptual disruption at sub-anaesthetic doses: expect transient blood-pressure and heart-rate rises and dose-session dissociation that usually settle with observation.[10][22]
Clinical effects and time course
Onset. Berman and Zarate established that antidepressant benefit can appear within hours of a single IV infusion, with peak effects often cited around 24 hours — orders of magnitude faster than classical ADs.[1][2]
Durability. Single-dose benefit often fades over days; repeated infusions and maintenance strategies extend benefit (Phillips and colleagues randomised single vs repeated vs maintenance-style IV ketamine exposure).[16]
Esketamine programme time course. Induction commonly twice weekly for four weeks, then weekly or every other week maintenance with ongoing oral AD; SUSTAIN-1 showed that continuing esketamine after response reduces relapse versus discontinuation.[13][15][18]
Session phenomenology. Dissociation, dizziness, nausea, sedation, and perceptual changes are common and usually transient; blood pressure rises require protocolised measurement and thresholds for intervention.[10][22]
Numbers every candidate must own
These anchors are exam orientation numbers from protocols and landmark programmes — always individualise to the patient, product information, and local governance.[2][13][15][23]
Differential diagnosis that changes the plan
| Presentation | Prefer | Do not miss |
|---|---|---|
| "TRD" after micro-doses or non-adherence | Optimise AD trial first | Infusion theatre without documentation |
| Depressive syndrome with prior mania | Bipolar pathway; specialist ketamine only | Uncritical unipolar TRD label |
| Acute SI drop after one dose | Continue safety plan and structure | Same-day unrestricted discharge |
| Severe hypertension peri-dose | Medical protocol, hold further dosing | "Anxiety only" without BP check |
| New psychotic content | Pause, reassess primary psychosis/substance | Pushing dose through frank psychosis |
| True TRD pathways fail when pseudo-resistance is ignored.[9][21][22] |
Assessment before first dose
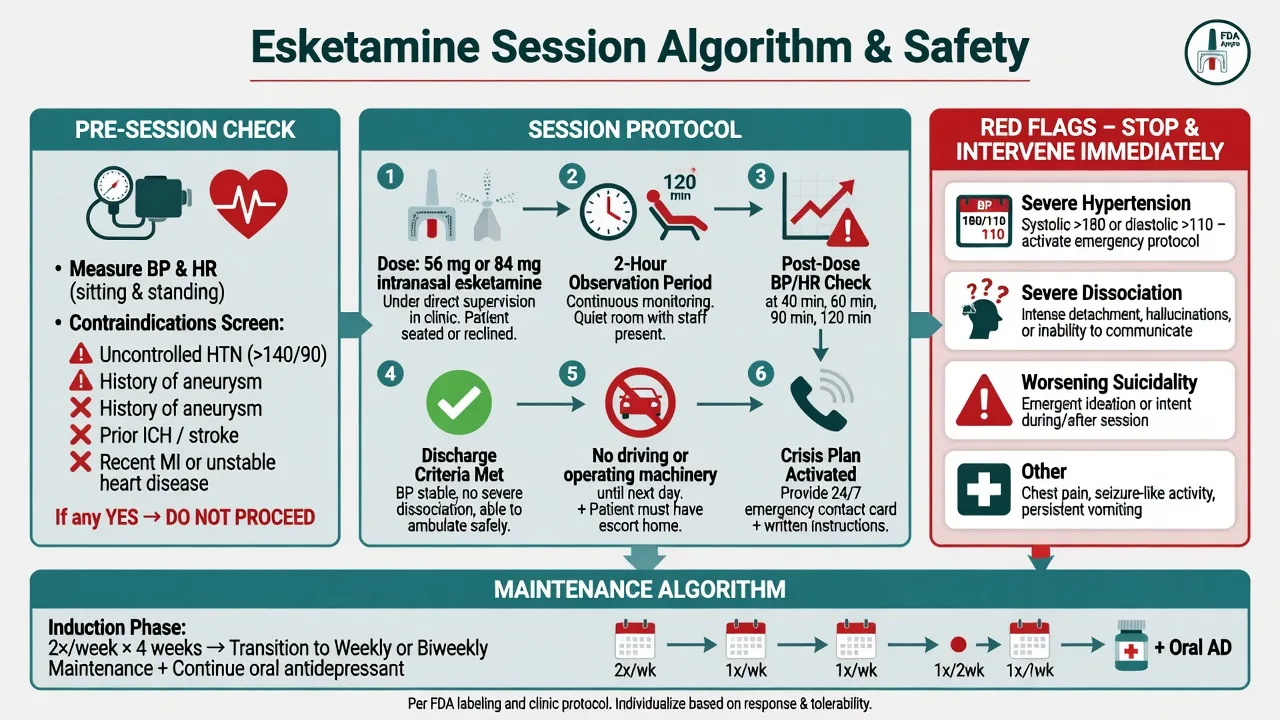
Document: confirmed MDD/TRD criteria and failed trials; bipolar and psychosis screen; full substance-use history (including non-medical ketamine); cardiovascular history (hypertension control, aneurysm, AVM, stroke/ICH); pregnancy status; current medicines; capacity and consent; baseline BP/HR; and whether the service can deliver supervised dosing and observation.[9][21][22]
Parallel suicide risk assessment is mandatory when treating high-risk depression: intent, plan, means, protective factors, collateral, and a written crisis plan that does not evaporate because a rapid-acting drug is on the medication chart.[11][12][19]
Investigations and monitoring
- Baseline: BP series, HR, weight; ECG if cardiac risk; urine drug screen when clinically indicated; pregnancy test when relevant.[9][22]
- Peri-dose: BP before dosing and after; observe for hypertensive urgency/emergency; watch sedation and dissociation severity.[10][22]
- No classic TDM level for antidepressant ketamine practice (unlike lithium or clozapine) — the "level" is the protocol and the observations.[9]
- Chronic exposure: urinary symptoms warrant assessment if misuse or very frequent dosing is suspected.[10][22]
Acute / session emergencies
Hypertensive crisis: stop further dosing that session, continuous monitoring, antihypertensives per clinic protocol, medical escalation if end-organ concern.[22]
Severe dissociation or agitation: quiet environment, reorientation, staff presence; benzodiazepines only within protocol; do not abandon observation early.[10][22]
Worsening suicidality or behavioural dysregulation: escalate containment and psychiatric intensity — a rapid-acting agent is an adjunct to risk management, not a substitute.[11][12][19][20]
Definitive management protocols
IV racemic ketamine (teaching scaffold)
Research-standard antidepressant protocol: racemic ketamine 0.5 mg/kg intravenous over approximately 40 minutes, with vital-sign monitoring during infusion and a post-infusion observation period defined by local protocol. Frequency varies (for example twice-weekly induction in some programmes, then spacing). This remains off-label for depression in many systems and requires institutional governance, informed consent, and resuscitation-ready settings appropriate to the dose and population.[2][3][9][16][21]
Murrough and colleagues used a midazolam-controlled design to reduce functional unblinding from dissociation while still showing antidepressant efficacy — cite this when examiners challenge "placebo and expectancy only."[3]
Intranasal esketamine (labelled pathway principles)
Adult dosing scaffold (product information is authority): common treatment doses 56 mg or 84 mg nasal under healthcare supervision; induction often twice weekly for four weeks, then weekly or every other week maintenance, always with a concurrent oral antidepressant in the TRD label paradigm. Patients remain under observation (commonly about two hours) with BP checks; they must not drive until the following day after dosing in labelled programmes.[13][14][15][21]
TRANSFORM-1 (fixed dose) and TRANSFORM-2 (flexible dose) established short-term TRD efficacy signals with oral AD; flexible-dose TRANSFORM-2 is the cleaner positive pivotal narrative candidates usually lead with.[13][14]
SUSTAIN-1 is the relapse-prevention exam pearl: after stabilisation, randomised continuation of esketamine plus oral AD delayed relapse versus switching to oral AD plus placebo nasal spray.[15]
SUSTAIN-2 supports longer-term safety/tolerability under open-label conditions with ongoing monitoring culture.[18]
Suicidal ideation populations
Canuso and the ASPIRE I/II programme tested esketamine nasal spray for rapid reduction of depressive symptoms in people with MDD and active suicidal ideation with intent, on a background of comprehensive standard of care. Expect rapid symptom signals; do not claim that a dose abolishes suicide risk or replaces admission decisions, means restriction, or follow-up intensity.[11][19][20]
Wilkinson and colleagues' individual participant data meta-analysis supports a rapid reduction in suicidal ideation after a single IV ketamine dose — again, as a time-limited signal within full risk care.[12]
Ketamine versus ECT
ELEKT-D (Anand et al., 2023): in nonpsychotic treatment-resistant major depression, IV ketamine was noninferior to ECT on the trial's primary response endpoint. Exam-safe reading: for nonpsychotic TRD, ketamine is a serious comparator; for psychotic depression, catatonia, or pregnancy with severe depression, ECT often remains preferred on clinical grounds outside that trial's population.[23][21]
Adverse-effect management
Prevention and management principles (Ceban/McIntyre group synthesis): screen BP risk, pretreat nausea when needed, set expectations about dissociation, use quiet low-stimulation rooms, protocolise BP thresholds, and plan for sedation recovery before discharge.[22][10]
Comparison board
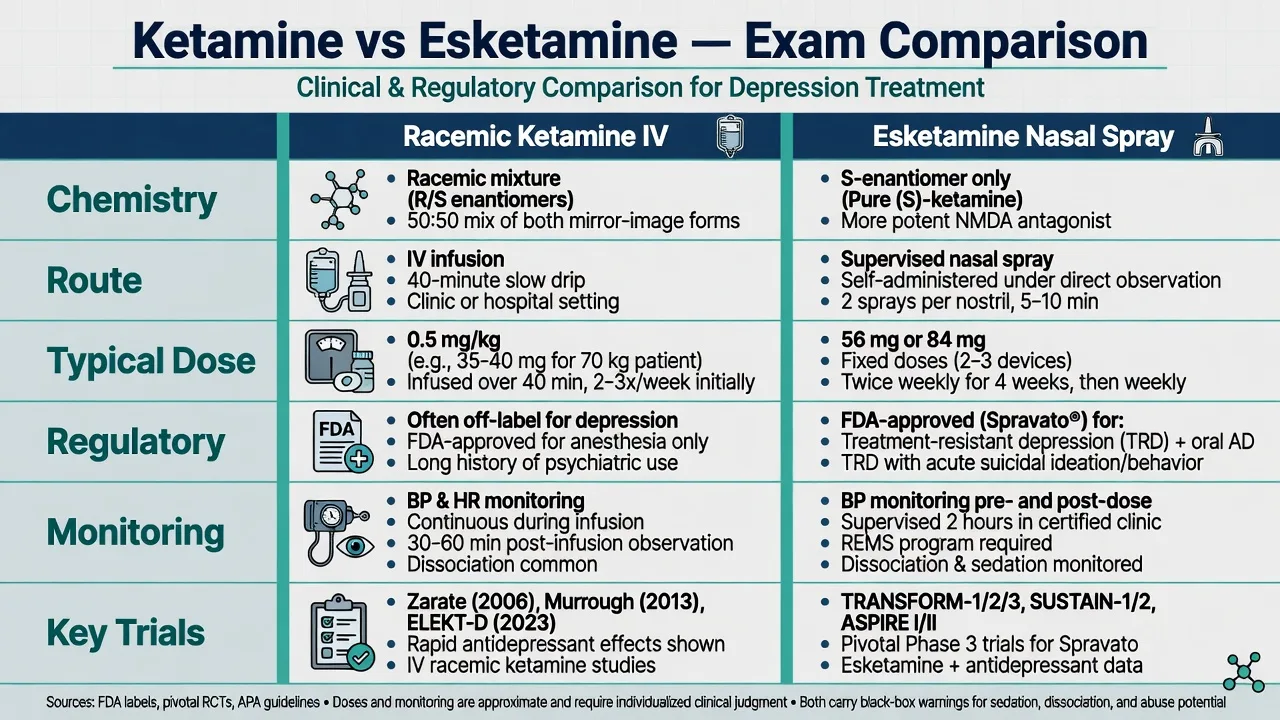
| Feature | Racemic ketamine (IV depression use) | Esketamine (IN) |
|---|---|---|
| Chemistry | R/S mixture | S-enantiomer |
| Typical research dose | 0.5 mg/kg IV over ~40 min | 56 or 84 mg nasal supervised |
| Regulatory for depression | Often off-label / local governance | Labelled TRD + oral AD; SI pathways where approved |
| Key trials | Berman, Zarate, Murrough, Phillips, ELEKT-D | TRANSFORM, SUSTAIN, ASPIRE, Canuso |
| Monitoring | Infusion obs, BP, mental state | ~2 h clinic obs, BP, REMS-style controls |
| This table is viva scaffolding — product labels and local protocols govern exact practice.[2][13][15][23] |
Special populations
Older adults. TRANSFORM-3 evaluated elderly TRD; results were more mixed than younger adult flexible-dose data — individualise, start carefully, watch BP, falls, and polypharmacy.[17]
Youth. Outside standard adult labelled pathways in most systems; research/specialist only with extreme caution.[21]
Pregnancy and lactation. Generally avoid ketamine/esketamine for depression; for severe perinatal TRD, ECT is often the preferred rapid somatic option after specialist perinatal discussion.[21]
Cardiovascular disease. Uncontrolled hypertension, aneurysmal vascular disease, AVM, and history of ICH are major barriers — treat as programme exclusions unless a highly specialised exception is explicitly justified.[22][21]
Substance use disorders. Higher diversion and relapse risk; clinic-only administration, urine monitoring when indicated, integrated dual-diagnosis care.[9][10]
Psychotic depression. Not the ELEKT-D population; favour ECT-led pathways.[23]
Prognosis and disposition
Responders often need a maintenance or booster strategy; abrupt stop after response risks relapse (SUSTAIN-1 logic). Disposition plans include supervised clinic slots, oral AD continuity, GP liaison, crisis contacts, driving advice, and occupational safety. Non-responders after adequate induction deserve reassessment of diagnosis, substances, and escalation to ECT or other advanced options rather than endless undirected infusions.[15][16][21][23]
Evidence, guidelines and regional differences
| Source | Exam take-home |
|---|---|
| Berman 2000 | First RCT antidepressant signal for ketamine |
| Zarate 2006 | IV ketamine in TRD; rapid robust effect |
| Murrough 2013 | Midazolam-controlled IV efficacy |
| Newport 2015 / Coyle 2015 | Early synthesis of NMDA antagonist trials |
| Sanacora 2017 | APA Council consensus on clinical ketamine use |
| Canuso 2018 / ASPIRE I–II | SI with intent populations; rapid symptom signals |
| TRANSFORM-1/2 | Short-term esketamine + oral AD in TRD |
| SUSTAIN-1 | Continuation prevents relapse |
| SUSTAIN-2 | Longer-term open-label safety culture |
| TRANSFORM-3 | Elderly — more cautious interpretation |
| McIntyre 2021 | International implementation expert opinion |
| ELEKT-D 2023 | IV ketamine noninferior to ECT in nonpsychotic TRD |
| Landmark synthesis for viva speed.[1][2][3][4][9][11][13][15][21][23] |
US: FDA-approved esketamine with REMS (certified centres, supervised administration, observation). Off-label IV racemic ketamine common in specialty clinics under variable governance. UK: NICE technology appraisals constrain NHS esketamine access; many candidates still need ECT literacy. ANZ: TGA registration and local funding/access rules evolve — do not invent current PBS line listings in a viva; state principles (specialist initiation, supervised dosing) and that access is jurisdiction- and time-specific. Europe: EMA pathway for esketamine with national implementation differences. Exact device strengths, observation minutes, and funding criteria are local product and payer rules — principles travel; numbers may not.[9][13][21]
Exam pearls
KETAMINE non-negotiables
KETAMINE
References
- [1]Berman RM, Cappiello A, Anand A, et al. Antidepressant effects of ketamine in depressed patients. Biol Psychiatry, 2000.PMID 10686270
- [2]Zarate CA Jr, Singh JB, Carlson PJ, et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry, 2006.PMID 16894061
- [3]Murrough JW, Iosifescu DV, Chang LC, et al. Antidepressant efficacy of ketamine in treatment-resistant major depression: a two-site randomized controlled trial. Am J Psychiatry, 2013.PMID 23982301
- [4]Newport DJ, Carpenter LL, McDonald WM, et al. Ketamine and Other NMDA Antagonists: Early Clinical Trials and Possible Mechanisms in Depression. Am J Psychiatry, 2015.PMID 26423481
- [5]Coyle CM, Laws KR The use of ketamine as an antidepressant: a systematic review and meta-analysis. Hum Psychopharmacol, 2015.PMID 25847818
- [6]Li N, Lee B, Liu RJ, et al. mTOR-dependent synapse formation underlies the rapid antidepressant effects of NMDA antagonists. Science, 2010.PMID 20724638
- [7]Zanos P, Moaddel R, Morris PJ, et al. NMDAR inhibition-independent antidepressant actions of ketamine metabolites. Nature, 2016.PMID 27144355
- [8]Singh JB, Fedgchin M, Daly E, et al. Intravenous Esketamine in Adult Treatment-Resistant Depression: A Double-Blind, Double-Randomization, Placebo-Controlled Study. Biol Psychiatry, 2016.PMID 26707087
- [9]Sanacora G, Frye MA, McDonald W, et al. A Consensus Statement on the Use of Ketamine in the Treatment of Mood Disorders. JAMA Psychiatry, 2017.PMID 28249076
- [10]Short B, Fong J, Galvez V, et al. Side-effects associated with ketamine use in depression: a systematic review. Lancet Psychiatry, 2018.PMID 28757132
- [11]Canuso CM, Singh JB, Fedgchin M, et al. Efficacy and Safety of Intranasal Esketamine for the Rapid Reduction of Symptoms of Depression and Suicidality in Patients at Imminent Risk for Suicide: Results of a Double-Blind, Randomized, Placebo-Controlled Study. Am J Psychiatry, 2018.PMID 29656663
- [12]Wilkinson ST, Ballard ED, Bloch MH, et al. The Effect of a Single Dose of Intravenous Ketamine on Suicidal Ideation: A Systematic Review and Individual Participant Data Meta-Analysis. Am J Psychiatry, 2018.PMID 28969441
- [13]Popova V, Daly EJ, Trivedi M, et al. Efficacy and Safety of Flexibly Dosed Esketamine Nasal Spray Combined With a Newly Initiated Oral Antidepressant in Treatment-Resistant Depression: A Randomized Double-Blind Active-Controlled Study. Am J Psychiatry, 2019.PMID 31109201
- [14]Fedgchin M, Trivedi M, Daly EJ, et al. Efficacy and Safety of Fixed-Dose Esketamine Nasal Spray Combined With a New Oral Antidepressant in Treatment-Resistant Depression: Results of a Randomized, Double-Blind, Active-Controlled Study (TRANSFORM-1). Int J Neuropsychopharmacol, 2019.PMID 31290965
- [15]Daly EJ, Trivedi MH, Janik A, et al. Efficacy of Esketamine Nasal Spray Plus Oral Antidepressant Treatment for Relapse Prevention in Patients With Treatment-Resistant Depression: A Randomized Clinical Trial. JAMA Psychiatry, 2019.PMID 31166571
- [16]Phillips JL, Norris S, Talbot J, et al. Single, Repeated, and Maintenance Ketamine Infusions for Treatment-Resistant Depression: A Randomized Controlled Trial. Am J Psychiatry, 2019.PMID 30922101
- [17]Ochs-Ross R, Daly EJ, Zhang Y, et al. Efficacy and Safety of Esketamine Nasal Spray Plus an Oral Antidepressant in Elderly Patients With Treatment-Resistant Depression-TRANSFORM-3. Am J Geriatr Psychiatry, 2020.PMID 31734084
- [18]Wajs E, Aluisio L, Holder R, et al. Esketamine Nasal Spray Plus Oral Antidepressant in Patients With Treatment-Resistant Depression: Assessment of Long-Term Safety in a Phase 3, Open-Label Study (SUSTAIN-2). J Clin Psychiatry, 2020.PMID 32316080
- [19]Fu DJ, Ionescu DF, Li X, et al. Esketamine Nasal Spray for Rapid Reduction of Major Depressive Disorder Symptoms in Patients Who Have Active Suicidal Ideation With Intent: Double-Blind, Randomized Study (ASPIRE I). J Clin Psychiatry, 2020.PMID 32412700
- [20]Ionescu DF, Fu DJ, Qiu X, et al. Esketamine Nasal Spray for Rapid Reduction of Depressive Symptoms in Patients With Major Depressive Disorder Who Have Active Suicide Ideation With Intent: Results of a Phase 3, Double-Blind, Randomized Study (ASPIRE II). Int J Neuropsychopharmacol, 2021.PMID 32861217
- [21]McIntyre RS, Rosenblat JD, Nemeroff CB, et al. Synthesizing the Evidence for Ketamine and Esketamine in Treatment-Resistant Depression: An International Expert Opinion on the Available Evidence and Implementation. Am J Psychiatry, 2021.PMID 33726522
- [22]Ceban F, Rosenblat JD, Kratiuk K, et al. Prevention and Management of Common Adverse Effects of Ketamine and Esketamine in Patients with Mood Disorders. CNS Drugs, 2021.PMID 34363603
- [23]Anand A, Mathew SJ, Sanacora G, et al. Ketamine versus ECT for Nonpsychotic Treatment-Resistant Major Depression. N Engl J Med, 2023.PMID 37224232