Psych · Psychopharmacology — lamotrigine
Lamotrigine
Also known as Lamictal · LTG · Lamotrigine bipolar · Lamotrigine titration · Lamotrigine SJS
Exam-exhaustive fellowship monograph on lamotrigine — depression-pole maintenance evidence (Calabrese, Bowden, Goodwin pooled, Geddes meta), slow titration schedules, SJS/TEN/DRESS stop rules, valproate and combined oral contraceptive pharmacokinetic interactions, pregnancy hierarchy, CANMAT/ISBD positioning. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
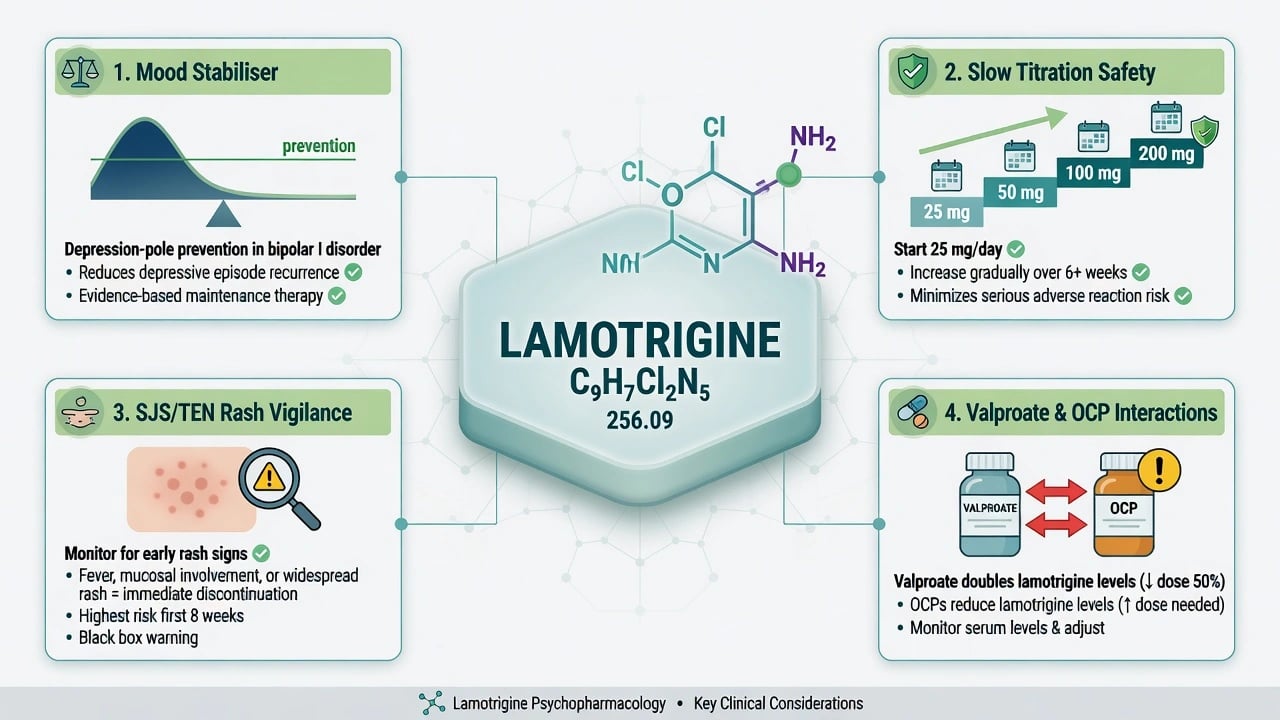
Lamotrigine is a high-yield fellowship psychopharmacology station because examiners test polarity matching, titration discipline, and interaction literacy in one stem. Landmark maintenance trials and pooled analyses show relatively stronger protection against depressive recurrence than against mania; rash-safety science and product dosing tables exist because rapid escalation and valproate co-therapy amplify serious cutaneous risk; oestrogen-containing contraceptives induce clearance and can unmask relapse if you ignore them.[2][3][4][8][9][10][11][12]
Definition and place in treatment
Lamotrigine is a phenyltriazine anticonvulsant used as a mood stabiliser. The working mechanism narrative is use-dependent voltage-gated sodium channel blockade with reduced excitatory (glutamate) release — enough mechanism for viva, not a licence to invent pathways.[7]
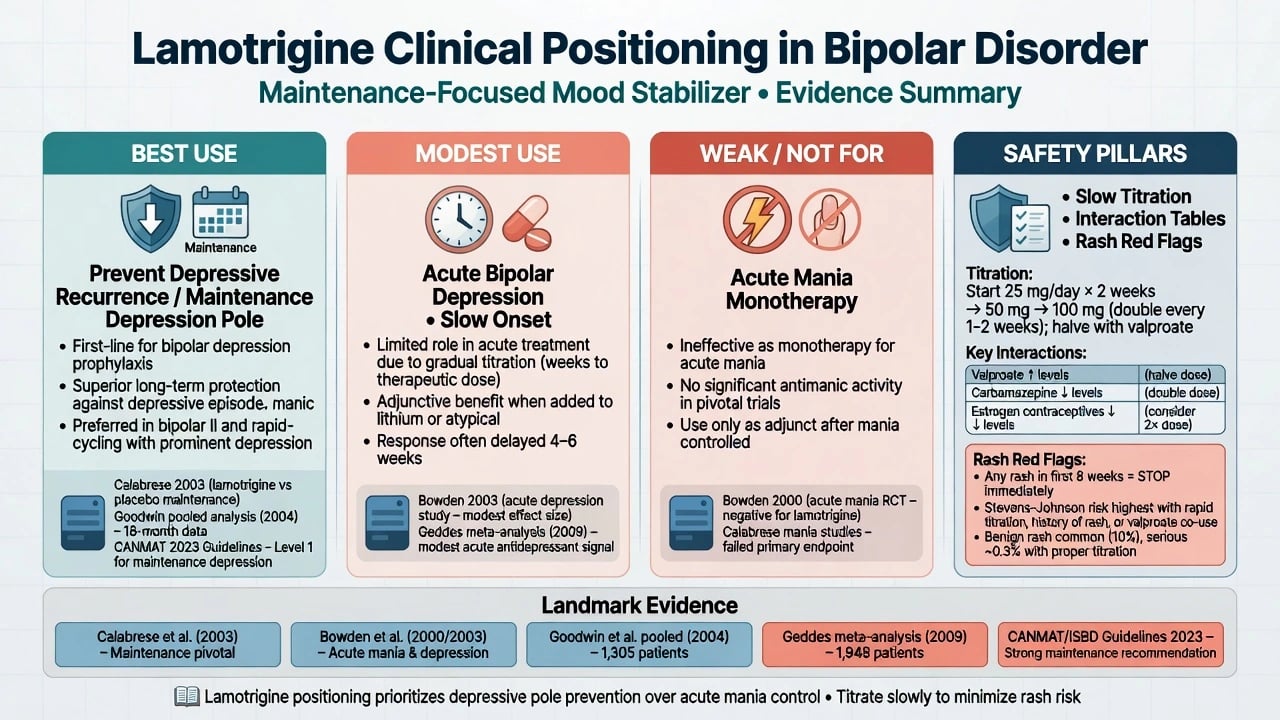
Psychiatric positioning examiners expect (Goodwin pooled polarity, modest acute depression signal, weak acute antimanic role):
| Role | Exam-safe stance |
|---|---|
| Bipolar I maintenance | Strongest LTG signal is delaying depressive recurrence (Goodwin pooled polarity message) |
| Acute bipolar depression | Modest effect, slow because of titration; not a rescue antidepressant |
| Acute mania | Weak / not monotherapy — stabilise mania with lithium, valproate or an antipsychotic first |
| Epilepsy | Origin of rash and interaction science still governing psychiatric prescribing |
| Polarity table anchors Goodwin pooled maintenance teaching, modest acute depression meta-signal, and weak acute antimanic role.[4][5][6][7] |
CANMAT/ISBD 2018 places lamotrigine within evidence-based bipolar algorithms for depression-pole and maintenance roles — cite guideline families rather than inventing local formulary ranks as universal law.[4][5][6][15]
Epidemiology and risk of harm
Serious cutaneous adverse reactions (SCARs) — SJS/TEN and related severe phenotypes — are rare but exam-defining. EuroSCAR-type pharmacoepidemiology lists lamotrigine among drugs with elevated SJS/TEN risk relative to background; risk concentrates early in treatment and rises with unsafe dosing patterns.[8][14]
Risk amplifiers you must name without prompting: high starting dose or rapid titration; valproate co-therapy without a slower schedule (valproate inhibits LTG clearance); younger age (historical paediatric rash signal higher); re-starting after a gap at previous maintenance dose without re-titration.[8][9][10]
Common benign rash is more frequent than SJS; the exam skill is not promising zero rash — it is discriminating stop-now features from watchful management and defaulting to safety when uncertain.[8][9]
Pathophysiology and pharmacokinetics
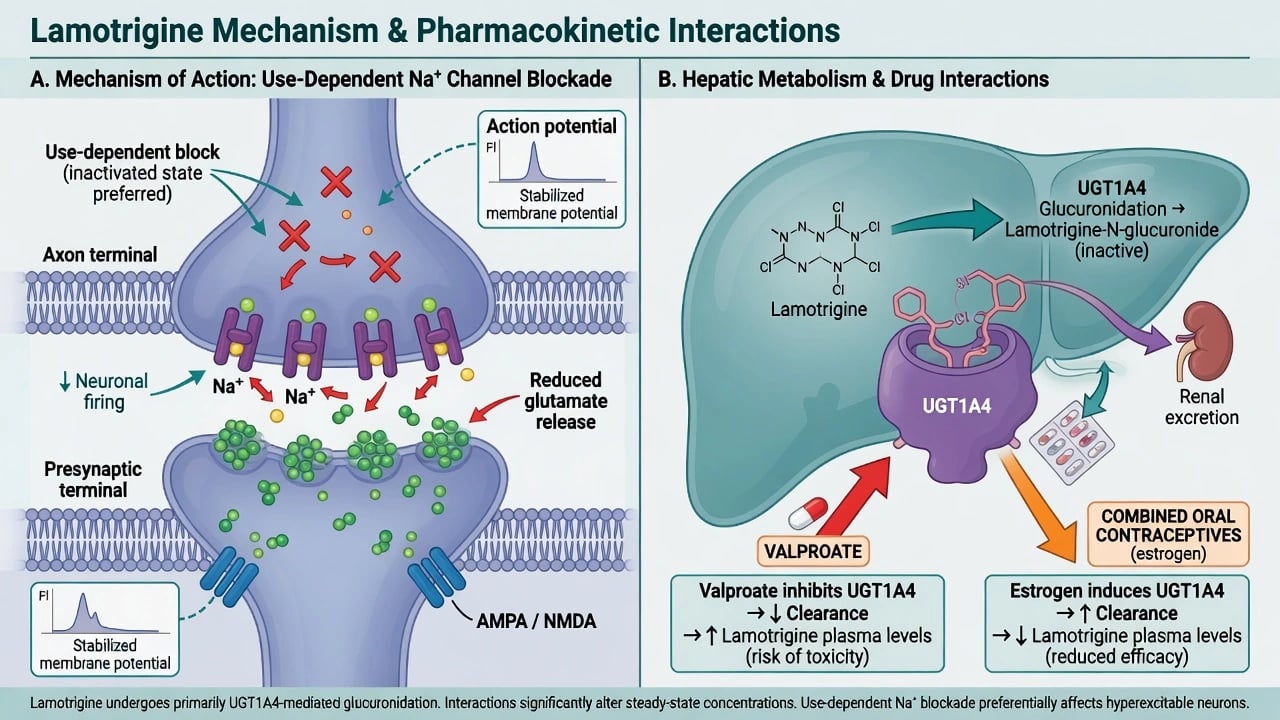
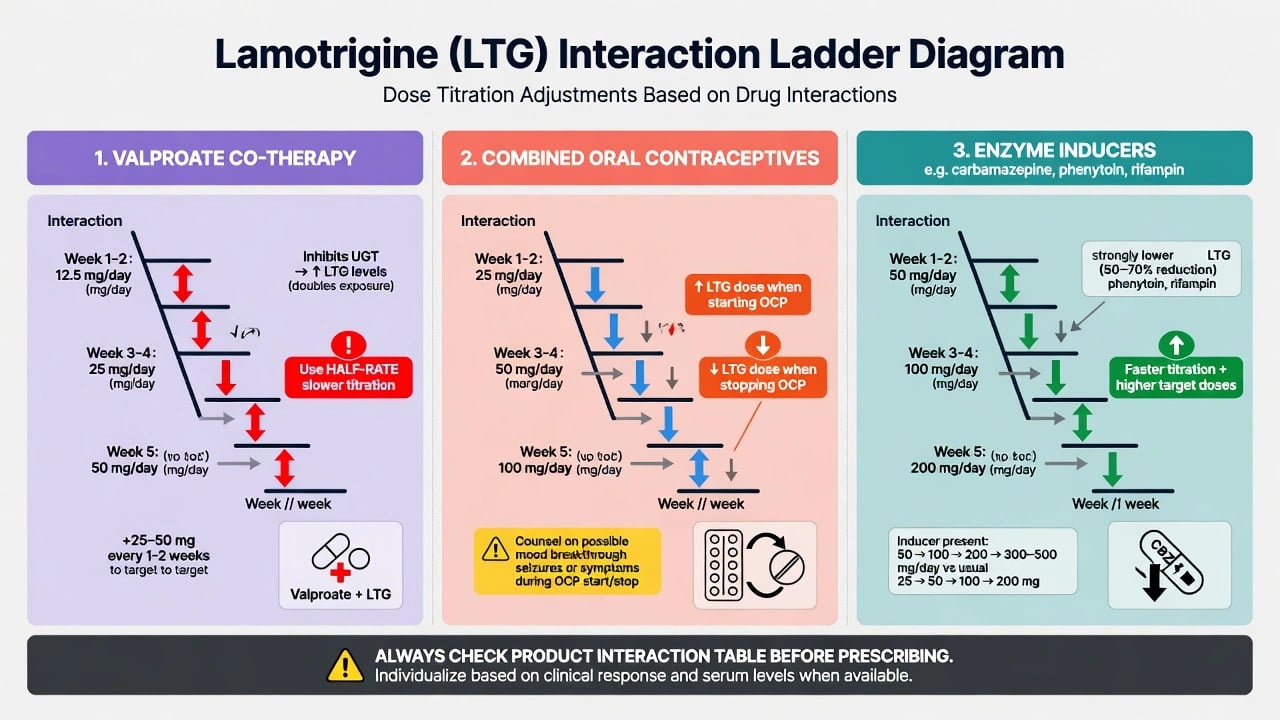
Hepatic glucuronidation (UGT1A4) is the main clearance pathway. That single fact structures three exam interactions. Valproate inhibits lamotrigine metabolism → higher LTG exposure → slower/lower titration mandatory.[10] Combined oral contraceptives (ethinylestradiol) induce lamotrigine clearance → lower LTG levels → dose increase may be needed when OCPs start; dose reduction when OCPs stop to avoid toxicity.[11][12][13] Enzyme-inducing AEDs (for example carbamazepine or phenytoin) lower LTG levels → product tables use a faster/higher schedule.[9]
Hypersensitivity is delayed T-cell mediated across a spectrum from morbilliform eruption to SJS/TEN and DRESS; titration rate is a modifiable risk factor embedded in labelled schedules.[8][9][14]
Clinical effects and time course
Expect weeks, not days, for meaningful mood benefit — titration itself delays target exposure. Maintenance benefit is about time to recurrence, not rapid symptom wipe-out. Spectrum data and acute depression packages show activity weighted toward depression; do not oversell acute mania efficacy.[1][5][6][7]
Common tolerability: headache, dizziness, nausea, insomnia, benign rash, blurred vision. Danger signals: progressive widespread rash, facial swelling, mucosal erosions (mouth, eyes, genitals), blistering, fever, lymphadenopathy, hepatitis — treat as SCAR until proven otherwise.[8][14]
Numbers and anchors every candidate owns
Anchors above are teaching scaffolds from product-aligned titration culture, PK studies and landmark maintenance synthesis — always re-check local product information for exact schedules.[4][9][10][11]
Differential diagnosis that saves skin and polarity
| Presentation | Prefer | Do not miss |
|---|---|---|
| Early rash + mucosa/systemic signs | SJS/TEN — stop LTG, hospitalise | "Benign drug rash, continue" |
| Fever, rash, eosinophilia, organ injury | DRESS — stop LTG | Treating as viral illness alone |
| Breakthrough depression after starting OCP | Level drop from induced clearance | Automatic antidepressant add without checking PK |
| Acute mania on LTG monotherapy | Wrong tool — need antimanic cover | Pushing LTG dose as if it were lithium |
| Worsening symptoms after stopping OCP | Rising LTG level / toxicity or mood instability | Ignoring the stop-OCP interaction |
| Rash, polarity and OCP-related level shifts are the differentials that separate safe LTG practice from missed SCARs and false "non-response."[4][8][11][12][14] |
Polarity and pharmacokinetics explain more "failures" than non-adherence alone.[4][8][11][12]
Assessment before and during treatment
Pre-start checklist: confirm depression-pole / maintenance indication; document why not lithium if suicide risk is prominent (lithium retains a separate anti-suicide discussion); exclude or stabilise acute mania before relying on LTG; pregnancy test when relevant with a contraception plan (method type matters); full medication list including valproate, enzyme inducers and oestrogen contraceptives; prior severe AED rash history; written rash red-flag card and slow-titration plan the patient can recite.[4][8][9][15]
On treatment: review after each titration step early on; inspect any reported rash the same day if possible; re-check interactions whenever partners change (new valproate, new OCP — smoking is not the CYP1A2 story here; do not import clozapine logic).[8][9][15]
Investigations
Routine psychiatric starts do not require weekly bloods like clozapine. Useful tests include pregnancy testing as indicated; baseline LFTs/FBC when comorbidity or polypharmacy warrants; plasma lamotrigine in selected scenarios such as pregnancy (clearance rises), OCP start/stop, complex polytherapy, suspected non-adherence or dual epilepsy care — not as a universal mandatory level; and clinical-first SCAR work-up with labs supporting organ involvement assessment.[8][11][17]
Do not invent a "lamotrigine registry" equivalent to clozapine REMS — the safety system is titration + education + stop rules.[8][9][11]
Titration — the core exam skill
Adult monotherapy teaching scaffold
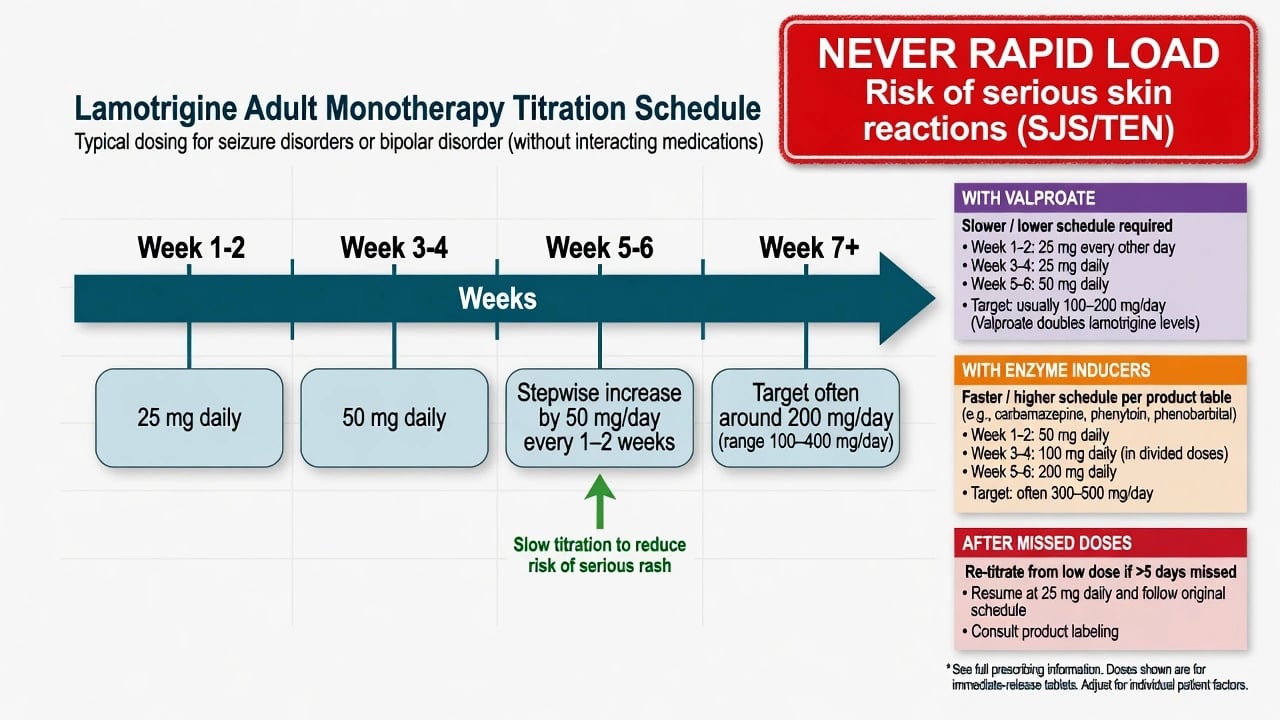
Always verify the current local product information. A classic adult monotherapy skeleton used in exam teaching is 25 mg orally daily for 2 weeks, then 50 mg orally daily for 2 weeks, then stepwise increases (commonly by 50 mg/day every 1–2 weeks) toward a target often around 200 mg/day (range individualised; some need more or less).[8][9]
That scaffold is a safety protocol, not a suggestion. Exceeding recommended escalation is how stems become SJS cases.[8][9]
With valproate
Valproate acutely inhibits lamotrigine metabolism, raising LTG concentrations. Use the valproate co-therapy table: lower starting doses and slower escalation (classically taught as roughly half-rate / lower targets — exact steps are product-table territory). Classic fail: start 25 mg daily on valproate as if monotherapy.[9][10]
With enzyme inducers
Carbamazepine and similar inducers lower LTG levels; labelled schedules use higher/faster steps. Re-titrate if the inducer is added or withdrawn later.[9]
Missed doses and restarts
Multi-day interruptions generally require re-titration from a low dose rather than slamming back to maintenance — follow product guidance for the gap duration. This is a frequent MCQ trap after hospital leave or non-adherence.[9]
Serious rash, SJS/TEN and DRESS — emergency management
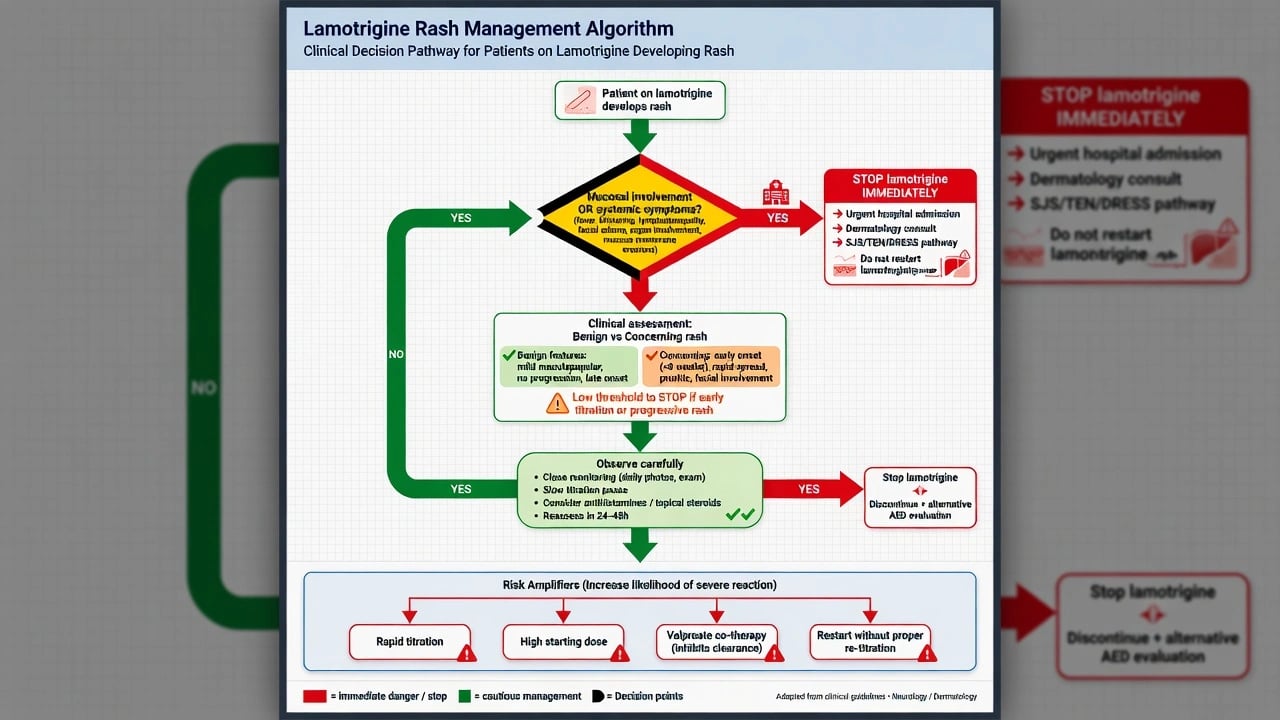
Immediate actions for concerning rash: stop lamotrigine the same day (do not taper a SCAR drug); urgent clinical assessment for mucosal involvement, blistering, skin pain and fever; hospital / dermatology / burn-unit pathway for suspected SJS/TEN; supportive care; avoid rechallenge after confirmed SJS/TEN; document and alert future records.[8][14]
DRESS presents later with fever, rash, internal organ involvement and haematologic abnormalities — still stop the drug and escalate. EuroSCAR risk assessment frames LTG as a relevant SCAR-associated medicine; Guberman and Messenheimer dosing papers exist to prevent that path.[8][9][14]
Definitive management and interactions
Valproate–lamotrigine
PK fact: sodium valproate inhibits LTG metabolism. Clinical rule: different titration table. When both are needed (e.g. mania cover with VPA plus depression-pole LTG), write the slow schedule explicitly and educate about rash.[10][9]
Combined oral contraceptives
Observational and experimental data show combined OCPs reduce lamotrigine plasma levels; ethinylestradiol induction of glucuronidation is the mechanism teaching point. When starting a combined OCP on stable LTG, expect lower levels — monitor mood/seizures and consider dose increase per clinical or TDM judgement. When stopping a combined OCP, levels rise — consider dose reduction to avoid toxicity. LTG does not behave like carbamazepine for contraceptive failure via CYP3A4 induction — do not mix the two contraceptive lectures, but still counsel comprehensive contraception choices. Sidhu, Sabers and Christensen provide the PK backbone examiners recognise.[11][12][13]
Other management points
Maintenance: continue when effective; pair with antimanic agents if mania risk remains high (lithium, selected antipsychotics, or valproate with interaction care).[4][15] Acute bipolar depression: modest benefit on meta-analysis of five RCTs; set expectations for slow onset; do not abandon after three under-dosed days.[5][6] Add-on strategies: combination with other mood stabilisers is common; always re-check the LTG table when partners change.[9][10]
Special populations
Pregnancy. EURAP comparative malformation data place lamotrigine more favourably than valproate (and generally better than several older AEDs), but risk is not zero and is dose-relevant in AED counselling culture. Clearance often rises in pregnancy (levels fall) and falls postpartum (toxicity risk if dose not reduced). Coordinate perinatal psychiatry and, when dual indication, neurology. NEAD cognitive data highlight valproate's worse neurodevelopmental profile — part of why LTG is often preferred among classic anticonvulsants when an AED-mood stabiliser is needed, still with shared decision.[17][18]
Lactation. Individualise with specialist sources; do not invent milk ratios in the exam room.[17]
Children and adolescents. Higher historical rash concern — adhere to paediatric schedules strictly; psychiatry use is specialist.[8][9]
Older adults. Dizziness/falls, polypharmacy, slower titration, renal/hepatic frailty.[9][15]
Intellectual disability / dual epilepsy–mood care. One unified interaction and rash plan across teams.[8][15][17]
Prognosis and disposition
Goodwin pooled analysis of the two 18-month maintenance RCTs is the polarity teaching classic: lamotrigine delayed mood episode recurrence with relatively greater effect on depressive poles, lithium relatively stronger on manic poles in that synthesis — modern practice still individualises combination therapy when both poles threaten.[2][3][4][16]
Disposition: written titration plan, red-flag card, pharmacy alignment on interaction table, early review during escalation, and long-term follow-up focused on polarity breakthrough and contraception changes.[4][8][11][15]
Evidence, guidelines and regional notes
| Source | Exam take-home |
|---|---|
| Calabrese 602 (1999) | Acute bipolar I depression monotherapy signal |
| Bowden 2003 / Calabrese 2003 | 18-month maintenance RCTs after mania or depression |
| Goodwin pooled 2004 | Depression-pole vs mania-pole differential vs lithium |
| Calabrese 2008 five trials + Geddes 2009 meta | Modest acute bipolar depression effect size |
| Spectrum 1999 | Activity across refractory bipolar presentations |
| Guberman / Messenheimer | Rash risk–benefit and dosing discipline |
| Yuen 1992 | Valproate inhibits LTG metabolism |
| Sabers / Christensen / Sidhu | OCP–LTG PK |
| Mockenhaupt EuroSCAR | SJS/TEN medication risk context |
| Miura 2014 NMA | Maintenance comparative landscape |
| CANMAT/ISBD 2018 | Guideline positioning |
| EURAP / NEAD | Pregnancy malformation and cognitive hierarchy |
| Landmark map for viva speed.[1][2][3][4][5][6][8][10][11][14][15][16][17] |
ANZ: bipolar care aligns with RANZCP-informed practice and product information; perinatal services emphasise valproate avoidance and LTG as a relative AED option with level-aware pregnancy care. UK: NICE bipolar guidance principles favour evidence-based mood stabilisers with safety counselling; product SPCs drive titration tables. US: APA bipolar practice and FDA labelling (boxed rash warning culture) stress slow titration. Europe: EuroSCAR pharmacovigilance culture and EURAP pregnancy data strongly influence counselling. Exact tablet strengths and co-therapy tables are local product rules — principles travel.[8][14][15][17]
Exam pearls
LAMOTRIGINE safety spine
LAMOTRIGINE
Note: mnemonic letters compress "I" twice as indication teaching — say the full prose in viva, not the crossword.[4][8][10][11]
Lamotrigine
- Depression-pole prevention
- Slow titration / rash rules
- VPA raises levels
- OCP lowers levels
Lithium
- Dual-pole maintenance
- Anti-suicide signal
- 12 h trough levels
- Toxicity pathway
Valproate
- Acute mania / mixed
- Pregnancy hierarchy avoid
- Inhibits LTG clearance
- LFT/FBC/weight monitor
Polarity and safety decide the prescription — not habit.[4][10][15][17]
References
- [1]Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group J Clin Psychiatry, 1999.PMID 10084633
- [2]Bowden CL, Calabrese JR, Sachs G, et al. A placebo-controlled 18-month trial of lamotrigine and lithium maintenance treatment in recently manic or hypomanic patients with bipolar I disorder Arch Gen Psychiatry, 2003.PMID 12695317
- [3]Calabrese JR, Bowden CL, Sachs G, et al. A placebo-controlled 18-month trial of lamotrigine and lithium maintenance treatment in recently depressed patients with bipolar I disorder J Clin Psychiatry, 2003.PMID 14628976
- [4]Goodwin GM, Bowden CL, Calabrese JR, et al. A pooled analysis of 2 placebo-controlled 18-month trials of lamotrigine and lithium maintenance in bipolar I disorder J Clin Psychiatry, 2004.PMID 15096085
- [5]Calabrese JR, Huffman RF, White RL, et al. Lamotrigine in the acute treatment of bipolar depression: results of five double-blind, placebo-controlled clinical trials Bipolar Disord, 2008.PMID 18271912
- [6]Geddes JR, Calabrese JR, Goodwin GM Lamotrigine for treatment of bipolar depression: independent meta-analysis and meta-regression of individual patient data from five randomised trials Br J Psychiatry, 2009.PMID 19118318
- [7]Calabrese JR, Bowden CL, McElroy SL, et al. Spectrum of activity of lamotrigine in treatment-refractory bipolar disorder Am J Psychiatry, 1999.PMID 10401445
- [8]Guberman AH, Besag FM, Brodie MJ, et al. Lamotrigine-associated rash: risk/benefit considerations in adults and children Epilepsia, 1999.PMID 10403224
- [9]Messenheimer JA, Guberman AH Rash with lamotrigine: dosing guidelines Epilepsia, 2000.PMID 10756418
- [10]Yuen AW, Land G, Weatherley BC, et al. Sodium valproate acutely inhibits lamotrigine metabolism Br J Clin Pharmacol, 1992.PMID 1524964
- [11]Sabers A, Ohman I, Christensen J, et al. Oral contraceptives reduce lamotrigine plasma levels Neurology, 2003.PMID 12939444
- [12]Christensen J, Petrenaite V, Atterman J, et al. Oral contraceptives induce lamotrigine metabolism: evidence from a double-blind, placebo-controlled trial Epilepsia, 2007.PMID 17346247
- [13]Sidhu J, Job S, Singh S, et al. The pharmacokinetic and pharmacodynamic consequences of the co-administration of lamotrigine and a combined oral contraceptive in healthy female subjects Br J Clin Pharmacol, 2006.PMID 16433873
- [14]Mockenhaupt M, Viboud C, Dunant A, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: assessment of medication risks with emphasis on recently marketed drugs. The EuroSCAR-study J Invest Dermatol, 2008.PMID 17805350
- [15]Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder Bipolar Disord, 2018.PMID 29536616
- [16]Miura T, Noma H, Furukawa TA, et al. Comparative efficacy and tolerability of pharmacological treatments in the maintenance treatment of bipolar disorder: a systematic review and network meta-analysis Lancet Psychiatry, 2014.PMID 26360999
- [17]Tomson T, Battino D, Bonizzoni E, et al. Comparative risk of major congenital malformations with eight different antiepileptic drugs: a prospective cohort study of the EURAP registry Lancet Neurol, 2018.PMID 29680205
- [18]Meador KJ, Baker GA, Browning N, et al. Cognitive function at 3 years of age after fetal exposure to antiepileptic drugs N Engl J Med, 2009.PMID 19369666