Psych · Psychopharmacology — lithium
Lithium
Also known as Lithium carbonate · Lithium citrate · Li+ mood stabiliser · Lithium monitoring · Lithium TDM
Exam-exhaustive fellowship monograph on lithium — initiation and 12-hour trough levels, acute mania and bipolar maintenance evidence (BALANCE, Geddes, Severus), anti-suicide efficacy (Cipriani), renal/thyroid/parathyroid monitoring (McKnight, Shine, Kessing), toxicity and EXTRIP, interaction ladder, pregnancy (Patorno, Munk-Olsen), special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Lithium remains a high-stakes fellowship monograph because examiners test efficacy discipline, level literacy, organ monitoring, and toxicity recognition in the same station. Long-term RCTs and meta-analyses support prophylaxis; BALANCE defends lithium against valproate monotherapy for relapse prevention; Cipriani meta-analysis supports suicide and mortality reduction; McKnight and Shine define the organ-toxicity profile that monitoring exists to catch.[1][2][3][5][6][7]
Definition and place in treatment
Lithium is a monovalent cation formulated as carbonate or citrate salts. It is not an anticonvulsant and not an antipsychotic; it is the reference mood stabiliser for bipolar disorder with unique population-level anti-suicide evidence among mood-disorder pharmacotherapies.[5][14]
Core indications examiners expect you to name: (1) acute mania (often with or after an antipsychotic/benzodiazepine for speed); (2) long-term prophylaxis of bipolar I (and many bipolar II pathways) as first-line maintenance in major guidelines; (3) high suicide-risk mood disorders where lithium is chosen for its anti-suicide signal as well as mood stability; (4) selected augmentation niches (including some treatment-resistant depression pathways) only with specialist framing — do not invent licence language.[1][3][4][5][14]
Guideline synthesis (Malhi and colleagues) consistently places lithium as a first-line long-term agent when monitoring infrastructure and patient suitability allow — under-use is a system problem, not proof of inferiority.[14]
Epidemiology, under-use and the risk–benefit paradox
Efficacy. Geddes 2004 meta-analysis showed long-term lithium reduces relapse versus placebo, with a clear anti-manic prophylactic effect and a less certain but still clinically used anti-depressive prophylactic role. Severus updated maintenance evidence and again supported lithium for prevention of mood episodes.[1][3]
BALANCE (2010). Open-label randomised trial in bipolar I: lithium monotherapy and lithium–valproate combination both outperformed valproate monotherapy for prevention of any mood episode. Exam one-liner: do not default to valproate alone as if it were lithium-equivalent for prophylaxis.[2]
Acute mania. Cipriani multiple-treatments meta-analysis places several antipsychotics ahead of lithium for short-term antimanic efficacy and acceptability, while lithium remains effective — so modern practice often combines speed (SGA) with lithium initiation for longer-term planning.[4]
Suicide. Cipriani 2013 updated meta-analysis of RCTs found lithium superior to placebo for reducing suicides and deaths from any cause in mood disorders. This is the anti-suicide pharmacotherapy pearl every viva expects — still embedded in a full risk plan, not a magic shield.[5]
Organ risk. McKnight systematic review/meta-analysis associates lithium with reduced urinary concentrating ability, hypothyroidism, hyperparathyroidism, and weight gain; absolute risk of end-stage renal disease was small in the synthesised data. Shine laboratory cohort work links long-term lithium with renal function decline, hypothyroidism, and hypercalcaemia. Kessing nationwide data associate modern lithium (and anticonvulsant) care with higher CKD rates — interpret with confounding by bipolar illness and age, but do not dismiss monitoring.[6][7][8]
Numbers every candidate must own
Level bands above are teaching scaffolds from TDM culture and product guidance — always individualise by age, renal function, tolerability and clinical phase.[6][12][13]
Pathophysiology and mechanism map
Teaching models emphasise GSK-3β inhibition and inositol monophosphatase (IMPase) pathway effects as intracellular candidates for mood-stabilising action — examiners want mechanism fluency without pretending any single pathway is fully explanatory.[12][14]
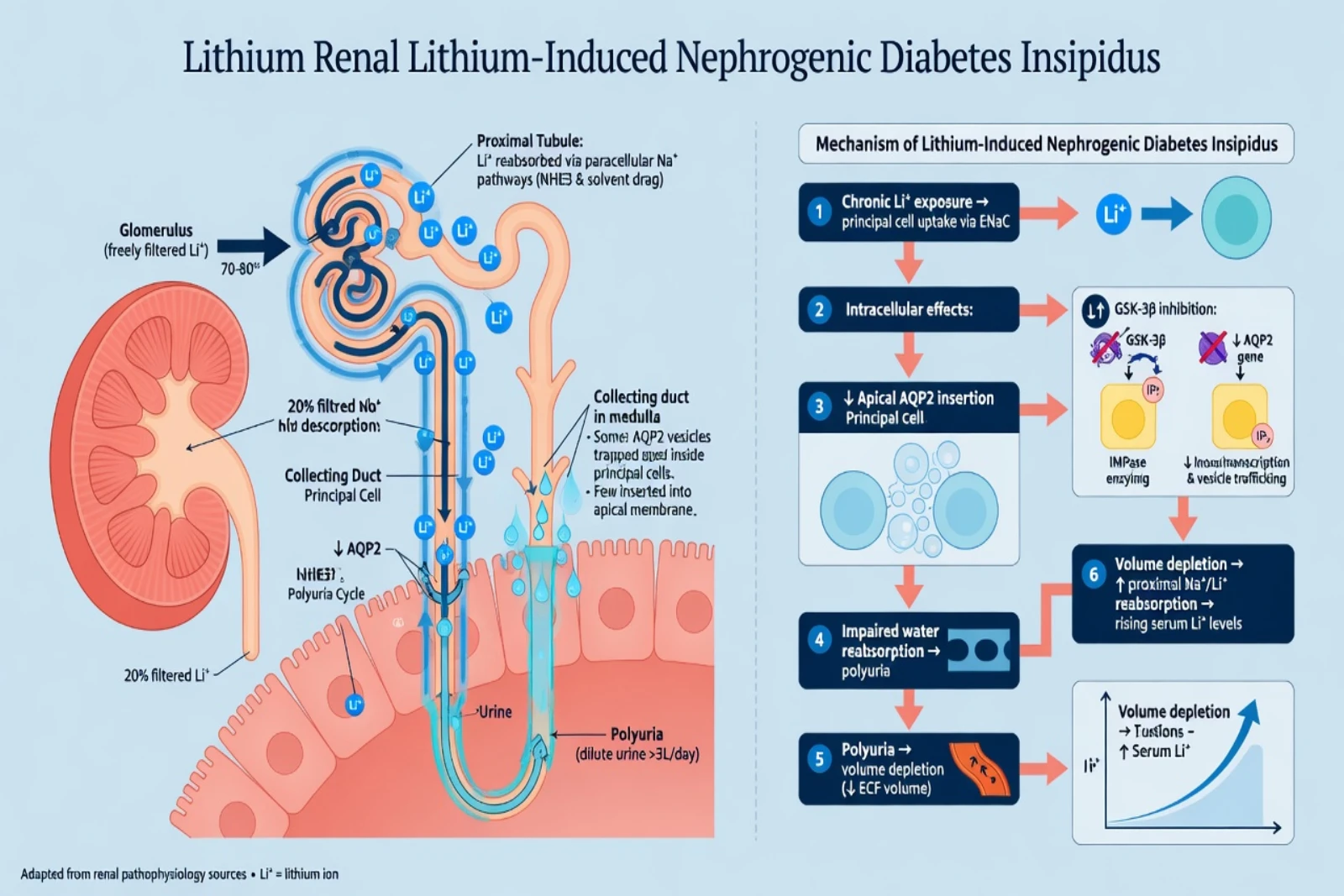
Renal handling. Lithium is freely filtered and largely reabsorbed proximally via sodium-related transporters. Volume depletion, low effective circulating volume, and drugs that increase proximal sodium reabsorption (classically thiazides; also ACE inhibitors/ARBs and NSAIDs via altered renal haemodynamics) raise lithium retention. Collecting-duct downregulation of aquaporin-2 pathways produces nephrogenic diabetes insipidus (NDI) — polyuria and polydipsia that can worsen volume depletion and feed a toxicity cycle.[6][11][12]
Thyroid and parathyroid. Lithium interferes with thyroid hormone release/synthesis pathways, raising hypothyroidism and goitre risk; hyperparathyroidism with hypercalcaemia is part of the McKnight/Shine organ profile and is why calcium monitoring sits beside TFT and eGFR.[6][7]
Neurotoxicity lag. Brain lithium kinetics lag serum — clinical neurotoxicity can persist or worsen as serum falls, and severe poisoning can leave lasting cerebellar/neurocognitive injury (SILENT spectrum teaching). Treat the patient and the trend, not a single mmol/L printout.[11][12]
Clinical effects and adverse-effect map
Common early effects: fine postural tremor, nausea, loose stools, polyuria/polydipsia, mild subjective cognitive dulling, weight gain. Most are dose/level related and manageable; they drive non-adherence if ignored.[6][12]
Hypothyroidism may be subclinical (TSH rise) or overt; treat with levothyroxine when indicated — successful lithium does not automatically require discontinuation for thyroid change alone.[6][7][12]
Toxicity phenotype (exam ladder): GI upset early (especially acute overdose) → coarse tremor, hyperreflexia, ataxia, dysarthria, nystagmus, confusion, myoclonus, seizures, coma. Chronic toxicity is often neuro-dominant with only modestly elevated serum levels and high tissue burden.[11][12]
Differentials that save lives
| Presentation on lithium | Prefer | Do not miss |
|---|---|---|
| New coarse tremor + ataxia | Toxicity work-up; stop lithium | "Just anxiety tremor" without level |
| Polyuria/polydipsia | NDI assessment; levels; fluids advice | Ignoring rising creatinine and levels |
| Delirium in older adult | Chronic toxicity + renal panel | Pure psychiatric decompensation only |
| Rising TSH | Thyroid replacement plan | Automatic lifelong lithium stop |
| First-trimester pregnancy | Perinatal risk–benefit with Patorno/Munk-Olsen framing | Panic cessation without relapse plan |
| Toxicity is a clinical diagnosis supported by levels — not a lab cut-off in isolation.[6][9][10][11][12] |
Pre-start assessment and consent
Before first dose, document: confirmed indication; capacity/consent or legal framework; suicide and self-harm risk; pregnancy intent and contraception when relevant; full medication list including OTC NSAIDs; alcohol/substance use; baseline renal function (U&E, creatinine/eGFR), TFT, calcium, weight/BMI; ECG if older or cardiac risk; and whether the service can deliver serial levels and organ bloods.[12][13][14]
Consent language must cover narrow therapeutic index, monitoring burden, sick-day rules (stop and seek advice if severe vomiting/diarrhoea/dehydration per local protocol), interaction drugs, and toxicity red flags — not a one-line "bloods sometimes."[12][14]
Investigations and therapeutic drug monitoring
How to take a level
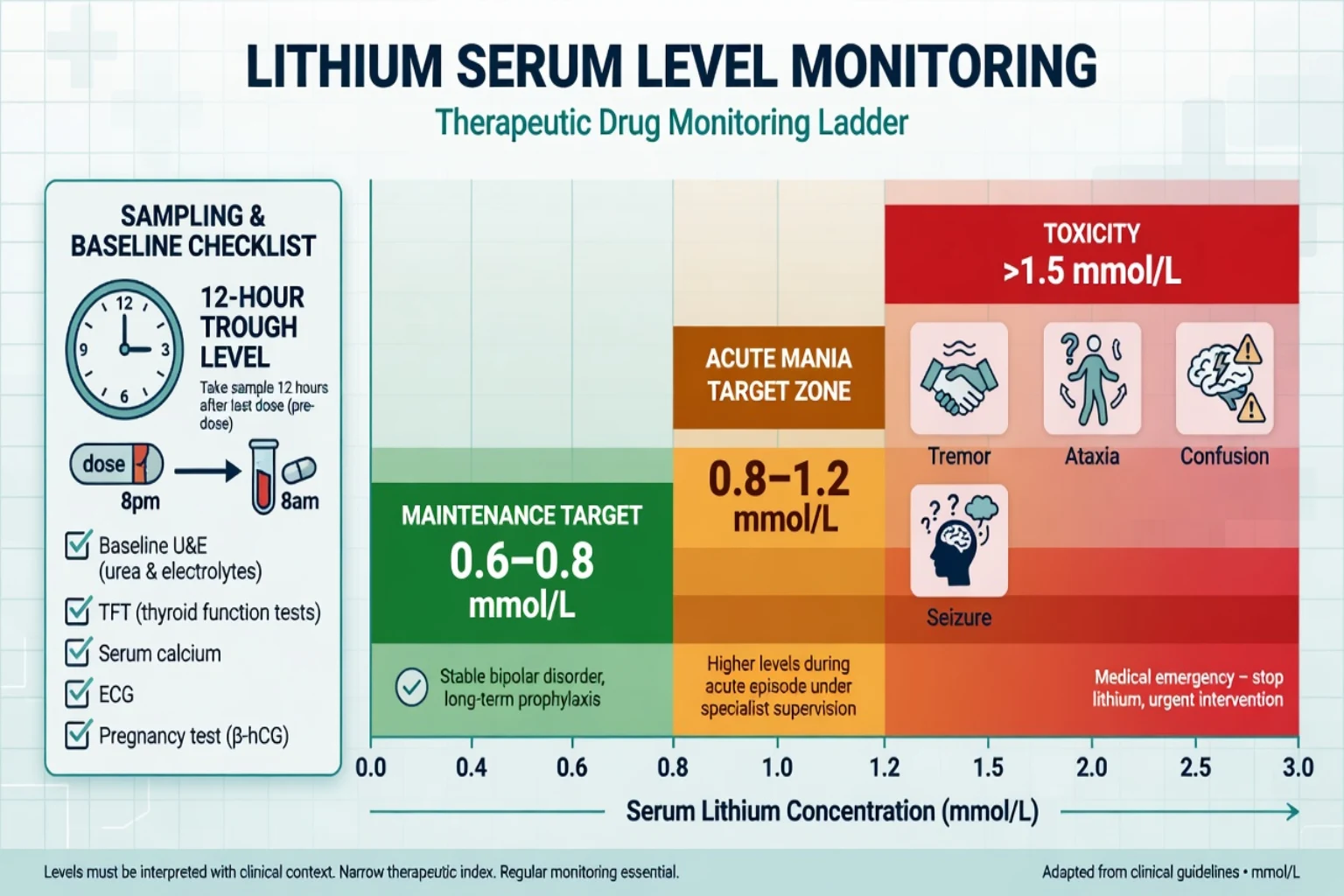
Standard teaching: 12-hour post-dose trough at steady state (typically after about 5 days of stable dosing for initiation/adjustment teaching). Label the time since last dose. Do not interpret a mid-absorption peak as a trough.[13]
AGNP-style TDM consensus supports lithium monitoring for efficacy targeting, adherence questions, interaction management, and toxicity — TDM is part of the prescription, not optional bureaucracy.[13]
Target bands (scaffolds — individualise)
| Phase | Common teaching trough band | Notes |
|---|---|---|
| Maintenance many adults | about 0.6–0.8 mmol/L | Often lowest effective level |
| Acute mania short-term | may aim higher within product-safe range | Speed often needs SGA cover too |
| Older adults | often lower (e.g. around 0.4–0.6 mmol/L teaching) | ISBD older-adult Delphi caution |
| Toxicity concern | often greater than 1.5 mmol/L plus signs | Chronic toxicity can be lower |
| Exact product information and local guidelines govern; older-adult Delphi (ISBD task force) emphasises lower targets and careful monitoring.[12][13][14][16] |
Organ monitoring calendar principles
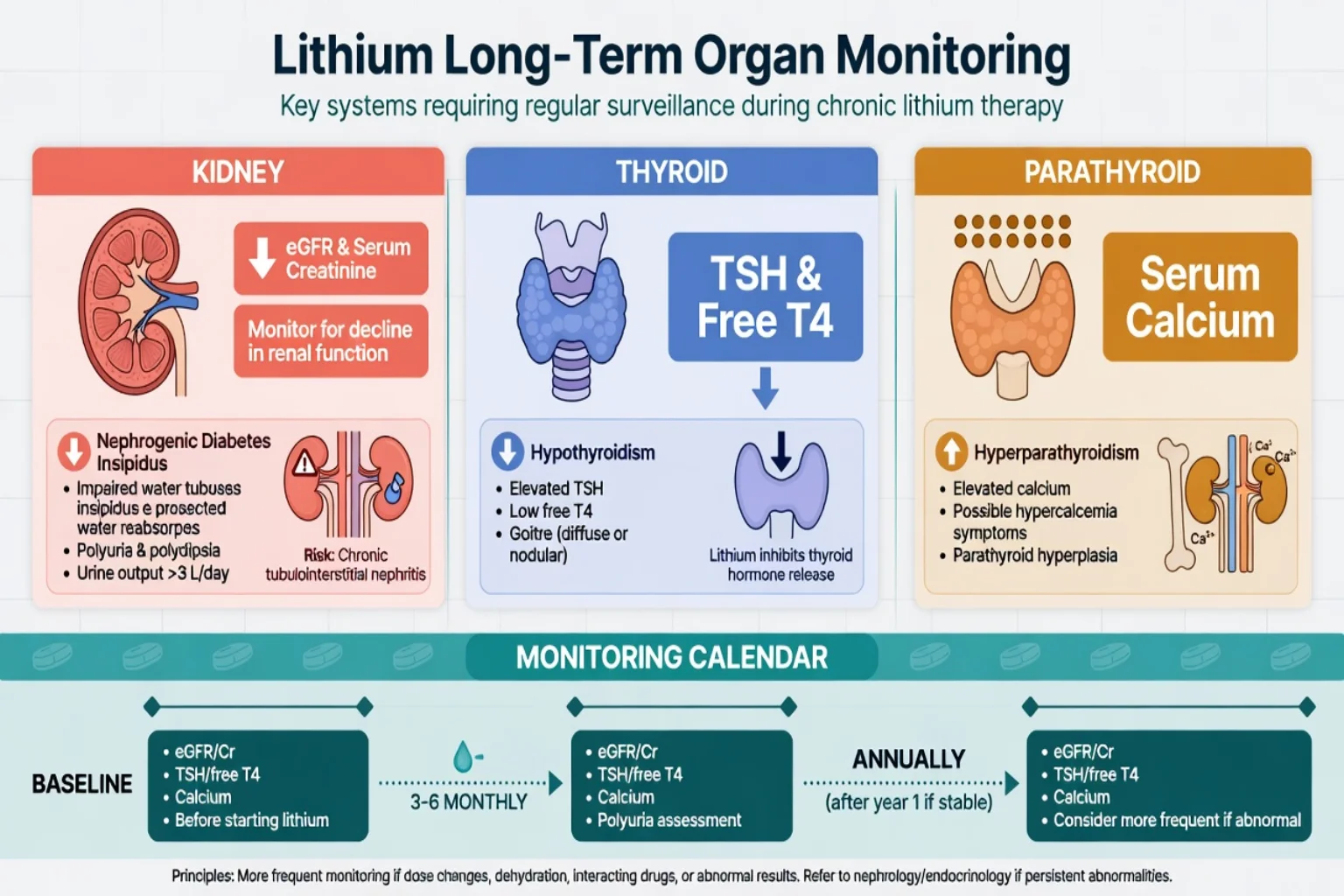
Baseline then periodic eGFR/creatinine, TFT, calcium, plus lithium level on a schedule denser early and after any change that alters clearance. Many services use roughly 3-monthly early then 6-monthly stable patterns — state principles and follow local protocol numbers rather than inventing universal law.[6][7][12][14]
Recheck urgently after intercurrent illness, dehydration, new interacting drug, or any toxicity symptom.[11][12]
Initiation and definitive prescribing
Start low, titrate to level and clinical effect. Typical adult teaching starts lithium carbonate in the 250–500 mg/day range (product-dependent; IR vs SR), divided or once-daily depending on formulation and tolerability, then titrates using 12-hour troughs. Acute mania often needs concurrent antipsychotic/benzodiazepine for behavioural control while lithium rises.[4][12][14]
Formulation notes: sustained-release products alter absorption kinetics and can prolong absorption in overdose — relevant for toxicology. Once-daily regimens are often preferred for adherence and may associate with lower 24-hour urine volume teaching than multiple daily doses in some literature summarised by Gitlin.[11][12]
Interaction ladder (exam favourites that raise levels): NSAIDs (including OTC), ACE inhibitors, ARBs, thiazide diuretics, dehydration/low effective volume, low-sodium states. Counsel patients before every new tablet and before every "just ibuprofen for a headache."[11][12]
Managing common adverse effects. Tremor: check level, reduce if high, consider beta-blocker when appropriate and not contraindicated. NDI: fluid access, specialist options including amiloride pathways, never ignore rising levels. Weight: lifestyle, metabolic co-management. Cognitive dulling: level optimisation and differential for depression.[12]
Hypothyroidism on lithium: replace thyroid hormone; continue lithium if psychiatric benefit is clear unless other reasons to stop.[6][12]
Falling eGFR: intensify monitoring, review levels and dose, nephrology partnership, shared decision about continuation versus switch — abrupt cessation without a mood plan is its own risk.[7][8][12]
Emergency management of toxicity
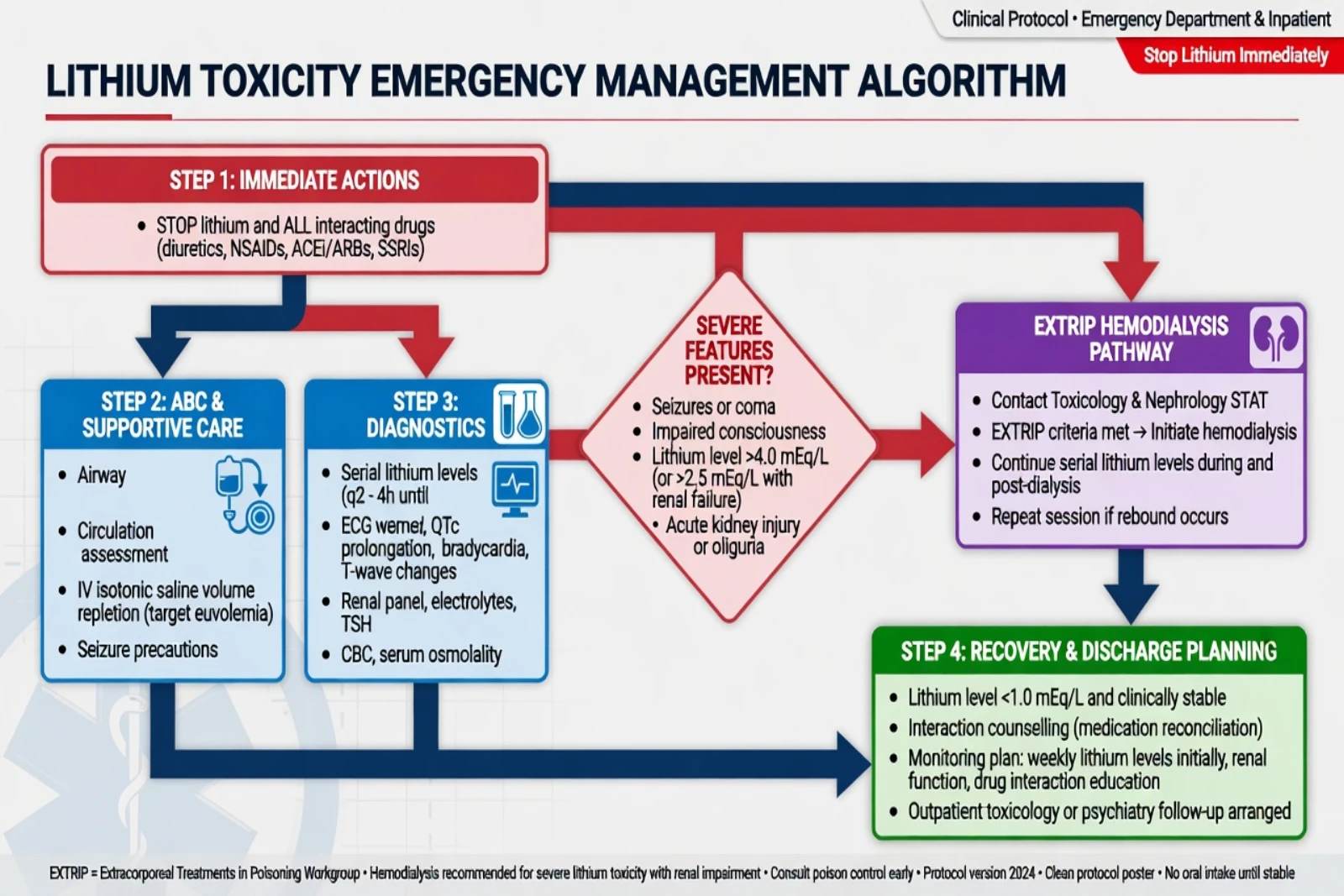
- Stop lithium and precipitating drugs (NSAIDs, ACEI/ARB, thiazides as relevant).
- ABC, glucose, treat seizures with benzodiazepines first-line framework.
- IV isotonic saline for volume repletion and renal perfusion when volume depleted — cornerstone supportive care; forced diuresis with loop diuretics is not the primary strategy.
- Serial lithium levels, U&E/creatinine, ECG; interpret with timing and clinical state.
- Decontamination: activated charcoal does not bind lithium; whole bowel irrigation may be considered for large recent sustained-release ingestions under toxicology advice.
- EXTRIP extracorporeal treatment recommended in severe poisoning (impaired kidney function with high level, or decreased consciousness, seizures, or life-threatening dysrhythmias irrespective of level; suggested for very high levels, significant confusion, or expected slow fall). Haemodialysis preferred; continuous RRT acceptable alternative; expect rebound from tissue redistribution and recheck levels after dialysis.[11]
After recovery: root-cause analysis (interaction, deliberate OD, NDI, dose error), suicide risk if intentional, restart-versus-switch decision, written sick-day and interaction plan.[5][11][12]
Suicide risk dimension
Cipriani RCT meta-analysis is the citation spine for lithium’s anti-suicide effect in mood disorders (fewer suicides and all-cause deaths versus placebo). In clinic this means: for high-risk bipolar patients, lithium is not interchangeable with “any mood stabiliser” when suicide risk is a primary driver — but it never replaces a full safety plan, leave, means restriction, and crisis pathway.[5][14]
Abrupt unsupervised cessation can unmask relapse and risk; planned changes need coverage and follow-up intensity.[1][5]
Pregnancy and lactation
Patorno 2017 (NEJM): first-trimester lithium associated with increased cardiac malformations including right-ventricular outflow tract obstruction spectrum; absolute risks modest compared with historical scare figures; dose relationship suggested (higher daily dose, higher risk). Use modern numbers, not 1970s folklore.[9]
Munk-Olsen 2018 (Lancet Psychiatry meta-analysis of six cohorts): lithium exposure not associated with the predefined pregnancy complications/delivery outcomes set; increased neonatal hospital readmission; first-trimester major malformations increased; major cardiac malformation difference not statistically significant in that pooled analysis — still counsel carefully and offer fetal cardiac assessment pathways per obstetric practice.[10]
Clinical synthesis for viva: untreated or poorly treated bipolar illness carries high relapse risk (especially postpartum); decisions are individualised with perinatal psychiatry and obstetrics; lowest effective level; peripartum level shifts with fluid status; do not panic-stop without a plan; lactation requires specialist risk–benefit because lithium enters breast milk.[9][10][14]
Special populations
Older adults. Lower targets, reduced GFR, polypharmacy interactions, falls, and toxicity presenting as delirium. ISBD Delphi emphasises cautious maintenance lithium practice in later life.[12][16]
Youth. Specialist initiation, family education, monitoring burden, and clear toxicity teaching.[14]
Renal impairment at baseline. Relative/absolute caution; nephrology partnership; sometimes lithium is still chosen for unique benefit with intensive monitoring — never casual.[7][8][12]
Intellectual disability / cognitive impairment. Capacity, fluid access, recognition of toxicity by carers, and constipation/dehydration risks amplify harm.[12]
Cognitive research niche. Forlenza randomised work explores long-term lithium in amnestic MCI — interesting, not a licence to prescribe lithium as a dementia drug in routine bipolar care without indication discipline.[15]
Prognosis and disposition
Long-term lithium reduces relapse risk when adhered to and monitored; BALANCE supports lithium-containing strategies over valproate monotherapy for bipolar I prophylaxis. Real-world effectiveness fails when levels are random, interactions ignored, or patients abandon treatment for unmanaged side effects. Shared care with GPs works when roles for levels, organ bloods, sick-day rules, and red-flag pathways are written down. Refer to specialist mood, perinatal, or nephrology services when complexity exceeds local capacity.[1][2][3][12][14]
Evidence, guidelines and regional differences
| Source | Exam take-home |
|---|---|
| Geddes 2004 | Long-term lithium reduces bipolar relapse vs placebo |
| BALANCE 2010 | Li ± valproate beat valproate alone for any episode |
| Severus 2014 | Maintenance efficacy reaffirmed |
| Cipriani 2011 mania NMA | SGAs often faster/acceptable; lithium still effective |
| Cipriani 2013 | Suicide and mortality reduction vs placebo |
| McKnight 2012 | NDI, hypothyroidism, hyperparathyroidism, weight |
| Shine 2015 | Long-term renal, thyroid, calcium laboratory signal |
| Kessing 2015 | CKD rates in modern lithium/anticonvulsant care |
| Patorno 2017 | Modest cardiac malformation increase first trimester |
| Munk-Olsen 2018 | Major malformation and neonatal readmission signals |
| EXTRIP 2015 | When to dialyse lithium poisoning |
| Gitlin 2016 | Side-effect management playbook |
| Malhi 2017 | Guideline first-line synthesis |
| Hiemke AGNP TDM | Level culture and sampling discipline |
| Landmark synthesis for viva speed.[1][2][3][4][5][6][7][8][9][10][11][12][13][14] |
ANZ: lithium remains a RANZCP-aligned first-line maintenance option when monitoring is feasible; product information drives exact level bands and pregnancy category language. UK: NICE bipolar guidance historically prioritises lithium for long-term treatment in many eligible adults with monitoring infrastructure (NICE Quality Standards/local shared-care). US: APA bipolar guidance supports lithium among first-line options; REMS not required (contrast clozapine). Europe: strong TDM culture (AGNP). Exact monitoring intervals and pregnancy labelling are local — principles travel; numbers may not.[13][14]
Exam pearls
LITHIUM non-negotiables
LITHIUM
References
- [1]Geddes JR, Burgess S, Hawton K, et al. Long-term lithium therapy for bipolar disorder: systematic review and meta-analysis of randomized controlled trials Am J Psychiatry, 2004.PMID 14754766
- [2]BALANCE investigators and collaborators, Geddes JR, Goodwin GM, et al. Lithium plus valproate combination therapy versus monotherapy for relapse prevention in bipolar I disorder (BALANCE): a randomised open-label trial Lancet, 2010.PMID 20092882
- [3]Severus E, Taylor MJ, Sauer C, et al. Lithium for prevention of mood episodes in bipolar disorders: systematic review and meta-analysis Int J Bipolar Disord, 2014.PMID 25530932
- [4]Cipriani A, Barbui C, Salanti G, et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis Lancet, 2011.PMID 21851976
- [5]Cipriani A, Hawton K, Stockton S, et al. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis BMJ, 2013.PMID 23814104
- [6]McKnight RF, Adida M, Budge K, et al. Lithium toxicity profile: a systematic review and meta-analysis Lancet, 2012.PMID 22265699
- [7]Shine B, McKnight RF, Leaver L, et al. Long-term effects of lithium on renal, thyroid, and parathyroid function: a retrospective analysis of laboratory data Lancet, 2015.PMID 26003379
- [8]Kessing LV, Gerds TA, Feldt-Rasmussen B, et al. Use of Lithium and Anticonvulsants and the Rate of Chronic Kidney Disease: A Nationwide Population-Based Study JAMA Psychiatry, 2015.PMID 26535805
- [9]Patorno E, Huybrechts KF, Bateman BT, et al. Lithium Use in Pregnancy and the Risk of Cardiac Malformations N Engl J Med, 2017.PMID 28591541
- [10]Munk-Olsen T, Liu X, Viktorin A, et al. Maternal and infant outcomes associated with lithium use in pregnancy: an international collaborative meta-analysis of six cohort studies Lancet Psychiatry, 2018.PMID 29929874
- [11]Decker BS, Goldfarb DS, Dargan PI, et al. Extracorporeal Treatment for Lithium Poisoning: Systematic Review and Recommendations from the EXTRIP Workgroup Clin J Am Soc Nephrol, 2015.PMID 25583292
- [12]Gitlin M Lithium side effects and toxicity: prevalence and management strategies Int J Bipolar Disord, 2016.PMID 27900734
- [13]Hiemke C, Bergemann N, Clement HW, et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017 Pharmacopsychiatry, 2018.PMID 29390205
- [14]Malhi GS, Gessler D, Outhred T The use of lithium for the treatment of bipolar disorder: recommendations from clinical practice guidelines J Affect Disord, 2017.PMID 28437764
- [15]Forlenza OV, Diniz BS, Radanovic M, et al. Disease-modifying properties of long-term lithium treatment for amnestic mild cognitive impairment: randomised controlled trial Br J Psychiatry, 2011.PMID 21525519
- [16]Shulman KI, Almeida OP, Herrmann N, et al. Delphi survey of maintenance lithium treatment in older adults with bipolar disorder: An ISBD task force report Bipolar Disord, 2019.PMID 30375703