Psych · Psychopharmacology — long-acting injectable antipsychotics
Long-acting injectable antipsychotics
Also known as LAI antipsychotics · Depot antipsychotics · Long-acting injectables · Paliperidone palmitate · Aripiprazole once-monthly · Risperidone microspheres · Olanzapine pamoate
Exam-exhaustive fellowship reference on long-acting injectable antipsychotics — agent map, oral overlap and loading, indications and adherence, real-world evidence (Tiihonen, Kishimoto), PRELAPSE and FEP data, PDSS, missed doses, monitoring, and when LAI does not replace clozapine. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Red flags
Long-acting injectable (LAI) antipsychotics are a high-yield fellowship topic because examiners test indication framing, agent-level initiation rules, oral overlap/loading traps, and the ability to reconcile real-world superiority with mixed RCT signals. Tiihonen nationwide cohorts, Kishimoto multi-design meta-analyses, PRELAPSE early-phase data, and Subotnik first-episode risperidone LAI form the evidence spine; Rosenheck VA unstable-schizophrenia RLAI is the classic negative-RCT counterpoint that tests design literacy.[1][2][3][5][6][7]
Definition and classification
An LAI (depot) antipsychotic is a parenteral extended-release formulation designed to maintain therapeutic antipsychotic exposure over weeks to months after intramuscular (or, for some products, subcutaneous) injection. It is not the same as short-acting IM antipsychotics used for acute agitation, and it is not chemical restraint. Core licensed territory is maintenance treatment of schizophrenia-spectrum illness; selected agents carry bipolar maintenance labels in some jurisdictions — always check local product information.[3][10]
Working exam taxonomy (agent families, intervals, and safety flags are teaching scaffolds anchored to labelled product evidence and comparative reviews — always verify local product information):[3][8][9][10]
| Class | Exam examples | Typical interval teaching scaffold | High-yield flag |
|---|---|---|---|
| FGA oil depots | Flupentixol, zuclopenthixol, fluphenazine, haloperidol (availability varies) | 1–4 weeks agent-specific | EPS, prolactin, TD risk higher than many SGAs |
| Risperidone microspheres | Risperidone LAI (classic q2-weekly product) | Every 2 weeks | Oral coverage commonly ~3 weeks at start |
| Paliperidone palmitate | PP1M, PP3M, PP6M (where marketed) | Monthly → 3-monthly → 6-monthly after stability | Day 1 + day 8 loading for monthly start; renal dosing |
| Aripiprazole LAIs | Aripiprazole monohydrate (once monthly); aripiprazole lauroxil (multi-week options) | Monthly or multi-week | Oral aripiprazole overlap or approved initiation kit/strategy |
| Olanzapine pamoate | Olanzapine LAI | 2–4 weekly depending on dose | PDSS — facility observation after every injection |
| The table summarises clinically distinct LAI families used in fellowship teaching; exact licensed sets vary by jurisdiction.[3][8][9] |
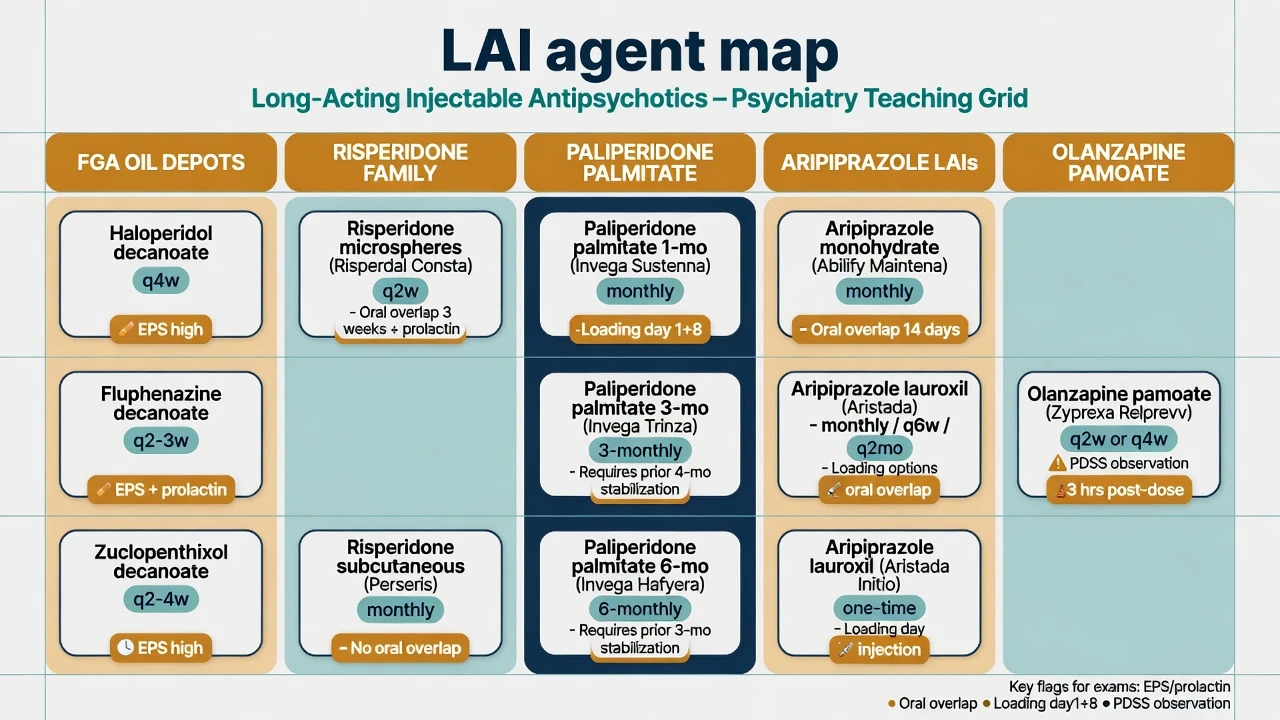
Formulation science matters clinically: oil depots (classic FGAs), aqueous nanocrystal suspensions (paliperidone palmitate, aripiprazole monohydrate), polymer microspheres (risperidone), and pamoate salt (olanzapine) each create different absorption kinetics and therefore different oral-overlap needs.[8][9]
Epidemiology, adherence and why LAIs exist
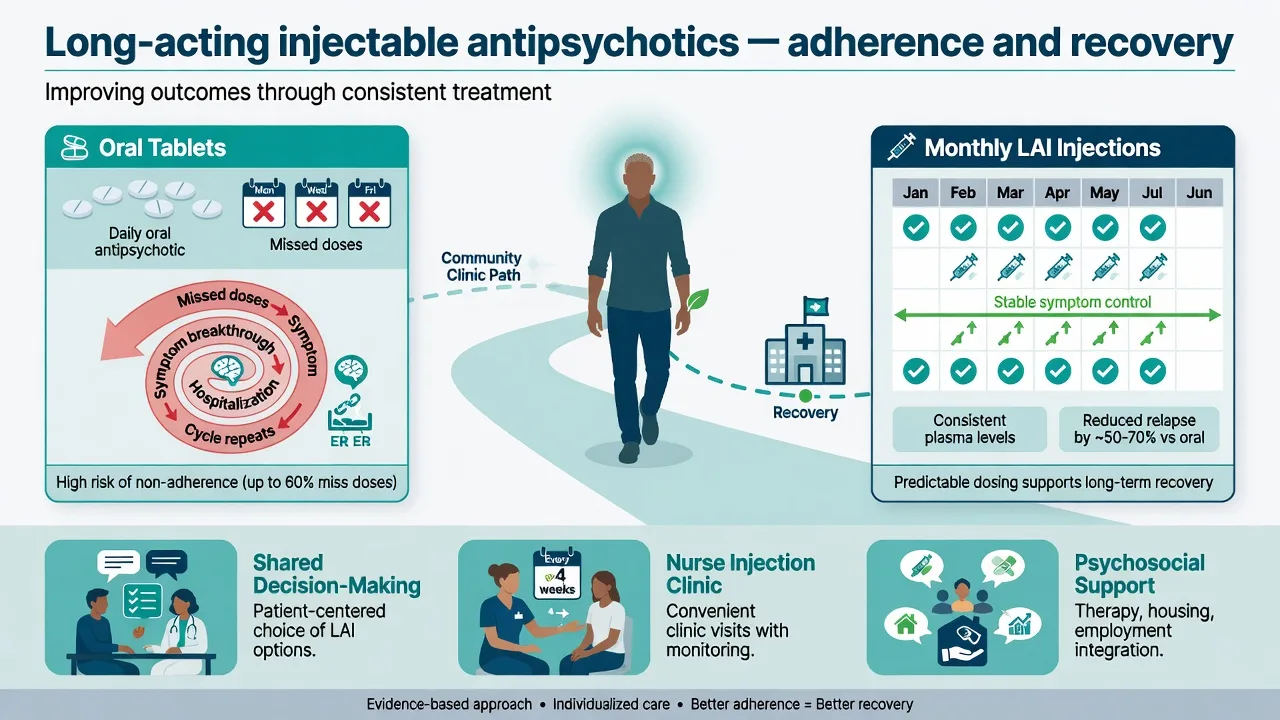
After first hospitalisation for schizophrenia, only a minority of patients reliably collect and continue their initial oral antipsychotic in nationwide data — early non-adherence is the norm, not the exception.[1] Non-adherence drives relapse, rehospitalisation, forensic risk, and mortality pathways; antipsychotic treatment as a class associates with lower mortality than no antipsychotic in large schizophrenia cohorts (FIN11-style message), so keeping people on treatment is a public-health intervention, not merely a clinic convenience.[11]
Under-use of LAIs remains common: clinician inertia, framing injectables as last-resort punishment, patient needle fear, service logistics, and cost/formulary barriers. Examiners reward candidates who offer LAIs early when adherence risk is high, including early-phase illness, rather than waiting for a revolving-door career.[5][6][15]
Numbers every candidate must own
These magnitudes are viva anchors from named studies — quote them as approximate effect sizes with design context, not as universal guarantees for the patient in front of you.[1][2][3][5][6]
Pathophysiology and pharmacokinetics
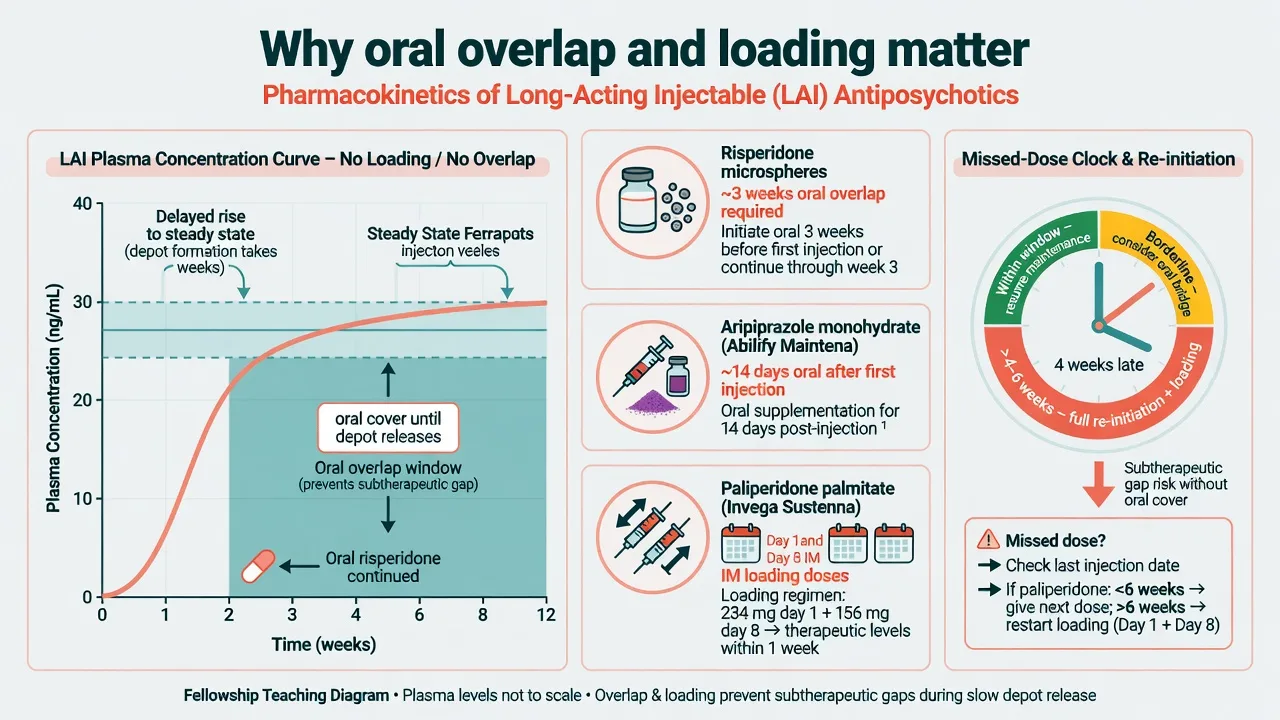
LAIs work by slow release from a tissue depot, producing absorption-rate-limited kinetics and long effective half-lives. Plasma levels rise more slowly than with oral dosing for many products; steady state can take weeks. That is why initiation regimens exist: oral overlap, loading injections, or approved one-day initiation kits keep exposure therapeutic while the depot fills.[3][8]
Therapeutic D2 occupancy principles match oral antipsychotics of the same molecule (efficacy window roughly ~60–80% occupancy teaching scaffold; EPS risk rises as occupancy climbs). The clinical advantage is not a new receptor — it is removing daily decision burden and covert partial adherence, with smoother peak–trough profiles for some agents.[10]
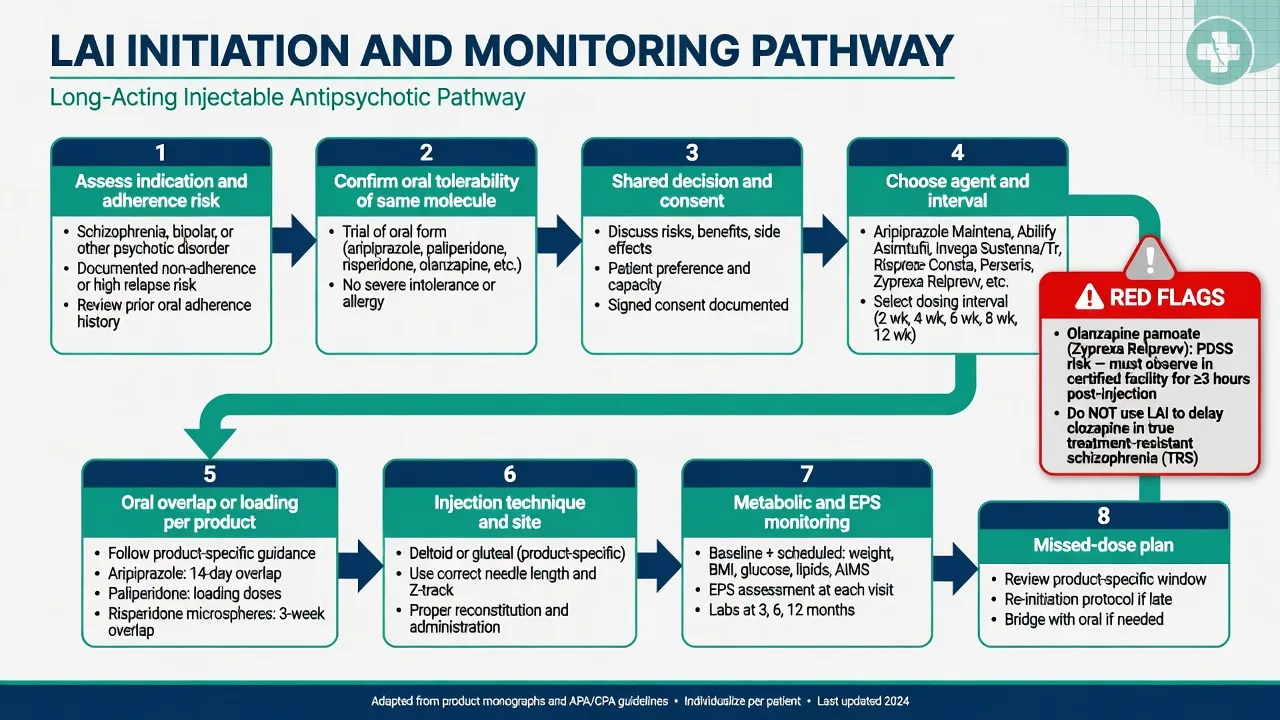
Olanzapine pamoate PDSS: accidental intravascular exposure can produce sudden high free olanzapine concentrations causing sedation, delirium, or coma — hence mandatory post-injection observation in a healthcare facility after every injection where the product is used.[9]
Clinical presentation and how to offer an LAI
Frame the conversation as shared decision: "This is a way to keep the medicine working even on hard weeks, reduce the chance of another admission, and free you from daily tablets if that fits your life." Do not say "you failed tablets so now we inject you." Ask about needle fear, cultural meaning of injectables, work/travel, preferred interval, and prior adverse effects.[5][13]
High-yield clinical scenarios: recurrent relapse with incomplete tablet taking; partial insight with family support for clinic attendance; supervised community treatment orders where injection visibility aids the legal plan; early-phase psychosis with known adherence risk; dual diagnosis with chaotic routines.[1][5][6]
Breakthrough symptoms between injections may mean true illness breakthrough, under-dosing, wrong interval, missed/late injection, substances, or psychosocial crisis — investigate before automatic dose escalation.[3]
Differentials that matter
| Problem | Prefer this thinking | Trap |
|---|---|---|
| "Failed two orals then failed LAI" | Was adherence actually secured? Was dose/interval adequate? TRRIP true TRS? | Endless SGA cycling instead of clozapine when TRS criteria met |
| Early relapse after LAI start | Missing oral overlap/loading | Labelling the molecule ineffective |
| Sedation minutes after olanzapine LAI | PDSS until proven otherwise | Sending home without observation |
| Patient refuses LAI with capacity | Respect, optimise oral supports, document | Coercive framing that destroys alliance |
| Good LAI but residual positives | Adequate dose? Substances? Need clozapine? | Adding third antipsychotic without structure |
| LAI success can unmask true treatment resistance once adherence is no longer the confounder — that is a feature, not a reason to stay on a failed LAI forever.[12] |
Assessment before first injection
- Indication and goals — maintenance psychosis control, relapse prevention, recovery goals (work, study, parenting).[13][15]
- Adherence assessment — prescription fills, collateral, hospitalisation pattern, pill counts, plasma levels if available for the oral agent.[1]
- Oral tolerability of the same molecule — document response and adverse effects before locking in multi-week exposure (allergy, severe EPS, prolactin symptoms, metabolic trajectory).[3][10]
- Baseline safety — weight/BMI/waist, BP, glucose/HbA1c, lipids, ECG when QTc risk factors, pregnancy test if relevant, renal function for paliperidone, prolactin if symptomatic or high-risk agent.[10]
- Capacity, consent, legal framework — voluntary shared decision whenever possible; if involuntary treatment applies, still explain and minimise coercion in process.[5]
- Logistics — who injects, where, reminder system, travel, deltoid vs gluteal feasibility, missed-dose plan in writing.[3]
Investigations and monitoring
Monitoring is class- and agent-matched, not "LAI-specific magic labs." Metabolic syndrome surveillance, EPS/TD examination, prolactin-as-indicated, and ECG risk stratification follow the parent molecule. Injection clinic contacts are opportunities for structured review — use them; do not treat the clinic as a drive-through needle stop.[2][10][11]
Plasma levels have a limited role for most LAIs but can help when delivery is uncertain or toxicity is suspected. Document every injection (date, dose, site, lot if required) and every PDSS observation period for olanzapine pamoate.[9]
Acute and emergency management
Acute dystonia / NMS on LAI: manage as for oral antipsychotics, but recognise the long residual exposure tail — stop further LAI doses, support, anticholinergics for dystonia, full NMS pathway if fever/rigidity/autonomic instability.[10]
Missed dose: treat as a relapse-risk emergency plan, not an afterthought. Product information defines windows for continuing on schedule versus re-initiation with loading/oral cover. Do not invent intervals in a viva — state the principle and that you would open the SmPC/local protocol.[3][8]
Definitive management — agents, oral overlap, dosing scaffolds
Always treat the tables below as teaching scaffolds. Exact milligram strengths, deltoid dose ceilings, and re-initiation clocks are product-information and jurisdiction-specific and change with new formulations. In exams, name the rule class and show you would verify the current label.[3][8][9]
Oral overlap and loading — the examiner favourite
Initiation scaffolds below follow labelled product principles for major SGA LAIs and classic depot practice; they are exam memory aids, not a substitute for the current SmPC.[5][6][8][9]
| Agent family | Initiation teaching scaffold | Maintenance interval scaffold |
|---|---|---|
| Risperidone microspheres | Continue oral risperidone (or equivalent cover) for about 3 weeks after first injection while microspheres release | Every 2 weeks IM (classic product) |
| Paliperidone palmitate monthly (PP1M) | Day 1 and day 8 IM loading doses (deltoid preferred for loads in many labels), then monthly maintenance; oral overlap often not required if loading is done correctly when switching from oral | Monthly; then consider PP3M after adequate stable PP1M (commonly taught after ≥4 monthly injections — verify label) |
| PP3M / PP6M | Only after stability on shorter-interval paliperidone LAI per label | Every 3 or 6 months |
| Aripiprazole monohydrate | After establishing oral aripiprazole tolerability, first injection often followed by ~14 days oral aripiprazole (or use an approved alternative initiation strategy/kit where available) | Monthly |
| Aripiprazole lauroxil | Oral aripiprazole overlap or one-day initiation options per label | Multi-week options (e.g. 4–8 weeks depending on strength) |
| Olanzapine pamoate | Conversion from oral olanzapine per label tables; no casual home injection | 2–4 weekly by dose; observe after every dose |
| FGA oil depots | Test dose concepts historically for some agents; establish oral/IM short-acting tolerability first | Agent-specific 1–4 weeks |
| These overlap and loading patterns are the high-yield traps examiners use to test pharmacokinetics literacy.[5][6][8][9] |
Paliperidone palmitate 3-month formulation significantly delayed relapse versus placebo in stabilised patients — longer intervals are evidence-based after shorter-interval stability, not a first jump from untreated illness.[8] Olanzapine LAI is efficacious in acute schizophrenia trials even without oral supplementation in study designs, but PDSS logistics dominate real-world use decisions.[9]
Choosing an agent
Match prior oral response, metabolic risk, EPS/prolactin sensitivity, interval preference, initiation complexity, and formulary. Partial-agonist LAIs (aripiprazole family) often suit patients needing lower prolactin/metabolic load; risperidone/paliperidone suit those who did well on that oral pathway but accept prolactin risk; olanzapine LAI for olanzapine responders who can access observation infrastructure; FGA depots where historically effective and EPS is managed.[2][5][10]
Network meta-analysis of oral antipsychotics still informs relative efficacy/tolerability of the parent molecules; Ostuzzi network work places oral and LAI options in a relapse-prevention evidence map — use it for ranking literacy, not brand marketing.[10][16]
Dose examples (scaffolds — verify label)
- Risperidone LAI (microspheres): commonly 25–50 mg IM every 2 weeks after oral establishment; oral cover ~3 weeks at initiation.[6][7]
- Aripiprazole monohydrate: commonly 400 mg IM monthly (with 300 mg option if tolerability requires) after oral aripiprazole establishment and labelled oral overlap/initiation strategy; PRELAPSE encouraged AOM within approved guidelines.[5]
- Paliperidone palmitate monthly: loading sequence then maintenance commonly in the 25–150 mg eq monthly range depending on prior oral dose and label — renal impairment needs dose adjustment.[8]
- Olanzapine pamoate: trial regimens included 210 mg/2 weeks, 300 mg/2 weeks, 405 mg/4 weeks versus placebo; convert from oral using label tables and observe for PDSS.[9]
What LAI does not replace
Psychosocial relapse-prevention interventions matter independently; LAI is one adherence technology inside multi-element care (early intervention, family work, CBT for psychosis where indicated, vocational support).[13][14][15]
TRRIP treatment-resistant schizophrenia: after two adequate failed antipsychotic trials with adherence confirmed (LAI can help prove adherence), offer clozapine — staying on a non-clozapine LAI is not a TRS strategy.[12]
Evidence and guidelines — how to answer the viva
Real-world signal is strong. In Finnish first-hospitalisation schizophrenia, depot formulations of the same compounds associated with roughly one-third the rehospitalisation risk of oral equivalents (adjusted HR 0.36).[1] In Swedish within-individual analyses, LAIs associated with about 20–30% lower rehospitalisation risk than equivalent orals (HR 0.78 total cohort), and clozapine plus LAIs ranked among the best options for preventing treatment failure.[2]
Meta-analytic signal is consistent when designs are pooled. Kishimoto cohort meta-analysis found lower hospitalisation rates with LAIs versus orals; the 2021 multi-design meta-analysis found LAI benefit on hospitalisation or relapse across RCTs, cohorts, and pre-post studies.[3][4]
Early-phase RCTs support earlier offer. PRELAPSE cluster-randomised encouragement of aripiprazole once-monthly versus usual care delayed time to first hospitalisation (HR 0.56; NNT frame ~7).[5] Subotnik randomised recent-onset schizophrenia to risperidone LAI versus oral: exacerbation/relapse 5% vs 33% with better positive-symptom control and adherence on LAI.[6]
Negative RCT literacy. Rosenheck VA trial in unstable schizophrenia found long-acting risperidone not superior to psychiatrist-choice oral on hospitalisation — intensive trial context can inflate oral adherence and dilute LAI advantage; cite this when an examiner attacks "all LAI hype."[7]
RANZCP / NICE / APA-aligned principles (region-aware): offer LAI when the person prefers it or when adherence threatens relapse; use shared decision; monitor cardiometabolic and neurological safety as for the parent drug; integrate with psychosocial care. Exact formulary agents, CTOs, and observation rules for olanzapine pamoate are jurisdiction-specific — state principles and follow local product information and service protocols rather than inventing universal milligram law. These principles align with evidence that earlier, preference-aligned LAI use can reduce hospitalisation risk when adherence is the failure mode.[1][3][5][9]
Special populations
Youth and early-phase: offer with careful counselling; evidence supports considering LAI earlier than traditional "last resort" culture.[5][6][15]
Older adults: start lower, watch falls, EPS, QTc, renal function (paliperidone), and injection technique practicality.[10]
Pregnancy and lactation: individualise; long half-life means exposure continues after the last injection — plan pre-conception when possible; do not stop abruptly without a relapse plan.[10]
Intellectual disability / capacity: supported decision-making; avoid framing LAI as behavioural control alone.[12]
Forensic / CTO contexts: LAI can support legal treatment plans but still requires dignity, explanation, and metabolic care.[2]
Prognosis and disposition
Hard outcomes that matter: time to hospitalisation, relapse, treatment discontinuation, and functioning. Real-world LAI use improves retention and reduces rehospitalisation at population scale; early-phase use can change trajectory if embedded in comprehensive care.[2][5][13] Longer-interval formulations (PP3M/PP6M) suit stable, recovery-oriented patients who want fewer clinic days — keep monthly contact when clinical risk or engagement needs are high.[8]
Complications and pitfalls
Initiation failures
- No oral tolerability trial
- Skipped oral overlap/loading
- Wrong site/volume for dose
- No missed-dose written plan
Safety failures
- Olanzapine LAI without observation
- Ignored prolactin/sexual dysfunction
- Metabolic neglect at injection clinic
- NMS/dystonia with long residual exposure
Strategic failures
- LAI as punishment
- Delaying clozapine in true TRS
- No psychosocial package
- Assuming LAI equals full recovery care
Exam correctives
- Shared decision early
- Same-molecule tolerability first
- Name Tiihonen/Kishimoto/PRELAPSE
- Product information for exact mg
Exam pearls
- LAI is adherence technology, not a new antipsychotic class with magical receptors.[3]
- Quote Tiihonen 0.36 (early depot vs oral same compound) and ~20–30% rehospitalisation reduction LAI vs oral (Sweden) with design humility.[1][2]
- PRELAPSE and Subotnik justify early-phase offer language.[5][6]
- Rosenheck is the negative RCT you must be able to explain.[7]
- Oral overlap traps: risperidone microspheres ~3 weeks; aripiprazole monohydrate often ~14 days oral after first injection; PP1M day 1 + day 8 loads.[5][6][8]
- PDSS = olanzapine pamoate observation every time.[9]
- LAI does not replace clozapine when TRRIP criteria are met.[12]
- Injection clinic without metabolic review is incomplete care.[11]
Controversies handled calmly
Whether every FEP patient should be offered LAI remains debated; the evidence-based exam answer is offer early when risk and preference align, not mandate universally. Whether RCTs or real-world data "win" is a false binary — RCTs minimise non-adherence differences; cohorts capture them. Cost-effectiveness and formulary politics are real but secondary to clinical framing in a fellowship station.[3][5][7]
Bottom line for the board
Master the agent map, the initiation/overlap rules, the named evidence ladder, and the ethics of offer. A candidate who can consent for aripiprazole once-monthly in early-phase illness, load paliperidone palmitate correctly, observe olanzapine pamoate, and still know when to stop cycling LAIs and start clozapine will pass LAI stations across FRANZCP, MRCPsych, ABPN and MD/DNB viva formats.[2][5][8][9][12]
References
- [1]Tiihonen J, Haukka J, Taylor M, et al. A nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophrenia Am J Psychiatry, 2011.PMID 21362741
- [2]Tiihonen J, Mittendorfer-Rutz E, Majak M, et al. Real-World Effectiveness of Antipsychotic Treatments in a Nationwide Cohort of 29 823 Patients With Schizophrenia JAMA Psychiatry, 2017.PMID 28593216
- [3]Kishimoto T, Hagi K, Kurokawa S, et al. Long-acting injectable versus oral antipsychotics for the maintenance treatment of schizophrenia: a systematic review and comparative meta-analysis of randomised, cohort, and pre-post studies Lancet Psychiatry, 2021.PMID 33862018
- [4]Kishimoto T, Hagi K, Nitta M, et al. Effectiveness of Long-Acting Injectable vs Oral Antipsychotics in Patients With Schizophrenia: A Meta-analysis of Prospective and Retrospective Cohort Studies Schizophr Bull, 2018.PMID 29868849
- [5]Kane JM, Schooler NR, Marcy P, et al. Effect of Long-Acting Injectable Antipsychotics vs Usual Care on Time to First Hospitalization in Early-Phase Schizophrenia: A Randomized Clinical Trial JAMA Psychiatry, 2020.PMID 32667636
- [6]Subotnik KL, Casaus LR, Ventura J, et al. Long-Acting Injectable Risperidone for Relapse Prevention and Control of Breakthrough Symptoms After a Recent First Episode of Schizophrenia. A Randomized Clinical Trial JAMA Psychiatry, 2015.PMID 26107752
- [7]Rosenheck RA, Krystal JH, Lew R, et al. Long-acting risperidone and oral antipsychotics in unstable schizophrenia N Engl J Med, 2011.PMID 21366475
- [8]Berwaerts J, Liu Y, Gopal S, et al. Efficacy and Safety of the 3-Month Formulation of Paliperidone Palmitate vs Placebo for Relapse Prevention of Schizophrenia: A Randomized Clinical Trial JAMA Psychiatry, 2015.PMID 25820612
- [9]Lauriello J, Lambert T, Andersen S, et al. An 8-week, double-blind, randomized, placebo-controlled study of olanzapine long-acting injection in acutely ill patients with schizophrenia J Clin Psychiatry, 2008.PMID 18452346
- [10]Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis Lancet, 2013.PMID 23810019
- [11]Tiihonen J, Lönnqvist J, Wahlbeck K, et al. 11-year follow-up of mortality in patients with schizophrenia: a population-based cohort study (FIN11 study) Lancet, 2009.PMID 19595447
- [12]Howes OD, McCutcheon R, Agid O, et al. Treatment-Resistant Schizophrenia: Treatment Response and Resistance in Psychosis (TRRIP) Working Group Consensus Guidelines on Diagnosis and Terminology Am J Psychiatry, 2017.PMID 27919182
- [13]Kane JM, Robinson DG, Schooler NR, et al. Comprehensive Versus Usual Community Care for First-Episode Psychosis: 2-Year Outcomes From the NIMH RAISE Early Treatment Program Am J Psychiatry, 2016.PMID 26481174
- [14]Bighelli I, Rodolico A, García-Mieres H, et al. Psychosocial and psychological interventions for relapse prevention in schizophrenia: a systematic review and network meta-analysis Lancet Psychiatry, 2021.PMID 34653393
- [15]Correll CU, Galling B, Pawar A, et al. Comparison of Early Intervention Services vs Treatment as Usual for Early-Phase Psychosis: A Systematic Review, Meta-analysis, and Meta-regression JAMA Psychiatry, 2018.PMID 29800949
- [16]Ostuzzi G, Bertolini F, Tedeschi F, et al. Oral and long-acting antipsychotics for relapse prevention in schizophrenia-spectrum disorders: a network meta-analysis of randomised trials Lancet Psychiatry, 2022.PMID 35524620