Psych · Psychopharmacology — monoamine oxidase inhibitors
Monoamine oxidase inhibitors
Also known as MAOIs · Phenelzine · Tranylcypromine · Isocarboxazid · Moclobemide · Selegiline patch · EMSAM · RIMA · Tyramine diet · Cheese reaction
Exam-exhaustive fellowship pharmacology of monoamine oxidase inhibitors — irreversible nonselective agents, RIMA moclobemide, selegiline transdermal system, tyramine and washouts, serotonin toxicity combinations, hypertensive crisis, atypical depression and STAR*D late-pathway TRD use. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Monoamine oxidase inhibitors are the fellowship drug class that separates candidates who can recite "avoid cheese" from those who can run a safe TRD pathway. Examiners stress classification, tyramine pharmacology, washout arithmetic, serotonin toxicity pairs, and the selegiline patch dose–diet interaction. Under-use is real; reckless use is examinable malpractice.[1][2][3][11]
Definition and classification
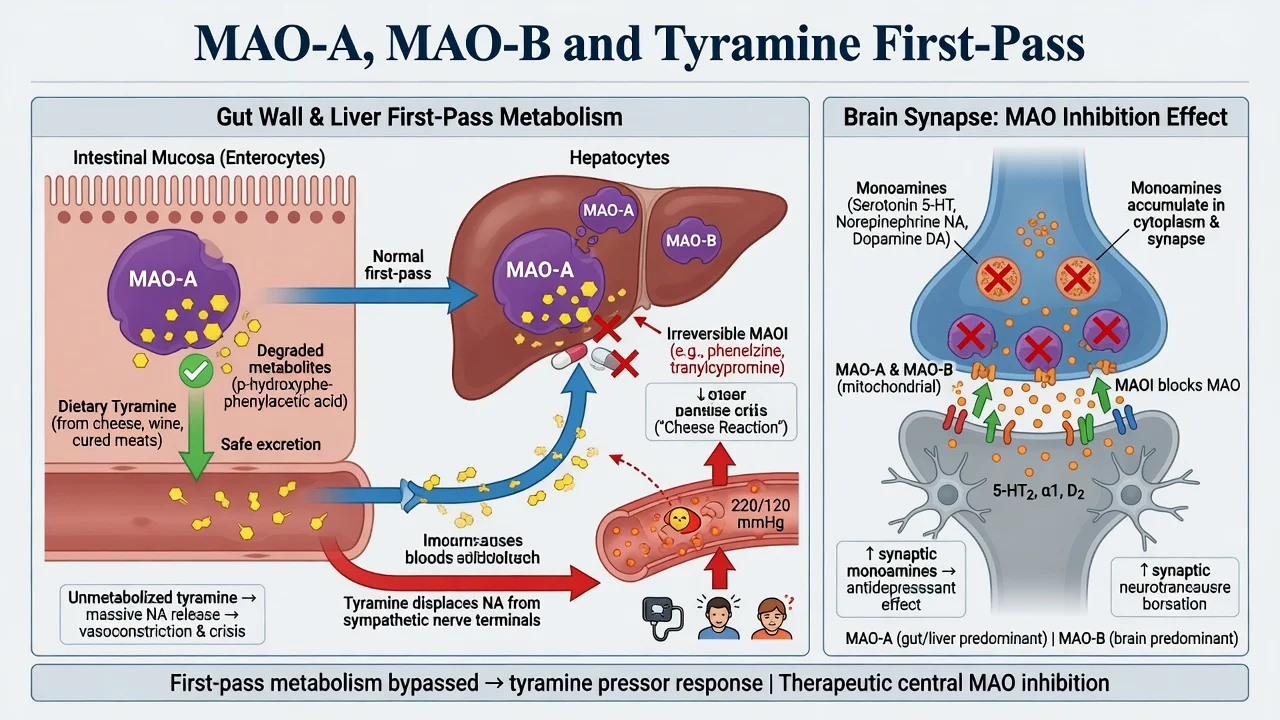
An MAOI antidepressant inhibits monoamine oxidase enzymes that catabolise serotonin, noradrenaline, dopamine and dietary monoamines such as tyramine. Clinical antidepressant effect tracks mainly MAO-A inhibition in the central nervous system; gut and hepatic MAO-A are the safety valve that normally destroys dietary tyramine before it can act as a pressor amine.[2][12]
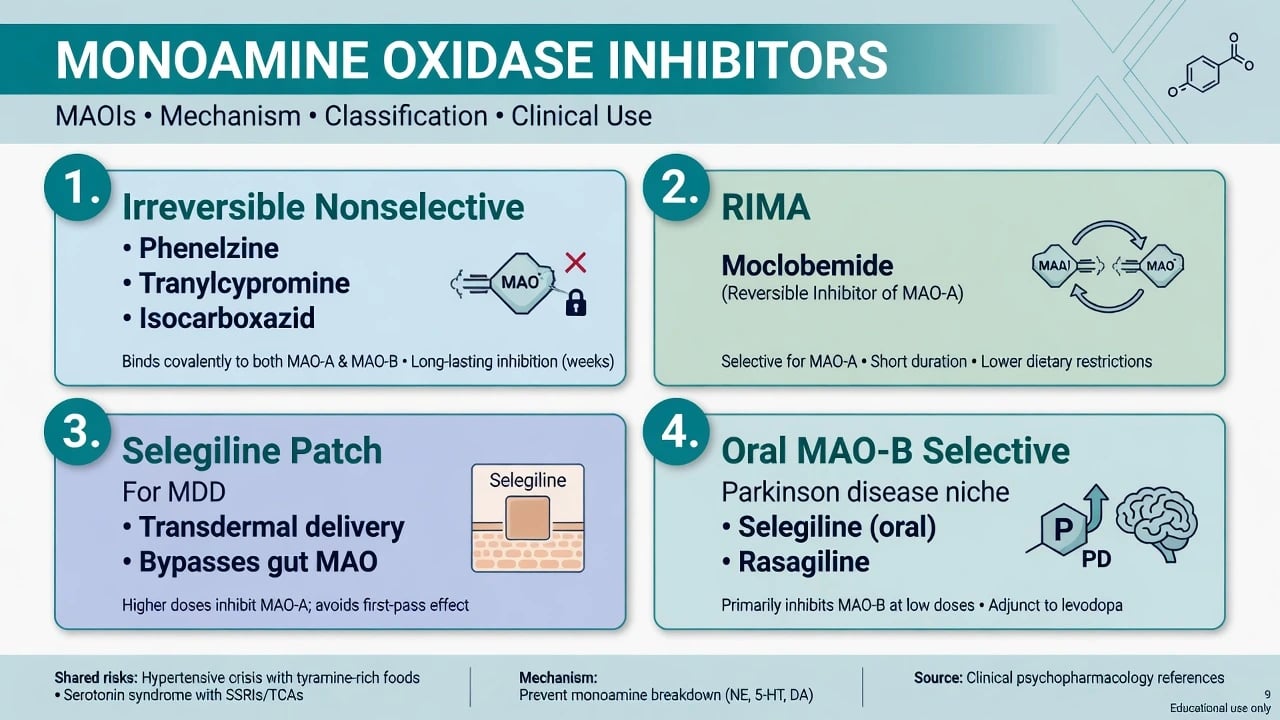
| Class | Agents (examples) | Reversibility | Exam hook |
|---|---|---|---|
| Irreversible nonselective | Phenelzine, tranylcypromine, isocarboxazid | Irreversible A+B | Full tyramine diet; longest safety checklist |
| RIMA (reversible MAO-A) | Moclobemide | Reversible selective A | Gentler diet; still serotonergic-interaction aware |
| Selegiline transdermal (MDD) | STS / selegiline patch | Dose-dependent CNS MAO inhibition | 6 mg/24 h diet teaching differs from 9–12 mg |
| Oral MAO-B selective | Oral selegiline (Parkinson doses) | Selective B at low oral dose | Not a routine antidepressant strategy at selective doses |
| Classification and patch dose–diet teaching above are exam orientation maps drawn from contemporary MAOI reviews and selegiline RCT programmes.[1][2][7][8] |
Chemistry trivia examiners still ask: hydrazine agents (phenelzine, isocarboxazid) versus non-hydrazine tranylcypromine (more activating; amphetamine-like structural flavour without equating them clinically).[1][2]
Epidemiology and place in care
MAOIs were among the first effective antidepressants and then fell from routine first-line use as SSRIs arrived with simpler safety narratives. Contemporary reviews document under-prescribing relative to residual efficacy in atypical depression and treatment-resistant depression (TRD), often because clinicians never learned practical diet and interaction management.[2][3]
STAR*D multi-step data show that remission falls as failed trials accumulate; late pathways including MAOI are hard, not obsolete. McGrath and colleagues compared tranylcypromine with venlafaxine plus mirtazapine after three failed medication trials — remission was low in both arms, reinforcing specialist intensity rather than casual MAOI improvisation.[5][6]
Anchors every viva should own
These are orientation anchors from landmark trials and standard product-safety teaching — always confirm current local product information.[4][5][7][8][1]
Pathophysiology — MAO isoforms and the cheese reaction
MAO-A preferentially deaminates serotonin, noradrenaline and tyramine. MAO-B handles phenylethylamine and shares dopamine. Irreversible inhibitors covalently inactivate enzyme; recovery requires new enzyme synthesis over roughly two weeks, which is why washouts are measured in weeks, not half-lives of the tablet alone.[2][12]
Tyramine hypertensive crisis ("cheese reaction"). Dietary tyramine is normally destroyed by gut and hepatic MAO-A. With irreversible nonselective inhibition, absorbed tyramine displaces noradrenaline from sympathetic terminals, producing acute hypertension, severe headache, and risk of intracranial haemorrhage. Risk is dose-related to tyramine load, not mystical — modern analytical work refined which foods truly exceed dangerous per-serving thresholds.[10][11][12]
RIMA logic. Reversible competitive MAO-A inhibitors can be displaced by high substrate loads, giving a pharmacological safety buffer against tyramine compared with irreversible agents, while retaining antidepressant utility in meta-analysis versus TCA comparators for moclobemide-class drugs.[9][12]
Selegiline patch logic. Transdermal delivery aims for CNS MAO inhibition while reducing first-pass gut MAO-A inhibition at the lowest approved antidepressant patch dose, supporting trials that treated MDD without routine dietary restriction at that dose level — higher patch doses reintroduce dietary caution in labelling teaching.[7][8][12]
Clinical indications and presentation context
Primary exam indications:
- Treatment-resistant unipolar depression after adequate failed trials, within a specialist TRD pathway (augmentation, switch, ECT consideration as parallel options).[1][5][16][17]
- Atypical depression — mood reactivity with rejection sensitivity, leaden paralysis, hypersomnia and hyperphagia historically showed preferential response to phenelzine over imipramine in the Columbia group programme; Liebowitz 1988 remains the classic stem.[4]
- Selected anxiety spectrum uses (jurisdiction-dependent), especially moclobemide where licensed for social anxiety in some regions — always check local product labels.[2][9]
MAOIs are not the default first tablet for uncomplicated mild–moderate MDD in stepped-care systems that favour psychological therapy and safer first-line antidepressants.[16][17][18]
Assessment before prescribing
Before the first irreversible MAOI dose, document: confirmed unipolar (or carefully formulated) diagnosis and bipolar screen; full medicine and OTC list including cold remedies with dextromethorphan or sympathomimetics, tramadol, pethidine, other opioids, triptans, stimulants, St John's wort and other antidepressants; capacity and practical ability to follow diet and interaction rules with written materials and pharmacy flag; baseline lying and standing BP, weight, sexual function, suicide risk and means access, and pregnancy potential; and an emergency plan for severe headache or neurological symptoms after restricted foods. Prescribing without a diet and interaction education plan is incomplete care, not elegant minimalism.[1][11][12]
Investigations
No routine plasma level monitoring is required for classic MAOIs in most services. Obtain general psychotropic baseline as indicated (U&E, LFT, ECG if cardiac risk or older adult, pregnancy test). In crisis: continuous BP and ECG for hypertensive emergencies; serotonin toxicity remains a clinical diagnosis using Hunter decision rules when a serotonergic agent is present.[14][15][1]
Definitive management — agents, doses, monitoring
Doses below are exam orientation ranges for adults; start low, titrate slowly, individualise, and verify current product information and local formulary. Older adults need lower starts and slower titration because of orthostasis.[1][2][17]
| Agent | Typical adult oral pattern | Practical notes |
|---|---|---|
| Phenelzine | Start 15 mg daily → often 45–90 mg/day in divided doses | Orthostasis common; weight gain; hydrazine class |
| Tranylcypromine | Start 10 mg daily/divided → often 20–60 mg/day | Activating; insomnia if late dosing; STAR*D L4 agent |
| Isocarboxazid | Specialist low start; titrate | Less commonly stocked; same interaction rules |
| Moclobemide | Often 300 mg/day → 300–600 mg/day after food | RIMA; shorter interaction horizon than irreversible agents but not free of serotonergic cautions |
| Selegiline patch | 6 mg/24 h; may increase to 9 or 12 mg/24 h | Apply to dry intact skin; rotate sites; diet rules dose-dependent |
| Ranges are exam orientation anchors from specialist MAOI guides, RIMA meta-analysis and selegiline patch trials — product information and local protocols override memory tables.[1][7][8][9] |
Adequate trial. Therapeutic dose for typically 4–8 weeks with adherence, diet compliance, and measurement-based symptom tracking before declaring failure. Pseudo-resistance still applies: wrong diagnosis, substances, non-adherence, under-dosing from fear of side-effects.[1][6][16]
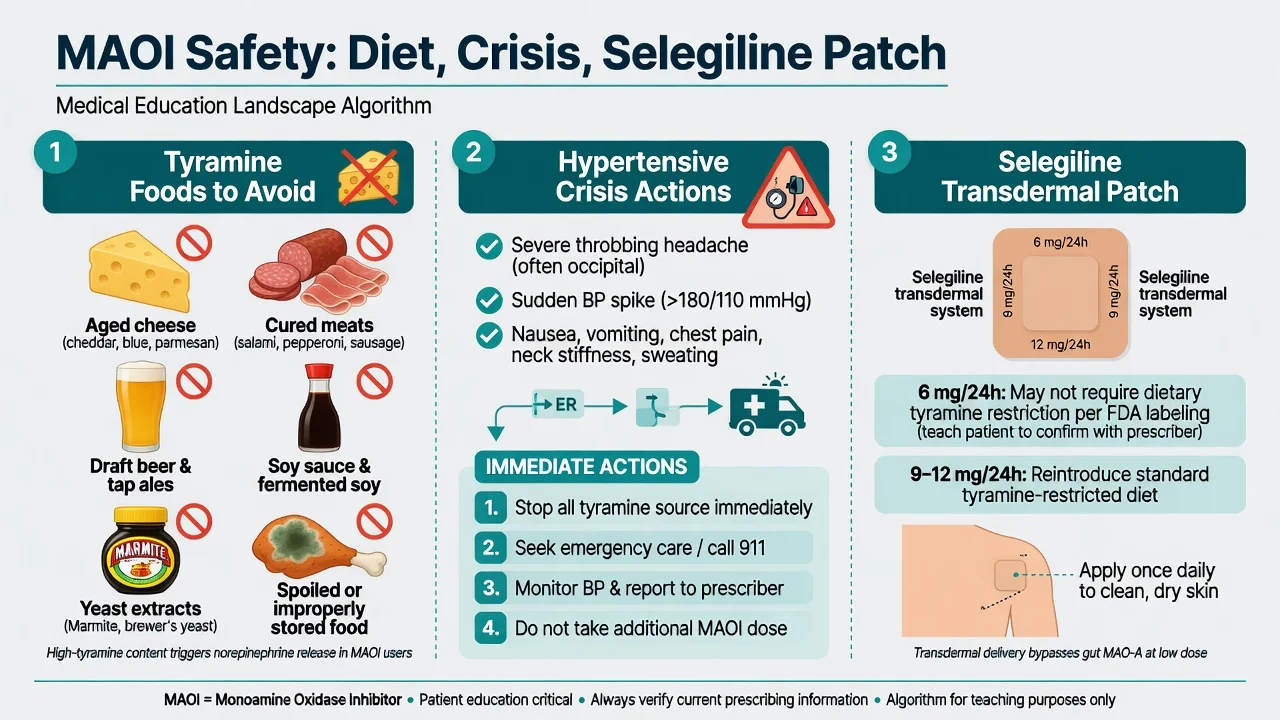
Selegiline transdermal system. Bodkin and Amsterdam demonstrated short-term antidepressant efficacy versus placebo. Amsterdam's 2003 trial specifically studied the system without dietary restrictions in the protocol design, supporting the low-dose dietary teaching that examiners still test: relaxed tyramine diet mainly at 6 mg/24 h; reimpose restrictions at 9–12 mg/24 h per product labelling logic. Drug–drug serotonergic prohibitions still apply at all doses.[7][8][1]
Tyramine diet — modern, not folklore
Analytical work by Walker, Shulman and colleagues refined which foods actually deliver high tyramine per serving (for example aged or poorly stored high-risk items such as certain aged cheeses, some fermented/cured products, soy sauce in quantity, yeast extracts, spoiled protein). Modern prescriber diet guides emphasise high-tyramine aged/fermented/spoiled foods, portion and storage, and practical patient language rather than endless forbidden lists that destroy adherence.[10][11]
Absolute teaching set (classic irreversible MAOI): aged cheeses, cured/aged meats, draft (tap) beer, concentrated yeast extracts, soy sauce in significant amounts, improperly stored protein foods, and other high-tyramine fermented products. Fresh foods prepared and refrigerated properly are far safer than historical scare-lists suggested. Continue diet restrictions for about two weeks after stopping an irreversible MAOI while enzyme regenerates.[10][11][12]
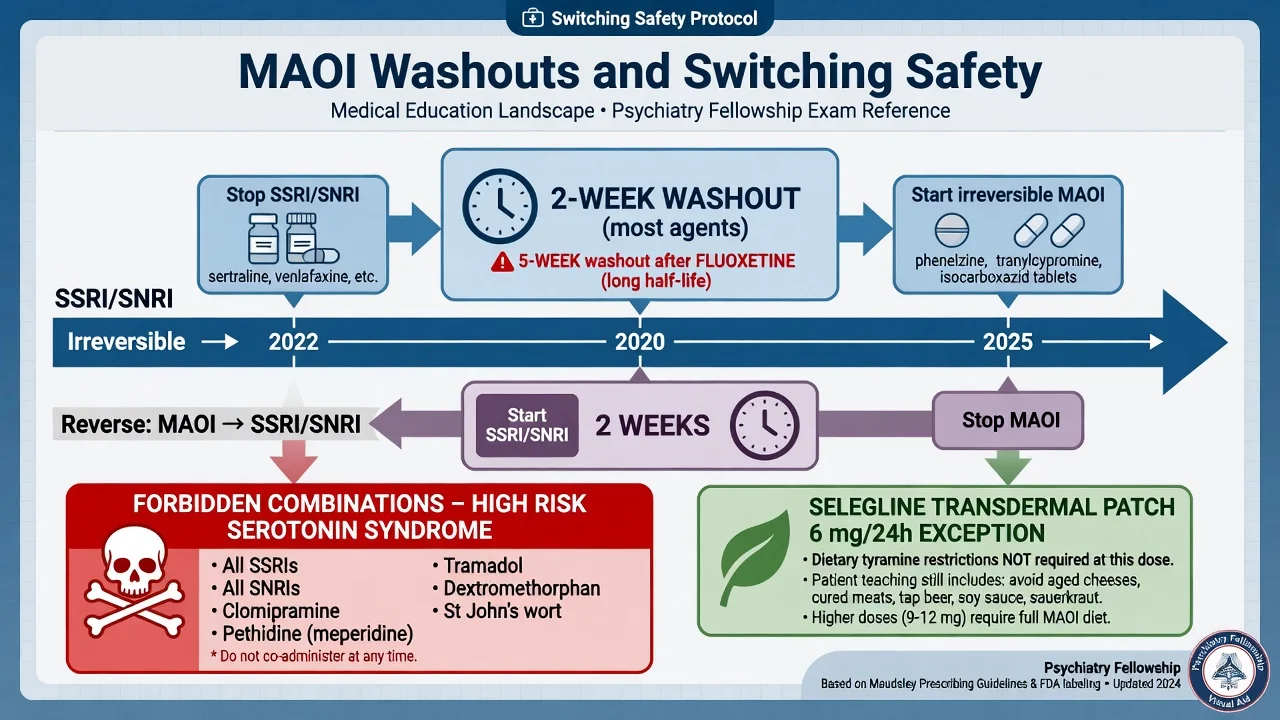
Washouts and switching — non-negotiable arithmetic
Standard exam teaching (always confirm product information): most SSRI/SNRI/TCA → irreversible MAOI about 2 weeks after stop; fluoxetine → irreversible MAOI about 5 weeks (long half-life norfluoxetine); irreversible MAOI → SSRI/SNRI/other serotonergic antidepressant about 2 weeks after stop; moclobemide switches use shorter product-specific horizons than irreversible agents but must still be planned — do not freestyle. Cross-taper into an irreversible MAOI from an SSRI is an exam fail. Direct combination of irreversible MAOI with SSRI, SNRI, clomipramine or imipramine is a classic cause of severe serotonin toxicity.[1][12][14]
Drug interactions — two lethal pathways
Tyramine / pressor pathway
- Unmetabolised dietary tyramine
- Noradrenaline displacement
- Hypertensive crisis, severe headache
- Risk of ICH if untreated
- Diet + storage education
Serotonin toxicity pathway
- MAOI + SRI or serotonergic opioid
- Hunter criteria neuromuscular signs
- Stop agents, support, cool, ICU if severe
- Pethidine, tramadol, dextromethorphan classic
- Not the same as cheese reaction
Sympathomimetic pathway
- Indirect amines, some cold remedies
- Stimulants, amphetamine-type agents
- Severe hypertension or toxicity
- Pharmacy alert essential
Selegiline patch nuance
- 6 mg/24 h: diet often liberalised in labelling teaching
- 9–12 mg: reintroduce tyramine caution
- Serotonergic drug rules still absolute
- Bodkin/Amsterdam efficacy base
Pathway map synthesises MAOI interaction reviews, serotonin toxicity literature and selegiline patch trial labelling teaching.[7][8][12][13][14]
Serotonergic high-risk partners: SSRIs, SNRIs, clomipramine, imipramine, St John's wort, linezolid (MAOI antibiotic context), methylene blue (specialist perioperative), and opioids with significant serotonin reuptake effects — especially pethidine (meperidine), tramadol and dextromethorphan. Gillman's anaesthesia-focused review is the standard citation for MAOI–opioid serotonin toxicity literacy; morphine-class agents without strong SRI activity are relatively preferred when analgesia is essential and coordinated.[13][14][12]
Serotonin toxicity is diagnosed clinically. Boyer and Shannon describe the triad of altered mental status, autonomic hyperactivity and neuromuscular excitation. Hunter Serotonin Toxicity Criteria improve specificity in the presence of a serotonergic agent (spontaneous clonus; inducible clonus plus agitation or diaphoresis; ocular clonus plus agitation or diaphoresis; tremor plus hyperreflexia; or hypertonia with temperature above 38°C plus ocular/inducible clonus — quote the published rules, not improvisation).[14][15]
Management principles: stop offending agents; ABC; benzodiazepines for agitation; active cooling; cyproheptadine in specialist protocols; ICU for severe hyperthermia and rigidity. Differentiate from NMS (dopamine-blocker context, bradyreflexia/lead-pipe pattern) and from pure tyramine crisis (pressor picture without the serotonergic neuromuscular signature).[14][15]
Hypertensive crisis management: emergency department pathway — continuous BP monitoring, short-acting parenteral antihypertensives per local protocol (historical teaching often names phentolamine; modern practice uses protocol-driven agents), stop ongoing tyramine exposure, evaluate for end-organ damage. Do not treat every headache as anxiety after aged cheese on an MAOI.[11][12]
Adverse effects beyond crises
Common and important non-crisis effects: orthostatic hypotension (especially phenelzine — check postural BP), dizziness, insomnia or activation (tranylcypromine), daytime sedation, weight gain, sexual dysfunction, oedema, myoclonus, and rare hepatotoxicity concerns with hydrazine agents. Sexual side-effects still matter for adherence even when the class is chosen for TRD. Early activation and suicide risk review apply as for any antidepressant start or dose increase.[1][2][3]
Special scenarios
Perioperative care. Coordinate with anaesthesia early. Avoid serotonergic opioids; plan holding and restart with washout awareness; do not assume the surgical team knows the MAOI list.[13][1]
Overdose. MAOI overdose can produce delayed severe toxicity — prolonged observation, supportive care, and interaction vigilance. This is an ED/toxicology interface, not a brief ED discharge without observation plans when significant ingestion is suspected.[12][14]
RIMA practice. Moclobemide meta-analysis supports efficacy comparable to TCAs with better average tolerability than older agents in that evidence set. Still counsel on high-tyramine extremes and serotonergic combinations; "safer diet" is not "no rules".[9][2]
Special populations
Older adults. Start very low; orthostasis and falls dominate risk; polypharmacy multiplies interaction chance.[2][1]
Youth. Limited evidence base for classic MAOIs; if ever considered, specialist setting with intensive monitoring — not routine CAMHS first-line.[16]
Pregnancy and lactation. Generally avoid classic MAOIs unless a perinatal specialist pathway judges residual benefit after failed safer options in severe TRD; untreated severe depression also harms. Coordinate obstetrics and perinatal psychiatry; never stop abruptly without a plan.[16][17]
Parkinson disease. Oral selegiline as MAO-B adjunct is a neurology dosing context distinct from antidepressant transdermal dosing for MDD — do not conflate in the viva.[2][7]
Prognosis and disposition
When used correctly in TRD or atypical depression, meaningful response is possible and historically under-offered. Continuation after response follows general antidepressant maintenance logic within a higher-intensity specialist follow-up model. Disposition should include written diet card, pharmacy alert, crisis contacts, and clear instructions for headache after restricted foods.[1][4][5][6]
Evidence, guidelines and regional deltas
RANZCP 2020 mood guidelines frame antidepressants within formulation-based stepped care and reserve complex biological pathways — including older agents — for appropriate severity and resistance. CANMAT 2016 and the 2023 update place pharmacological sequencing and TRD options in granular line tables widely used in exams; MAOIs appear as later or specialist options depending on the algorithm version and local availability. US practice retains phenelzine, tranylcypromine, isocarboxazid and selegiline patch (EMSAM) with product-specific diet labelling. Moclobemide availability is stronger in ANZ/Europe than in the US. Exam constant: washouts, tyramine literacy, and serotonergic combination bans travel better than any single formulary list.[16][17][18][1]
Exam pearls
- 2 / 5 / 2: ~2 weeks most antidepressants → MAOI; ~5 weeks after fluoxetine; ~2 weeks MAOI → SSRI/SNRI.[1][12]
- Pethidine + MAOI and tramadol + MAOI are automatic fail stems.[13]
- Atypical depression → phenelzine historical preferential response (Liebowitz).[4]
- Patch 6 mg/24 h diet exception teaching; 9–12 mg reintroduce diet; serotonergic drug bans at all doses.[7][8]
- Cheese reaction ≠ serotonin syndrome — different mechanism, different co-triggers, overlapping emergency urgency.[11][14]
- Written diet + pharmacy alert are part of the prescription.[1][11]
References
- [1]Van den Eynde V, Abdelmoemin WR, Abraham MM, et al. The prescriber's guide to classic MAO inhibitors (phenelzine, tranylcypromine, isocarboxazid) for treatment-resistant depression CNS Spectr, 2023.PMID 35837681
- [2]Shulman KI, Herrmann N, Walker SE Current place of monoamine oxidase inhibitors in the treatment of depression CNS Drugs, 2013.PMID 23934742
- [3]Fiedorowicz JG, Swartz KL The role of monoamine oxidase inhibitors in current psychiatric practice J Psychiatr Pract, 2004.PMID 15552546
- [4]Liebowitz MR, Quitkin FM, Stewart JW, et al. Antidepressant specificity in atypical depression Arch Gen Psychiatry, 1988.PMID 3276282
- [5]McGrath PJ, Stewart JW, Fava M, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report Am J Psychiatry, 2006.PMID 16946177
- [6]Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report Am J Psychiatry, 2006.PMID 17074942
- [7]Bodkin JA, Amsterdam JD Transdermal selegiline in major depression: a double-blind, placebo-controlled, parallel-group study in outpatients Am J Psychiatry, 2002.PMID 12411221
- [8]Amsterdam JD A double-blind, placebo-controlled trial of the safety and efficacy of selegiline transdermal system without dietary restrictions in patients with major depressive disorder J Clin Psychiatry, 2003.PMID 12633131
- [9]Lotufo-Neto F, Trivedi M, Thase ME Meta-analysis of the reversible inhibitors of monoamine oxidase type A moclobemide and brofaromine for the treatment of depression Neuropsychopharmacology, 1999.PMID 10063483
- [10]Walker SE, Shulman KI, Tailor SA, et al. Tyramine content of previously restricted foods in monoamine oxidase inhibitor diets J Clin Psychopharmacol, 1996.PMID 8889911
- [11]Van den Eynde V, Gillman PK, Blackwell BB The Prescriber's Guide to the MAOI Diet-Thinking Through Tyramine Troubles Psychopharmacol Bull, 2022.PMID 35721816
- [12]Gillman PK Advances pertaining to the pharmacology and interactions of irreversible nonselective monoamine oxidase inhibitors J Clin Psychopharmacol, 2011.PMID 21192146
- [13]Gillman PK Monoamine oxidase inhibitors, opioid analgesics and serotonin toxicity Br J Anaesth, 2005.PMID 16051647
- [14]Boyer EW, Shannon M The serotonin syndrome N Engl J Med, 2005.PMID 15784664
- [15]Dunkley EJ, Isbister GK, Sibbritt D, et al. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity QJM, 2003.PMID 12925718
- [16]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [17]Kennedy SH, Lam RW, McIntyre RS, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments Can J Psychiatry, 2016.PMID 27486148
- [18]Lam RW, Kennedy SH, Adams C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder Can J Psychiatry, 2024.PMID 38711351