Psych · Psychopharmacology — metabolic syndrome and psychotropic monitoring
Metabolic syndrome and psychotropic monitoring
Also known as Antipsychotic metabolic monitoring · Cardiometabolic risk psychotropics · ADA APA antipsychotic monitoring · Antipsychotic weight gain · Metabolic syndrome schizophrenia · Clozapine olanzapine diabetes risk
Exam-exhaustive fellowship reference on metabolic syndrome and psychotropic monitoring — NCEP/IDF criteria, agent ranking by cardiometabolic liability, ADA/APA monitoring schedule, mechanisms, switch and metformin strategies, youth risk, CATIE/Correll/De Hert evidence, and RANZCP/NICE/APA physical-health expectations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
People with severe mental illness die years earlier than peers, largely from cardiovascular and metabolic disease rather than only suicide. Antipsychotics — especially second-generation agents with high histaminergic and serotonergic off-target burden — accelerate weight gain, insulin resistance, dyslipidaemia and hypertension. Fellowship exams test whether you can define metabolic syndrome, rank agents, monitor like an internist who also understands psychosis, and intervene early without therapeutic nihilism about needed medicines.[8][9][11][12]
Definition and classification
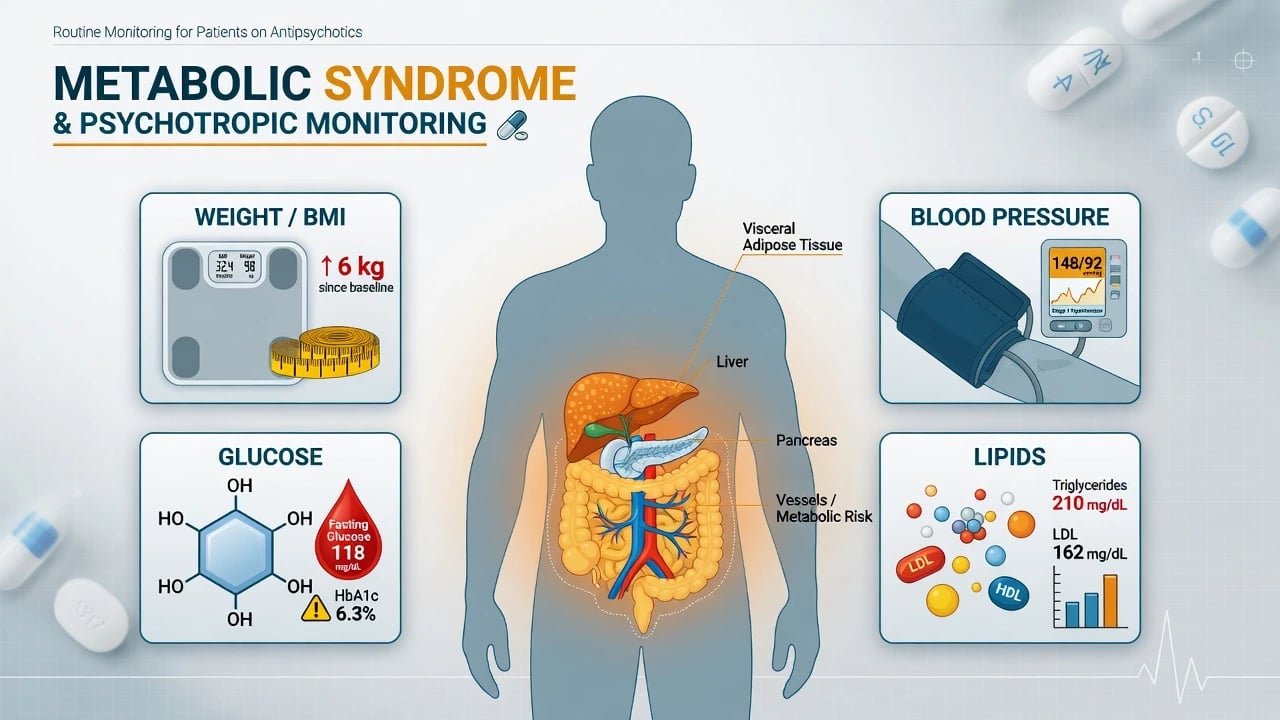
Metabolic syndrome (MetS) is a clustering of central adiposity, dysglycaemia, atherogenic lipids and elevated blood pressure that multiplies atherosclerotic cardiovascular risk. Two frameworks dominate viva answers.[19][11]
- NCEP ATP III–style teaching: three or more of elevated waist circumference (population-specific cut-offs), triglycerides ≥1.7 mmol/L (150 mg/dL), low HDL-C, elevated blood pressure, and elevated fasting glucose — examiners want the cluster concept even when exact SI conversions are table-looked-up.[19]
- IDF: central obesity (ethnicity-specific waist) as a required entry criterion plus two additional factors — useful when the stem emphasises waist as the visceral driver.[19]
Psychotropic metabolic adverse effect is not identical to MetS: a patient can gain 8 kg without yet meeting MetS criteria, and can develop early hyperglycaemia with modest weight change on olanzapine or clozapine.[4][8]
Agent ranking (must-know hierarchy)
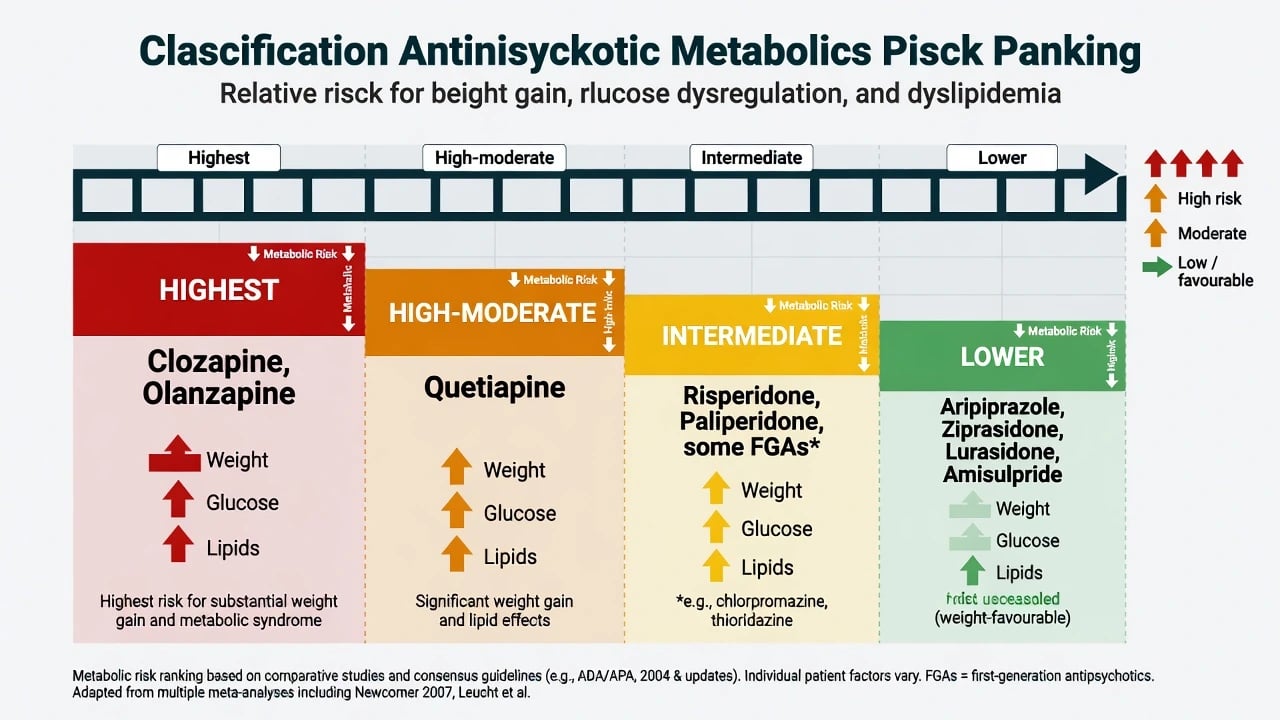
Relative metabolic liability for exams (individuals still vary; monitoring remains mandatory on lower-tier agents too).[3][13][14]
| Tier | Typical agents | Exam emphasis |
|---|---|---|
| Highest | Clozapine, olanzapine | Largest mean weight gain; strong diabetes/dyslipidaemia signals |
| High–moderate | Quetiapine | Meaningful weight and metabolic effects; dose and duration matter |
| Intermediate | Risperidone, paliperidone; some low-potency FGAs (e.g. chlorpromazine) | Intermediate weight; still monitor |
| Lower (weight-favourable) | Aripiprazole, ziprasidone, lurasidone; amisulpride relatively favourable for weight in many datasets | Prefer when efficacy allows; not zero risk |
| Relative ranking above synthesises comparative weight and metabolic data — not an absolute safety guarantee for any single agent.[3][13][14][20] |
Allison’s synthesis established large differences between agents in mean weight change; head-to-head and network analyses reinforce clozapine/olanzapine at the top of metabolic harm and partial agonists or selected SGAs lower for weight.[3][13][14][20]
Mood stabilisers and antidepressants matter secondarily: lithium and valproate contribute weight; mirtazapine and some TCAs and paroxetine add appetite weight — but SGA ranking remains the core viva spine for MetS stems.[8]
Epidemiology and risk
Meta-analyses show substantially higher MetS prevalence in schizophrenia-spectrum illness (and elevated rates in bipolar and major depression) than general-population baselines, with waist, lipids and glucose components all over-represented.[11][12] Excess mortality in SMI is heavily cardiometabolic. Under-monitoring remains common: guidelines exist, implementation fails — a De Hert system-level point examiners love.[9][10]
Youth first exposure is a special risk band: Correll and colleagues showed large early weight and metabolic parameter shifts during first-time SGA use in children and adolescents — do not wait for adult-style “annual checks” alone.[7]
Pathophysiology
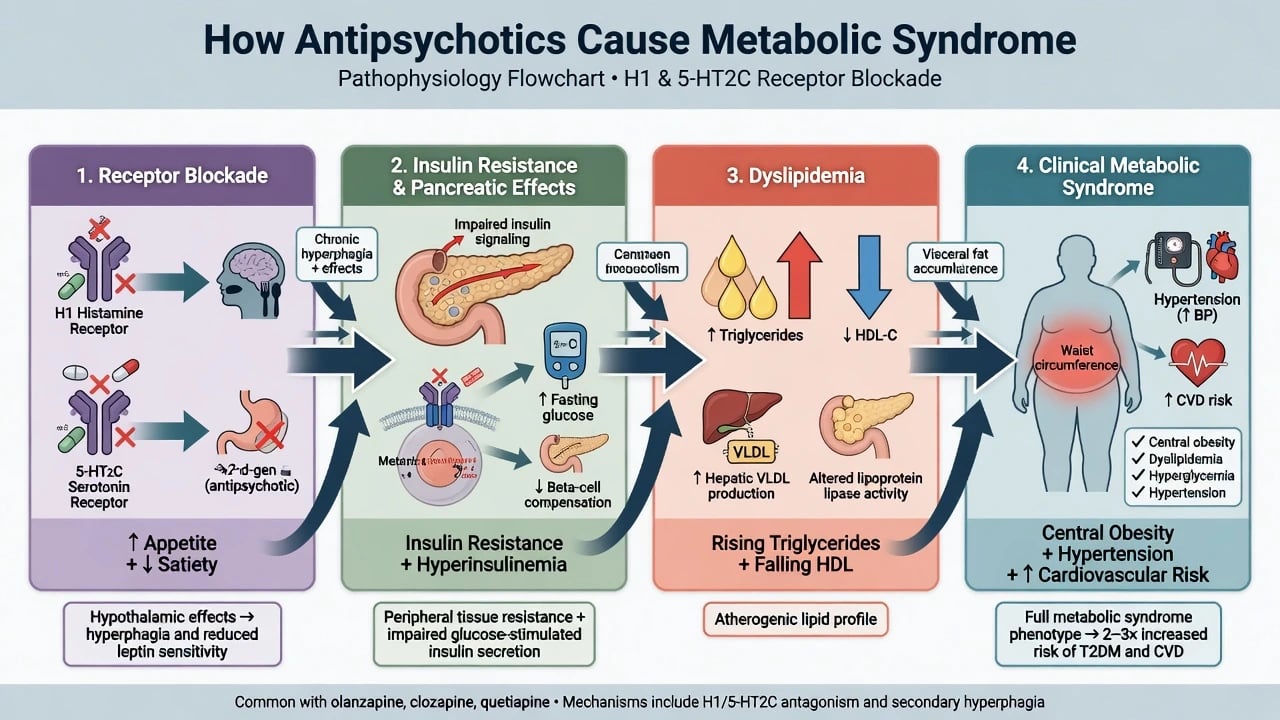
Mechanisms are multi-hit (receptor, insulin, lipid and lifestyle pathways).[4][8]
- Appetite and satiety: H1 and 5-HT2C antagonism increase hunger and reduce satiety signalling; sedation reduces activity energy expenditure.[4][8]
- Insulin resistance: high-risk SGAs associate with reduced insulin sensitivity; some data support direct effects on glucose regulation beyond kilograms alone.[4][8]
- Lipids: triglycerides rise and HDL falls in an atherogenic pattern, sometimes early.[4][6]
- Blood pressure and CVD: weight, sodium retention context, autonomic effects and lifestyle (smoking, diet, inactivity) stack risk.[8][12]
Lifestyle does not replace pharmacology — it multiplies or mitigates drug risk. Smoking cessation is cardiovascular gold but can change antipsychotic levels (see interactions topic for CYP1A2/clozapine).[8]
Clinical presentation and differential
Early metabolic harm is silent. The first signal is often the scale and waist tape, not thirst. Late diabetes clues (polyuria, polydipsia, blurred vision, infections) mean you are already late.[1][4]
Differential for weight/glucose change: primary obesity trajectory, binge-eating disorder, steroids, hypothyroidism, fluid retention, alcohol, non-adherence to diabetes treatment, and illness-related lifestyle collapse after psychosis. Do not auto-blame the tablet without a timeline linking drug start/dose rise to trajectory.[8]
Assessment before first dose
Document a cardiometabolic baseline package before the first dose of a higher-risk psychotropic.[1][2]
- Weight, BMI, waist circumference (correct plane)[1]
- Blood pressure[1]
- Fasting glucose and/or HbA1c[1]
- Fasting lipids[1]
- Personal/family history of diabetes and premature CVD[1]
- Smoking, diet, activity, sleep[2]
- Pregnancy potential; ethnicity-linked diabetes risk[2]
- Current psychotropic polypharmacy[2]
This package is the ADA/APA consensus and Marder physical-health monitoring spine translated into clinic language.[1][2]
Risk-stratify: planned high-tier agent, youth, prior rapid gain, family diabetes, Indigenous or other high-prevalence groups, intellectual disability with environmental diet risk.[7][9]
Investigations and monitoring schedule
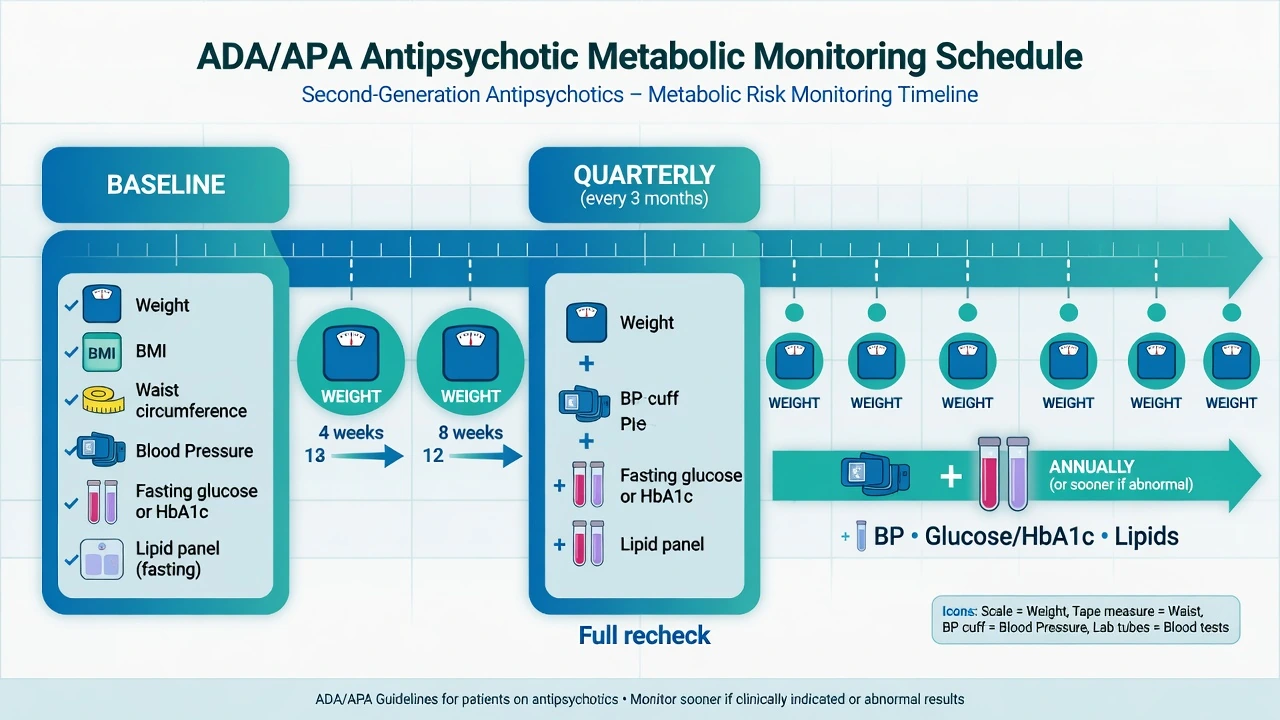
ADA/APA 2004 consensus schedule (exam skeleton): baseline package, early serial weight, then structured glucose/lipid/BP rechecks.[1][2]
| Parameter | Baseline | 4 weeks | 8 weeks | 12 weeks | Quarterly | Annually |
|---|---|---|---|---|---|---|
| Personal/family history | Yes | Review | ||||
| Weight (BMI) | Yes | Yes | Yes | Yes | Yes | Yes |
| Waist | Yes | Yes | Yes | |||
| Blood pressure | Yes | Yes | Yes | |||
| Fasting glucose / HbA1c | Yes | Yes | Yes | |||
| Fasting lipids | Yes | Yes | Yes | |||
| Teaching schedule above follows the ADA/APA consensus skeleton used in fellowship exams; recheck sooner if trajectory is adverse.[1][2] |
Weight is deliberately frequent early because the first 12 weeks set the trajectory. Recheck glucose and lipids sooner if rapid weight gain, symptoms, or high-risk agent. Local forms differ; the principle of structured baseline plus early serial weight is constant across RANZCP-aligned, NICE and APA physical-health expectations.[1][2][10]
ECG belongs to cardiac safety (QTc topic), not as a substitute for metabolic labs.[2]
ANZ (RANZCP-aligned care): cardiometabolic monitoring embedded in routine psychosis and SGA care; shared care with GPs common — the psychiatrist still owns the plan and escalation. UK (NICE-style): hard-wired physical health checks in serious mental illness pathways. US (APA practice): measurement-based care and ADA-linked diabetes standards for treatment of identified diabetes. Thresholds and paperwork differ; abandonment of monitoring does not.[1][2][9][10]
Acute / emergency metabolic management
Psychosis still needs treatment: plan a lower-metabolic alternative or intensive management if clozapine is indispensable.[5][17]
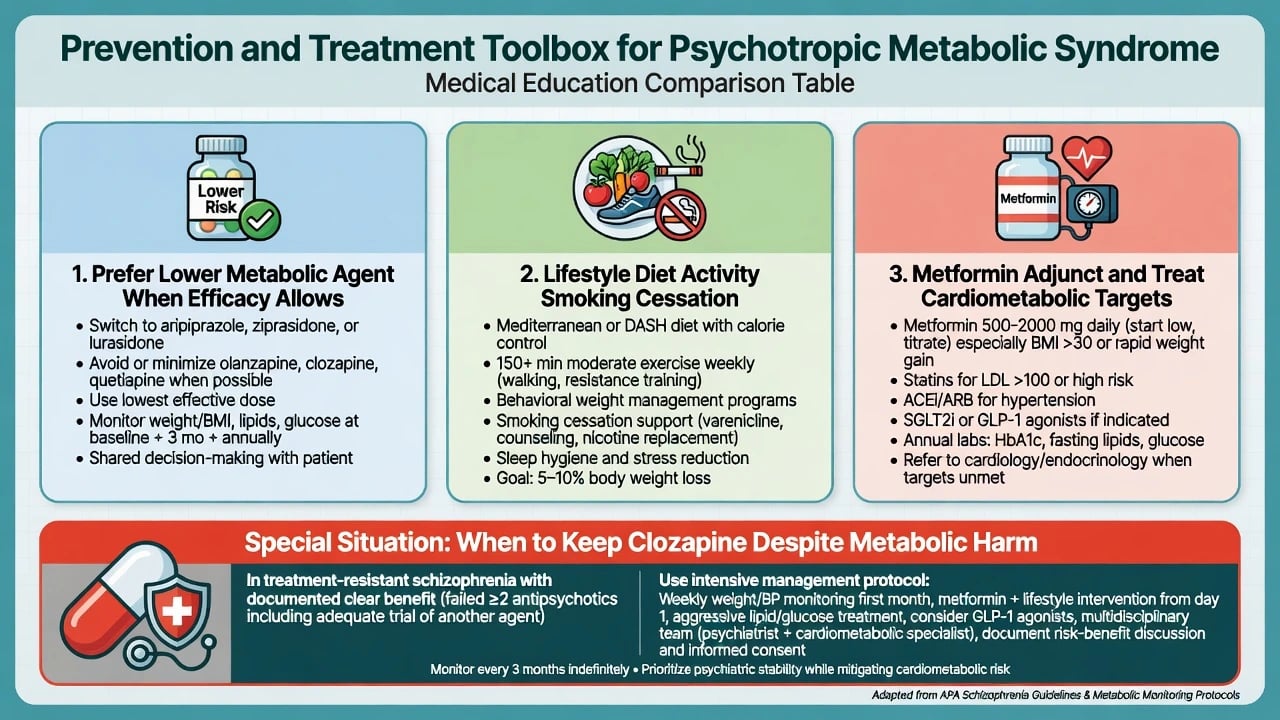
Definitive management algorithm
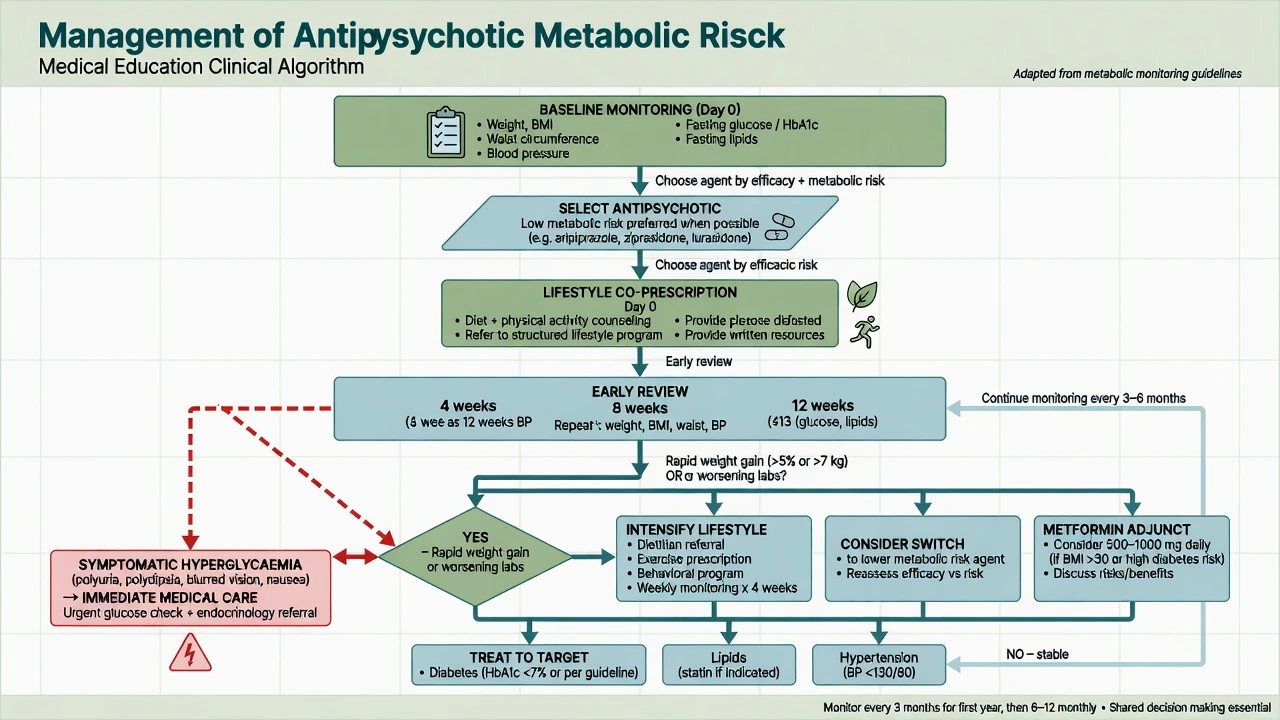
1. Primary prevention (day 0)
- Prefer a lower-metabolic agent when efficacy allows (shared decision in FEP is the classic setting).[18][20]
- Co-prescribe lifestyle: diet quality, calorie awareness, activity, sleep, smoking cessation support — not a pamphlet after 15 kg.[15][9]
- Avoid unjustified dual high-metabolic antipsychotics.[8]
2. Early secondary prevention (weeks 4–12)
Action triggers used in exams and practice include early substantial weight gain and new lab abnormalities.[1][15]
- Rapid weight gain (commonly taught as ≥5% early, or clearly adverse trajectory; trial literature often reports ≥7% as a categorical threshold)[1][3]
- New prediabetes/diabetes labs or sharp lipid rise[1][4]
- New hypertension[1][8]
Options (combine as needed): intensify lifestyle; switch to a lower-liability agent when psychiatric status allows (e.g. olanzapine → aripiprazole switch data show metabolic benefit potential); add metformin where evidence and safety allow; treat BP/lipids/glucose to medical targets with GP/endocrinology.[15][16][17]
3. Metformin (fellowship dose language)
Evidence supports metformin for antipsychotic-associated weight gain as an adjunct to lifestyle and agent choice.[15][16]
- Wu et al. (JAMA 2008): lifestyle plus metformin outperformed either alone in antipsychotic-induced weight gain.[15]
- Jarskog et al. (METS; Am J Psychiatry 2013): metformin produced greater weight loss and metabolic improvement vs placebo in overweight outpatients with schizophrenia-spectrum illness.[16]
Practical adult teaching band (always check local product information, eGFR, contraindications): start metformin 500 mg orally once or twice daily with food, titrate toward 1000–2000 mg/day in divided doses as tolerated if eGFR allows; hold or avoid in significant renal impairment, decompensated heart failure, acute illness with lactic acidosis risk, and heavy alcohol use; counsel GI effects; monitor B12 with long-term use in line with diabetes practice. Metformin is an adjunct, not a licence to ignore agent choice.[15][16]
4. Treat the syndrome, not only the psychiatry note
Diabetes, lipids and hypertension are treated to the same cardiometabolic standards as in non-psychiatric patients, with attention to adherence and diagnostic overshadowing.[1][9]
5. When not to abandon clozapine
Clozapine remains uniquely effective in treatment-resistant schizophrenia. Metabolic harm is managed intensively (monitoring, lifestyle, metformin, cardiometabolic drugs, possible partial agonist adjunct strategies in selected practice) rather than automatic cessation that risks relapse, violence or suicide. Document shared decision.[5][8][16]
Prefer lower-risk agent
- FEP when efficacy comparable
- Prior severe metabolic harm
- High baseline diabetes risk
- Still monitor after switch
Lifestyle from day 0
- Diet and activity plan
- Smoking cessation support
- Sleep and structured routine
- Family/environment engagement
Metformin and medical Rx
- Evidence in AP weight gain
- Renal/GI safety checks
- Treat BP, lipids, diabetes
- Endocrine/GP co-management
Keep clozapine if TRS
- Unique efficacy context
- Intensive monitoring
- Do not casual-stop
- Shared decision documented
Landmark evidence (name the papers)
| Source | Exam takeaway |
|---|---|
| ADA/APA consensus 2004 | Monitoring table skeleton still quoted worldwide |
| Marder 2004 | Physical health monitoring package for schizophrenia |
| Allison 1999 | Quantitative weight-gain differences across agents |
| CATIE (Lieberman 2005) + metabolic analyses | Effectiveness trade-offs; olanzapine efficacy vs metabolic cost |
| EUFEST (Kahn 2008) | FEP effectiveness/discontinuation context across agents |
| Correll 2009 JAMA | Large early cardiometabolic shifts in youth first SGA use |
| Rummel-Kluge 2010; Bak 2014; Huhn/Leucht NMA 2019 | Head-to-head and network metabolic/tolerability ranking |
| De Hert reviews/guidelines | CVD mechanisms, barriers, monitoring quality |
| Mitchell 2013; Vancampfort 2015 | MetS prevalence magnitude in SMI |
| Wu 2008; Jarskog 2013; Newcomer switch 2008 | Lifestyle, metformin, and switch as interventions |
Special populations
Children and adolescents. Highest relative early gain; family-based lifestyle; prefer lower-metabolic agents when appropriate; denser early weight checks than adult annual myths allow.[7]
Older adults. Diabetes, sarcopenic obesity, polypharmacy, fall risk from antihypertensives; start low, monitor BP and glucose carefully.[8]
Pregnancy. Some antipsychotics associate with gestational diabetes risk signals; coordinate obstetric medicine; untreated psychosis also harms mother and fetus (see pregnancy psychopharmacology topic).[8]
Intellectual disability. Capacity, consent, group-home diet, higher support needs for blood draws and lifestyle change.[9]
High diabetes-prevalence ethnic groups and Indigenous peoples. Lower threshold for intensive monitoring and early action; culturally safe lifestyle programmes.[9][12]
Prognosis and disposition
Early weight trajectory predicts longer-term gain — the first quarter is the intervention window.[1][7] Disposition: written shared-care plan naming who orders which labs, review dates, and escalation thresholds; involve GP, diabetes services and dietetics early rather than after myocardial infarction.[9][10]
Exam pearls
WATCH the metabolic prescription
WATCH
References
- [1]American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity Consensus development conference on antipsychotic drugs and obesity and diabetes Diabetes Care, 2004.PMID 14747245
- [2]Marder SR, Essock SM, Miller AL, et al. Physical health monitoring of patients with schizophrenia Am J Psychiatry, 2004.PMID 15285957
- [3]Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis Am J Psychiatry, 1999.PMID 10553730
- [4]Newcomer JW, Haupt DW The metabolic effects of antipsychotic medications Can J Psychiatry, 2006.PMID 16933585
- [5]Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia N Engl J Med, 2005.PMID 16172203
- [6]Nasrallah HA Metabolic findings from the CATIE trial and their relation to tolerability CNS Spectr, 2006.PMID 16816798
- [7]Correll CU, Manu P, Olshanskiy V, et al. Cardiometabolic risk of second-generation antipsychotic medications during first-time use in children and adolescents JAMA, 2009.PMID 19861668
- [8]De Hert M, Detraux J, van Winkel R, et al. Metabolic and cardiovascular adverse effects associated with antipsychotic drugs Nat Rev Endocrinol, 2011.PMID 22009159
- [9]De Hert M, Cohen D, Bobes J, et al. Physical illness in patients with severe mental disorders. II. Barriers to care, monitoring and treatment guidelines, plus recommendations at the system and individual level World Psychiatry, 2011.PMID 21633691
- [10]De Hert M, Vancampfort D, Correll CU, et al. Guidelines for screening and monitoring of cardiometabolic risk in schizophrenia: systematic evaluation Br J Psychiatry, 2011.PMID 21804146
- [11]Mitchell AJ, Vancampfort D, Sweers K, et al. Prevalence of metabolic syndrome and metabolic abnormalities in schizophrenia and related disorders—a systematic review and meta-analysis Schizophr Bull, 2013.PMID 22207632
- [12]Vancampfort D, Stubbs B, Mitchell AJ, et al. Risk of metabolic syndrome and its components in people with schizophrenia and related psychotic disorders, bipolar disorder and major depressive disorder: a systematic review and meta-analysis World Psychiatry, 2015.PMID 26407790
- [13]Rummel-Kluge C, Komossa K, Schwarz S, et al. Head-to-head comparisons of metabolic side effects of second generation antipsychotics in the treatment of schizophrenia: a systematic review and meta-analysis Schizophr Res, 2010.PMID 20692814
- [14]Bak M, Fransen A, Janssen J, et al. Almost all antipsychotics result in weight gain: a meta-analysis PLoS One, 2014.PMID 24763306
- [15]Wu RR, Zhao JP, Jin H, et al. Lifestyle intervention and metformin for treatment of antipsychotic-induced weight gain: a randomized controlled trial JAMA, 2008.PMID 18182600
- [16]Jarskog LF, Hamer RM, Catellier DJ, et al. Metformin for weight loss and metabolic control in overweight outpatients with schizophrenia and schizoaffective disorder Am J Psychiatry, 2013.PMID 23846733
- [17]Newcomer JW, Campos JA, Marcus RN, et al. A multicenter, randomized, double-blind study of the effects of aripiprazole in overweight subjects with schizophrenia or schizoaffective disorder switched from olanzapine J Clin Psychiatry, 2008.PMID 18605811
- [18]Kahn RS, Fleischhacker WW, Boter H, et al. Effectiveness of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: an open randomised clinical trial Lancet, 2008.PMID 18374841
- [19]Alberti KG, Zimmet P, Shaw J Metabolic syndrome—a new world-wide definition. A Consensus Statement from the International Diabetes Federation Diabet Med, 2006.PMID 16681555
- [20]Huhn M, Nikolakopoulou A, Schneider-Thoma J, et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis Lancet, 2019.PMID 31303314