Psych · Psychopharmacology — atypical and multimodal antidepressants
Mirtazapine, bupropion and multimodal antidepressants
Also known as NaSSA · NDRI · Remeron · Wellbutrin · Zyban · Vortioxetine · Vilazodone · Agomelatine · California rocket fuel · Multimodal antidepressants
Exam-exhaustive fellowship pharmacology of mirtazapine (NaSSA), bupropion (NDRI) and multimodal agents (vortioxetine, vilazodone, agomelatine) — mechanisms, adult oral doses, sexual-function and smoking niches, seizure risk, STAR*D/CO-MED combination evidence, and RANZCP/CANMAT practice frames. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
These agents are the fellowship bridge between “first-line SSRI/SNRI” answers and true TRD pathways. Examiners want mechanism labels, phenotype matching, doses with monitoring, seizure and metabolic safety, and the difference between clever combination pharmacology and CO-MED-style over-combination from day one.[8][10][15][16]
Definition and classification
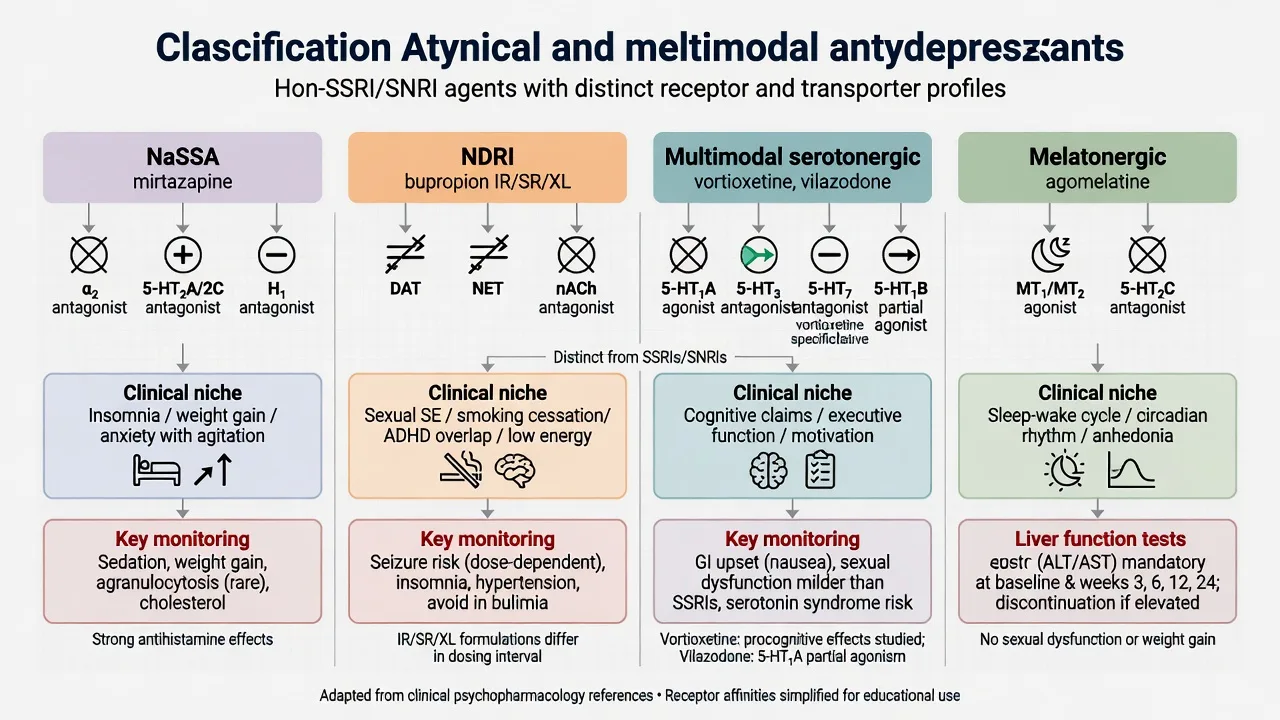
| Class label | Core agents | Primary mechanism line | Exam niches |
|---|---|---|---|
| NaSSA | Mirtazapine | α2 auto/hetero-receptor antagonism; 5-HT2/5-HT3 antagonism; H1 antagonism | Insomnia, anorexia, SSRI sexual intolerance, combination strategies |
| NDRI | Bupropion (IR/SR/XL) | NET and DAT reuptake inhibition; nAChR antagonism (smoking) | Fatigue phenotype, sexual SE, smoking cessation, SSRI switch/augment |
| Multimodal SERT+ | Vortioxetine | SERT inhibition plus multi-5-HT receptor modulation | MDD with cognitive residual symptom marketing; ordinary AD trial rules |
| SPARI-type | Vilazodone | SERT inhibition + 5-HT1A partial agonism | MDD where available; GI SE and food-with-dose teaching |
| Melatonergic | Agomelatine | MT1/MT2 agonism + 5-HT2C antagonism | MDD/sleep-wake narrative; LFT monitoring; regional availability |
| Do not call mirtazapine an SSRI. Do not call bupropion “serotonergic dual action.” Multimodal is a receptor-profile marketing category, not a licence to skip bipolar screen or early suicide review.[1][10][14][15] |
Mechanisms — the viva core
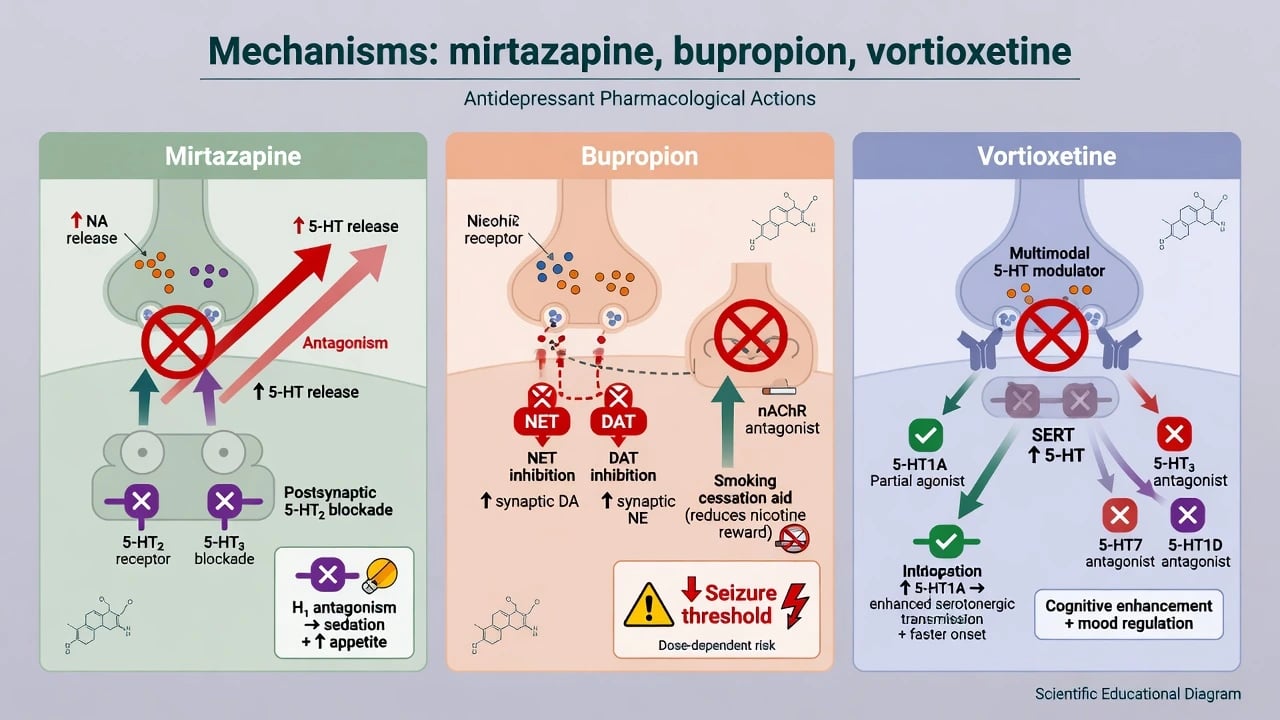
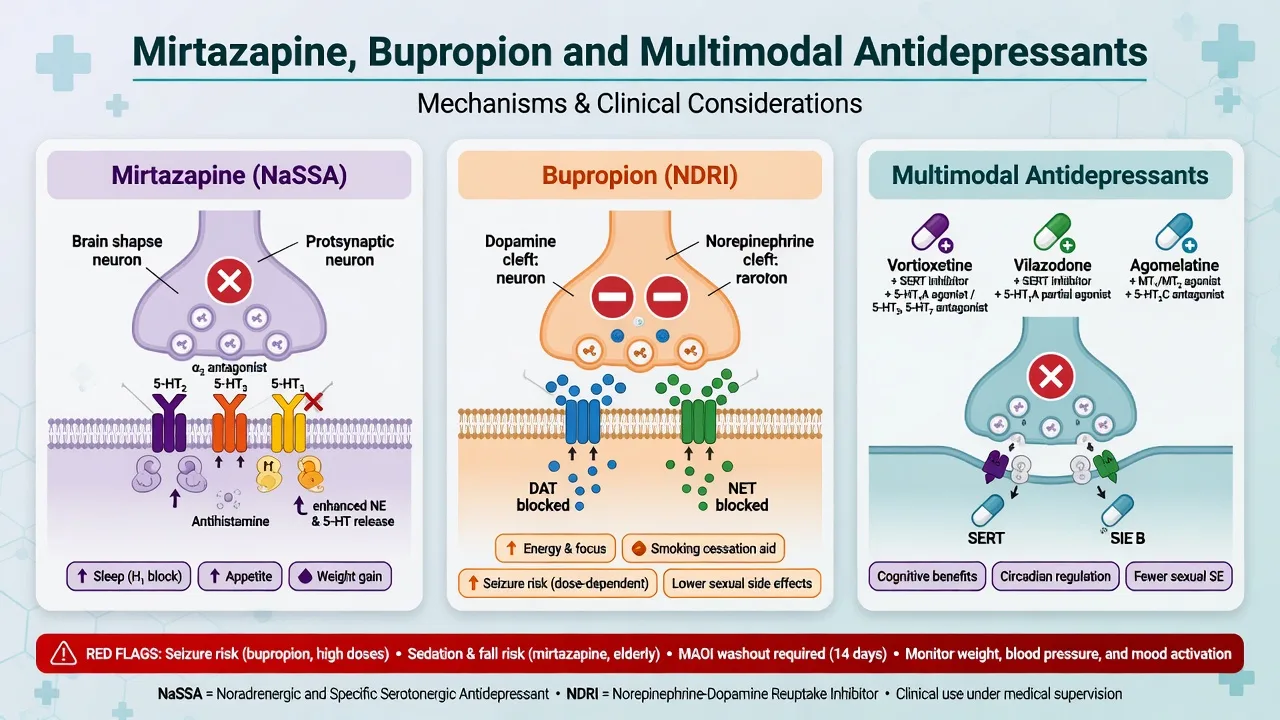
Mirtazapine (NaSSA). de Boer’s pharmacologic profile frames mirtazapine as enhancing noradrenergic and serotonergic transmission via blockade of central α2-adrenergic auto- and heteroreceptors, with additional 5-HT2 and 5-HT3 antagonism that steers the side-effect map away from classic SSRI sexual/GI patterns and toward histamine H1–linked sedation and appetite increase.[1] Exam translation: useful when the depressive syndrome includes insomnia and poor intake; risky when obesity, sleep apnoea, or fall risk dominate.
Bupropion (NDRI). Clinical experience syntheses emphasise NET/DAT activity with minimal serotonergic reuptake — the mechanistic reason sexual dysfunction and SSRI-like GI packages are less prominent — plus development from IR to SR to XL to smooth peaks and adherence.[10] nAChR antagonism underpins the smoking-cessation indication demonstrated in controlled trials of sustained-release bupropion with or without nicotine patch.[12]
Multimodal agents. Vortioxetine combines SERT inhibition with 5-HT receptor modulation; randomised data support antidepressant efficacy and a cognitive-function signal in depressed adults, which examiners accept as possible differentiator, not proof of a dementia drug.[14] Vilazodone is taught as SERT + 5-HT1A partial agonism (SPARI-type). Agomelatine is the melatonergic/5-HT2C story with sleep–wake marketing and hepatic monitoring where licensed.
Epidemiology and risk context
These drugs sit among widely used second-generation antidepressants. Cipriani’s 2018 network meta-analysis of 21 antidepressants keeps the class honest: efficacy differences are modest, while acceptability and side-effect fingerprints drive real-world choice — mirtazapine often appears in higher efficacy/acceptability bands in NMA league tables, which is not a licence to ignore weight gain.[15]
Risk language for exams clusters as:
- Bupropion seizures — dose- and risk-factor dependent; classic review literature and modern formulation history both matter.[11][10]
- Mirtazapine metabolic/sedation burden — weight, daytime somnolence, falls.
- Sexual function — relative advantage for bupropion versus many serotonergic agents in head-to-head sexual-function endpoints.[13]
- Combination intensity — rocket-fuel and late STAR*D steps are specialist pathways with low absolute remission yields.[7][8]
Named evidence anchors
When to choose which agent
RANZCP mood-disorder guidance frames antidepressant choice within formulation-based stepped care: prior response, comorbidity, tolerability priorities and risk — not brand loyalty.[16]
Choose mirtazapine when insomnia, anorexia/weight loss, nausea on SSRIs, or need for a non-SERT-primary agent dominate, and when weight gain/sedation are acceptable trade-offs. Benkert’s comparison with paroxetine supports antidepressant efficacy in major depression with a different tolerability fingerprint.[2][16]
Choose bupropion when sexual dysfunction, smoking, hypersomnia/fatigue phenotype, or SSRI nonresponse switch logic applies — after excluding high seizure-risk contexts.[4][12][13]
Consider multimodal agents when formulary access exists and residual cognitive complaints (vortioxetine discussion), SPARI marketing interest (vilazodone), or melatonergic sleep–wake framing (agomelatine) matter to the patient — still run an adequate trial and safety plan.[14][15]
Do not choose any of these to treat bipolar I depressive syndromes as if unipolar, to avoid monitoring, or to “stack cleverly” at first presentation contrary to CO-MED lessons.[8][16]
Agent-level doses (adult oral exam frameworks)
Ranges are orientation anchors for exams. Check current product information, renal/hepatic labels, and local formulary rules; start lower in older or frail patients.[10][16]
| Agent | Typical start | Usual range / notes | Killer monitoring |
|---|---|---|---|
| Mirtazapine | 15 mg orally nocte ( 7.5–15 mg frail/older) | 15–45 mg nocte; ODT option for adherence | Sedation, weight, falls; rare blood dyscrasia teaching |
| Bupropion XL | 150 mg orally once daily | After several days, 300 mg daily if tolerated; labelled max often 450 mg with caution | Seizure risk factors; activation/insomnia; BP |
| Bupropion SR | Divided dosing historically (e.g. 150 mg twice daily band) | Smoking-cessation programmes often used SR | Same seizure rules; adherence complexity vs XL |
| Vortioxetine | 5–10 mg orally daily | 10–20 mg daily usual antidepressant band | Nausea; cognitive claim humility |
| Vilazodone | Low start then titrate (commonly toward 20–40 mg) | Take with food per product teaching | GI SE; serotonergic stack literacy |
| Agomelatine (where available) | 25 mg nocte | May increase to 50 mg | LFTs at baseline and on label schedule |
| Adult dose frameworks above are exam orientation anchors drawn from clinical experience syntheses, comparative trials and guideline stepped-care teaching — always re-check current product information before prescribe.[2][10][14][16] |
Landmark evidence every candidate must own
STAR*D Level 2 switch. After SSRI (citalopram) failure, switching to bupropion-SR, sertraline or venlafaxine-XR produced broadly similar remission rates — choose by comorbidity and tolerability, not mythology that one switch always wins.[4]
STAR*D Level 2 augmentation. Adding bupropion-SR versus buspirone after incomplete SSRI response is the classic “augment with NDRI” exam stem; know that both strategies are legitimate measurement-based options with different side-effect drivers.[5]
STAR*D Level 3 mirtazapine. After two failed treatments, mirtazapine versus nortriptyline is a named late-step comparison with limited absolute yields — humility about sequential pharmacotherapy is the point.[6]
STAR*D Level 4 “rocket fuel.” Venlafaxine plus mirtazapine versus tranylcypromine after three failures: low remission, high intensity — not a casual outpatient hobby combination.[7]
CO-MED. Single-blind randomised comparison of combination antidepressant strategies from treatment initiation versus escitalopram-based monotherapy pathways did not justify routine first-step dual antidepressant therapy for all-comers.[8]
Blier combination from initiation. Mechanistic and clinical combination work (mirtazapine with paroxetine from the start) fuels the physiological rationale for combinations in selected patients — still interpret beside CO-MED population results, not instead of them.[9]
Carpenter augmentation. Placebo-controlled mirtazapine augmentation of ongoing antidepressant supports the “add NaSSA” move in partial responders.[3]
Sexual function and smoking. Thase/Clayton bupropion XL versus venlafaxine XR shows sexual-function advantages with comparable antidepressant efficacy framing; Jorenby establishes bupropion SR smoking-cessation efficacy with/without patch.[13][12]
Vortioxetine cognition. McIntyre’s RCT is the named cognitive-function citation — cite it, then refuse magic thinking.[14]
Selection algorithm and monitoring
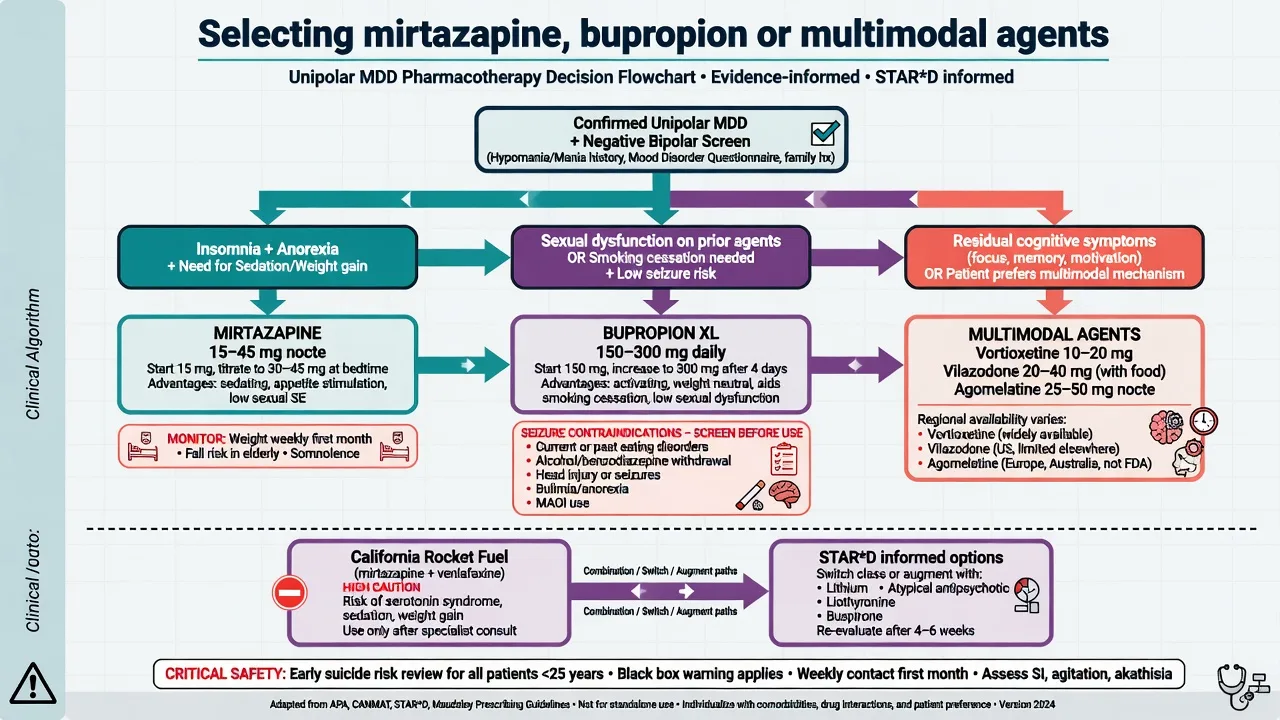
Before first dose (document): unipolar vs bipolar/mixed screen; suicide risk and means; sexual function; sleep and appetite targets; smoking status; seizure history, eating-disorder history, alcohol/benzo withdrawal risk if bupropion; falls/obesity/sleep apnoea if mirtazapine; pregnancy potential; full drug list (MAOI washouts, other pro-seizure agents); baseline weight; LFTs if agomelatine planned.[10][11][16]
Early follow-up: days to 2 weeks for sedation or activation, insomnia, anxiety, suicidality (especially under 25 and after dose increases); then efficacy at 2–4–6 weeks.[16]
Maintenance. Continuation after response reduces relapse risk for antidepressants as a class; plan duration by episode number and residual symptoms; taper thoughtfully rather than stop cold when serotonergic multimodal agents or combinations are involved.[15][16]
RANZCP 2020 anchors ANZ stepped mood care. CANMAT pharmacological sections (and later updates) are widely used in exams for first-line agent lists that include mirtazapine and bupropion among options depending on edition and indication nuance. NICE stepped care emphasises psychological therapy access and review intensity. US practice emphasises product labels (bupropion seizure warnings; vilazodone/vortioxetine brands) and measurement-based care. Agomelatine availability is region-specific — know the mechanism and LFT story even if your local formulary lacks it.[16][15]
Adverse effects and emergencies
Mirtazapine
- Sedation, increased appetite, weight gain
- Dry mouth, constipation
- Falls risk in older adults
- Rare agranulocytosis teaching — investigate unexplained fever/sore throat
Bupropion
- Insomnia, activation, anxiety, tremor
- Dose-related seizure risk
- Contraindication/caution: eating disorders, withdrawal states, prior seizures
- Lower sexual dysfunction vs many serotonergic ADs
Multimodal
- Vortioxetine: nausea common early
- Vilazodone: GI SE; food with dose
- Agomelatine: LFT monitoring
- Serotonergic stack / MAOI rules still apply
Combinations
- Rocket fuel = intensity + monitoring
- CO-MED: not routine day-1 dual AD
- Watch BP if SNRI involved
- Do not combine with MAOI
Seizure risk (bupropion)
Davidson’s review crystallises the clinical message that seizures are the defining serious risk of bupropion, historically more visible with higher IR peaks and dose escalation; modern SR/XL use lowers but does not erase risk, especially when absolute contraindications are ignored.[11][10] Exam checklist before prescribe: prior seizure, CNS tumour, abrupt alcohol/sedative withdrawal, current anorexia/bulimia, dose above labelled maximum, interacting pro-seizure drugs.
Sexual dysfunction contrast
Montejo-level class sexual dysfunction rates make SSRI/SNRI problems examinable; bupropion’s relative advantage appears in dedicated sexual-function trials against venlafaxine XR and in clinical switching/antidote strategies after SSRI-induced sexual dysfunction.[13][15] Mirtazapine is often relatively favourable on sexual function because of 5-HT2 antagonism, but do not promise zero risk.
Toxicity and overdose
Bupropion overdose can present with seizures, tachycardia and altered mental status — supportive care and seizure control dominate. Mirtazapine overdose is usually less cardiotoxic than TCAs but still requires medical assessment. Serotonin toxicity is primarily a stacked serotonergic problem (including multimodal SERT agents and mirtazapine combinations with MAOIs), not a pure bupropion story.[10][16]
Switching, combinations and scenarios
SSRI failure → bupropion switch: STAR*D Level 2 supports bupropion-SR as one equal option beside sertraline and venlafaxine-XR.[4]
Partial SSRI response → bupropion augment: STAR*D Level 2 augmentation arm is the named pathway.[5]
Partial response → mirtazapine add-on: Carpenter placebo-controlled augmentation and Blier combination physiology support selected dual therapy after partial response — document targets and stop rules.[3][9]
Late TRD: STAR*D Level 3 mirtazapine versus nortriptyline and Level 4 venlafaxine+mirtazapine versus MAOI teach diminishing returns and the need to escalate to lithium/atypical/neuromodulation frameworks rather than endless dual AD stacking alone.[6][7][16]
Smoking cessation: Bupropion SR with behavioural support ± nicotine patch is evidence-based; screen psychiatric status and seizure risk before Zyban-style use.[12]
Sexual dysfunction on SSRI: Switch to bupropion or carefully add bupropion; discuss alternatives including mirtazapine switch depending on sleep/weight priorities.[13]
Special populations
Older adults. Start mirtazapine 7.5–15 mg nocte; prioritise falls, hyponatraemia if combined with SSRI, and metabolic effects. Bupropion may activate or disturb sleep; seizure threshold and drug interactions still apply.[16]
Youth. Class antidepressant suicidality monitoring applies; these agents are less often first-line than fluoxetine pathways in many paediatric frameworks — specialist territory.[16]
Pregnancy and lactation. Individualised perinatal risk–benefit; untreated depression harms mother and fetus; avoid abrupt unsupervised stops of effective regimens.[16]
Epilepsy and eating disorders. Prefer non-bupropion options when seizure risk is material. Eating disorders are a classic bupropion red flag.[11]
Hepatic disease. Agomelatine demands LFT literacy where used; other agents need label-based caution in severe hepatic impairment.[16]
Prognosis and disposition
Target remission, not mere response. Residual insomnia may still justify mirtazapine even when mood partially improves; residual anorgasmia may justify bupropion strategy even when PHQ improves. After nonresponse to optimised trials, move deliberately through switch/augment/combination/neuromodulation rather than random polypharmacy.[4][8][15][16]
Evidence, guidelines and controversies
Controversies to handle calmly: how large mirtazapine’s NMA rank advantage is versus weight cost; whether combination from day one ever helps selected severe phenotypes despite CO-MED; how clinically meaningful vortioxetine’s cognitive endpoints are outside trials. Answer with phenotype, dose, monitoring and patient values.[8][14][15]
Exam pearls
MAP DOSE before atypical AD prescribe
MAPDOSE
References
- [1]de Boer T The pharmacologic profile of mirtazapine J Clin Psychiatry, 1996.PMID 8636062
- [2]Benkert O, Szegedi A, Kohnen R Mirtazapine compared with paroxetine in major depression J Clin Psychiatry, 2000.PMID 11030486
- [3]Carpenter LL, Yasmin S, Price LH A double-blind, placebo-controlled study of antidepressant augmentation with mirtazapine Biol Psychiatry, 2002.PMID 11822997
- [4]Rush AJ, Trivedi MH, Wisniewski SR, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression N Engl J Med, 2006.PMID 16554525
- [5]Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentation after the failure of SSRIs for depression N Engl J Med, 2006.PMID 16554526
- [6]Fava M, Rush AJ, Wisniewski SR, et al. A comparison of mirtazapine and nortriptyline following two consecutive failed medication treatments for depressed outpatients: a STAR*D report Am J Psychiatry, 2006.PMID 16816220
- [7]McGrath PJ, Stewart JW, Fava M, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report Am J Psychiatry, 2006.PMID 16946177
- [8]Rush AJ, Trivedi MH, Stewart JW, et al. Combining medications to enhance depression outcomes (CO-MED): acute and long-term outcomes of a single-blind randomized study Am J Psychiatry, 2011.PMID 21536692
- [9]Blier P, Gobbi G, Turcotte JE, et al. Mirtazapine and paroxetine in major depression: a comparison of monotherapy versus their combination from treatment initiation Eur Neuropsychopharmacol, 2009.PMID 19345072
- [10]Fava M, Rush AJ, Thase ME, et al. 15 years of clinical experience with bupropion HCl: from bupropion to bupropion SR to bupropion XL Prim Care Companion J Clin Psychiatry, 2005.PMID 16027765
- [11]Davidson J Seizures and bupropion: a review J Clin Psychiatry, 1989.PMID 2500425
- [12]Jorenby DE, Leischow SJ, Nides MA, et al. A controlled trial of sustained-release bupropion, a nicotine patch, or both for smoking cessation N Engl J Med, 1999.PMID 10053177
- [13]Thase ME, Clayton AH, Haight BR, et al. A double-blind comparison between bupropion XL and venlafaxine XR: sexual functioning, antidepressant efficacy, and tolerability J Clin Psychopharmacol, 2006.PMID 16974189
- [14]McIntyre RS, Lophaven S, Olsen CK A randomized, double-blind, placebo-controlled study of vortioxetine on cognitive function in depressed adults Int J Neuropsychopharmacol, 2014.PMID 24787143
- [15]Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis Lancet, 2018.PMID 29477251
- [16]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391