Psych · Psychopharmacology — mood stabilisers
Mood stabilisers
Also known as Lithium · Valproate · Sodium valproate · Divalproex · Lamotrigine · Carbamazepine · Mood stabilizers · Anticonvulsant mood stabilisers
Exam-exhaustive fellowship psychopharmacology of mood stabilisers — lithium, valproate, lamotrigine, carbamazepine: mechanisms, levels, monitoring, toxicity and EXTRIP, teratogenicity hierarchy, BALANCE and maintenance evidence, enzyme-induction interactions, HLA-B*1502, pregnancy and contraception, when not to use valproate. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Mood-stabiliser pharmacology is high-weight across FRANZCP, MRCPsych and ABPN because examiners test levels, toxicity, teratogenicity hierarchy, interactions, and trial names — not brand slogans. This topic is the drug-class spine that bipolar mania, bipolar depression, maintenance and perinatal stations plug into.[1][16][21]
Definition and classification
A mood stabiliser, used carefully in exams, is a medicine that treats and/or prevents manic and/or depressive poles of bipolar illness with an acceptable long-term safety plan. The term is clinical, not a single receptor class.[16][4]
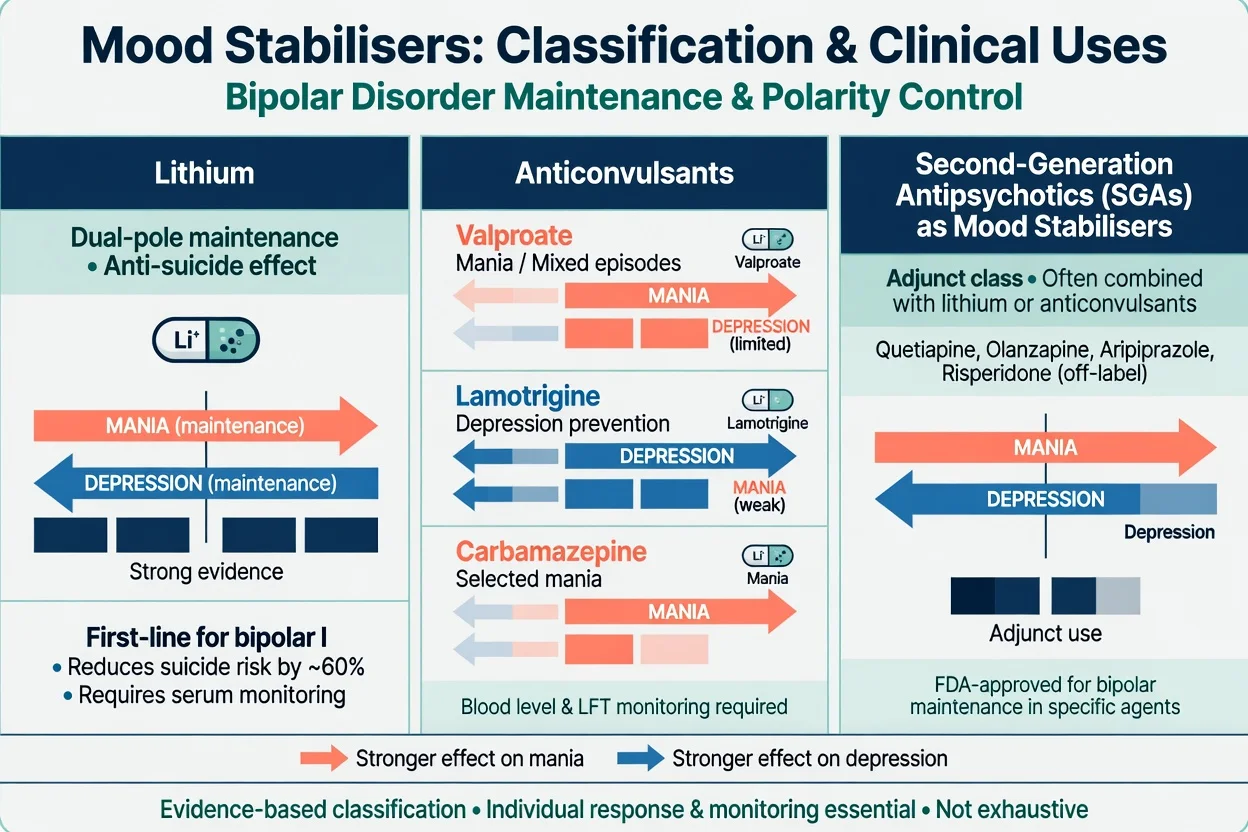
Working taxonomy for exam prescribing (pole fit, not marketing labels):
| Class | Core agents | Exam pole strength (simplified) |
|---|---|---|
| Lithium salt | Lithium carbonate (formulations vary by region) | Dual-pole maintenance; anti-suicide signal; antimanic |
| Anticonvulsant mood stabilisers | Valproate/divalproex; lamotrigine; carbamazepine (± oxcarbazepine niche) | VPA/CBZ stronger for mania; LTG stronger for depression prevention |
| SGAs used as mood stabilisers | Quetiapine, olanzapine, aripiprazole, others (local labels) | Acute mania and selected bipolar depression — detail in antipsychotics topic |
| Classification is for prescribing logic across mania, depression prevention and dual maintenance — not marketing categories.[3][4][16] |
Mechanisms — viva depth without fluff
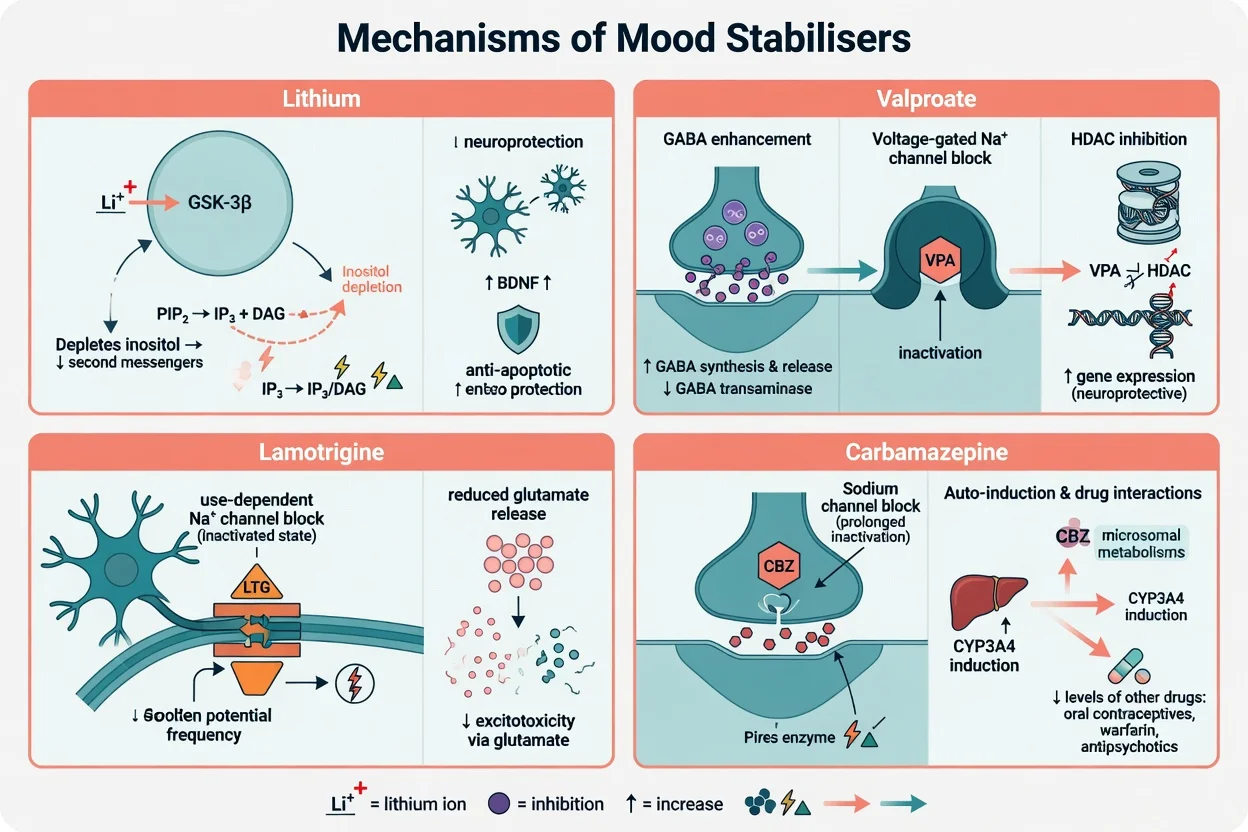
Lithium. Multiple intracellular actions are taught: inhibition of GSK-3β, inositol monophosphatase depletion reducing PIP2-derived second messengers, and broader neuroprotective signalling (BDNF-related hypotheses). Exam point: mechanism is multi-target; toxicity is renal handling and narrow therapeutic index, not a single receptor overdose story.[20][15]
Valproate. Enhances GABAergic tone, blocks voltage-gated sodium channels, and inhibits histone deacetylases — explaining antimanic efficacy and some metabolic/teratogenic concerns discussed elsewhere in reproductive toxicology, not as a single clean receptor story.[6][11]
Lamotrigine. Use-dependent sodium channel blockade and reduced glutamate release; clinical corollary is slow titration to reduce serious rash risk, and weaker acute antimanic punch than lithium/valproate/SGAs.[8][7][22]
Carbamazepine. Sodium channel blockade plus potent CYP3A4 induction and autoinduction — the interaction engine that makes oral contraceptives and many co-medications fail or underperform.[9][10]
Landmark evidence every candidate must own
Trials that change viva answers
BALANCE. In bipolar I relapse prevention, lithium monotherapy outperformed valproate monotherapy; lithium–valproate combination was also effective. This is the classic exam lever against casual valproate-for-all maintenance.[1]
Long-term lithium meta-analysis (Geddes). Lithium reduces relapse versus placebo across poles in randomised evidence — the maintenance backbone.[5]
Antimanic network meta-analysis (Cipriani). Several SGAs, lithium and valproate sit in the effective set; choose by tolerability, prior response, psychosis, and pregnancy potential.[3]
Maintenance network meta-analysis (Miura). Supports lithium among the most robust long-term options while placing other agents in a comparative field by efficacy and tolerability.[4]
Lithium and suicide (Cipriani). Updated systematic review/meta-analysis supports lithium for prevention of suicide and related outcomes in mood disorders — a unique pharmacologic signal among classic mood stabilisers.[2]
Lamotrigine maintenance (Goodwin pooled) and depression trials (Calabrese). Lamotrigine’s signal is relatively stronger for delaying depressive recurrence than for acute mania; acute bipolar depression monotherapy effects are modest and slow compared with several SGAs used for bipolar depression.[7][8][22]
Divalproex mania (Bowden). Landmark placebo-controlled comparison with lithium established valproate/divalproex as an antimanic option.[6]
STEP-BD adjunctive antidepressants. Adjunctive antidepressants are not a substitute mood-stabiliser strategy and do not show broad effectiveness for bipolar depression in that effectiveness design — polarity safety still rules.[17]
Clinical selection algorithm
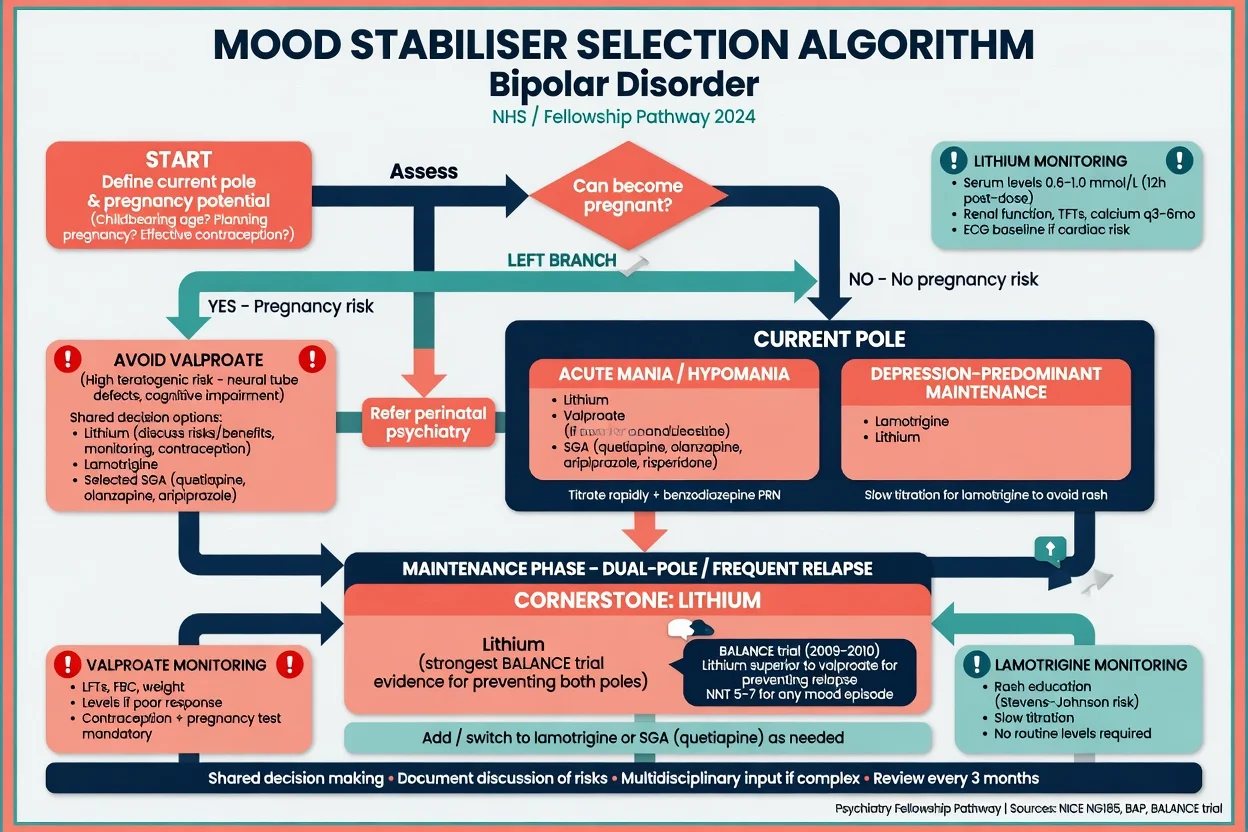
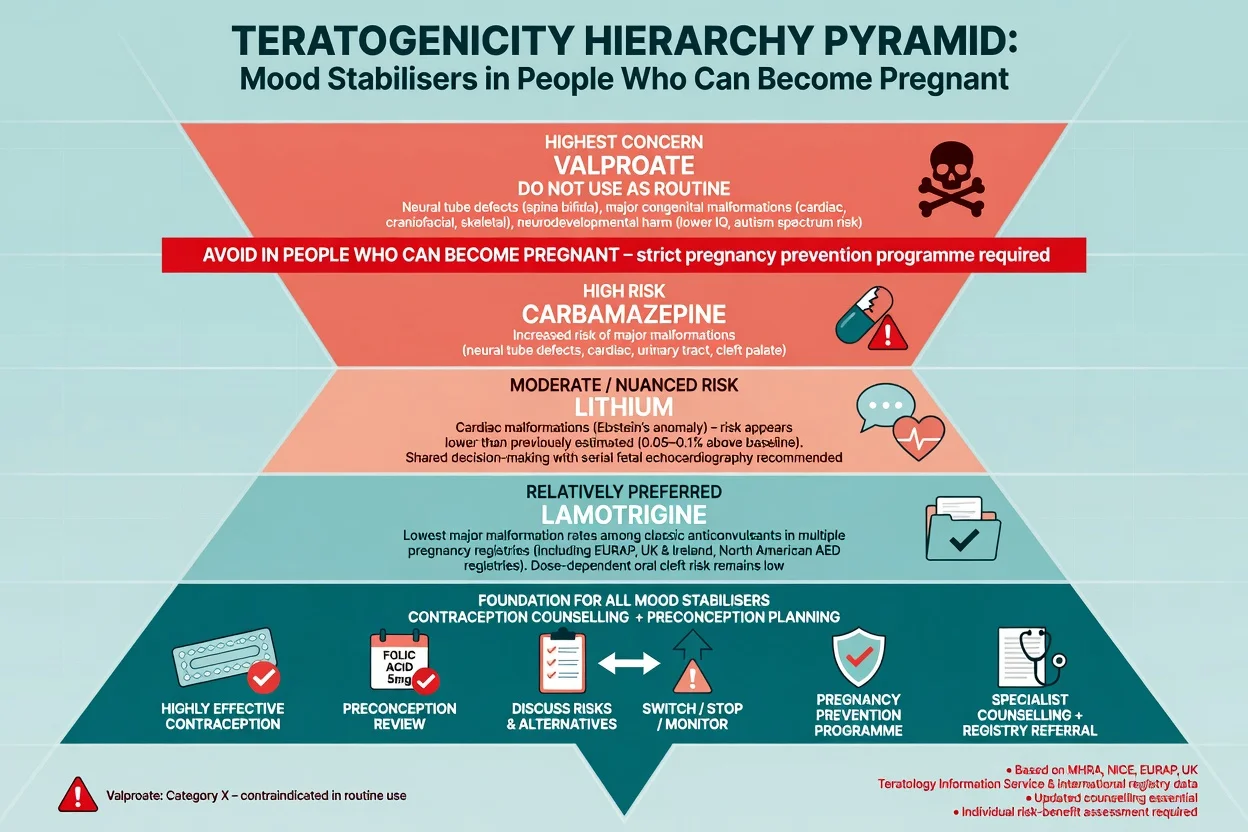
Step 0 — pregnancy potential. If the person can become pregnant, do not use valproate as routine bipolar care. Document counselling, contraception, and alternatives (lithium shared decision, lamotrigine, selected SGAs) with perinatal psychiatry when complex.[11][12][19][16]
Acute mania / mixed features. Lithium, valproate (if pregnancy risk excluded), and several SGAs are evidence-based; combination lithium or valproate plus SGA is common in severe illness. Network data support multiple options rather than one universal winner.[3][6][16]
Bipolar depression / depression-predominant course. Prefer polarity-safe strategies (selected SGAs with bipolar depression evidence; lamotrigine for prevention; lithium where levels feasible). Do not treat as unipolar depression with antidepressant monotherapy in bipolar I.[8][17][16]
Maintenance after bipolar I. Lithium first-line when tolerated and monitorable (BALANCE + Geddes + Miura + anti-suicide). Lamotrigine for depression-pole burden. Valproate maintenance is weaker than lithium in BALANCE monotherapy comparison.[1][5][4][2]
Lithium — initiation, levels, monitoring
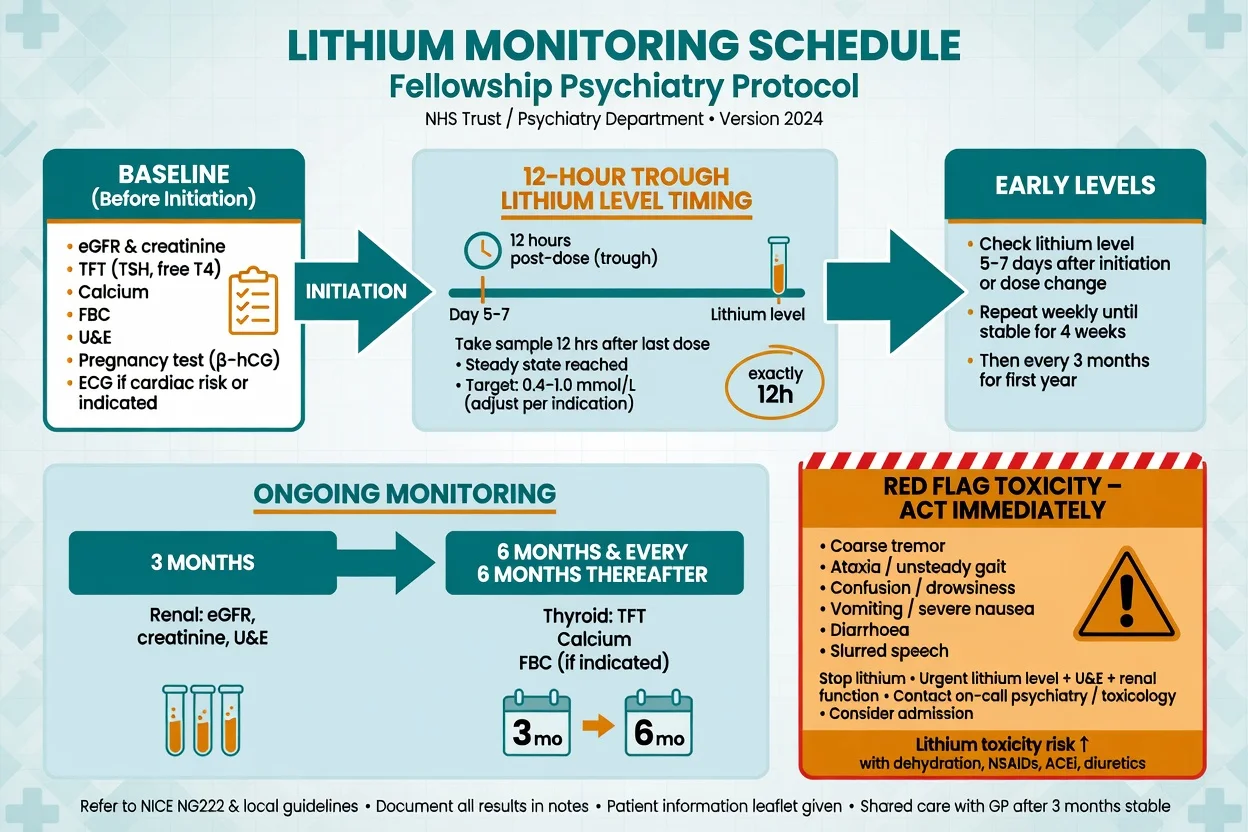
Baseline (document before first dose): eGFR/creatinine and electrolytes, TFT, calcium (parathyroid risk long-term), FBC as local practice, pregnancy test when relevant, weight, and ECG when cardiac risk or older age. Educate on hydration, intercurrent illness, and interacting drugs.[15][20][21]
Dosing (adult orientation — always localise to product information). Typical initiation is lithium carbonate in divided or once-daily regimens depending on formulation and local practice, titrated to clinical response and trough level. Older adults and reduced GFR need lower starts and closer levels.[14][21]
12-hour trough. Draw level approximately 12 hours after the last dose, at steady state (often around day 5–7 after initiation or dose change, depending on half-life and formulation). Random daytime levels are not troughs — say this in every viva.[14][15]
Target ranges (ISBD/IGSLI framework). The ISBD/IGSLI lithium task force synthesises evidence toward maintenance levels commonly around 0.6–0.8 mmol/L for many adults, with individualisation (lower in older adults/frailty; higher ends sometimes used short-term in acute mania under close supervision). Always interpret level with clinical state, renal function and timing quality.[14]
Ongoing monitoring. Recheck levels after dose changes and during intercurrent illness; then periodically (commonly every 3 months early, then about every 6 months when stable) with renal function, TFT and calcium. Increase frequency if interacting drugs start, dehydration, or fluctuating levels.[15][20][21]
Lithium toxicity — emergency ladder
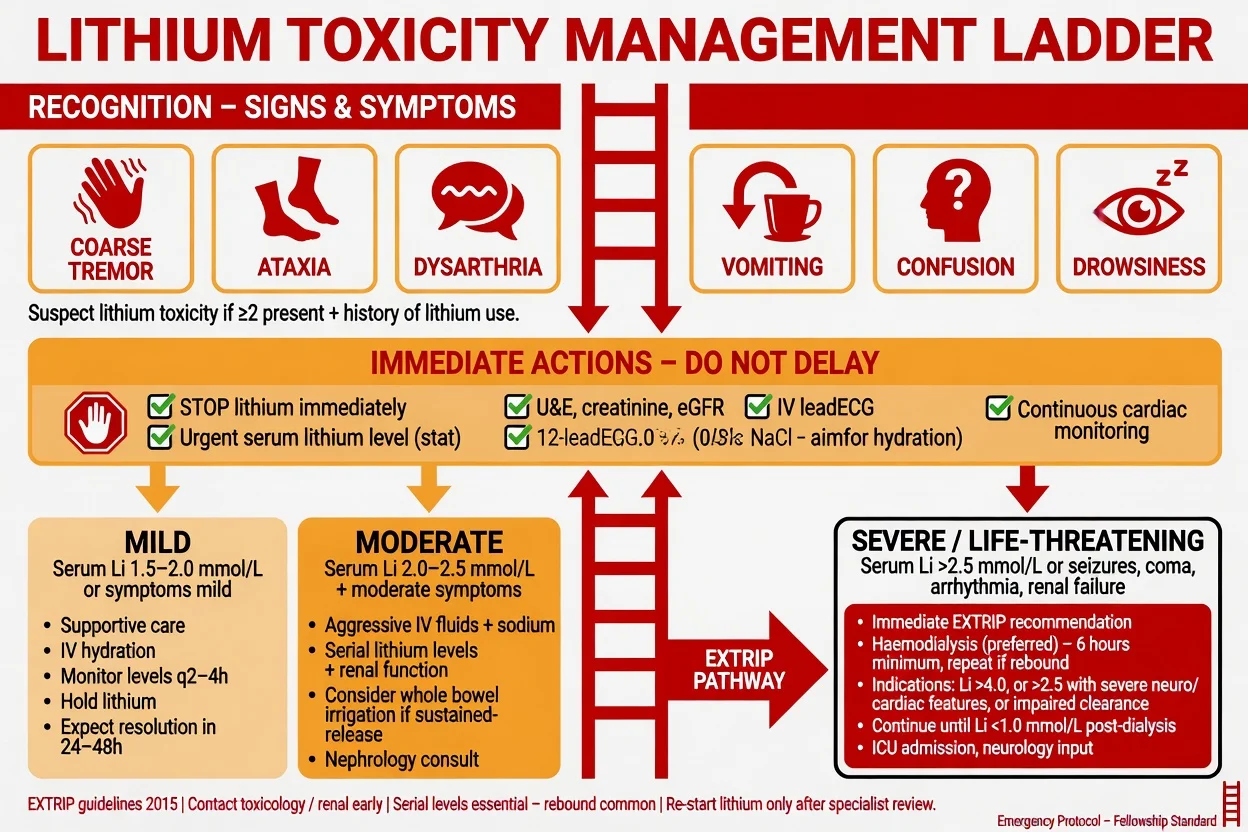
Clinical pattern: coarse tremor, ataxia, dysarthria, vomiting/diarrhoea, confusion, drowsiness, progressing to seizures and coma. Acute overdose, chronic accumulation, and acute-on-chronic patterns differ; chronic toxicity can be severe at levels that look only moderately high.[18][15]
Immediate actions: stop lithium; urgent serum lithium, U&E/creatinine/eGFR; ECG and monitoring; IV fluids as indicated; exclude precipitants (NSAIDs, ACE inhibitors/ARBs, thiazides, dehydration, low salt intake).[18][15]
Extracorporeal treatment (EXTRIP). The EXTRIP workgroup provides systematic recommendations for extracorporeal treatment in lithium poisoning for severe clinical toxicity, impaired elimination, or high levels with concerning features — involve toxicology/nephrology early rather than waiting for catastrophic decline.[13]
Chronic adverse effects to name: reduced urinary concentrating ability / NDI spectrum, long-term GFR decline risk, hypothyroidism, hyperparathyroidism/hypercalcaemia, tremor, weight gain, acne/psoriasis flares. Manage with monitoring and shared decision, not lithium nihilism when the indication is strong.[15][20]
Valproate (divalproex / sodium valproate)
Use cases: acute mania and mixed features; selected maintenance when lithium unsuitable and pregnancy potential is excluded or under a formal pregnancy-prevention framework required by local regulation.[6][3][16]
Dosing orientation (adult): standard titration or, in selected acute mania protocols, higher initial dosing strategies toward clinical response; many labs use therapeutic total valproate ranges roughly on the order of 50–100 mg/L (lab-specific; free levels in hypoalbuminaemia). Loading concepts appear in some acute protocols — always localise to product information and comorbidity.[6][16]
Monitoring: baseline LFT, FBC, pregnancy test, weight; ongoing LFT/FBC/weight; levels when adherence, toxicity or poor response questions arise; ammonia if unexplained encephalopathy.[16]
Adverse effects: tremor, weight gain, hair loss, thrombocytopenia, hepatotoxicity, pancreatitis (rare but serious), hyperammonaemia, PCOS-like features in some reproductive-age patients.[16][11]
When not to use valproate
Lamotrigine
Best exam niche: maintenance prevention of depressive episodes; spectrum activity in treatment-refractory bipolar depression-prone courses; less useful as a fast acute antimanic.[7][8][22]
Titration (classic adult monotherapy skeleton — always follow product information): often 25 mg daily for 2 weeks, 50 mg daily for 2 weeks, then stepwise toward common targets around 200 mg/day as tolerated. Halve escalation speed / lower doses with valproate (valproate inhibits lamotrigine clearance). Faster schedules or higher targets may be needed with enzyme inducers such as carbamazepine — product tables rule, not memory freestyle.[8][7]
Rash discipline: educate day 0; stop and urgent review for widespread, blistering, mucosal, or systemic rash; never rechallenge after serious cutaneous reaction without specialist dermatology/allergy input.[8]
Carbamazepine (and HLA)
Niche: selected mania, lithium non-response, historical bipolar subtypes; not the modern first-line maintenance default for most patients given interactions and alternatives.[3][16]
HLA-B*1502. Strong association with carbamazepine-induced SJS/TEN in many East and South-East Asian populations (classic Nature genetics marker paper). Screen per local guidance before starting in high-prevalence ancestry groups; if positive, avoid carbamazepine and related aromatic risk agents as directed locally.[9]
HLA-A*3101. Associated with a broader spectrum of carbamazepine hypersensitivity in European ancestry cohorts — another reason to take allergy history and local pharmacogenetic guidance seriously.[10]
Monitoring: baseline FBC, LFT, sodium, pregnancy status; levels when useful; watch for hyponatraemia (SIADH spectrum), rash, rare blood dyscrasias, and interaction-driven contraceptive failure.[9][10]
Interactions that examiners love
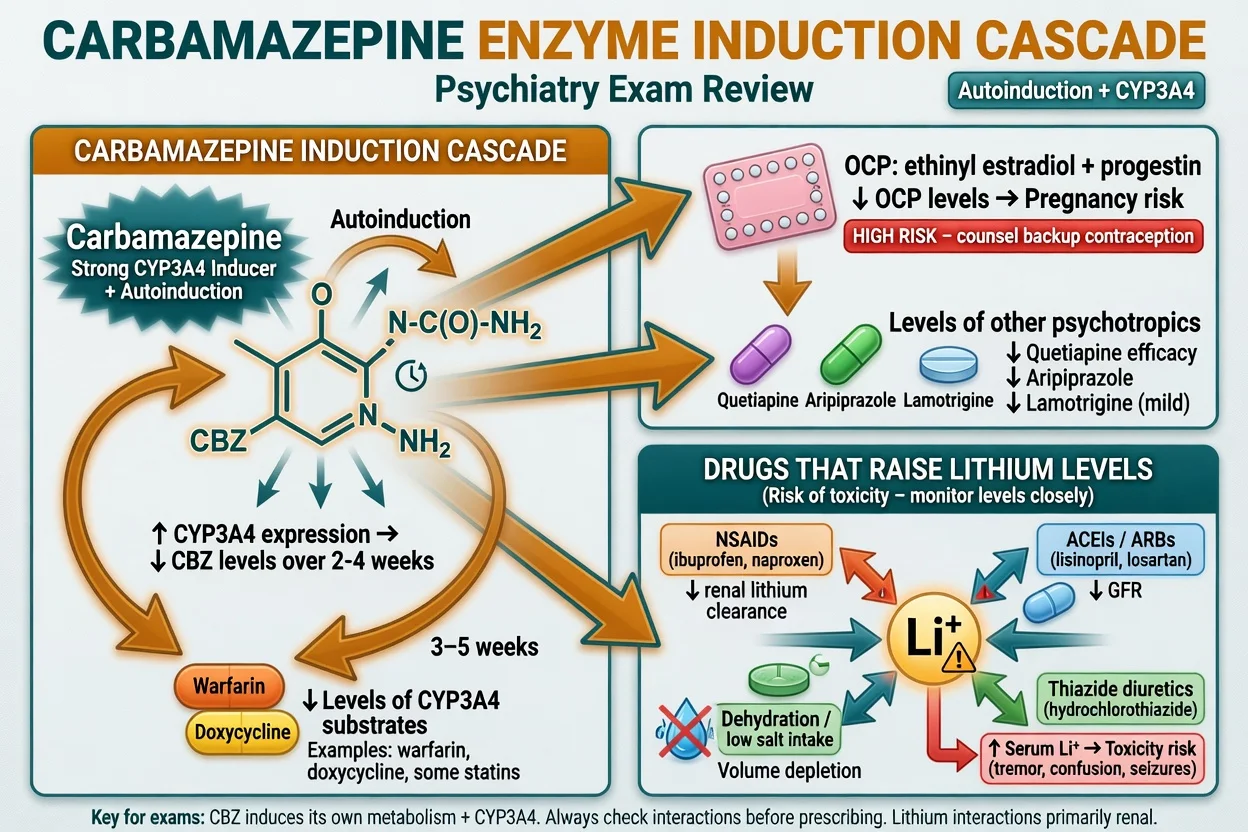
Lithium rises with: NSAIDs, ACE inhibitors/ARBs, thiazide diuretics, dehydration, low effective circulating volume. Educate and recheck levels when these appear.[15][18]
Carbamazepine induces CYP3A4 (and autoinduces): reduces ethinylestradiol/progestogen exposure (contraceptive failure risk — counsel backup methods), and can lower levels of many co-prescribed agents (selected antipsychotics, lamotrigine, others). Re-titrate partners when CBZ starts or stops.[9][10]
Valproate–lamotrigine: valproate increases lamotrigine levels — slower LTG titration mandatory.[8]
Special populations
Older adults. Lower lithium targets and doses; fall risk; renal senescence; delirium mimics of toxicity. Prefer careful monotherapy.[14][15]
Renal impairment. Lithium often avoided or used only with specialist monitoring; choose alternatives.[15][20]
Youth. Specialist initiation, family engagement, metabolic and reproductive counselling for anticonvulsants/SGAs.[16]
Pregnancy and lactation. Preconception counselling is part of mood-stabiliser competence. Hierarchy: avoid valproate; lithium is a nuanced shared decision with cardiac malformation risk lower than older dogma but not zero — coordinate obstetric–psychiatry care and imaging pathways as indicated; lamotrigine often relatively preferred among classic anticonvulsants in registry malformation comparisons, with dose-aware counselling; carbamazepine carries meaningful malformation risk and enzyme-induction contraceptive issues. Lactation is agent-specific — localise guidance rather than invent milk ratios in the exam room.[11][12][19][16]
Evidence, guidelines and regional deltas
RANZCP-aligned and local ANZ practice retains lithium as a core maintenance option with structured monitoring and strong valproate pregnancy cautions. UK practice is tightly shaped by valproate pregnancy-prevention regulations and NICE-style lithium infrastructure. CANMAT/ISBD hierarchical tables are common ABPN/global study sources for line-of-treatment language. APA-framed care emphasises measurement-based polarity treatment and shared decision. Exam constant: name the hierarchy and the monitoring, not a single global tablet.[16][21][1]
Guideline synthesis for lithium (Malhi et al.). Clinical practice guidelines converge on lithium’s central role when monitoring systems exist — use this when asked why lithium remains first-line despite “old drug” rhetoric.[21]
Exam pearls
LITHIUM checklist
LITHIUM
Lithium
- Dual-pole maintenance
- Anti-suicide signal
- 12 h trough + renal/thyroid/Ca
- Toxicity emergency pathway
Valproate
- Acute mania / mixed
- Avoid if pregnancy possible
- LFT/FBC/weight
- Weaker than Li monotherapy in BALANCE
Lamotrigine
- Depression-pole prevention
- Slow titration / rash rules
- Slower with valproate
- Not a rapid antimanic
Carbamazepine
- Selected mania niche
- HLA-B*1502 / A*3101 context
- CYP3A4 induction
- Contraceptive failure risk
References
- [1]BALANCE investigators and collaborators, Geddes JR, Goodwin GM, et al. Lithium plus valproate combination therapy versus monotherapy for relapse prevention in bipolar I disorder (BALANCE): a randomised open-label trial Lancet, 2010.PMID 20092882
- [2]Cipriani A, Hawton K, Stockton S, et al. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis BMJ, 2013.PMID 23814104
- [3]Cipriani A, Barbui C, Salanti G, et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis Lancet, 2011.PMID 21851976
- [4]Miura T, Noma H, Furukawa TA, et al. Comparative efficacy and tolerability of pharmacological treatments in the maintenance treatment of bipolar disorder: a systematic review and network meta-analysis Lancet Psychiatry, 2014.PMID 26360999
- [5]Geddes JR, Burgess S, Hawton K, et al. Long-term lithium therapy for bipolar disorder: systematic review and meta-analysis of randomized controlled trials Am J Psychiatry, 2004.PMID 14754766
- [6]Bowden CL, Brugger AM, Swann AC, et al. Efficacy of divalproex vs lithium and placebo in the treatment of mania. The Depakote Mania Study Group JAMA, 1994.PMID 8120960
- [7]Goodwin GM, Bowden CL, Calabrese JR, et al. A pooled analysis of 2 placebo-controlled 18-month trials of lamotrigine and lithium maintenance in bipolar I disorder J Clin Psychiatry, 2004.PMID 15096085
- [8]Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group J Clin Psychiatry, 1999.PMID 10084633
- [9]Chung WH, Hung SI, Hong HS, et al. Medical genetics: a marker for Stevens-Johnson syndrome Nature, 2004.PMID 15057820
- [10]McCormack M, Alfirevic A, Bourgeois S, et al. HLA-A*3101 and carbamazepine-induced hypersensitivity reactions in Europeans N Engl J Med, 2011.PMID 21428769
- [11]Tomson T, Battino D, Bonizzoni E, et al. Dose-dependent risk of malformations with antiepileptic drugs: an analysis of data from the EURAP epilepsy and pregnancy registry Lancet Neurol, 2011.PMID 21652013
- [12]Meador KJ, Baker GA, Browning N, et al. Cognitive function at 3 years of age after fetal exposure to antiepileptic drugs N Engl J Med, 2009.PMID 19369666
- [13]Decker BS, Goldfarb DS, Dargan PI, et al. Extracorporeal Treatment for Lithium Poisoning: Systematic Review and Recommendations from the EXTRIP Workgroup Clin J Am Soc Nephrol, 2015.PMID 25583292
- [14]Nolen WA, Licht RW, Young AH, et al. What is the optimal serum level for lithium in the maintenance treatment of bipolar disorder? A systematic review and recommendations from the ISBD/IGSLI Task Force on treatment with lithium Bipolar Disord, 2019.PMID 31112628
- [15]Gitlin M Lithium side effects and toxicity: prevalence and management strategies Int J Bipolar Disord, 2016.PMID 27900734
- [16]Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder Bipolar Disord, 2018.PMID 29536616
- [17]Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression N Engl J Med, 2007.PMID 17392295
- [18]Okusa MD, Crystal LJ Clinical manifestations and management of acute lithium intoxication Am J Med, 1994.PMID 7942943
- [19]Tomson T, Battino D, Bonizzoni E, et al. Comparative risk of major congenital malformations with eight different antiepileptic drugs: a prospective cohort study of the EURAP registry Lancet Neurol, 2018.PMID 29680205
- [20]Gitlin M, Bauer M Lithium: current state of the art and future directions Int J Bipolar Disord, 2024.PMID 39609318
- [21]Malhi GS, Gessler D, Outhred T The use of lithium for the treatment of bipolar disorder: Recommendations from clinical practice guidelines J Affect Disord, 2017.PMID 28437764
- [22]Calabrese JR, Bowden CL, McElroy SL, et al. Spectrum of activity of lamotrigine in treatment-refractory bipolar disorder Am J Psychiatry, 1999.PMID 10401445