Psych · Psychopharmacology — pharmacogenomics
Pharmacogenomics in psychiatry
Also known as Psychiatric pharmacogenetics · CYP2D6 CYP2C19 antidepressants · HLA-B*1502 carbamazepine · CPIC psychiatry · PGx testing depression · Atomoxetine CYP2D6
Exam-exhaustive fellowship reference on psychiatric pharmacogenomics — CYP metaboliser phenotypes, CPIC antidepressant and atomoxetine guidance, HLA safety testing for carbamazepine/oxcarbazepine, commercial panel limits, GUIDED/PRIME Care literacy, TDM integration, and counselling. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Pharmacogenomics sits at the junction of pharmacokinetics, immunology, and commercial medicine. Fellowship examiners want candidates who can translate star alleles into phenotypes, apply CPIC-style tables without worshipping combinatorial marketing, prevent HLA-mediated SJS/TEN, and appraise GUIDED and PRIME Care without either nihilism or hype.[3][8][9][10]

Overview and definition
Pharmacogenetics usually denotes single gene–drug effects; pharmacogenomics the broader multi-gene landscape. In psychiatry the high-yield content is almost entirely: (1) pharmacokinetic (PK) variants that change exposure (mainly CYP2D6, CYP2C19, CYP2B6); (2) HLA variants that change immune risk for severe cutaneous adverse reactions with aromatic anticonvulsants; and (3) pharmacodynamic (PD) variants (for example SLC6A4, HTR2A) that remain largely non-actionable for routine prescribing under current CPIC evidence summaries.[3][8][16]
A metaboliser phenotype is the clinically usable label derived from genotype (and sometimes copy number): poor (PM), intermediate (IM), normal/extensive (NM), rapid (RM), ultrarapid (UM). CYP2D6 activity scores formalise allele function into a continuous-ish scale that maps to those bins.[1][3]
Classification — actionability framework
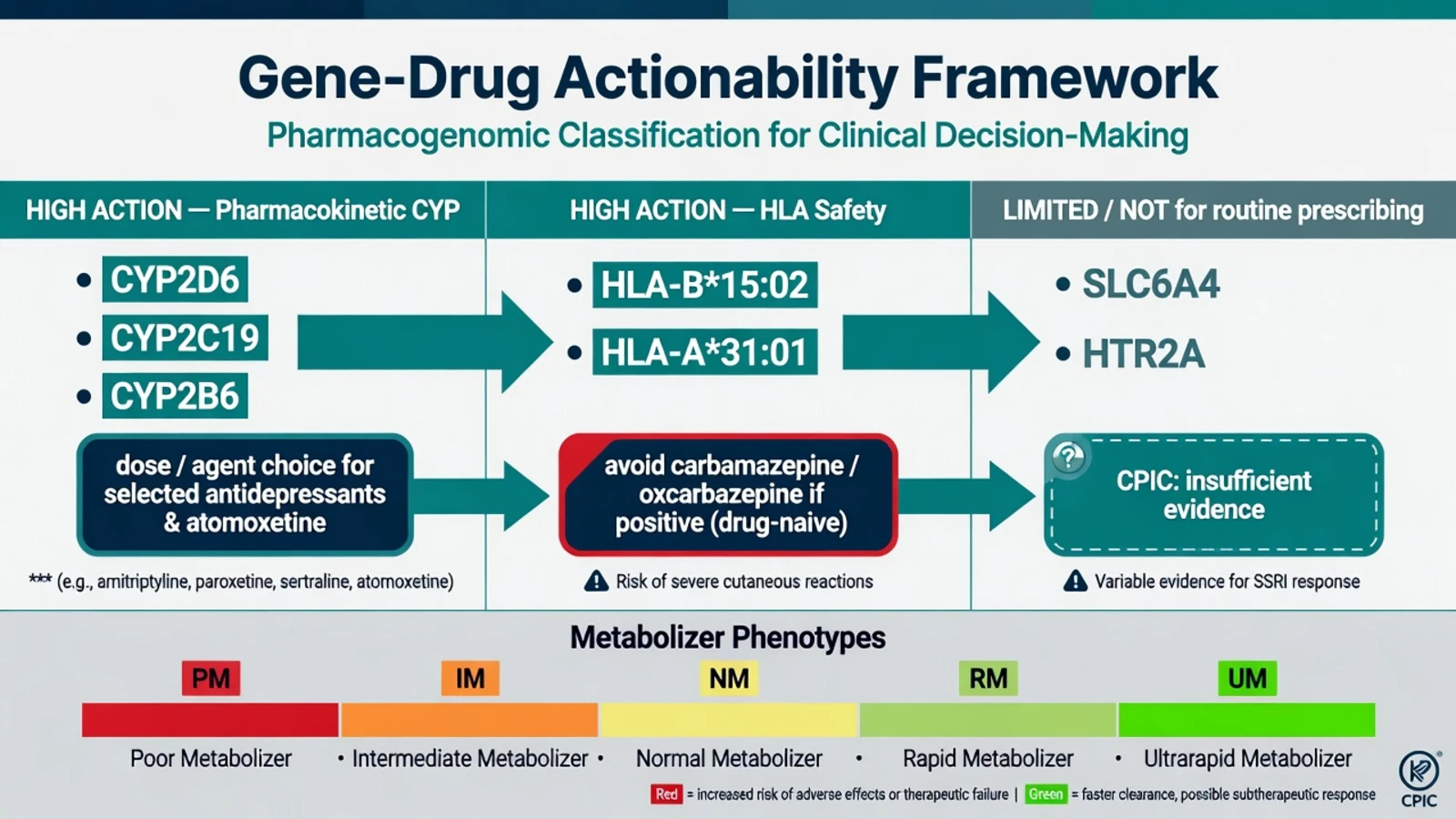
High-action PK genes are CYP2D6, CYP2C19, and CYP2B6 (dose start/adjustment or alternative agent for selected SRIs, TCAs, and atomoxetine). High-action safety genes are HLA-B15:02 and HLA-A31:01 (avoid carbamazepine/oxcarbazepine if positive and drug-naive per guideline frames). Limited / not for routine choice includes SLC6A4, HTR2A, and many panel extras (do not use alone to pick an antidepressant). Infrastructure lives in PharmGKB/CPIC annotations rather than a memorised one-off paper. Actionability ranks PK CYP pairs and HLA safety above unsupported PD marketing claims.[3][4][8][16]
ISPG consensus language aligns with this hierarchy: strongest clinical support for CYP2D6/CYP2C19 dosing of selected antidepressants/antipsychotics and for HLA before carbamazepine/oxcarbazepine; weaker support for many marketed PD markers.[3][4][8]
Epidemiology and risk
CYP allele frequencies vary by ancestry. CYP2D6 PM status is classically taught around roughly one in ten people of European ancestry (order-of-magnitude exam figure, not a statute); UM rates and CYP2C19*17 rapid alleles differ substantially across populations — always interpret lab reports with local allele coverage in mind.[1][3][16]
HLA-B*15:02 is more prevalent in many East and Southeast Asian populations and is tightly linked to carbamazepine-induced SJS/TEN; prospective screening in Taiwan essentially eliminated carbamazepine SJS/TEN in the screened pathway when carriers avoided the drug.[5][7] HLA-A*31:01 associates with a broader carbamazepine hypersensitivity spectrum in European ancestry cohorts, including SJS/TEN and milder cutaneous reactions.[6]
Commercial depression PGx is marketed into a large non-response / intolerance market; average trial effect sizes are modest and heterogeneous, which is why viva answers must separate safety HLA (high stakes, clear action) from optional combinatorial MDD panels (implementation science, not magic).[9][10][13][14]
Pathophysiology — genotype to phenotype
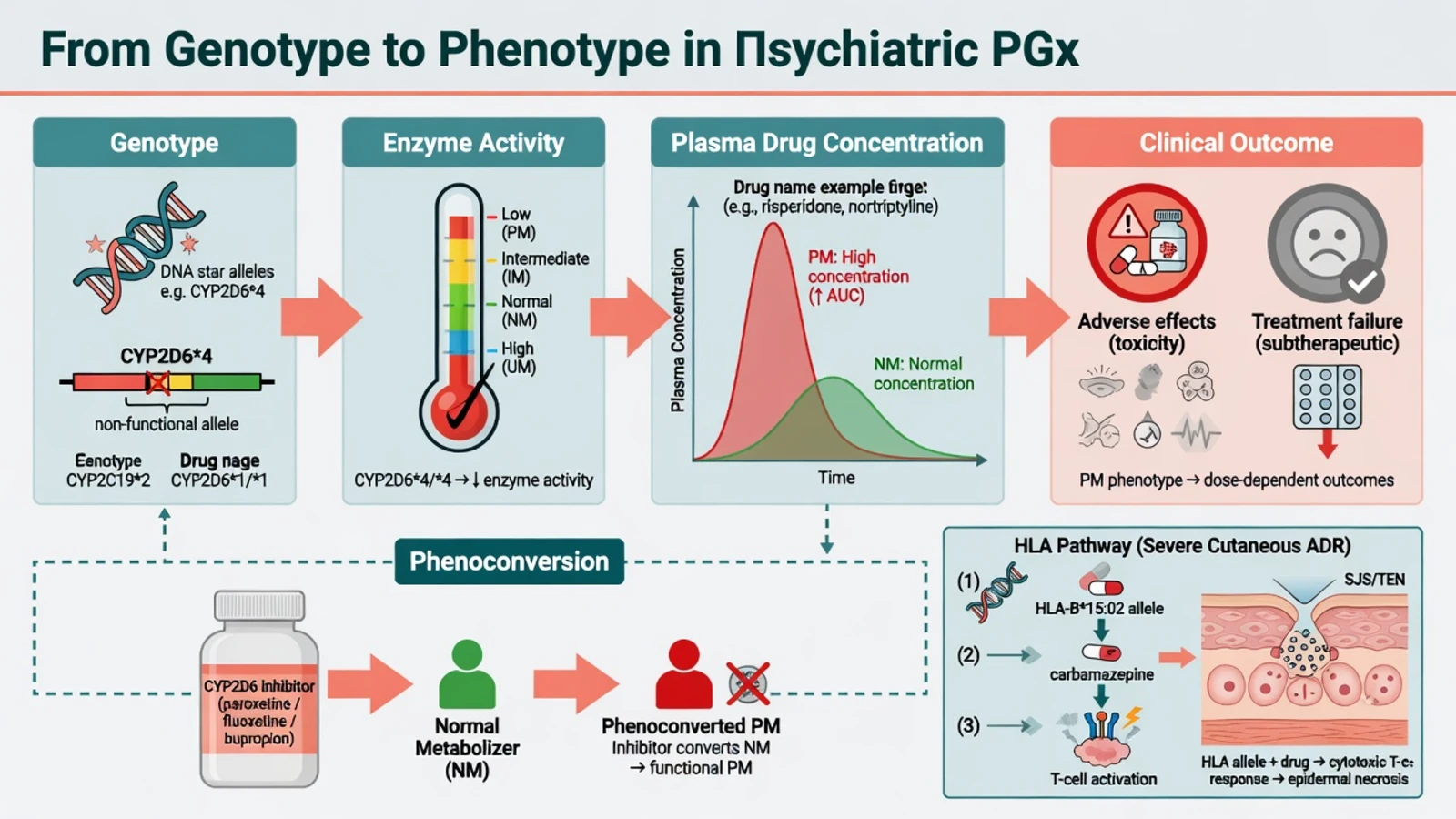
PK pathway. Loss-of-function alleles reduce CYP enzyme activity → slower clearance of parent substrate → higher steady-state concentrations at a standard oral dose → more concentration-dependent adverse effects. Gain-of-function or multiplications can create UM phenotypes with lower levels and risk of apparent non-response. For some prodrugs (codeine via CYP2D6 — classic non-psych teaching contrast), PM reduces active metabolite; most psychiatric substrates of exam interest are active parents where PM increases parent exposure.[1][2][3]
Phenoconversion. Strong CYP2D6 inhibitors (classic teaching: paroxetine, fluoxetine, bupropion) can push a genotypic NM toward a functional PM. Genotype without interaction review is incomplete — the same logic as the smoking–clozapine CYP1A2 story in the interactions topic.[3][12]
HLA pathway. Drug–HLA complexes can activate cytotoxic T cells that attack keratinocytes, producing SJS/TEN. This is immune pharmacogenomics, not a CYP clearance story — dose reduction does not make a high-risk HLA allele safe for a drug-naive patient who should avoid the agent.[4][5][7]
PD genes. Serotonin transporter (SLC6A4) and receptor (HTR2A) variants have been extensively studied; effect sizes and replication are inconsistent. CPIC 2023 explicitly states existing data do not support using SLC6A4 or HTR2A genotypes to guide serotonin reuptake inhibitor prescribing.[3]
Clinical presentation
Clinical patterns cluster as PM-type adverse effects at modest CYP-substrate doses (including TCA anticholinergic load and atomoxetine intolerance), UM-type non-response despite adherence, HLA-type severe cutaneous reactions days to weeks after carbamazepine/oxcarbazepine, and clinic visits driven by commercial green/yellow/red reports demanding switches.[3][4][11][15]
Differential diagnosis of "PGx failure"
Non-response may reflect UM/subtherapeutic exposure but more often non-adherence, inadequate duration, wrong diagnosis, substances, or psychosocial load. Intolerance may reflect PM/high exposure or nocebo, organ impairment, interactions, or age-inappropriate dosing. Rash on carbamazepine may relate to HLA-B15:02 / A31:01 risk yet still requires urgent clinical discrimination from viral exanthem, other drugs, and DRESS. High plasma levels may reflect genetic PM status or an inhibitor, inflammation, lab timing, or smoking change for CYP1A2 substrates. Always rank non-adherence, wrong diagnosis, phenoconversion, and organ impairment beside genotype before attributing failure solely to alleles.[3][4][8][12]
Assessment
Assessment requires full medication reconciliation (inhibitors/inducers, OTC, herbals, smoking), prior psychotropic trial detail with any TDM, ancestry and severe drug-reaction history before aromatic anticonvulsants, capacity/consent framing for optional CYP versus strongly indicated HLA testing, and — if a report exists — extraction of diplotype → phenotype → drug-specific recommendation while parking proprietary composite scores until validated against CPIC/DPWG pairs.[3][4][8][16]
Investigations
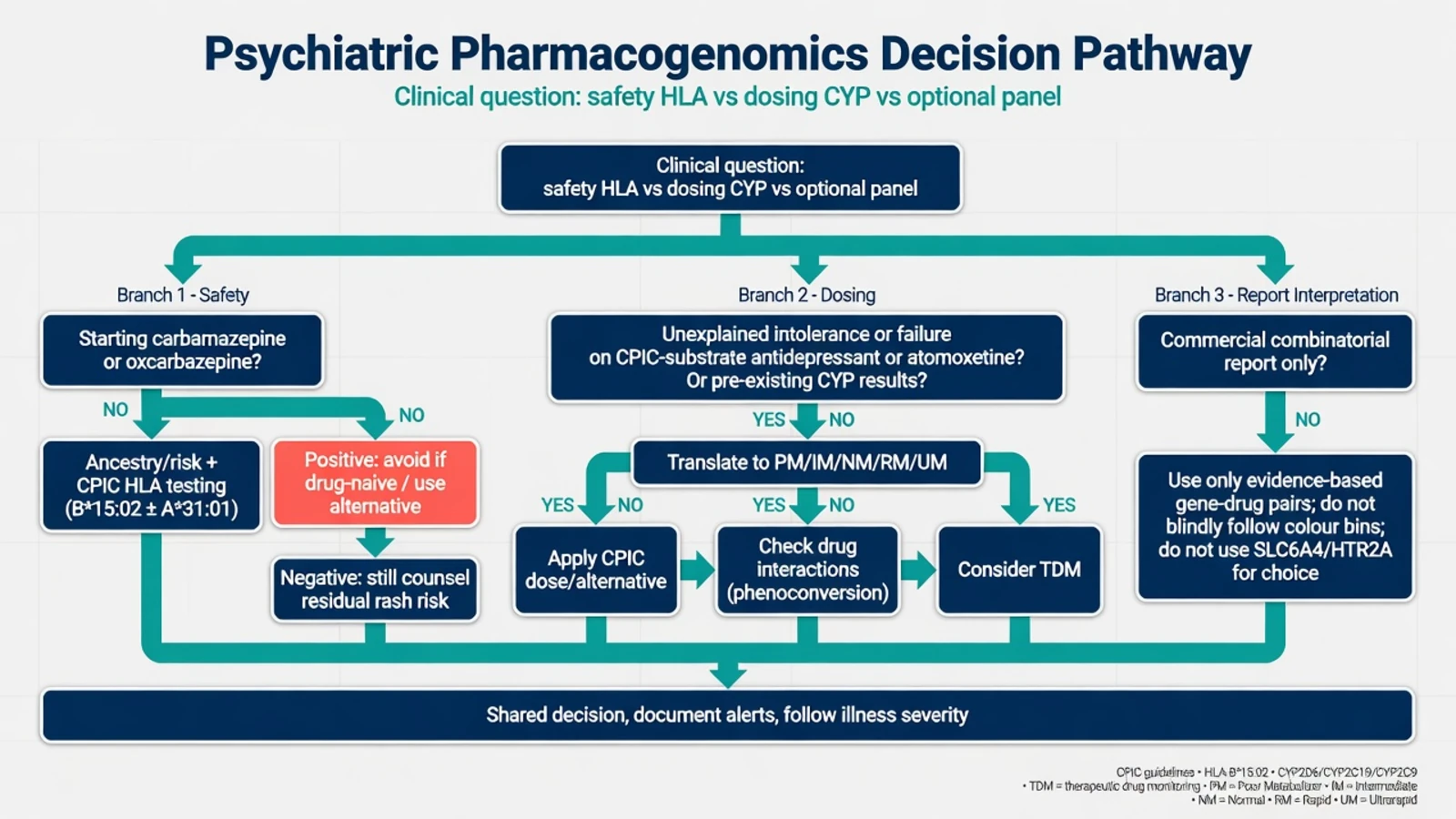
Order / use CYP results when: results already in the record; multiple unexplained intolerances or failures on CPIC-substrate agents; atomoxetine extremes; pre-emptive institutional programmes. Do not treat optional multi-gene depression panels as mandatory before every first SSRI in ordinary care — regional pathways (including NICE-style stepped care ethos) still prioritise clinical algorithms.[3][8][14]
HLA testing: before starting carbamazepine or oxcarbazepine, especially when HLA-B15:02 prevalence is not negligible; interpret with CPIC and product-label frames. Negative HLA-B15:02 lowers SJS/TEN probability in relevant ancestries but does not abolish all rash risk.[4][5]
TDM (AGNP principles): plasma levels are the in vivo phenotype and complement genotype for TCAs, some antipsychotics, and complex polypharmacy.[12]
Baseline metabolic and ECG monitoring still follow agent risk — PGx does not replace physical health workup.[8][12]
Acute / emergency management
For suspected SJS/TEN/DRESS, stop the culprit aromatic agent immediately, escalate to urgent medical/dermatology care, and never rechallenge carbamazepine after SJS/TEN. For severe concentration-related toxicity, support, stop/reduce the culprit, review inhibitors, consider a plasma level, and document possible PM/phenoconversion. Genetic testing is not an emergency intervention once severe cutaneous reaction is evolving — stop the drug first.[4][5][12]
Definitive management — how to use results
Antidepressants (SRI and related)
CPIC recommendations (2015 Hicks SSRI guideline; 2023 Bousman update expanding CYP2D6/2C19/2B6 and reviewing PD genes) translate phenotype into standard dosing, lower starting dose / slower titration, or alternative agent depending on drug–gene pair. Teaching examples: CYP2C19 PM status raises concern for higher exposure on citalopram/escitalopram/sertraline pathways (dose reduction or alternative); CYP2D6 PM status is high-yield for paroxetine, fluvoxamine, vortioxetine contexts and many TCAs; UM phenotypes risk therapeutic failure on some substrates and may need alternatives or level-guided strategies. Exact milligram steps belong in the living CPIC table for the drug in front of you — viva credit is for correct direction of change and naming the enzyme, not inventing a fixed universal milligram for every product label.[1][3]
Tricyclic antidepressants
Hicks CPIC TCA guidance: CYP2D6 and CYP2C19 alter tertiary amine and metabolite ratios. PM status → avoid or substantially reduce dose with TDM; UM → risk of failure / need for alternative. Classic fellowship pairing: amitriptyline/nortriptyline + CYP2D6.[2][12]
Atomoxetine
CYP2D6 is the major clearance path. PMs show higher exposure and more adverse effects but also greater efficacy signals in paediatric data; CPIC provides phenotype-guided initiation and plasma-level strategies rather than one fixed paediatric mg/kg for all genotypes.[11][15]
Carbamazepine and oxcarbazepine (HLA)
If HLA-B*15:02 positive and patient is carbamazepine-naive, avoid carbamazepine; similar caution for oxcarbazepine per CPIC. If HLA-A*31:01 positive, increased hypersensitivity risk — prefer alternatives unless benefit is exceptional and counselling is explicit. Already tolerant patients on long-term therapy without reaction are a different risk calculus than drug-naive starts.[4][5][6]
What not to do
Do not switch a stable, effective, tolerated regimen purely because a commercial report painted it yellow. Do not use SLC6A4/HTR2A to choose an SSRI. Do not ignore phenoconversion.[3][8]
Subtypes and high-yield scenarios
- East Asian ancestry, first manic episode, considering carbamazepine — HLA pathway before first dose.[5]
- European ancestry, family severe CBZ rash — discuss HLA-A*31:01 and alternatives.[6]
- TRD clinic with combinatorial report — extract CPIC pairs only; continue psychotherapy and guideline TRD steps.[9][10]
- Adolescent atomoxetine intolerance — consider CYP2D6; adjust or switch with CAP collaboration.[11][15]
- Escitalopram + CYP2C19 PM + QTc risk factors — exposure and cardiac risk stack; dose/agent rethink (cross-link QTc topic).[3]
- Risperidone or TCA + new paroxetine — phenoconversion trap from strong CYP2D6 inhibition.[2][3]
Complications and pitfalls
Pitfalls include false reassurance after HLA-B*15:02 negative, panels that miss copy-number variants (missed UM), ordering genotype after SJS without first stopping the drug, and using PGx language to justify therapeutic nihilism in severe depression or psychosis.[3][4][5][8]
Prognosis and disposition
GUIDED (combinatorial testing, patient- and rater-blinded design elements) reported improved response/remission versus treatment as usual in MDD — industry-supported context requires critical appraisal of generalisability and algorithm opacity.[9][14]
PRIME Care (VA pragmatic RCT, JAMA 2022): pharmacogenomic results reduced prescriptions with predicted gene–drug interactions and showed time-limited remission advantages at some mid-trial points rather than a durable panacea — perfect viva nuance.[10]
Meta-analyses of prospective controlled trials suggest small-to-moderate average benefit on remission/response with heterogeneity — consistent with selective use, not universal reflex testing.[13][14]
Document actionable genotypes in allergy/alert systems (especially HLA), share with GP and pharmacy, and set follow-up by illness severity and risk, not by how colourful the PDF was.[4][8][10]
Special populations
Children and adolescents: atomoxetine CYP2D6 is high-yield while SSRI paediatric PGx RCT evidence is thinner — consent with caregivers. Older adults: polypharmacy phenoconversion often outranks exotic alleles. Pregnancy: do not delay necessary treatment for non-urgent optional panels; HLA still matters if starting carbamazepine. Intellectual disability or limited historians: collateral on prior severe drug reactions. Ancestry-aware care without stereotyping: base HLA decisions on epidemiology and guidelines, not assumptions about appearance, with interpreter-supported consent in multicultural ANZ practice.[4][8][11][15]
Evidence and regional guidance
Core evidence anchors are CPIC tables (Hicks SSRIs/TCAs; Bousman 2023 SRI; Brown atomoxetine; Phillips HLA), ISPG consensus (Bousman 2021), GUIDED and PRIME Care trial literacy, HLA discovery/prevention papers (Chung, Chen, McCormack), AGNP TDM (Hiemke), and PharmGKB knowledge infrastructure.[1][3][4][8][9][10][12][16]
Regional deltas: FDA-style labels emphasise HLA-B*15:02 screening in at-risk ancestry for carbamazepine; ANZ practice should follow product information plus specialist society safety culture. NICE-style depression pathways do not mandate routine multi-gene PGx for every first-line MDD episode. APA and local formulary documents evolve — state principles, not invented statutes.[4][8][10]
In FRANZCP settings, lead with HLA prevention for aromatic anticonvulsants and CPIC-style CYP interpretation when results exist; treat direct-to-consumer combinatorial reports as optional adjuncts requiring sceptical translation, shared decision, and equity of access — not as a new standard of care for every antidepressant start.[3][4][8]
Exam pearls
PGx viva map
Summary table — fellowship quick reference
Starting CBZ/OXC: HLA risk assessment/testing per CPIC/label and avoid if B*15:02 positive and drug-naive. Known CYP2C19 PM on escitalopram: lower start or alternative with adverse-effect and QTc-factor vigilance. Known CYP2D6 PM on a TCA: avoid or major dose reduction plus TDM. Atomoxetine extremes: CYP2D6-informed plan. Commercial red/yellow lists: map to CPIC pairs only and prefer clinical stability. Severe rash on an aromatic AED: stop the drug and use the emergency pathway first.[2][3][4][5][11][12]
Fellowship standard is precision where evidence is precise, and humility where marketing outruns data. That balance is the whole topic.[3][4][8][10]
References
- [1]Hicks JK, Bishop JR, Sangkuhl K, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors Clin Pharmacol Ther, 2015.PMID 25974703
- [2]Hicks JK, Sangkuhl K, Swen JJ, et al. Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update Clin Pharmacol Ther, 2017.PMID 27997040
- [3]Bousman CA, Stevenson JM, Ramsey LB, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6, CYP2C19, CYP2B6, SLC6A4, and HTR2A Genotypes and Serotonin Reuptake Inhibitor Antidepressants Clin Pharmacol Ther, 2023.PMID 37032427
- [4]Phillips EJ, Sukasem C, Whirl-Carrillo M, et al. Clinical Pharmacogenetics Implementation Consortium Guideline for HLA Genotype and Use of Carbamazepine and Oxcarbazepine: 2017 Update Clin Pharmacol Ther, 2018.PMID 29392710
- [5]Chen P, Lin JJ, Lu CS, et al. Carbamazepine-induced toxic effects and HLA-B*1502 screening in Taiwan N Engl J Med, 2011.PMID 21428768
- [6]McCormack M, Alfirevic A, Bourgeois S, et al. HLA-A*3101 and carbamazepine-induced hypersensitivity reactions in Europeans N Engl J Med, 2011.PMID 21428769
- [7]Chung WH, Hung SI, Hong HS, et al. Medical genetics: a marker for Stevens-Johnson syndrome Nature, 2004.PMID 15057820
- [8]Bousman CA, Bengesser SA, Aitchison KJ, et al. Review and Consensus on Pharmacogenomic Testing in Psychiatry Pharmacopsychiatry, 2021.PMID 33147643
- [9]Greden JF, Parikh SV, Rothschild AJ, et al. Impact of pharmacogenomics on clinical outcomes in major depressive disorder in the GUIDED trial: A large, patient- and rater-blinded, randomized, controlled study J Psychiatr Res, 2019.PMID 30677646
- [10]Oslin DW, Lynch KG, Shih MC, et al. Effect of Pharmacogenomic Testing for Drug-Gene Interactions on Medication Selection and Remission of Symptoms in Major Depressive Disorder: The PRIME Care Randomized Clinical Trial JAMA, 2022.PMID 35819423
- [11]Brown JT, Bishop JR, Sangkuhl K, et al. Clinical Pharmacogenetics Implementation Consortium Guideline for Cytochrome P450 (CYP)2D6 Genotype and Atomoxetine Therapy Clin Pharmacol Ther, 2019.PMID 30801677
- [12]Hiemke C, Bergemann N, Clement HW, et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017 Pharmacopsychiatry, 2018.PMID 29390205
- [13]Brown LC, Stanton JD, Bharthi K, et al. Pharmacogenomic Testing and Depressive Symptom Remission: A Systematic Review and Meta-Analysis of Prospective, Controlled Clinical Trials Clin Pharmacol Ther, 2022.PMID 36111494
- [14]Rosenblat JD, Lee Y, McIntyre RS Does Pharmacogenomic Testing Improve Clinical Outcomes for Major Depressive Disorder? A Systematic Review of Clinical Trials and Cost-Effectiveness Studies J Clin Psychiatry, 2017.PMID 28068459
- [15]Michelson D, Read HA, Ruff DD, et al. CYP2D6 and clinical response to atomoxetine in children and adolescents with ADHD J Am Acad Child Adolesc Psychiatry, 2007.PMID 17242628
- [16]Whirl-Carrillo M, McDonagh EM, Hebert JM, et al. Pharmacogenomics knowledge for personalized medicine Clin Pharmacol Ther, 2012.PMID 22992668