Psych · Psychopharmacology — phototherapy and chronotherapy
Phototherapy and chronotherapy
Also known as Bright light therapy · Light therapy · BLT · Wake therapy · Sleep deprivation antidepressant · Triple chronotherapy · Dark therapy
Exam-exhaustive fellowship reference on phototherapy (bright light therapy) and chronotherapy — 10,000 lux protocols, SAD and nonseasonal depression evidence (Golden, Can-SAD, Lam 2016, Pjrek), circadian phase-response logic, bipolar midday light (Sit), wake therapy and triple chronotherapy, safety and regional deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Phototherapy and chronotherapy are high-yield because examiners test dose parameters, timing relative to the circadian phase-response curve, indication discipline (SAD vs nonseasonal vs bipolar), and safety (switch risk, eyes, severity) in the same station. Rosenthal defined the modern SAD–light story; Eastman, Terman, and Lewy locked in placebo-controlled winter light timing; Golden and Pjrek meta-analysed efficacy; Can-SAD and Lam 2016 put light next to fluoxetine; Sit and Benedetti programmes carry bipolar and rapid chronotherapeutic packages into viva depth.[1][2][3][4][5][8][15][17]
Definition and place in treatment
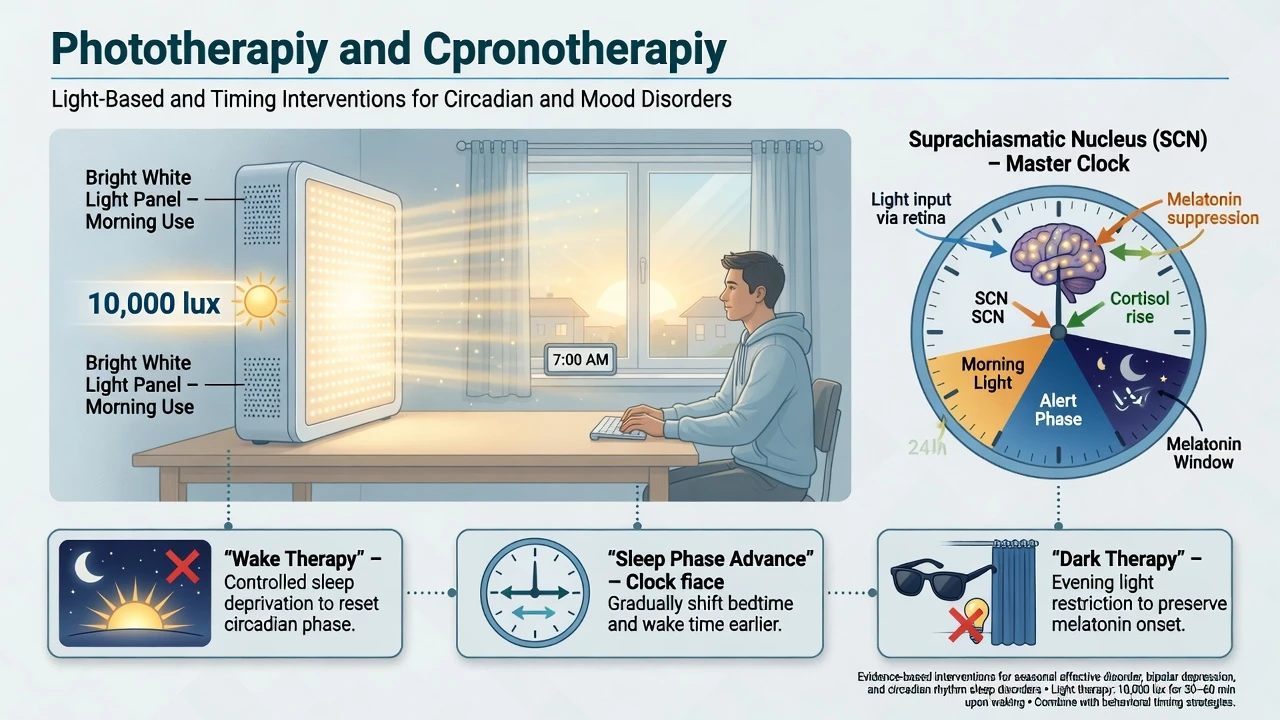
Phototherapy (bright light therapy, BLT) is controlled exposure to bright artificial light at a prescribed intensity, duration, and clock time to treat mood disorders and realign circadian phase. It is not "sitting near a window and hoping," though natural morning light is a useful behavioural adjunct. Chronotherapy is the broader class of interventions that manipulate biological rhythms: BLT, wake therapy (therapeutic sleep deprivation), sleep phase advance (SPA), dark therapy, and timed melatonin as a phase-shifting agent.[6][7]
In stepped care, BLT is often first-line for winter-type seasonal pattern major depression and an evidence-based adjunct or monotherapy option in selected nonseasonal MDD. It sits alongside antidepressants, CBT-SAD, and — when severity demands — hospitalisation or ECT. Chronotherapeutic combinations are specialist rapid-response packages, not casual DIY overnight experiments.[5][7][14][15]
Classification of chronotherapeutic tools
| Tool | Core action | Classic exam indication |
|---|---|---|
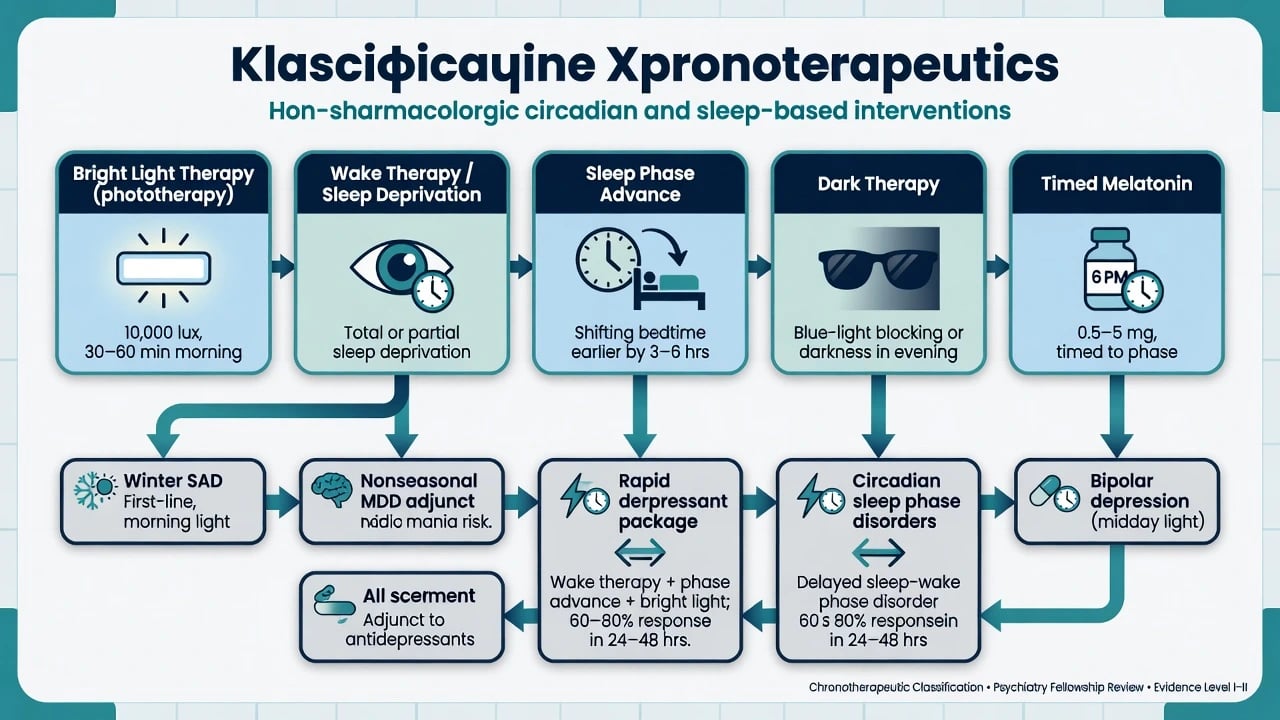
| Bright light therapy | Morning phase advance + antidepressant signal | Winter SAD; nonseasonal MDD mono/adjunct |
| Midday BLT (bipolar protocols) | Antidepressant signal with lower early-morning switch concern in Sit programme | Bipolar depression under stabiliser cover |
| Wake therapy (TSD/partial) | Rapid antidepressant effect within hours–1 day | Severe depression inpatient packages |
| Sleep phase advance | Stabilise response after wake therapy | Combined chronotherapy |
| Dark therapy | Reduce light stimulation in mania/mixed states | Specialist bipolar adjunct |
| Timed melatonin | Phase shift (PRC roughly opposite light) | DSPS and jet lag; adjunct rhythm care |
| These are teaching scaffolds — local protocols govern exact schedules.[6][7][11][17] |
Epidemiology and clinical need
Winter-type seasonal pattern depression is more common at higher latitudes and often presents with reverse-vegetative (atypical) features: hypersomnia, hyperphagia with carbohydrate craving, and marked anergy. Seasonal pattern is a specifier of major depressive (or bipolar) episodes across successive years, not a freestanding casual diagnosis of "winter blues."[1]
Meta-analyses support BLT efficacy for SAD (Golden; Pjrek updated synthesis with significant advantage over placebo on depression ratings and response). For nonseasonal depression, Al-Karawi and colleagues meta-analysed clinical trials favouring BLT, particularly as monotherapy over multi-week courses, while Lam 2016 provides a landmark RCT of light, fluoxetine, and combination versus sham–placebo conditions.[5][15][16][18]
Pathophysiology and circadian mechanisms
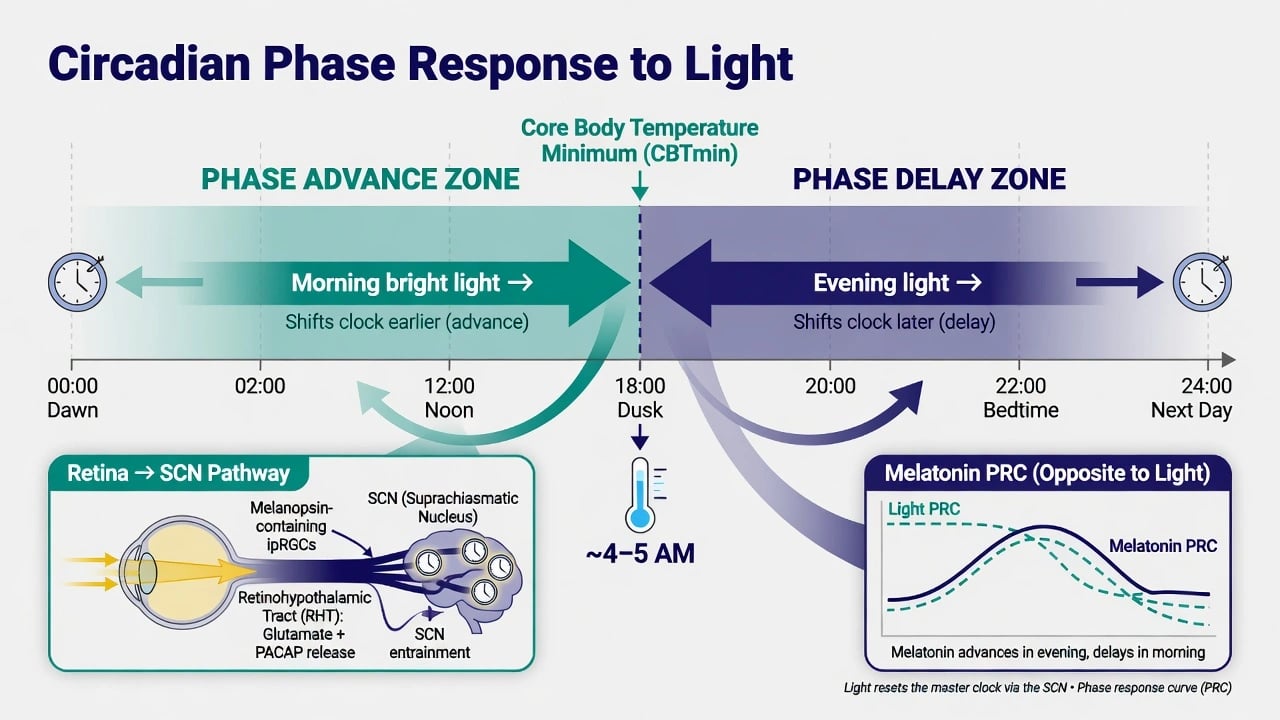
Light reaches intrinsically photosensitive retinal ganglion cells and projects via the retinohypothalamic tract to the suprachiasmatic nucleus (SCN) — the master circadian pacemaker. The phase response curve (PRC) for light is viva core material: light in the biological morning (after the core body temperature minimum) advances the clock (earlier sleep propensity); light in the biological evening/night delays it. Melatonin's PRC is approximately opposite, which is why timing matters more than "melatonin equals sleeping tablet" folklore.[6][9][10]
Phase-delay hypotheses of winter depression (Lewy and colleagues) propose that many patients with winter depression are phase-delayed relative to sleep, so morning light that advances the circadian system can improve alignment and mood. Therapeutic response relates to circadian time of administration, not merely total lux-hours without a clock context.[9][10]
Wake therapy produces rapid antidepressant effects through interrelated monoaminergic, glutamatergic, and circadian mechanisms; the clinical problem is relapse after recovery sleep, which combination packages (light, SPA, lithium/antidepressants) aim to lock in.[7][12][13]
Clinical presentation and time course
SAD phenotype. Recurrent autumn–winter major depressive episodes with spring–summer remission; reverse vegetative signs are classic teaching hooks but not mandatory for diagnosis. Subsyndromal seasonal symptoms exist but should not dilute criteria for major depression when risk is high.[1]
BLT time course. Some patients improve within days; controlled winter trials (Eastman) emphasised that a specific antidepressant effect versus placebo may take about three weeks to declare clearly — exam-safe nuance against overclaiming overnight cure for every patient.[2][3]
Morning versus evening. Lewy and colleagues and related programmes favour morning light over evening light for winter depression efficacy and circadian logic; evening bright light risks insomnia and phase delay.[4][6]
Wake therapy time course. Improvement can appear within 24 hours; without stabilisation, many lose gains after sleep resumes — hence triple chronotherapy thinking.[7][12]
Numbers every candidate must own
These are exam orientation numbers from protocols and landmark programmes — individualise distance, device validation, and comorbidity.[6][8][15][18]
Differential diagnosis that changes the plan
| Presentation | Prefer | Do not miss |
|---|---|---|
| Winter low mood without major episode criteria | Behavioural light, exercise, watchful waiting | Over-medicalising normal seasonality |
| Seasonal pattern + prior mania/hypomania | Bipolar pathway; midday BLT under stabiliser | Unipolar SAD morning megadoses unsupervised |
| Hypersomnia dominant | OSA, hypothyroid, substances work-up | Light box as sole explanation |
| Delayed sleep phase with low mood | DSPS chronotherapy (morning light + evening melatonin timing principles) | Antidepressant-only without rhythm plan |
| Severe melancholic/psychotic winter depression | Urgent psychiatry intensity; consider ECT | Light box as sole therapy |
| Seasonality is a pattern, not a safety guarantee.[1][6][11][17] |
Assessment before prescribing light
Document: major depression criteria and seasonal pattern (≥2 years of seasonal relationship for classic SAD teaching); bipolar screen; sleep–wake schedule and work light exposure; substance use; ocular history; photosensitising medicines; migraine/epilepsy if relevant; MSE and suicide risk at the same intensity as any depression; capacity and consent for device use and mania watch.[6][8]
Scales that examiners may name: SPAQ (seasonality), SIGH-SAD (structured interview for seasonal depression severity), plus PHQ-9/MADRS for nonseasonal trial framing.[6][15]
Investigations
No routine laboratory is required purely to "approve" BLT. Investigate as for any depressive presentation when organic differentials are live. Ophthalmology review is prudent for retinal disease, significant cataract decisions, recent eye surgery, or high-risk photosensitivity. Actigraphy/DLMO are research/specialist tools, not mandatory clinic entry tickets for standard morning BLT.[6]
Acute and safety management
Hypomania/mania on light: stop or substantially reduce BLT immediately, reassess bipolar diagnosis, institute or optimise mood stabilisation, and contain risk.[6][11]
Severe depression: active SI, psychosis, catatonia, or nutritional collapse need the full acute pathway — BLT may continue as an adjunct only when logistics allow, never as a substitute for containment.[7][13]
Ocular pain or severe photophobia: cease BLT and obtain ophthalmic assessment.[6]
Wake therapy nights: supervised settings for high-risk patients; monitor falls, agitation, and mood elevation, especially in bipolar spectrum illness.[7][12]
Definitive management protocols
Standard bright light therapy (unipolar seasonal teaching scaffold)
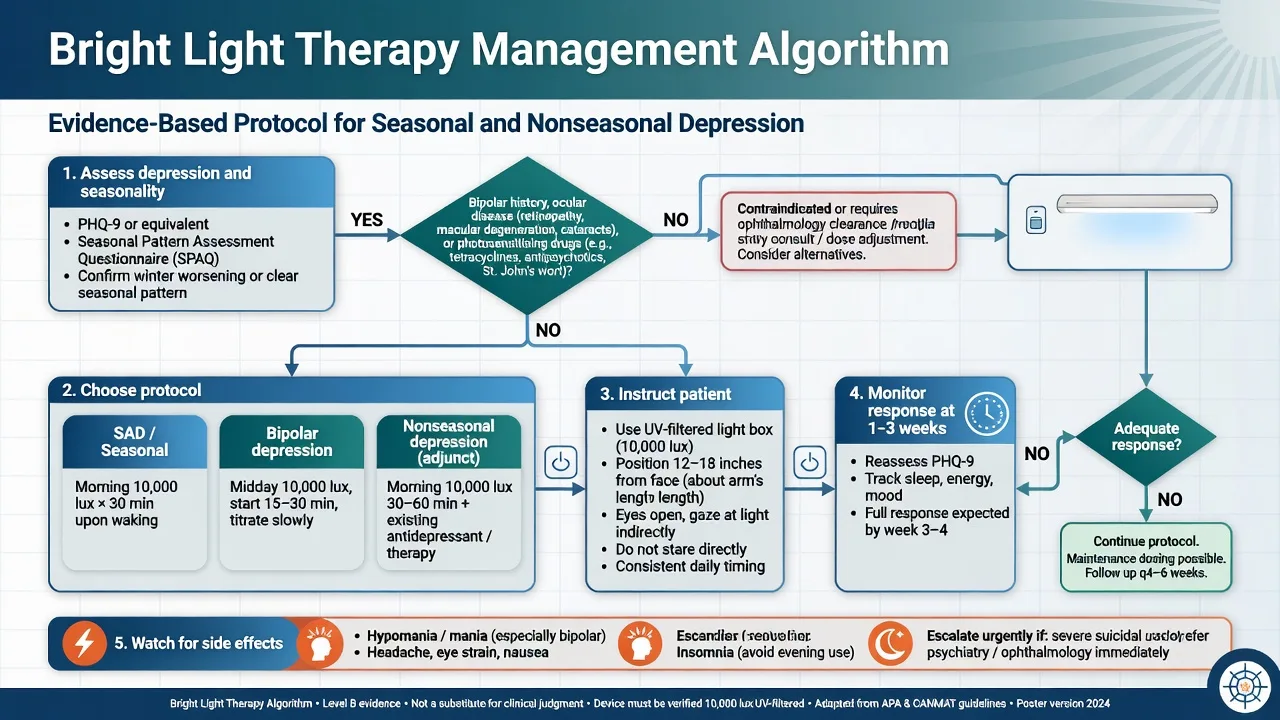
Device: commercial light box delivering approximately 10,000 lux at the manufacturer's recommended distance, with UV filtration, diffuse white light (not unvalidated coloured gadgets as exam first choice). Patient sits with eyes open, facing toward the box while reading or working — not staring into the lamps. Typical starting prescription: ~30 minutes shortly after habitual wake time, daily through the symptomatic season. Older protocols used ~2,500 lux for 1–2 hours; intensity and duration trade off roughly inversely within validated ranges.[5][6]
Timing pearl: individual circadian time can refine morning placement; Terman and colleagues linked circadian timing of morning light to therapeutic response in winter depression.[10]
Can-SAD: light versus fluoxetine in winter SAD
Lam and colleagues' Can-SAD RCT found light therapy and fluoxetine 20 mg oral daily comparably effective for winter seasonal affective disorder, with light showing a faster early response signal and a different adverse-effect profile (more agitation early with light in some reports; more sexual/side-effect burden patterns with SSRI). Exam message: offer either evidence-based option and choose by preference, logistics, comorbidities, and speed needed.[8]
Nonseasonal major depression: Lam 2016
In nonseasonal MDD, 30 minutes of morning bright light as monotherapy and especially light plus fluoxetine 20 mg oral daily outperformed sham device plus placebo pill on MADRS change; fluoxetine monotherapy did not clearly beat placebo in that four-arm design. Use this when examiners ask whether light is "only for SAD."[15][16]
Bipolar depression: Sit programme principles
Early case-series work raised switch concerns with morning light in bipolar disorder. Sit and colleagues later showed adjunctive midday bright white light (roughly noon to mid-afternoon window), titrated from shorter sessions toward about 45–60 minutes, under concurrent mood-stabiliser treatment, with remission advantages versus dim red placebo light in a double-blind trial. Exam rules: mood stabiliser cover, titrate duration, prefer midday over unsupervised aggressive early morning in bipolar depression, monitor for mixed/manic switch daily early on.[11][17]
Wake therapy and combination chronotherapy
Total sleep deprivation (wake therapy) for one night (or repeated alternate-night protocols) can produce rapid antidepressant effects. Colombo and Benedetti programmes combine TSD with light and often lithium in bipolar depression to enhance and sustain response; Benedetti and colleagues also reported rapid reduction of suicidal symptoms within chronotherapeutic packages in drug-resistant bipolar depression — still inside comprehensive risk care, not as a solo discharge plan.[7][12][13]
Triple chronotherapy teaching package: wake therapy + sleep phase advance + morning BLT (schedules vary by centre). Feasible in specialist inpatient or carefully structured outpatient pathways; requires staffing, consent, and mania/SI monitoring.[7]
CBT-SAD and durability
Rohan and colleagues showed CBT adapted for SAD is acutely competitive with light and may offer better durability across subsequent winters after the acute phase — pair behavioural skills with light rather than treating them as mutually exclusive forever.[14]
Adverse effects and practical troubleshooting
Common: headache, eye strain, nausea, irritability, insomnia (especially if timed too late), agitation. Serious: hypomania/mania. Mitigate with correct morning timing, gradual duration build if sensitive, UV-filtered validated devices, and early review at 3–7 days then 2–3 weeks.[6]
Special populations
Older adults. May benefit; screen cataracts/glaucoma and falls; start carefully with seating stability and eye comfort.[6]
Youth. Limited high-quality trial depth relative to adults — specialist paediatric/adolescent practice; do not invent adult lux rules as paediatric licence without supervision.[6]
Pregnancy. Non-drug appeal for mild–moderate seasonal symptoms is real; severe perinatal depression still follows full perinatal pathways (including ECT when indicated).[6][15]
Ocular disease and photosensitising drugs. Specialist ophthalmic/medication review before high-intensity BLT.[6]
Prognosis and disposition
Many SAD responders continue daily light through the dark months and stop or taper in spring. Recurrence next winter is common without a prevention plan (early autumn light restart; CBT-SAD skills; selected pharmacoprevention belongs primarily in SAD pharmacotherapy topics). Non-responders after 2–4 weeks of adequate BLT need dose/timing audit, bipolar re-screen, and stepped antidepressant or specialty care — not endless underdosed gadgets.[6][8][14][18]
Evidence, guidelines and regional differences
| Source | Exam take-home |
|---|---|
| Rosenthal 1984 | SAD syndrome + early light findings |
| Eastman 1998 | Placebo-controlled winter BLT; multi-week specificity |
| Terman 1998 | Timed bright light (± ions) antidepressant signal |
| Lewy 1998 / 2006 | Morning vs evening; circadian basis of winter depression |
| Terman 2001 | Circadian time of morning light predicts response |
| Golden 2005 | Meta-analysis supports light for mood disorders |
| Terman 2005 CNS | Protocol, safety, side-effect handbook depth |
| Wirz-Justice 2005 | Chronotherapeutics class: light + wake therapy |
| Can-SAD 2006 | Light ≈ fluoxetine 20 mg oral in winter SAD |
| Lam 2016 | Nonseasonal MDD: light ± fluoxetine > sham–placebo |
| Al-Karawi 2016 | Nonseasonal BLT meta-support |
| Sit 2007/2018 | Bipolar light: switch caution → midday adjunct RCT |
| Colombo/Benedetti | TSD + light ± lithium rapid packages |
| Rohan 2015 | CBT-SAD vs light acute outcomes |
| Pjrek 2020 | Updated SAD BLT meta-analysis |
| Landmark synthesis for viva speed.[1][2][5][8][15][17][18] |
ANZ: Light therapy is established for seasonal pattern depression in specialist and primary care teaching; device quality and patient education vary — quote principles (10,000 lux, morning timing, UV filter) rather than inventing current subsidy codes. Align with RANZCP-informed mood disorder practice and local health-service protocols. UK: NICE depression guidance historically emphasises psychological and pharmacological stepped care; BLT is commonly discussed for SAD in clinical practice — state evidence and patient preference without inventing a single universal NHS device pathway. US/Canada: APA and CANMAT traditions strongly support BLT for SAD; Can-SAD and Lam nonseasonal data are North American exam staples. Europe: Strong chronobiology centres (Wirz-Justice, Benedetti lineages) normalise wake therapy packages in specialist units. Exact product standards and funding are local — principles travel.[5][7][8][15]
Exam pearls
LIGHT rules for BLT
LIGHT
References
- [1]Rosenthal NE, Sack DA, Gillin JC, et al. Seasonal affective disorder. A description of the syndrome and preliminary findings with light therapy. Arch Gen Psychiatry, 1984.PMID 6581756
- [2]Eastman CI, Young MA, Fogg LF, et al. Bright light treatment of winter depression: a placebo-controlled trial. Arch Gen Psychiatry, 1998.PMID 9783558
- [3]Terman M, Terman JS, Ross DC. A controlled trial of timed bright light and negative air ionization for treatment of winter depression. Arch Gen Psychiatry, 1998.PMID 9783557
- [4]Lewy AJ, Bauer VK, Cutler NL, et al. Morning vs evening light treatment of patients with winter depression. Arch Gen Psychiatry, 1998.PMID 9783559
- [5]Golden RN, Gaynes BN, Ekstrom RD, et al. The efficacy of light therapy in the treatment of mood disorders: a review and meta-analysis of the evidence. Am J Psychiatry, 2005.PMID 15800134
- [6]Terman M, Terman JS. Light therapy for seasonal and nonseasonal depression: efficacy, protocol, safety, and side effects. CNS Spectr, 2005.PMID 16041296
- [7]Wirz-Justice A, Benedetti F, Berger M, et al. Chronotherapeutics (light and wake therapy) in affective disorders. Psychol Med, 2005.PMID 16045060
- [8]Lam RW, Levitt AJ, Levitan RD, et al. The Can-SAD study: a randomized controlled trial of the effectiveness of light therapy and fluoxetine in patients with winter seasonal affective disorder. Am J Psychiatry, 2006.PMID 16648320
- [9]Lewy AJ, Lefler BJ, Emens JS, et al. The circadian basis of winter depression. Proc Natl Acad Sci U S A, 2006.PMID 16648247
- [10]Terman JS, Terman M, Lo ES, et al. Circadian time of morning light administration and therapeutic response in winter depression. Arch Gen Psychiatry, 2001.PMID 11146760
- [11]Sit D, Wisner KL, Hanusa BH, et al. Light therapy for bipolar disorder: a case series in women. Bipolar Disord, 2007.PMID 18076544
- [12]Colombo C, Lucca A, Benedetti F, et al. Total sleep deprivation combined with lithium and light therapy in the treatment of bipolar depression: replication of main effects and interaction. Psychiatry Res, 2000.PMID 10904122
- [13]Benedetti F, Riccaboni R, Locatelli C, et al. Rapid treatment response of suicidal symptoms to lithium, sleep deprivation and light therapy (chronotherapeutics) in drug-resistant bipolar depression. J Clin Psychiatry, 2014.PMID 24345382
- [14]Rohan KJ, Mahon JN, Evans M, et al. Randomized Trial of Cognitive-Behavioral Therapy Versus Light Therapy for Seasonal Affective Disorder: Acute Outcomes. Am J Psychiatry, 2015.PMID 25859764
- [15]Lam RW, Levitt AJ, Levitan RD, et al. Efficacy of Bright Light Treatment, Fluoxetine, and the Combination in Patients With Nonseasonal Major Depressive Disorder: A Randomized Clinical Trial. JAMA Psychiatry, 2016.PMID 26580307
- [16]Al-Karawi D, Jubair L. Bright light therapy for nonseasonal depression: Meta-analysis of clinical trials. J Affect Disord, 2016.PMID 27011361
- [17]Sit DK, McGowan J, Wiltrout C, et al. Adjunctive Bright Light Therapy for Bipolar Depression: A Randomized Double-Blind Placebo-Controlled Trial. Am J Psychiatry, 2018.PMID 28969438
- [18]Pjrek E, Friedrich ME, Cambioli L, et al. The Efficacy of Light Therapy in the Treatment of Seasonal Affective Disorder: A Meta-Analysis of Randomized Controlled Trials. Psychother Psychosom, 2020.PMID 31574513