Psych · Psychopharmacology — pregnancy and lactation
Psychopharmacology in pregnancy and lactation
Also known as Perinatal psychopharmacology · Psychotropics in pregnancy · Antidepressants pregnancy · Lithium pregnancy · Valproate pregnancy · Breastfeeding psychotropics · Lactation psychopharmacology · Perinatal medication counselling
Exam-exhaustive fellowship perinatal psychopharmacology — untreated illness versus drug risks, antidepressants (cardiac absolute risk, PNAS, PPHN), antipsychotics and gestational diabetes, lithium/valproate/lamotrigine hierarchy with valproate avoid, benzodiazepines, lactation RID principles, shared decision and multi-guideline frames. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship examiners test whether you can counsel in absolute risks, name the landmark signals (Huybrechts, Patorno, EURAP/NEAD, Grigoriadis, Viguera), and run a continue / switch / stop / dose-adjust algorithm without ideology. This topic is the drug spine for perinatal mood, bipolar, psychosis and CASC medication stations.[18][20][22]
Definition and decision domains
Perinatal psychopharmacology is not a single “safe drug list.” It is structured prescribing across preconception, trimesters, labour/delivery, and lactation, integrating five domains every time: (1) severity and natural history of the maternal illness, (2) fetal/neonatal drug risk by window, (3) obstetric and metabolic risk, (4) lactation goals, and (5) values, capacity and social support.[18][22]
Baseline major congenital malformation (MCM) risk in the general population is roughly 2–3%. Every drug conversation starts from that floor so candidates do not invent a “zero-risk non-drug pregnancy.”[4][10]
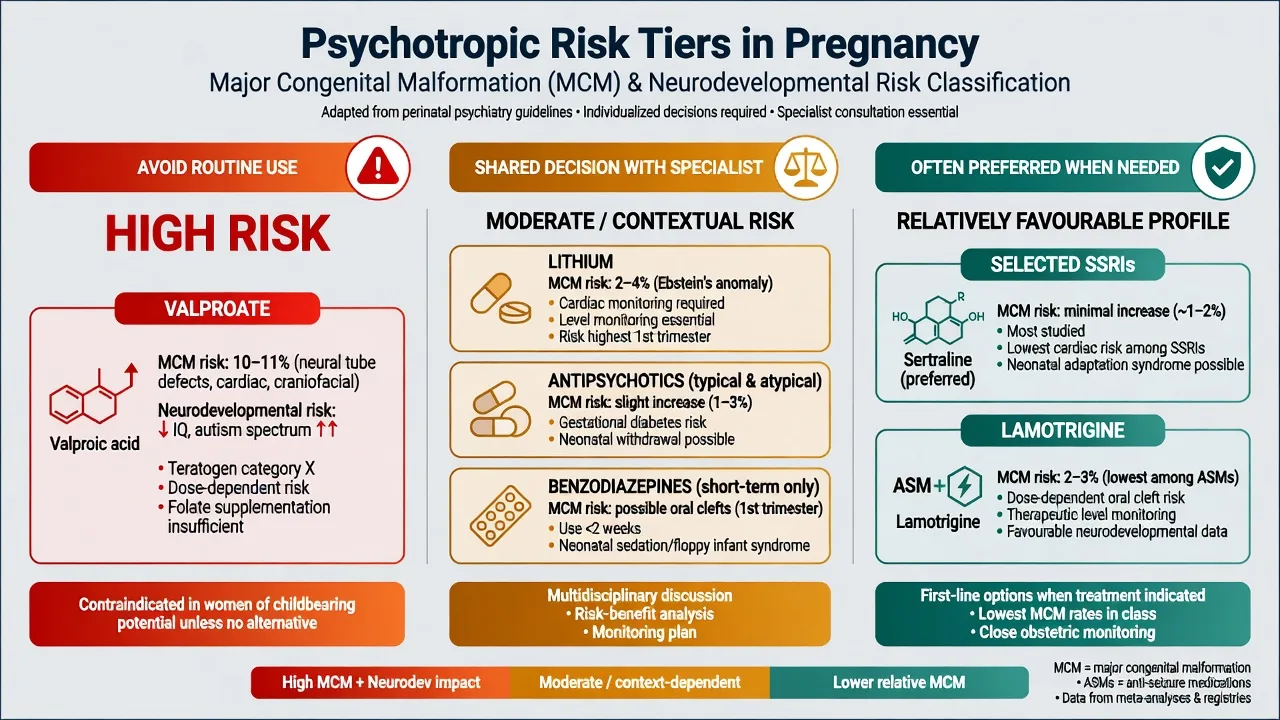
| Tier | Agents (exam examples) | Exam action |
|---|---|---|
| Avoid as routine | Valproate (highest MCM and neurodevelopmental signal among common ASMs) | Switch before conception whenever feasible; pregnancy-prevention programmes where mandated |
| Shared decision / specialist | Lithium; many SGAs; carbamazepine; short-term benzodiazepines | Document absolute risks, monitoring, and alternatives |
| Often preferred when a drug is needed | Selected SSRIs (e.g. sertraline frequently cited); lamotrigine relatively favourable MCM among ASMs | Still not “risk free” — dose, indication, and neonate plans matter |
| Class tiers organise viva answers; individual history still overrides any table row.[9][10][11][4][22] |
Epidemiology and untreated-illness risk
Antenatal depression is associated with preterm birth, low birth weight and intrauterine growth restriction in meta-analysis — the classic counterweight to “just stop the tablet.”[1]
In bipolar disorder, discontinuing mood stabilisers in pregnancy is associated with high recurrence risk; Viguera and colleagues showed substantial relapse after discontinuation versus continuation frameworks, and earlier lithium-discontinuation work showed high recurrence whether pregnant or not — pregnancy is not protective.[2][3]
The postpartum window concentrates risk for bipolar recurrence and postpartum psychosis, which is a psychiatric emergency with mother–infant safety implications.[21][8]
Numbers examiners expect you to frame (order-of-magnitude)
Pathophysiology — windows, placenta, milk
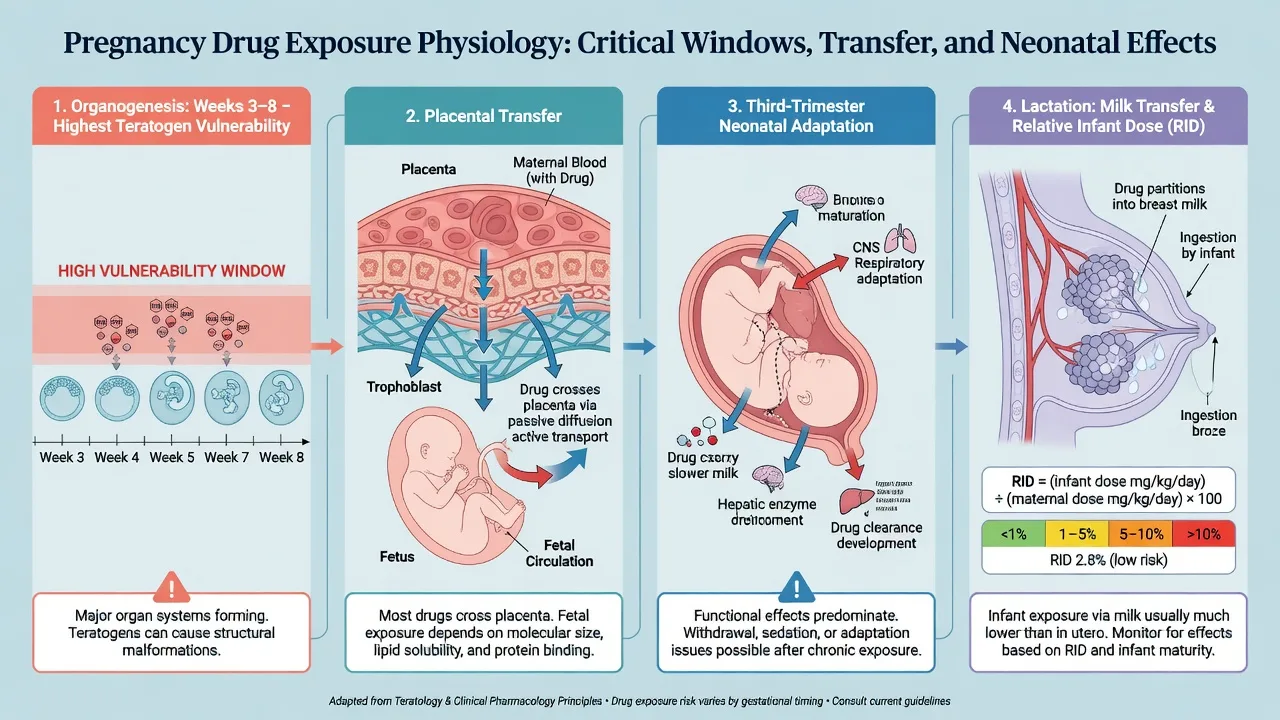
Organogenesis (roughly embryonic weeks 3–8) is the major structural teratogen window (neural tube, cardiac septation, other organ systems). Later pregnancy risks shift toward growth, preterm birth, neonatal adaptation, and functional outcomes.[22][9]
Placental transfer means almost all psychotropics reach the fetus to some degree; fetal drug-metabolising enzyme and transporter ontogeny change exposure across gestation. Third-trimester physiology (expanded volume of distribution, GFR rise then peripartum swings) alters levels — lithium is the classic exam example requiring closer levels.[7][8][22]
Lactation exposure is quantified clinically with concepts such as milk:plasma ratio and relative infant dose (RID) — infant dose as a percentage of the weight-adjusted maternal dose. Many teaching frameworks treat RID under about 10% as relatively more reassuring for term healthy infants, but prematurity, polypharmacy, and poor feeding override any single cut-off. “Pump and dump forever” is usually wrong teaching.[22][8]
Clinical approach and bedside assessment
Structure every consultation: illness history and pole (unipolar vs bipolar vs psychosis), prior perinatal episodes, suicide and infant-related risk language (precise, non-stigmatising), sleep, supports, substance use, obstetric dating, folic acid, and contraception if not pregnant. Capacity for shared decision and documentation standards matter as much as the molecule chosen.[18][19][21]
Investigations are indication-driven: pregnancy test before teratogenic agents; baseline metabolic panel and ECG when starting antipsychotics; lithium baseline renal/thyroid/calcium and serial troughs; high-resolution anomaly ultrasound and fetal echo pathways when lithium or other higher-concern exposures occur — follow local obstetric protocol rather than inventing a universal scan list.[7][22][19]
Shared decision algorithm
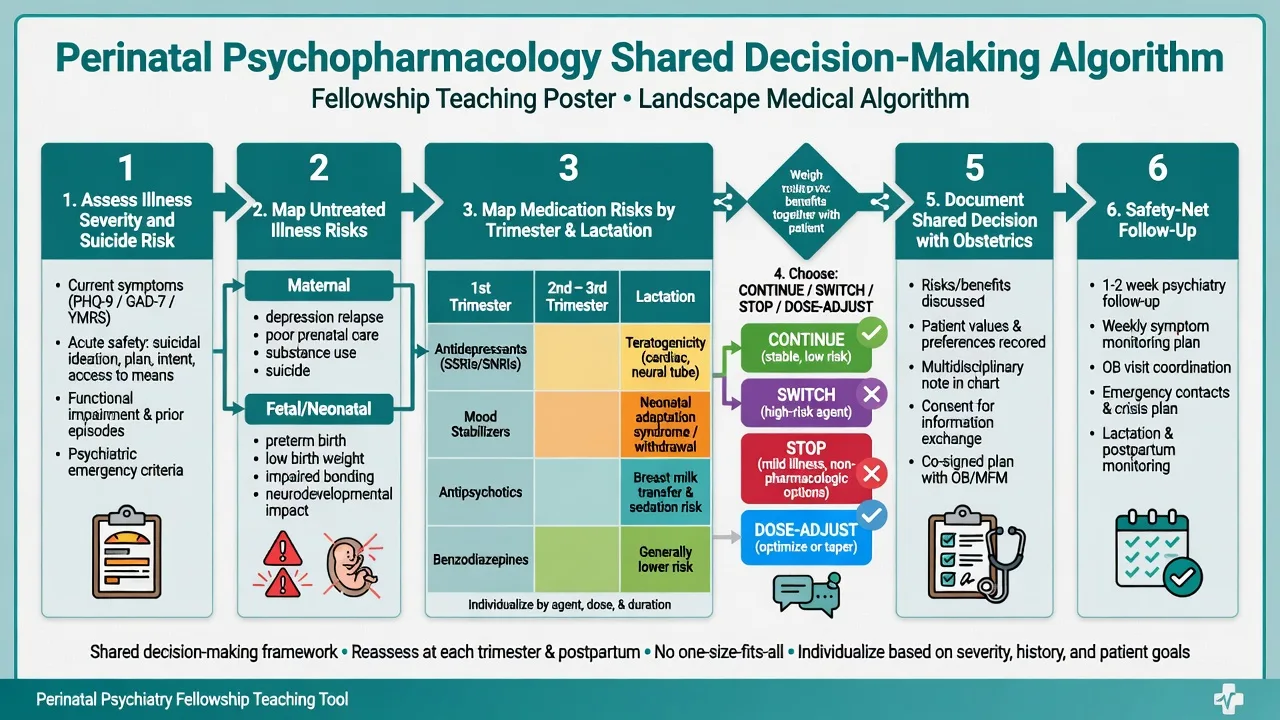
- Stabilise safety — suicide, psychosis, mania, domestic safety, legal status principles (jurisdiction-specific statutes — do not invent section numbers).[21]
- Map illness risk if untreated or undertreated — relapse data (Viguera), depression birth-outcome meta-analysis (Grote), bonding and care capacity.[1][2]
- Map drug risk by window — first-trimester MCM, third-trimester neonatal syndromes, lactation.[4][5][22]
- Choose one of four actions: continue effective monotherapy; switch to a better-characterised agent before conception when time allows; stop if mild illness and strong non-drug plan; dose-adjust (e.g. lithium levels; lamotrigine rises in pregnancy).[22][8]
- Coordinate with obstetrics, primary care, and when needed perinatal psychiatry / mother–baby services.[19][20]
CARERS
Antidepressants in pregnancy and lactation
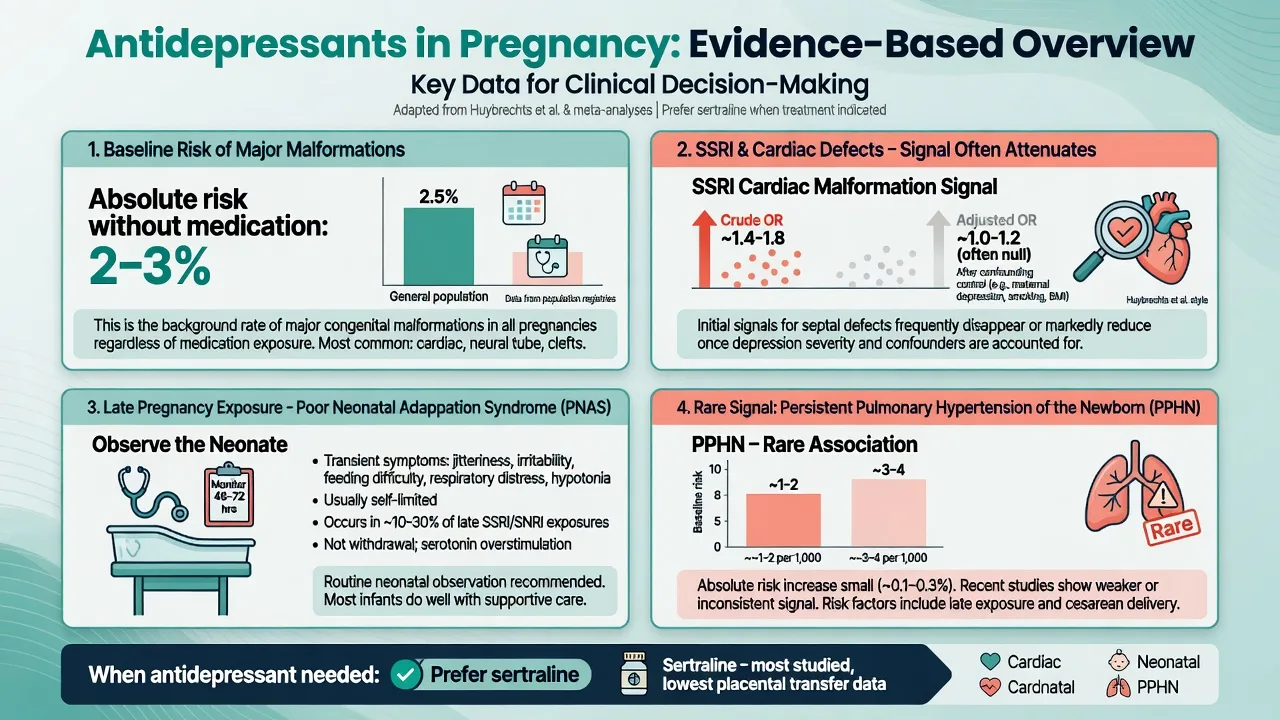
Cardiac defects. Large confounding-adjusted work (Huybrechts et al., NEJM) found that the association between antidepressants and cardiac defects attenuates substantially after adjustment — exam pearl: do not recite unadjusted scare figures as if they were causal truth.[4]
Poor neonatal adaptation syndrome (PNAS) after late-pregnancy SSRI/SNRI exposure is supported by meta-analysis: transient respiratory, tone, feeding and irritability signs — usually self-limited but warrants neonatal observation, not reflexive maternal drug cessation at 36 weeks without a relapse plan.[5]
Persistent pulmonary hypertension of the newborn (PPHN) has a small absolute increased risk signal in meta-analysis after late SSRI exposure — rare enough that counselling must keep perspective against baseline rates and untreated depression harms.[6]
Agent choice (practical fellowship defaults, always individualise): many services prefer sertraline or other well-characterised SSRIs when an antidepressant is needed, including lactation contexts; paroxetine historically attracted more cardiac concern messaging and is often avoided as a first new start in pregnancy when alternatives exist. Dosing is standard adult antidepressant ranges with clinical titration — e.g. sertraline commonly initiated around 50 mg oral daily and titrated (product information / local formulary). Never invent exotic pregnancy-only doses without a source.[18][19][22]
Lactation. Sertraline is frequently preferred because of favourable milk transfer data relative to some alternatives; still monitor infant sleep, feeding and weight. Avoid blanket “cannot breastfeed on any SSRI.”[22][20]
Antipsychotics
Multi-country analyses of in-utero antipsychotic exposure (Huybrechts et al., JAMA Psychiatry) inform modern malformation counselling — overall signals are generally modest after design strengths, and illness severity confounding remains critical.[13]
Gestational diabetes risk rises with continuation of several atypical antipsychotics in early pregnancy (Park et al.) and in register data (Heinonen et al.) — counsel metabolic screening, dietetic support, and prefer the lowest effective metabolic burden agent that still treats psychosis or mania.[14][15]
Clozapine is never stopped casually in pregnancy because of relapse risk in treatment-resistant schizophrenia; coordinate haematology, obstetric high-risk care, and neonatal plans — specialised review, not exam dogma to stop at first positive test.[22]
Acute mania or psychosis in pregnancy prioritises safety, legal frameworks, and an antipsychotic the patient has previously responded to when known; add mood stabiliser logic only after pregnancy-tier filters (no casual valproate).[21][19]
Mood stabilisers — lithium, valproate, lamotrigine hierarchy
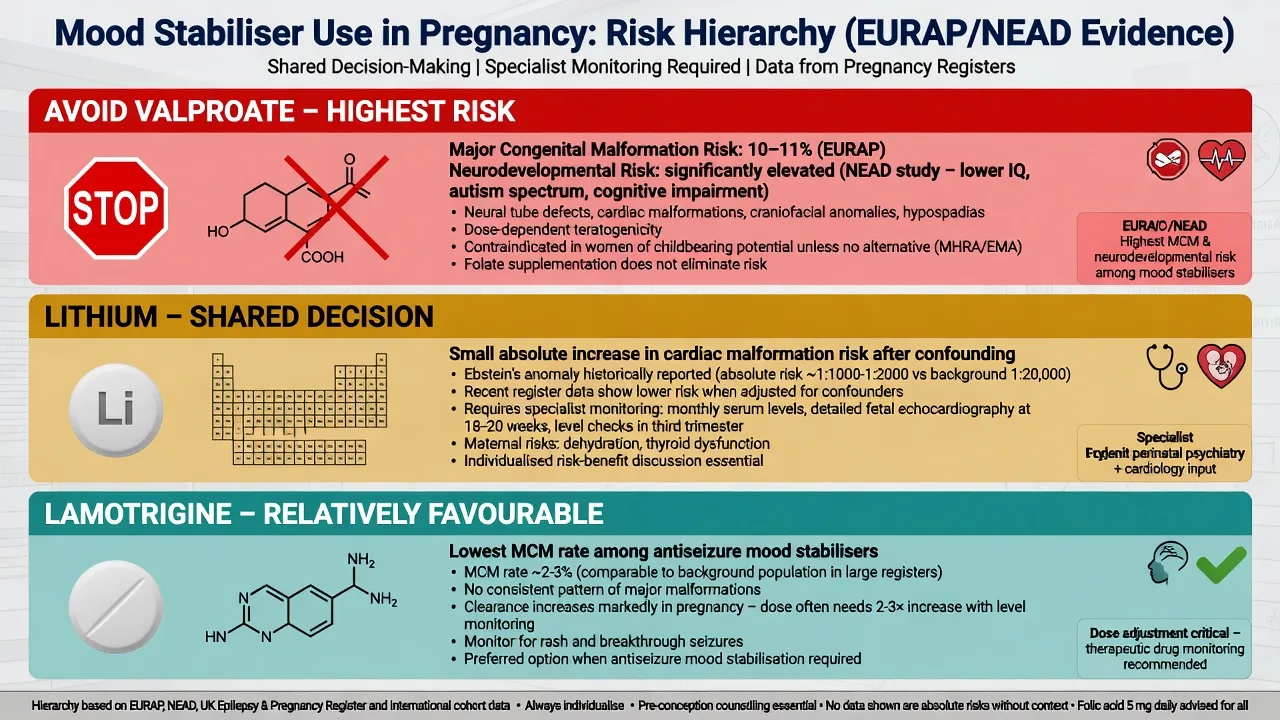
Valproate — avoid as routine
EURAP and related ASM registries show dose-dependent major malformation risk highest with valproate among commonly used antiseizure/mood agents; modern monotherapy registry updates (Battino/Tomson) keep valproate at the top of concern.[9][10]
NEAD cognitive data show adverse neurodevelopmental / IQ outcomes after fetal valproate versus other ASMs at ages 3 and 6 years — this is the exam reason valproate is not merely “another mood stabiliser.”[11][12]
Lithium — shared decision, not automatic ban
Patorno et al. (NEJM) re-estimated cardiac malformation risk with first-trimester lithium: elevated versus non-exposed, but absolute risks remain small after modern design — far from historical overstatement, and not an automatic stop for every stable bipolar patient.[7]
Fornaro et al. systematic review/meta-analysis synthesises pregnancy and postpartum lithium safety and efficacy outcomes — useful when examiners ask for more than one citation.[8]
Practical lithium plan: preconception counselling; folic acid per obstetric norms; more frequent levels as GFR rises; discuss anomaly scan / fetal echo pathways; peripartum plan for maternal level shifts and neonatal observation (hypotonia, feeding, thyroid/renal concerns in exposed neonates). Breastfeeding on lithium is possible only with strict infant monitoring frameworks in specialised settings — many services still counsel caution or alternatives depending on supports.[7][8][22]
Lamotrigine
Among ASMs used in bipolar care, lamotrigine generally shows a more favourable MCM profile than valproate in registry hierarchies, though not zero risk.[9][10]
Pregnancy often lowers lamotrigine levels (clearance rise) — dose increases with level/clinical monitoring and structured postpartum reduction plans prevent toxicity after delivery. Slow titration / rash rules still apply whenever (re)starting.[22][10]
Benzodiazepines and sedatives
Meta-analyses (Grigoriadis) examine congenital malformation signals and broader pregnancy/delivery outcomes with benzodiazepine exposure, alone or with antidepressants — signals are heterogeneous and confounded; exam stance is short-term, lowest dose, avoid poly-sedative stacks, and plan for neonatal hypotonia / withdrawal / respiratory depression if late exposure occurs.[16][17]
Do not use benzodiazepines as a long-term “pregnancy anxiolytic strategy” when SSRI, psychological therapy, or illness-specific treatment is indicated.[18][20]
Lactation principles
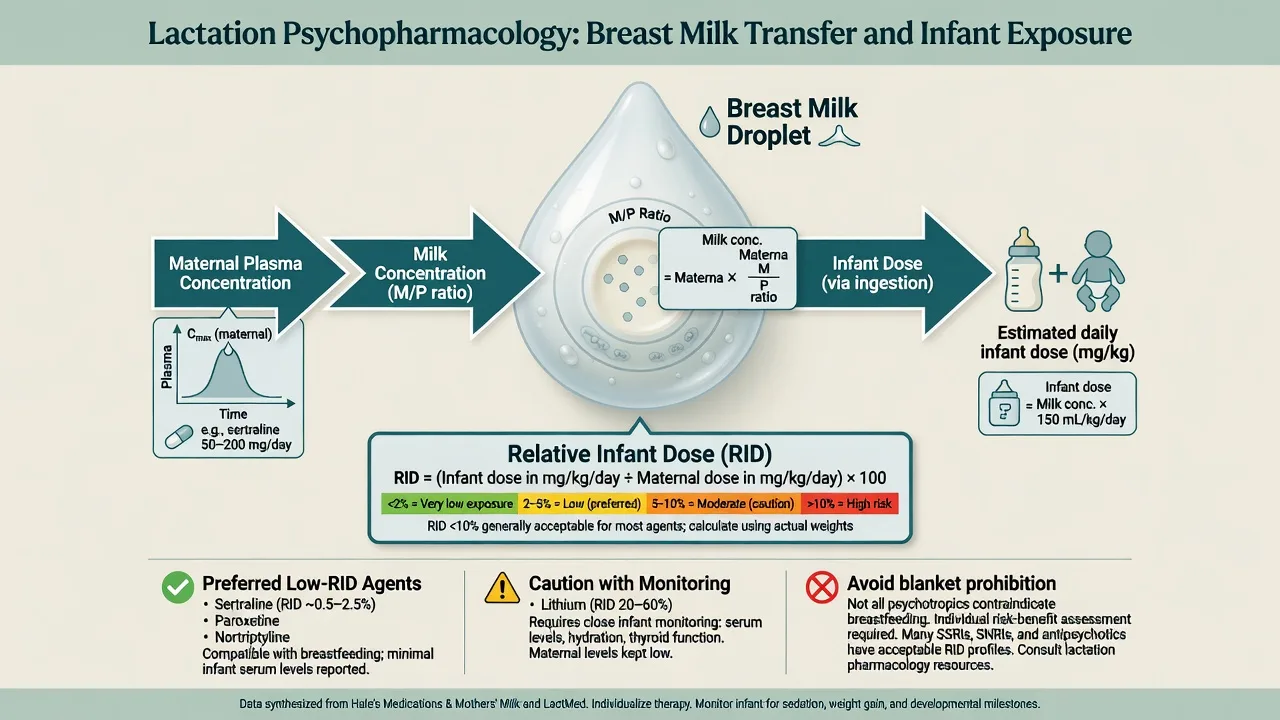
Principles that pass exams: prefer monotherapy at the lowest effective maternal dose; prefer agents with more lactation data and lower transfer when efficacy is equal (sertraline often cited among antidepressants); calculate/consult RID where data exist (RID under about 10% is a relative reassurance teaching cut-off for many term infants — not absolute safety); premature or ill infants tolerate exposure less well; lithium and clozapine need specialist lactation plans with infant clinical review ± levels per local protocol; do not stop breastfeeding solely because a drug is “psychotropic”; coordinate with paediatricians when exposure is higher-risk.[22][8][20]
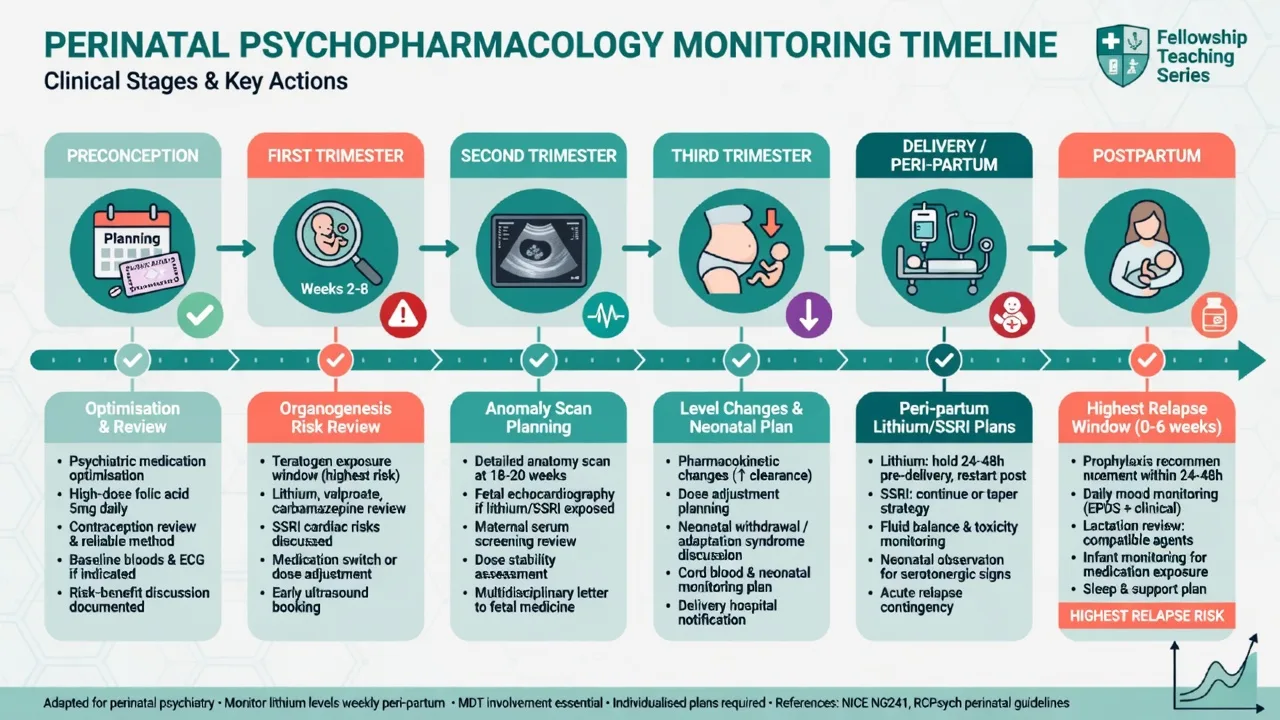
Timeline: preconception to postpartum
| Phase | High-yield tasks |
|---|---|
| Preconception | Optimise diagnosis and monotherapy; stop/switch valproate; document contraception until plan set; folic acid; relapse history |
| T1 | Confirm dating; avoid panic poly-switches; anomaly-scan pathway if higher-risk drug |
| T2–T3 | Levels (lithium, sometimes lamotrigine); GDM screening if SGA; birth plan and neonatal observation plan |
| Delivery | Lithium level/peripartum strategy; avoid sedative stacking; neonatal team aware |
| Postpartum | Highest bipolar/psychosis risk window; sleep protection; restart/continue prophylaxis; lactation review |
| Postpartum planning is part of antenatal care, not an afterthought.[2][8][21][19] |
Acute / emergency scenarios
Postpartum psychosis — rapid onset mania, confusion, delusions often with infant content: emergency assessment, do not leave mother alone with infant if risk unclear, admit to appropriate unit, treat as bipolar-spectrum emergency (antipsychotic ± lithium, ECT in selected severe cases). Prior episode informs prophylaxis for subsequent pregnancies.[21][8]
Severe depression with risk — do not withhold treatment because of pregnancy; stepped care includes intensive psychological therapy, antidepressant when indicated, and ECT for life-threatening illness — pregnancy is not a contraindication to emergency psychiatry.[18][19]
Neonatal adaptation after late SSRI/benzo — observe, support feeding/respiration, avoid labelling all jitteriness as permanent injury.[5][17]
Complications and pitfalls
- Panic discontinuation → bipolar or psychotic relapse, suicide risk, obstetric harm.[2][3]
- Valproate inertia → preventable MCM and cognitive harm.[9][11]
- Relative-risk scaremongering without baseline MCM framing.[4][7]
- Ignoring GDM on olanzapine/quetiapine-class agents.[14][15]
- Forbidding breastfeeding by class label without RID thinking.[22]
- Missing postpartum peak after a “perfectly medicated” pregnancy.[21]
Prognosis and disposition
Prognosis tracks illness severity, adherence, sleep, substances, and social support more than any single tablet. Disposition ranges from community perinatal teams to mother–baby units for complex risk. Safety-net with written plans, crisis contacts, and early postpartum review dates.[19][20][21]
Special populations
Adolescent pregnancy needs guardian/capacity frameworks and simpler regimens. Premature neonates change lactation risk calculus. Intellectual disability requires supported decision-making. Substance use comorbidity alters risk–benefit (e.g. sedative stacking). Cultural and interpreter access is part of valid consent, not optional etiquette.[19][22]
Evidence, guidelines and regional differences
- Foundational depression-in-pregnancy risk–benefit frame
- Still cited for process of shared decision
- Pair with newer ACOG CPG 5 for updates
- Broader mental health conditions pregnancy/postpartum
- Treatment access and management emphasis
- US obstetric anchor
- Mood, anxiety and related perinatal disorders
- Contemporary stepped pharmacologic advice
- Useful global exam comparator
Anchor counselling in shared decision, perinatal psychiatry pathways, and local medicines information (e.g. obstetric medicines advice services). Valproate avoidance in pregnancy-potential bipolar care is standard consultant practice; document contraception and specialist oversight if any exceptional scenario arises. Coordinate mother–baby units and child-protection interfaces using local statutes — state principles of capacity and least restrictive care, without inventing foreign section numbers.[19][20][22]
Landmark evidence spine for viva flashcards: Grote untreated depression birth outcomes; Viguera bipolar recurrence after stabiliser stop; Huybrechts SSRI cardiac (adjusted); Grigoriadis PNAS and PPHN; Patorno lithium cardiac; Fornaro lithium SR/MA; EURAP/Battino ASM MCM; Meador NEAD valproate cognition; Huybrechts 2023 antipsychotics malformations; Park/Heinonen antipsychotic GDM; Bergink postpartum psychosis; CANMAT 2024 and ACOG CPG 5 guideline frames.[1][2][4][5][6][7][8][10][11][13][14][20][21]
Exam pearls
- Baseline MCM ~2–3% — always say it.[4]
- Valproate is the hierarchy top for avoid.[9][11]
- Lithium: small absolute cardiac risk increase after modern data — shared decision, not superstition.[7]
- SSRI cardiac story is mostly confounding in large adjusted analyses; PNAS is the commoner late-pregnancy issue.[4][5]
- PPHN is rare; keep absolute risk language.[6]
- SGA → think GDM surveillance.[14]
- Lactation: RID + infant maturity + monitoring; sertraline often workable.[22]
- Postpartum is the danger week(s) for bipolar/psychosis — plan before birth.[21]
Self-test: unplanned pregnancy on valproate and lithium history
Stem: 28-year-old with bipolar I, unplanned 6-week pregnancy, currently on valproate 1000 mg and quetiapine 300 mg, last mania 2 years ago. What do you do first? Model points: Stop framing as “stop everything.” Confirm viability/dating with obstetrics; plan switch off valproate urgently with teratogen counselling and anomaly-scan pathway; decide whether lithium (if previously effective) or SGA monotherapy is the safer ongoing stabiliser for her history; do not leave her untreated if high relapse risk; document shared decision; arrange perinatal psychiatry and early anomaly imaging; discuss folic acid and supports; plan postpartum prophylaxis early.[2][9][7][19]
References
- [1]Grote NK, Bridge JA, Gavin AR, et al. A meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction Arch Gen Psychiatry, 2010.PMID 20921117
- [2]Viguera AC, Whitfield T, Baldessarini RJ, et al. Risk of recurrence in women with bipolar disorder during pregnancy: prospective study of mood stabilizer discontinuation Am J Psychiatry, 2007.PMID 18056236
- [3]Viguera AC, Nonacs R, Cohen LS, et al. Risk of recurrence of bipolar disorder in pregnant and nonpregnant women after discontinuing lithium maintenance Am J Psychiatry, 2000.PMID 10671384
- [4]Huybrechts KF, Hernández-Díaz S, Avorn J, et al. Antidepressant use in pregnancy and the risk of cardiac defects N Engl J Med, 2014.PMID 25229932
- [5]Grigoriadis S, VonderPorten EH, Mamisashvili L, et al. The effect of prenatal antidepressant exposure on neonatal adaptation: a systematic review and meta-analysis J Clin Psychiatry, 2013.PMID 23656856
- [6]Grigoriadis S, Vonderporten EH, Mamisashvili L, et al. Prenatal exposure to antidepressants and persistent pulmonary hypertension of the newborn: systematic review and meta-analysis BMJ, 2014.PMID 24429387
- [7]Patorno E, Huybrechts KF, Bateman BT, et al. Lithium Use in Pregnancy and the Risk of Cardiac Malformations N Engl J Med, 2017.PMID 28591541
- [8]Fornaro M, Maritan E, Ferranti R, et al. Lithium Exposure During Pregnancy and the Postpartum Period: A Systematic Review and Meta-Analysis of Safety and Efficacy Outcomes Am J Psychiatry, 2020.PMID 31623458
- [9]Tomson T, Battino D, Bonizzoni E, et al. Dose-dependent risk of malformations with antiepileptic drugs: an analysis of data from the EURAP epilepsy and pregnancy registry Lancet Neurol, 2011.PMID 21652013
- [10]Battino D, Tomson T, Bonizzoni E, et al. Risk of Major Congenital Malformations and Exposure to Antiseizure Medication Monotherapy JAMA Neurol, 2024.PMID 38497990
- [11]Meador KJ, Baker GA, Browning N, et al. Cognitive function at 3 years of age after fetal exposure to antiepileptic drugs N Engl J Med, 2009.PMID 19369666
- [12]Meador KJ, Baker GA, Browning N, et al. Fetal antiepileptic drug exposure and cognitive outcomes at age 6 years (NEAD study): a prospective observational study Lancet Neurol, 2013.PMID 23352199
- [13]Huybrechts KF, Straub L, Karlsson P, et al. Association of In Utero Antipsychotic Medication Exposure With Risk of Congenital Malformations in Nordic Countries and the US JAMA Psychiatry, 2023.PMID 36477338
- [14]Park Y, Hernandez-Diaz S, Bateman BT, et al. Continuation of Atypical Antipsychotic Medication During Early Pregnancy and the Risk of Gestational Diabetes Am J Psychiatry, 2018.PMID 29730938
- [15]Heinonen E, Forsberg L, Nörby U, et al. Antipsychotic Use During Pregnancy and Risk for Gestational Diabetes: A National Register-Based Cohort Study in Sweden CNS Drugs, 2022.PMID 35220525
- [16]Grigoriadis S, Graves L, Peer M, et al. Benzodiazepine Use During Pregnancy Alone or in Combination With an Antidepressant and Congenital Malformations: Systematic Review and Meta-Analysis J Clin Psychiatry, 2019.PMID 31294935
- [17]Grigoriadis S, Graves L, Peer M, et al. Pregnancy and Delivery Outcomes Following Benzodiazepine Exposure: A Systematic Review and Meta-analysis Can J Psychiatry, 2020.PMID 32148076
- [18]Yonkers KA, Wisner KL, Stewart DE, et al. The management of depression during pregnancy: a report from the American Psychiatric Association and the American College of Obstetricians and Gynecologists Gen Hosp Psychiatry, 2009.PMID 19703633
- [19]ACOG Treatment and Management of Mental Health Conditions During Pregnancy and Postpartum: ACOG Clinical Practice Guideline No. 5 Obstet Gynecol, 2023.PMID 37486661
- [20]Vigod SN, Frey BN, Clark CT, et al. Canadian Network for Mood and Anxiety Treatments 2024 Clinical Practice Guideline for the Management of Perinatal Mood, Anxiety, and Related Disorders Can J Psychiatry, 2025.PMID 39936923
- [21]Bergink V, Rasgon N, Wisner KL Postpartum Psychosis: Madness, Mania, and Melancholia in Motherhood Am J Psychiatry, 2016.PMID 27609245
- [22]Betcher HK, Wisner KL Psychotropic Treatment During Pregnancy: Research Synthesis and Clinical Care Principles J Womens Health (Larchmt), 2020.PMID 31800350