Psych · Psychopharmacology — sedation and driving
Psychotropics, sedation and driving advice
Also known as Fitness to drive psychotropics · Medications and driving psychiatry · Sedation and driving · Benzodiazepines and crash risk · Zopiclone residual impairment
Exam-exhaustive fellowship monograph on psychotropic medications, residual sedation and fitness to drive — illness vs drug effects, BZD and zopiclone hangover evidence, SDLP on-road science, crash epidemiology, counselling algorithms, commercial vs private licences, ADHD stimulant nuance, and regional fitness-to-drive frameworks. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Driving is a complex continuous performance task. Psychiatrists are asked daily whether a patient “can drive on this tablet.” Fellowship answers separate illness impairment, drug residual effects, and context (private vs commercial, alcohol, sleep debt), cite the experimental SDLP literature and epidemiological crash signals, and produce documented counselling rather than vague hope.[1][5][9][14]
Definition and classification
Fitness to drive in mental health means the person can safely control a vehicle given current mental state, cognition, psychomotor capacity, insight into risk, and the kinetic/pharmacodynamic profile of any psychoactive medicines — judged against the licence class and local medical standards (Austroads in ANZ, DVLA in the UK, jurisdiction-specific US rules).[1][13]
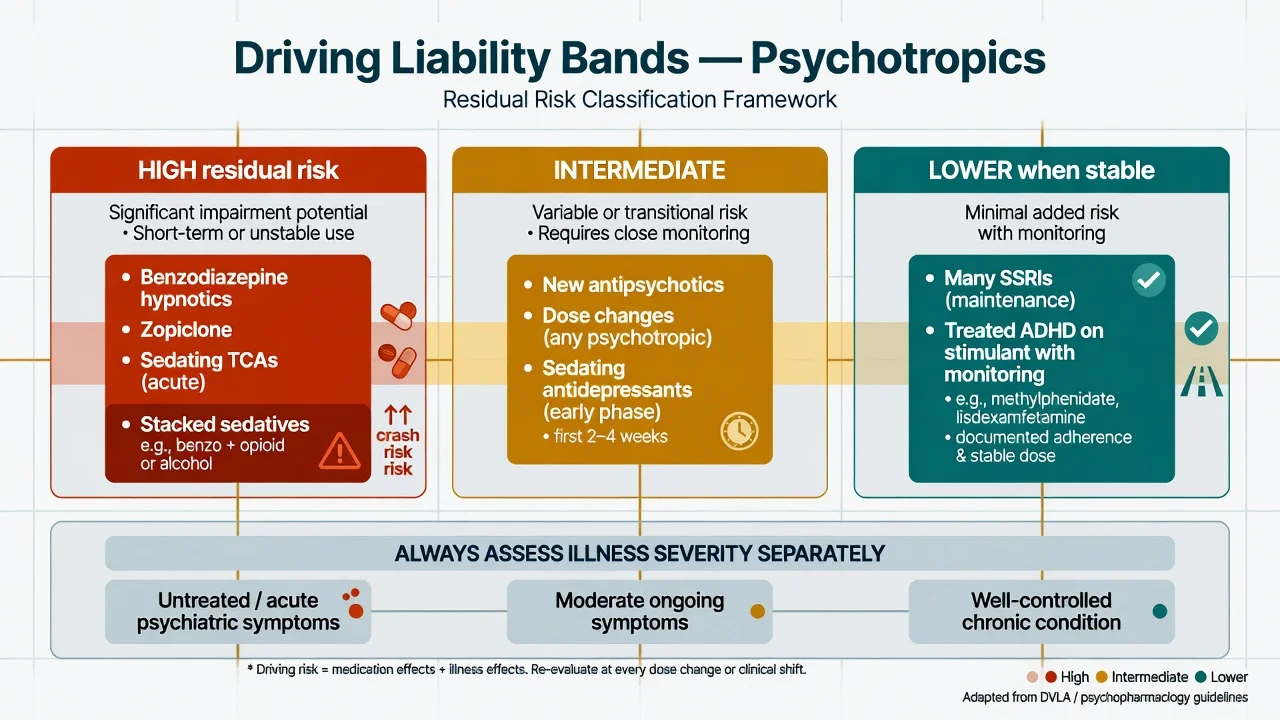
Impairment sources stack — illness, residual sedation, titration windows, substances and motor effects must be assessed separately and then combined.[1][5][9]
| Source | Teaching examples | Drive implication |
|---|---|---|
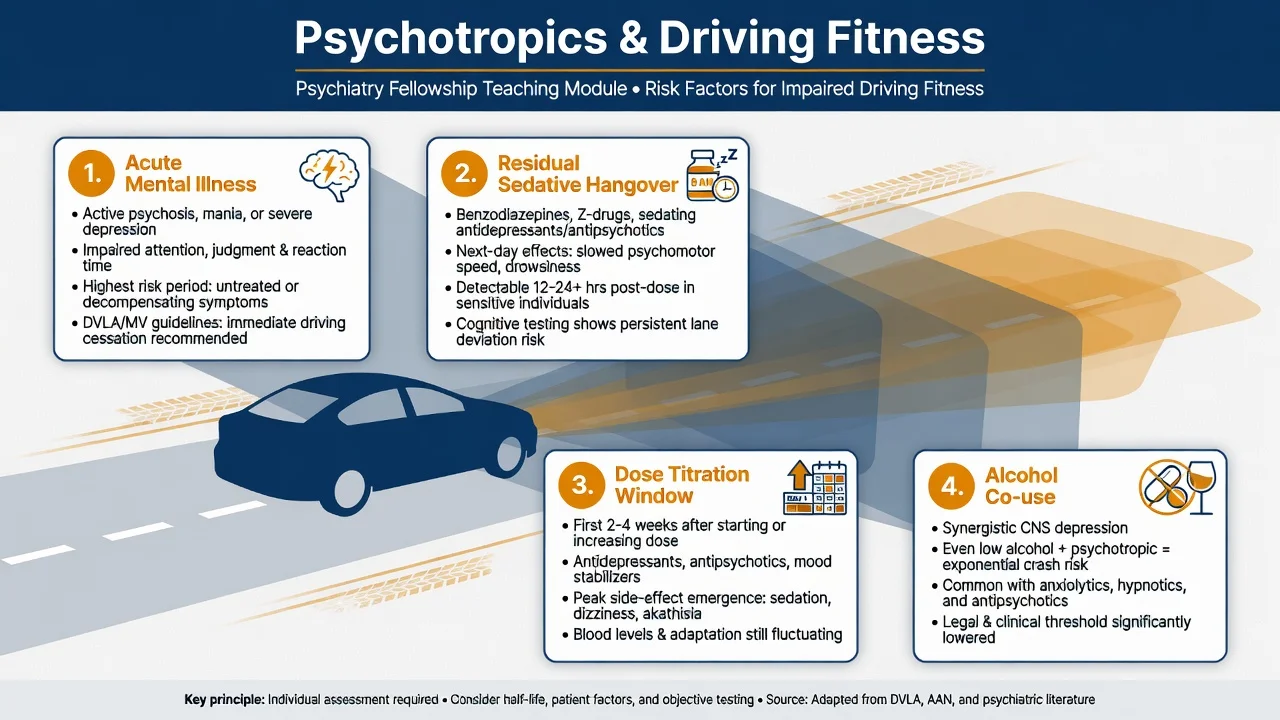
| Acute illness | Mania with grandiosity, psychosis with disorganisation, severe melancholia with slowed cognition, panic storm | Often temporary no-drive until contained |
| Residual sedation | BZD hypnotics, zopiclone next morning, sedating TCAs/mirtazapine early course | Time-limited restriction; hangover literacy |
| Dose change window | New start, rapid titration, PRN stacks | Highest risk days–weeks |
| Substances | Alcohol, cannabis, opioids with psychotropics | Multiplicative risk — absolute counsel |
| Motor/EPS | Parkinsonism, severe akathisia | Functional motor check |
| These rows synthesise experimental and epidemiological teaching; individualise always.[1][5][9][10] |
SDLP (standard deviation of lateral position) is the on-road gold-standard proxy for lane weaving used in experimental psychopharmacology; increases similar to low-level alcohol BAC are treated as clinically meaningful impairment signals in that literature.[1][5][7]
Epidemiology and risk
Thomas’s systematic review of case-control evidence concluded that benzodiazepine use approximately doubles motor vehicle accident risk, with older drivers a high-vulnerability group.[2] Hemmelgarn’s elderly cohort linked long-half-life benzodiazepines to elevated crash risk; short-acting patterns differ and must not be assumed identical.[3] Barbone’s population study associated benzodiazepine exposure with road-traffic accidents, anchoring the epidemiology examiners expect by name.[4]
Hypnotics are not exempt because they are “only for sleep.” Gustavsen linked prescriptions of zopiclone, zolpidem, flunitrazepam and nitrazepam to road traffic accident risk — residual morning impairment is a public-health, not only a pharmacology, problem.[6] Verster’s residual-effects review shows benzodiazepine hypnotics and zopiclone impair on-road driving the morning after bedtime dosing; half-life, dose and hours since dose modulate magnitude.[5]
Dassanayake’s systematic review and meta-analysis synthesises experimental and epidemiological evidence across benzodiazepines, antidepressants and opioids.[9] Rudisill’s broader medication–MVC systematic review and Orriols’s medicinal-drugs traffic-safety review place psychotropics in the wider pharmacoepidemiology of crash risk — several sedating agents repeatedly appear among positive associations.[10][14] Fournier showed concurrent benzodiazepine + antidepressant use in older drivers raises MVA risk, especially with long-acting BZDs — the classic polypharmacy stem.[11]
Pathophysiology
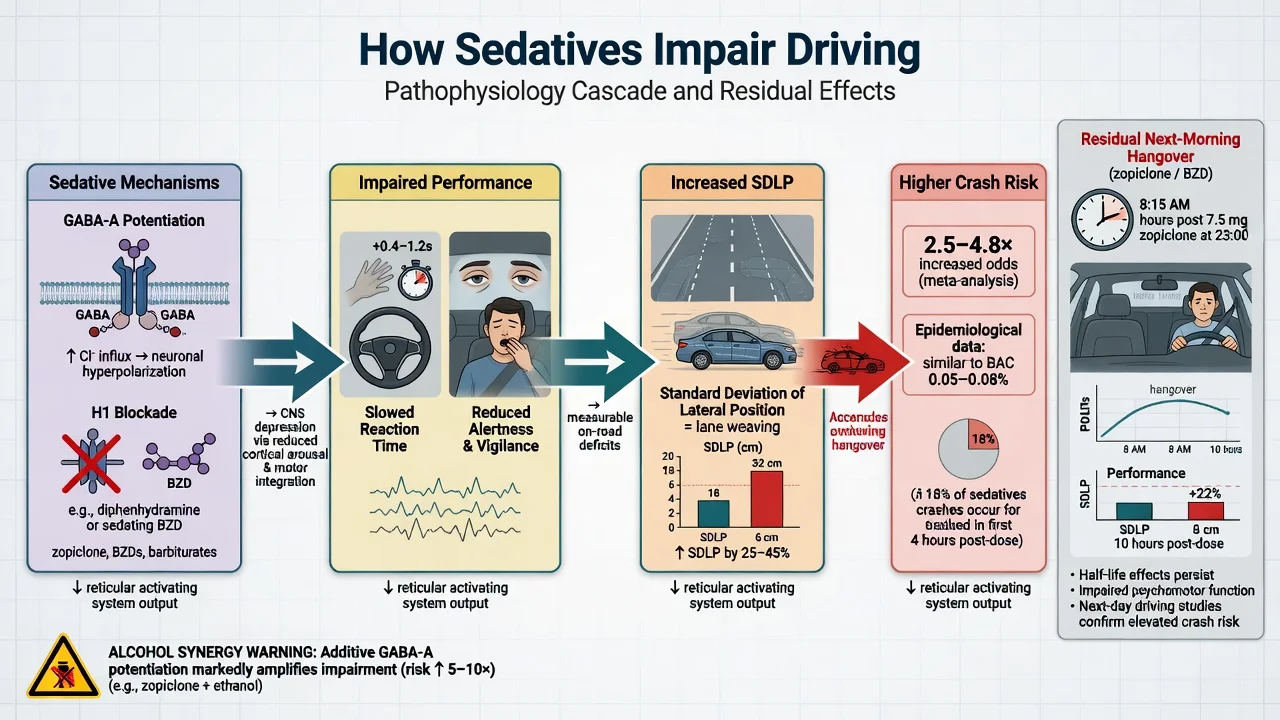
GABA-A potentiation (BZDs, Z-drugs) slows reaction time, fragments divided attention and leaves residual receptor occupancy into the commute window when half-life and dose allow.[1][5] H1 antihistamine and muscarinic blockade from sedating TCAs, some antipsychotics and mirtazapine produce daytime sleepiness and psychomotor slowing, especially early in treatment.[1][7] D2 blockade can add bradykinesia and EPS that degrade pedal/steering control.[1][13]
Illness mechanisms matter independently: depression impairs attention and decision speed; untreated ADHD produces attention lapses; psychosis undermines reality testing and judgment. Wingen found depressed patients on long-term SSRI/SNRI still showed on-road impairment versus controls — residual illness is a plausible contributor when the drug class itself is relatively non-sedating.[8] Conversely, Verster and Roth showed methylphenidate can reduce attention lapses during highway driving in ADHD — treating the disorder may improve fitness.[12]
Alcohol shares CNS-depressant pathways with sedatives; co-use is the multiplicative failure mode every counselling script must name.[1][9][10]
Clinical presentation and differential
Patients may report morning hangover, lane drift, delayed braking, near-misses, or “not feeling right” after a new night sedative. On MSE look for reduced alertness, slowed processing, ataxia, EPS, and impaired insight into risk. Mania may present as overconfidence in driving skill despite clear danger.[1][5][13]
Differential of “can’t drive safely”: medication residual effect vs primary insomnia/OSA sleepiness vs depression/ADHD attention failure vs substance intoxication vs neurological disease (seizure, dementia, parkinsonism). Do not collapse all of these into “stop the antidepressant forever.”[1][8][13]
Clinical and bedside assessment
Ask: licence class (private vs commercial/heavy), occupational driving, weekly kilometres, crashes/near-misses, time of last dose vs planned drive, alcohol/cannabis/OTC antihistamines, sleep duration, and suicidal ideation involving vehicles.[1][13] Reconcile the full sedative load (prescribed + OTC + alcohol). Assess judgment and insight; obtain collateral when available. There is no single blood test of fitness — clinical judgment plus guideline frameworks rule.[1][14]
Investigations
Targeted only: electrolytes if confusion/hyponatraemia possible on antidepressants; toxicology if acute intoxication suspected; sleep assessment if OSA likely; specialist occupational driving assessment for commercial licences or contested fitness. Experimental SDLP testing is research methodology, not a clinic tool.[1][8][13]
Management — resuscitation / emergencies
Severe oversedation is a medical emergency pathway (ABC, supportive care); outpatient flumazenil improvisation is not fellowship-standard care for routine BZD exposure.[1]
Management — definitive counselling and prescribing
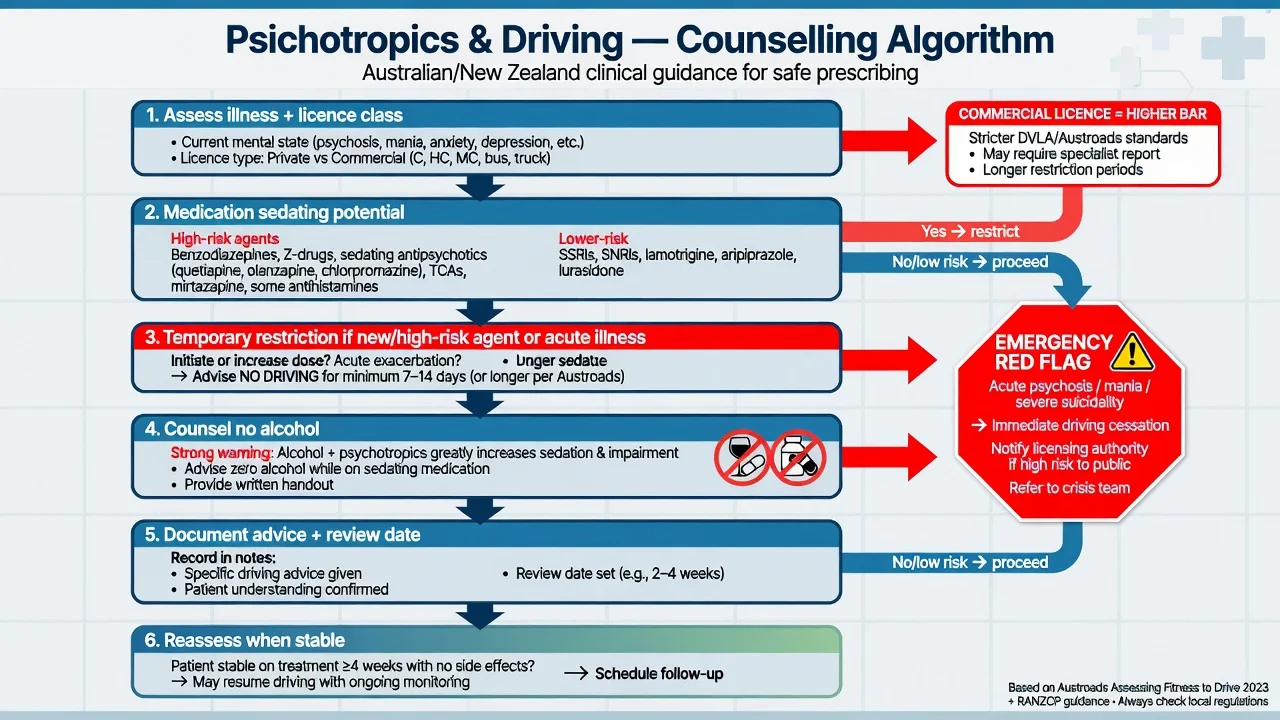
- Treat the psychiatric indication — untreated severe illness is itself a crash risk.[8][13]
- Prefer lower-sedation options when efficacy is comparable (e.g. non-sedating antidepressant strategy vs heavy TCA load for a commuting patient).[7][13]
- Warn at first prescription of any sedating psychotropic: do not drive until individual response is known; avoid alcohol; watch for next-day hangover after hypnotics.[1][5]
- Temporary restriction windows — commonly the first days after starting or increasing BZDs, Z-drugs, sedating antidepressants/antipsychotics, or during acute decompensation; reassess rather than ban indefinitely.[1][9][13]
- Hypnotic literacy — bedtime benzodiazepines and zopiclone impair morning on-road performance; zopiclone is used as a positive control for residual impairment in experimental designs precisely because effects are reliable.[5][6] If a hypnotic is used, choose the lowest effective dose for the shortest period, ensure an adequate sleep-to-commute interval, and prefer non-drug insomnia care first.
- Antidepressants — sedating TCAs and acute mirtazapine need early caution; many SSRIs show less residual on-road impairment in experimental work, but patient samples can still underperform controls when depression persists.[7][8][13]
- Antipsychotics — stabilise psychosis first; reassess fitness as acute phase settles; counsel sedation and EPS.[1][13]
- ADHD — methylphenidate reduced highway attention lapses in on-road work; treat ADHD rather than assuming stimulants automatically unfit a private driver.[12]
- Document the advice, the patient’s understanding, any temporary restriction, and the review date — medico-legal spine of the encounter.[1][13]
Illustrative counselling anchors (not product-label substitutes)
| Scenario | Teaching action | Monitoring / review |
|---|---|---|
| New oral BZD anxiolytic (e.g. lorazepam 0.5–1 mg PRN teaching band) | Advise no driving until effects known; avoid alcohol; prefer non-drive days when PRN used | Sedation, falls, dependence risk; early clinical review |
| Night zopiclone 7.5 mg oral | Explicit residual morning impairment warning; avoid early commute until individual residual known; shortest course | Next-day alertness, near-misses; deprescribe promptly |
| Mirtazapine 15–30 mg oral nocte early weeks | Morning hangover caution; consider dose timing and commute | Weight, sedation trajectory over 2–4 weeks |
| Stable SSRI, remitted depression, no sedation | Usually fit for private driving if illness controlled and no other red flags | Recheck after any new sedative or relapse |
| Adult ADHD on methylphenidate (individualised oral regimen) | May improve attention lapses; still counsel misuse, sleep, and commercial-licence rules | BP, appetite, symptom control, driving near-miss history |
| Dose and timing examples are teaching scaffolds from common practice bands and experimental protocols (e.g. zopiclone 7.5 mg residual studies); verify current product information and local protocols.[5][6][7][12][13] |
High residual risk
- BZD hypnotics & zopiclone hangover
- Sedating TCA early course
- Sedative stacks + alcohol
- Acute mania/psychosis
Reassess window
- New start or dose increase
- PRN BZD days
- Inpatient discharge planning
- Older adult polypharmacy
Often fit when stable
- Remitted illness, non-sedating AD
- Stable AP without sedation/EPS
- Treated ADHD (individualise)
- Documented review passed
Specific subtypes and scenarios
- Panic disorder, new lorazepam PRN: counsel no drive on days of use until response known; prioritise SSRI/CBT longer-term so PRN BZD is not chronic.[1][9]
- Insomnia, zopiclone 7.5 mg nocte, early shift work: residual impairment risk is high — non-drug sleep care first; if used, protect the commute window.[5][6]
- MDD 6 months on sertraline, well, no sedation: private driving usually appropriate; illness recovery supports fitness more than fear of the SSRI class alone.[7][8][13]
- First-episode psychosis discharge: illness risk dominates until stable; stepwise return to driving with documented review.[1][13]
- Older adult, long-half-life diazepam + SSRI: Fournier concurrent-risk phenotype — deprescribe BZD, restrict until safe.[3][11]
- Commercial driver on sedating antipsychotic: higher standard; occupational medicine involvement; do not clear lightly.[1][13]
- ADHD adult, untreated vs methylphenidate: on-road data support attention benefit of treatment — individualise, counsel, monitor.[12]
Complications and pitfalls
Permanent bans without reassessment; ignoring zopiclone because it is “not a benzodiazepine”; missing alcohol counselling; failing to document; inventing jurisdiction-specific legal cut-offs from memory; assuming stable non-sedating medication is worse than untreated psychosis; overlooking OTC antihistamines and opioids in the sedative load.[1][5][9][10]
Prognosis and disposition
Most private drivers regain fitness once illness is controlled and sedating loads are minimised. Temporary restrictions of days to weeks are common and reversible. Commercial licences need longer stability and specialist pathways. Disposition: written advice, GP/occupational liaison, planned review after titration or recovery.[1][13]
Special populations
Older adults carry higher BZD crash signals, polypharmacy and frailty — deprescribe sedatives aggressively.[2][3][11] New young drivers combine inexperience with nightlife alcohol and PRN anxiolytics. Shift workers mis-time residual hypnotic peaks against commute. Intellectual disability needs collateral and supported decision-making. Remote patients may lack transport alternatives — still prioritise safety while problem-solving access.[1][9]
Evidence, guidelines and regional differences
Landmark spine: Verster psychoactive traffic-safety and residual hypnotic reviews; Thomas BZD–MVC systematic review; Hemmelgarn elderly BZD crashes; Barbone population BZD accidents; Gustavsen hypnotic prescription–accident risk; Ramaekers on-road antidepressant impairment; Wingen long-term treated depression driving; Dassanayake meta-analysis; Rudisill and Orriols medication–traffic systematic reviews; Fournier concurrent BZD+AD older drivers; Brunnauer patient-sample driving performance synthesis; Verster/Roth methylphenidate ADHD highway lapses.[1][2][3][4][5][6][7][8][9][10][11][12][13][14]
Use local medical standards as living documents: Austroads Assessing Fitness to Drive (ANZ), UK DVLA psychiatric and drug standards, and US state medical advisory frameworks plus FDA residual-impairment labelling. Principles are shared (illness + drug + licence class + documentation); exact mandatory reporting triggers and commercial thresholds are jurisdictional — state the principle in viva and check the current standard rather than inventing statutes.[1][13]
Exam pearls
DRIVE-SAFE counsel
DRIVESAFE
References
- [1]Verster JC, Mets MA. Psychoactive medication and traffic safety Int J Environ Res Public Health, 2009.PMID 19440432
- [2]Thomas RE. Benzodiazepine use and motor vehicle accidents. Systematic review of reported association Can Fam Physician, 1998.PMID 9585853
- [3]Hemmelgarn B, Suissa S, Huang A, et al. Benzodiazepine use and the risk of motor vehicle crash in the elderly JAMA, 1997.PMID 9207334
- [4]Barbone F, McMahon AD, Davey PG, et al. Association of road-traffic accidents with benzodiazepine use Lancet, 1998.PMID 9802269
- [5]Verster JC, Veldhuijzen DS, Volkerts ER. Residual effects of sleep medication on driving ability Sleep Med Rev, 2004.PMID 15233958
- [6]Gustavsen I, Bramness JG, Skurtveit S, et al. Road traffic accident risk related to prescriptions of the hypnotics zopiclone, zolpidem, flunitrazepam and nitrazepam Sleep Med, 2008.PMID 18226959
- [7]Ramaekers JG. Antidepressants and driver impairment: empirical evidence from a standard on-the-road test Hum Psychopharmacol, 2003.PMID 12590619
- [8]Wingen M, Ramaekers JG, Schmitt JA. Driving impairment in depressed patients receiving long-term antidepressant treatment Psychopharmacology (Berl), 2006.PMID 16865389
- [9]Dassanayake T, Michie P, Carter G, et al. Effects of benzodiazepines, antidepressants and opioids on driving: a systematic review and meta-analysis of epidemiological and experimental evidence Drug Saf, 2011.PMID 21247221
- [10]Rudisill TM, Zhu M, Kelley GA, et al. Medication use and the risk of motor vehicle collisions among licensed drivers: A systematic review Accid Anal Prev, 2016.PMID 27569655
- [11]Fournier JP, Wilchesky M, Patenaude V, et al. Concurrent Use of Benzodiazepines and Antidepressants and the Risk of Motor Vehicle Accident in Older Drivers: A Nested Case-Control Study CNS Drugs, 2015.PMID 26847674
- [12]Verster JC, Roth T. Methylphenidate significantly reduces lapses of attention during on-road highway driving in patients with ADHD J Psychopharmacol, 2014.PMID 24978156
- [13]Brunnauer A, Herpich F, Zwanzger P, et al. Driving Performance Under Treatment of Most Frequently Prescribed Drugs for Mental Disorders: A Systematic Review of Patient Studies Int J Neuropsychopharmacol, 2021.PMID 34038545
- [14]Orriols L, Salmi LR, Philip P, et al. The impact of medicinal drugs on traffic safety: a systematic review of epidemiological studies Pharmacoepidemiol Drug Saf, 2009.PMID 19418468