Psych · Psychopharmacology — renal and hepatic disease
Psychotropics in renal and hepatic disease
Also known as Psychotropics in CKD · Psychotropics in cirrhosis · Renal dosing psychotropics · Hepatic dosing psychotropics · Dialysis psychopharmacology
Exam-exhaustive fellowship monograph on psychotropic prescribing in renal impairment (including dialysis) and hepatic disease — PK/PD principles, agent selection, lithium–CKD evidence, CAST/ASCEND depression trials, hepatotoxicity, Child–Pugh dosing, benzodiazepine encephalopathy risk, TDM and toxicity pathways. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Organ impairment turns ordinary psychopharmacology into a clearance and free-fraction problem. Fellowship exams reward candidates who can stage the kidney and the liver, name which drugs are renally versus hepatically dependent, integrate modern depression-in-CKD trial evidence, and manage toxicity without abandoning indicated treatment. This topic is a safety monograph for consultation-liaison and general adult practice, not a substitute for product information on every molecule.[1][5][13][15]
Definition and classification
Psychotropic prescribing in renal and hepatic disease means adapting agent choice, dose, interval, monitoring and emergency plans to altered absorption, distribution, metabolism and excretion (ADME) and to heightened CNS sensitivity — not a universal “halve the dose” rule.[1][13]
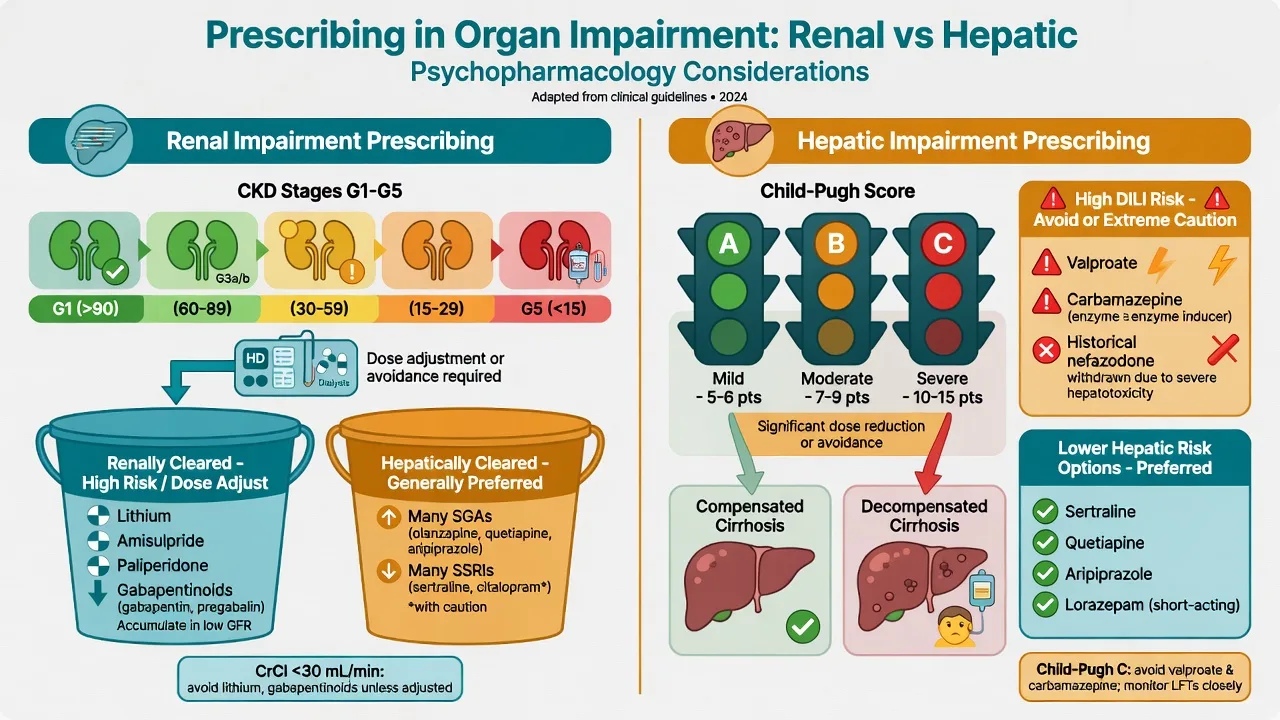
Renal staging for prescribing uses estimated glomerular filtration rate (eGFR) constructs such as CKD-EPI rather than creatinine alone when possible, recognising limitations in extremes of muscle mass and acute kidney injury (AKI).[18] Practically, group patients as mild impairment, moderate–severe CKD (often CrCl or eGFR thresholds in product labels), dialysis-dependent end-stage kidney disease (ESKD), and AKI-on-CKD.[1][18]
Hepatic staging for prescribing uses clinical severity (compensated vs decompensated cirrhosis) and the Child–Pugh construct (bilirubin, albumin, INR/prothrombin time, ascites, encephalopathy) more usefully than an isolated ALT for dosing risk in chronic liver disease.[13][15] Separate pre-existing liver disease from drug-induced liver injury (DILI) after a psychotropic start.[14]
Clearance classes examiners expect
| Class | Teaching examples | Clinical implication |
|---|---|---|
| Largely renally cleared parent | Lithium; amisulpride; paliperidone; gabapentin/pregabalin | Dose reduce or avoid at low CrCl; dialysis may remove small water-soluble ions (lithium) |
| Hepatic metabolism, renal metabolite contribution | Many SGAs and antidepressants | Prefer in advanced CKD when efficacy allows; still monitor free fraction and PD |
| High first-pass / CYP-UGT dependent | Many oral antipsychotics and antidepressants | Reduced clearance and higher free fraction in cirrhosis/hypoalbuminaemia |
| Notable DILI or metabolic liver risk | Valproate, carbamazepine; historical nefazodone/tacrine/pemoline | Avoid or use extreme caution when liver already fragile |
| These rows synthesise class-level PK teaching used in renal and hepatic psychopharmacology reviews — always check current product information for exact CrCl cuts.[1][13][14] |
Epidemiology and risk
Major depressive episode is common in CKD — about one in five patients in a carefully assessed cohort — and overlaps symptomatically with uraemia, anaemia and sleep disruption.[6] Depression in CKD associates with worse quality of life, adherence and medical outcomes, so “do nothing because CAST was negative” is as wrong as “force full-dose SSRI without PK thought.”[5][6]
Psychiatric illness is likewise dense in alcohol-related and other cirrhosis pathways, transplant work-ups and intensive care. The dual failure mode is therapeutic nihilism (stopping all psychotropics) versus toxicity (ignoring clearance, free fraction and GABA sensitivity).[13][15]
Lithium remains the exemplar of organ-aware mood-stabiliser risk–benefit: McKnight’s systematic review profiles NDI, hypothyroidism and related harms; Shine’s laboratory series maps long-term renal/thyroid/parathyroid change; Kessing’s nationwide data put modern CKD rates in context for lithium and anticonvulsants — absolute end-stage risk is not “everyone on lithium ends on dialysis,” but monitoring is non-negotiable.[7][8][9]
Pathophysiology
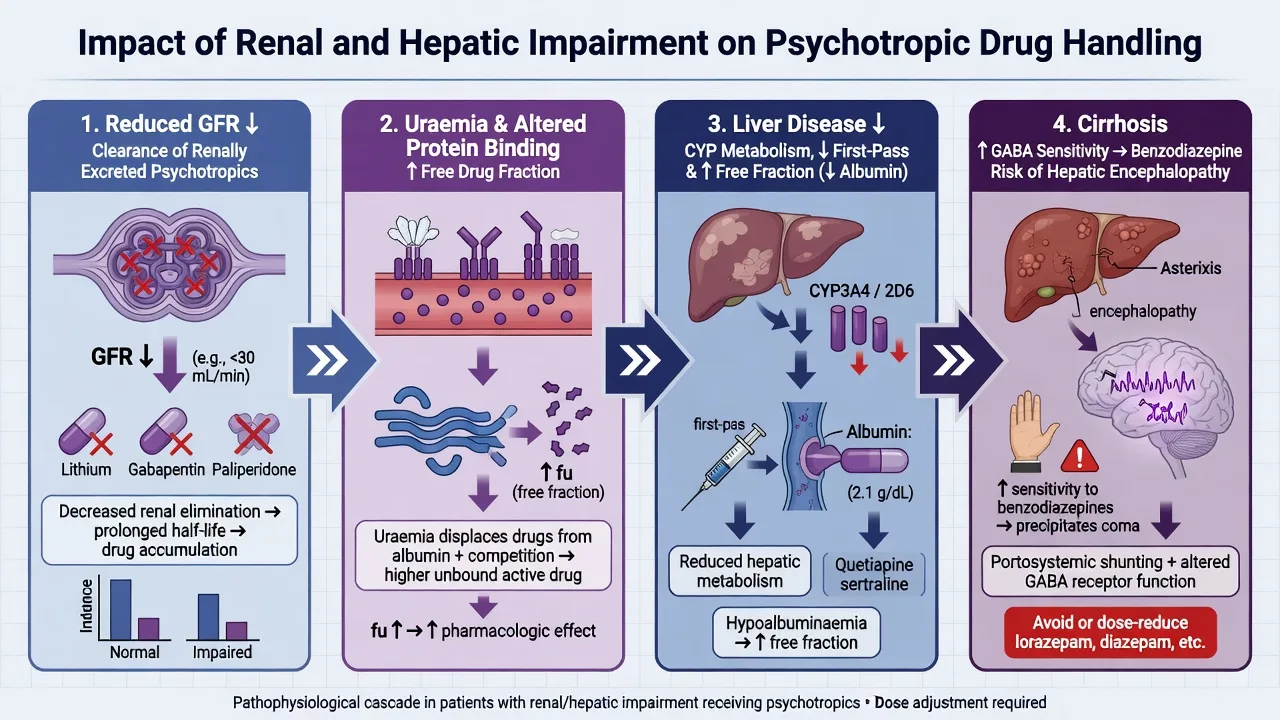
Kidney. Falling GFR reduces elimination of renally excreted parent drugs and active metabolites. Uraemia can alter protein binding and volume of distribution. Small water-soluble ions such as lithium are dialysable — useful in toxicity, disruptive to steady-state levels around dialysis sessions.[1][10][11] Lithium is filtered then reabsorbed in parallel with sodium: volume depletion, NSAIDs, ACE inhibitors/ARBs and thiazides raise levels and drive chronic toxicity.[11]
Liver. Cirrhosis reduces hepatic blood flow, enzyme capacity and first-pass extraction; portosystemic shunting bypasses metabolic machinery; hypoalbuminaemia raises free fraction of highly bound drugs so total plasma levels understate effect.[13][15]
Pharmacodynamics. Uraemic and cirrhotic brains are more sensitive to sedation and delirium. Benzodiazepines interact with GABA pathways already perturbed in hepatic encephalopathy (HE); observational data in cirrhosis with ascites show a clear risk window for first-time HE after new benzodiazepine use.[16]
Valproate hyperammonemic encephalopathy (HAE) can present with reduced consciousness and raised ammonia with relatively modest LFT change — a classic trap if you only “check the ALT.”[17]
Clinical presentation and differential
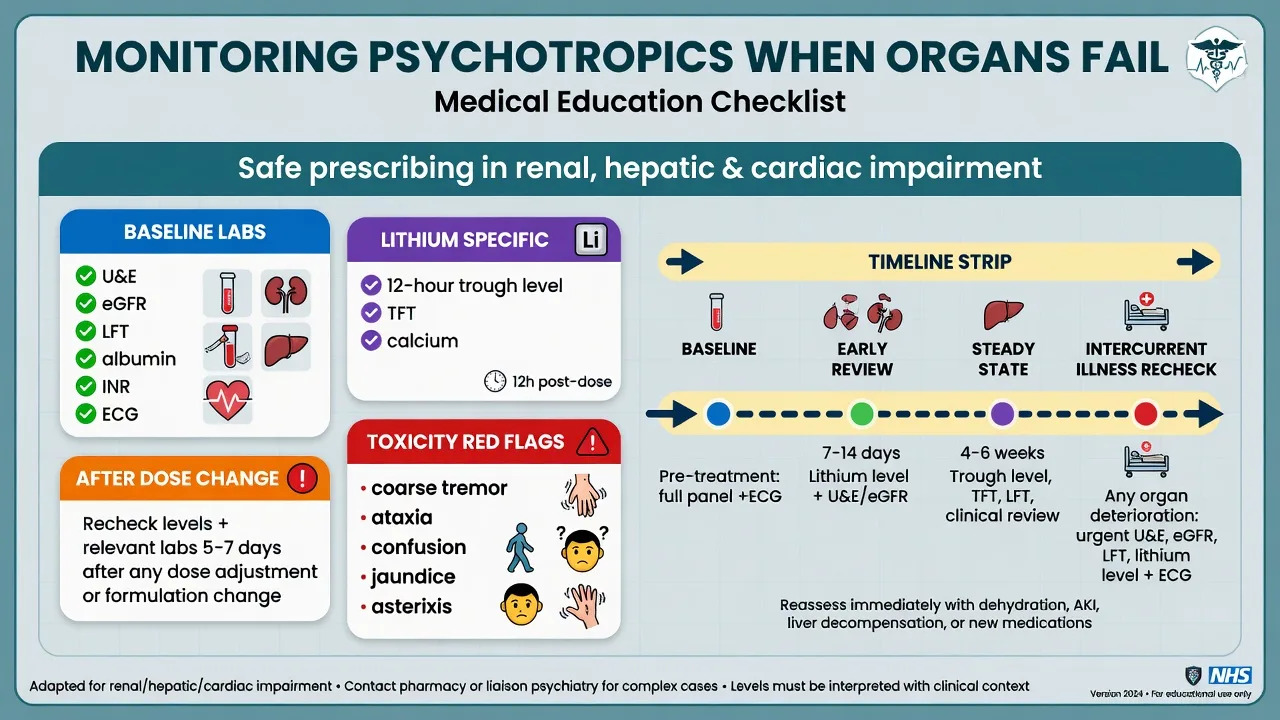
Toxicity phenotypes. Lithium: fine therapeutic tremor → coarse tremor, ataxia, dysarthria, confusion, seizures. Renally cleared antipsychotics: EPS, akathisia, sedation out of proportion to dose. Cirrhosis plus sedatives: asterixis, sleep–wake reversal, HE. DILI: fatigue, jaundice, dark urine, coagulopathy.[11][14][16]
Depression in CKD. Low mood, anhedonia, guilt and suicidal ideation still matter; fatigue and anorexia alone do not diagnose MDD. Structured assessment beats “everyone on dialysis is depressed.”[5][6]
Differential of confusion. In renal failure: uraemia, infection, sodium/calcium, seizure, drug toxicity/withdrawal, primary psychiatric relapse. In cirrhosis: HE, hyponatraemia, sepsis/SBP, intracranial bleed, sedative stack, Wernicke in alcohol use.[15][16] Rising creatinine on lithium is not automatically “lithium nephropathy forever” — dehydation, intercurrent illness and other nephrotoxins come first in the acute work-up.[7][11]
Clinical and bedside assessment
Reconcile every medicine including OTC NSAIDs, herbals and high acetaminophen loads. Examine hydration, orthostatic vital signs, tremor quality, asterixis, jaundice, ascites, and mental state. Estimate GFR with a modern equation (CKD-EPI teaching) and stage liver disease clinically toward Child–Pugh domains.[15][18] Consent must include monitoring burden, sick-day rules for lithium, and who to call if neurotoxicity or HE features appear.[11][12]
Investigations
Baseline before high-stakes psychotropics: U&E/creatinine/eGFR, LFT, albumin, coagulation when cirrhosis is present, FBC, pregnancy test when relevant, ECG if QT-risk agents, TSH and calcium if lithium is planned, and ammonia when valproate encephalopathy is suspected.[11][12][17]
TDM. Lithium requires disciplined 12-hour trough sampling at steady state; AGNP consensus supports concentration-guided care when clearance is unstable or toxicity is suspected for selected other agents (e.g. clozapine, valproate).[12] Around haemodialysis, time levels and doses with nephrology so post-dialysis “lows” and rebound are not misread.[10][11]
Management — resuscitation / emergencies
Sedative-precipitated HE. Hold benzodiazepines and other CNS depressants; treat HE medically; reverse iatrogenic drivers (constipation, infection, electrolytes) with the medical team.[15][16]
Suspected DILI. Stop the culprit psychotropic, urgent LFT/INR, hepatology referral; do not rechallenge high-risk agents casually.[14]
Valproate HAE. Stop valproate, check ammonia and LFTs, supportive care, specialist advice (many protocols consider L-carnitine as an adjunct — follow local toxicology/neurology practice rather than improvising doses from memory).[17]
Management — definitive and stepwise
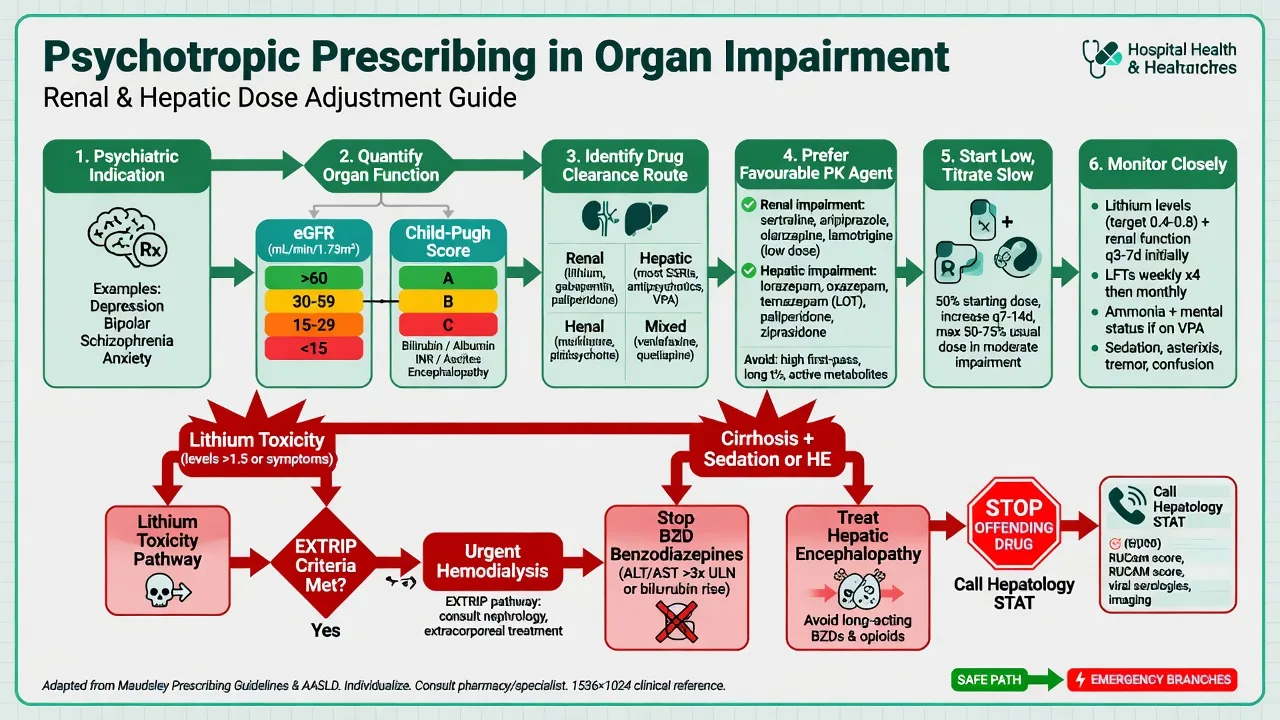
- Confirm the psychiatric indication and non-drug options (psychotherapy access, behavioural support, substance treatment).[5]
- Quantify organs: eGFR/CrCl; Child–Pugh domains; dialysis modality and schedule.[15][18]
- Pick clearance-friendly agents when efficacy is comparable.[1][13]
- Start low, titrate slowly, reassess efficacy and toxicity early.[1][5]
- Use TDM for lithium always; selectively for other AGNP-supported drugs when kinetics are chaotic.[12]
- Document a review date and GP/nephrology/hepatology communication.[5]
Antidepressants in CKD and dialysis
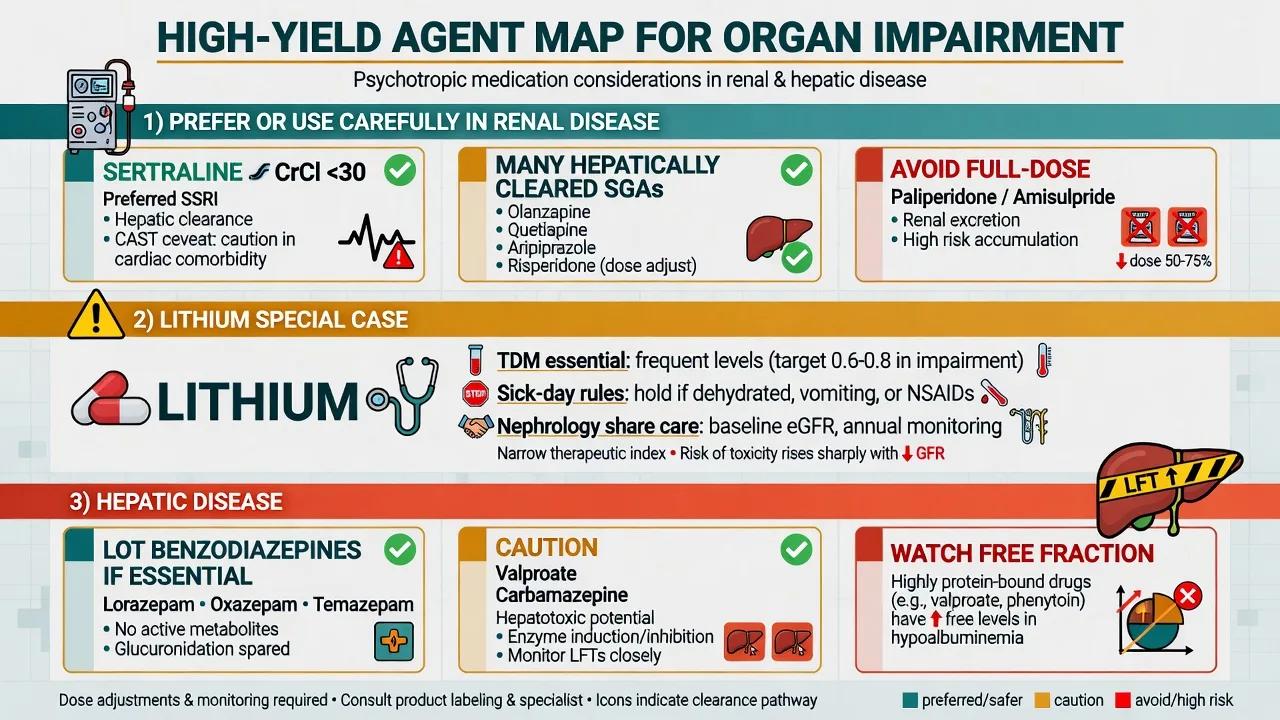
ERBP’s systematic review maps antidepressant pharmacokinetics, sparse efficacy data and safety signals in CKD stages 3–5 — dose adjustment needs are agent-specific, not class-uniform.[2] Sertraline is often chosen for a relatively favourable renal PK profile in practical reviews, but CAST (non-dialysis CKD with MDD) found sertraline not superior to placebo on depressive symptoms over 12 weeks, with more GI adverse effects — use this as shared-decision evidence, not as a ban on treating depression.[3][5] ASCEND compared sertraline with CBT engagement strategies in maintenance haemodialysis depression and is the key dialysis comparative trial name for exams; outcomes require careful reading rather than slogan-level recall.[4] Practical care still combines psychosocial intervention, medical optimisation and, when drugs are used, lower starts with monitoring for hyponatraemia, bleeding risk with antiplatelets, and QT-aware SSRI choices in the elderly CKD phenotype.[2][5]
Antipsychotics
Many second-generation antipsychotics undergo hepatic metabolism and are relatively preferred in advanced CKD when psychosis must be treated, with attention to orthostasis and QT.[1] Paliperidone (renal excretion of active moiety) and amisulpride (largely renal) are classic exam traps: reduce dose or avoid per product CrCl thresholds; do not start full labelled schizophrenia doses in moderate–severe renal impairment.[1] Long-acting injectables demand extra caution when renal function is unstable because you cannot “stop tomorrow.” Prefer oral titration to a stable, tolerated dose first when organs are moving targets.[1]
Lithium and mood stabilisers
If bipolar illness truly benefits from lithium, co-manage with nephrology: lower targets in older adults and impaired clearance, denser levels after any clearance shock, sick-day rules, and ruthless NSAID counselling.[7][11][12] Progressive CKD may force a switch (e.g. toward carefully chosen alternatives), but do not discard lithium’s unique anti-suicide and maintenance profile without a plan.[7][9] Valproate is hepatically handled and carries DILI and HAE risk — poor first choice in active hepatitis or advanced cirrhosis when alternatives exist; carbamazepine shares enzyme-induction and DILI concerns.[13][14][17] Lamotrigine is metabolised hepatically (glucuronidation) — use slow titration literacy and organ-aware caution rather than “free pass” language.[13]
Anxiolytics and hypnotics in liver disease
If a benzodiazepine is unavoidable (e.g. severe alcohol withdrawal under medical protocols), prefer agents with glucuronidation-predominant metabolism in teaching algorithms — lorazepam, oxazepam, temazepam (LOT) — at reduced dose and short course, rather than long-acting diazepam/chlordiazepoxide stacks in decompensated cirrhosis.[13][15][16] Grønbæk’s data support avoiding casual new benzodiazepines in cirrhosis with ascites because of HE risk in early days of exposure.[16]
Illustrative dosing anchors (always verify product labels)
| Scenario | Teaching anchor | Monitoring |
|---|---|---|
| Lithium maintenance with reduced eGFR | Individualise; often lower daily dose; target trough commonly toward lower maintenance bands in older/impaired clearance (e.g. principles around 0.4–0.8 mmol/L range depending on age and indication — local protocol) | 12-h trough, eGFR, TFT, calcium; recheck after illness or new ACEI/NSAID/thiazide |
| Sertraline for MDD in CKD | Start low (e.g. oral sertraline 25–50 mg daily) and titrate by effect/tolerability; CAST tempers expectations | Mood scales, Na+ in older adults, GI adverse effects |
| Paliperidone oral mild renal impairment | Product-style reduction (e.g. lower start such as 3 mg oral daily with max lower than usual label) | EPS, prolactin, renal panel |
| Lorazepam if essential in cirrhosis | Low intermittent oral/IV doses (e.g. 0.5–1 mg) rather than scheduled high-dose stacks | Sedation, asterixis, respiratory status |
| Dose numbers above are teaching scaffolds grounded in common product-information patterns and organ-impairment reviews; institutional protocols and current labels overrule memory.[1][3][11][12][13] |
Advanced CKD / dialysis
- Avoid/adjust paliperidone & amisulpride
- Lithium only with ironclad TDM plan
- CAST/ASCEND-informed depression care
- Many SGAs OK if hepatically cleared
Decompensated cirrhosis
- Minimise benzodiazepines (HE risk)
- Prefer LOT if BZD essential
- Avoid casual valproate/carbamazepine
- Watch free fraction & sedation
Emergency toxicity
- Lithium → stop, saline, EXTRIP
- HE → stop sedatives, medical Rx
- DILI → stop drug, hepatology
- VPA HAE → stop, ammonia path
Specific subtypes and scenarios
- CKD G4, not on dialysis, new MDD: structured diagnosis; offer psychotherapy access; if medication, start low-dose SSRI such as sertraline with CAST-informed expectations and safety monitoring.[2][3][5]
- Maintenance HD with depression: ASCEND comparative framing; integrate dialysis-unit psychology where available.[4]
- Bipolar I, lithium responder, eGFR drifting down: denser monitoring, interaction purge, nephrology co-decision on continue vs switch.[7][8][9]
- Schizophrenia, CrCl 40 mL/min on paliperidone: switch or formal dose reduction; do not ignore label thresholds.[1]
- Child–Pugh C with anxiety and insomnia: non-drug first; avoid chronic BZD; treat HE drivers.[15][16]
- Mania with acute hepatitis: prefer agents with lower acute DILI hierarchy than valproate when feasible; consider antipsychotics with hepatic literacy.[13][14]
- AKI on lithium + ACEI + NSAID: stop NSAID, hold lithium, rehydrate, serial levels.[11]
Complications and pitfalls
Missing OTC NSAIDs; using creatinine alone in sarcopenia; treating total drug levels as free-effect in hypoalbuminaemia; full-dose renally cleared antipsychotics; interpreting CAST as “never prescribe antidepressants”; stacking sedatives in cirrhosis; failing to name EXTRIP in lithium viva; stopping clozapine or other critical agents solely for mild enzyme rises without a plan.[3][10][13][16]
Prognosis and disposition
Organ-aware prescribing reduces iatrogenic admissions and protects psychiatric recovery. Disposition is shared care: CL psychiatry with nephrology or hepatology, pharmacist review, written sick-day and interaction lists, and realistic lab access plans for remote patients.[5][15] Transplant pathways add adherence, substance use and capacity dimensions without turning every clinic visit into a morality play.[15]
Special populations
Older adults combine reduced GFR, polypharmacy and PD sensitivity — start lower, monitor sodium and falls risk.[5] Pregnancy with organ failure needs perinatal psychiatry cross-cover (see companion perinatal topic). Children carry classic high valproate hepatotoxicity risk bands in young ages — extreme caution.[14] Alcohol use disorder dual-presents withdrawal and cirrhosis: protocolised withdrawal care with HE-aware sedative choice.[15][16] Intellectual disability residential polypharmacy plus CKD is a high-harm setting for unreviewed long-term antipsychotics and anticholinergics.[1]
Evidence, guidelines and regional differences
Landmark spine for exams: Baghdady renal psychotropic translation; Nagler/ERBP antidepressant CKD review; CAST and ASCEND for depression treatment evidence; McKnight/Shine/Kessing/Gitlin/EXTRIP for lithium; Hiemke AGNP TDM; Telles-Correia and Sedky for hepatic psychopharmacology and DILI ranking; Lewis & Stine for cirrhosis prescribing practicality; Grønbæk for BZD–HE; Segura-Bruna for VPA HAE; Levey CKD-EPI for GFR estimation literacy.[1][2][3][4][7][8][9][10][12][13][14][15][16][17][18]
Product information CrCl cut-offs (especially paliperidone and amisulpride) and local dialysis unit protocols govern exact milligrams. RANZCP-informed practice expects physical health monitoring and CL collaboration; NICE/APA depression and bipolar pathways still apply but must be filtered through organ PK. Do not invent jurisdiction-specific legal thresholds in viva — state principles and check labels.[1][5][15]
Exam pearls
ORGAN-SAFE prescribing
ORGANSAFE
References
- [1]Baghdady NT, Banik S, Swartz SA, et al. Psychotropic drugs and renal failure: translating the evidence for clinical practice Adv Ther, 2009.PMID 19444657
- [2]Nagler EV, Webster AC, Vanholder R, et al. Antidepressants for depression in stage 3-5 chronic kidney disease: a systematic review of pharmacokinetics, efficacy and safety with recommendations by European Renal Best Practice (ERBP) Nephrol Dial Transplant, 2012.PMID 22859791
- [3]Hedayati SS, Gregg LP, Carmody T, et al. Effect of Sertraline on Depressive Symptoms in Patients With Chronic Kidney Disease Without Dialysis Dependence: The CAST Randomized Clinical Trial JAMA, 2017.PMID 29101402
- [4]Mehrotra R, Cukor D, Unruh M, et al. Comparative Efficacy of Therapies for Treatment of Depression for Patients Undergoing Maintenance Hemodialysis: A Randomized Clinical Trial Ann Intern Med, 2019.PMID 30802897
- [5]Hedayati SS, Yalamanchili V, Finkelstein FO A practical approach to the treatment of depression in patients with chronic kidney disease and end-stage renal disease Kidney Int, 2012.PMID 22012131
- [6]Hedayati SS, Minhajuddin AT, Toto RD, et al. Prevalence of major depressive episode in CKD Am J Kidney Dis, 2009.PMID 19493599
- [7]McKnight RF, Adida M, Budge K, et al. Lithium toxicity profile: a systematic review and meta-analysis Lancet, 2012.PMID 22265699
- [8]Shine B, McKnight RF, Leaver L, et al. Long-term effects of lithium on renal, thyroid, and parathyroid function: a retrospective analysis of laboratory data Lancet, 2015.PMID 26003379
- [9]Kessing LV, Gerds TA, Feldt-Rasmussen B, et al. Use of Lithium and Anticonvulsants and the Rate of Chronic Kidney Disease: A Nationwide Population-Based Study JAMA Psychiatry, 2015.PMID 26535805
- [10]Decker BS, Goldfarb DS, Dargan PI, et al. Extracorporeal Treatment for Lithium Poisoning: Systematic Review and Recommendations from the EXTRIP Workgroup Clin J Am Soc Nephrol, 2015.PMID 25583292
- [11]Gitlin M Lithium side effects and toxicity: prevalence and management strategies Int J Bipolar Disord, 2016.PMID 27900734
- [12]Hiemke C, Bergemann N, Clement HW, et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017 Pharmacopsychiatry, 2018.PMID 29390205
- [13]Telles-Correia D, Barbosa A, Cortez-Pinto H, et al. Psychotropic drugs and liver disease: A critical review of pharmacokinetics and liver toxicity World J Gastrointest Pharmacol Ther, 2017.PMID 28217372
- [14]Sedky K, Nazir R, Joshi A, et al. Which psychotropic medications induce hepatotoxicity? Gen Hosp Psychiatry, 2012.PMID 22133982
- [15]Lewis JH, Stine JG Review article: prescribing medications in patients with cirrhosis - a practical guide Aliment Pharmacol Ther, 2013.PMID 23638982
- [16]Grønbæk L, Watson H, Vilstrup H, et al. Benzodiazepines and risk for hepatic encephalopathy in patients with cirrhosis and ascites United European Gastroenterol J, 2018.PMID 29774154
- [17]Segura-Bruna N, Rodriguez-Campello A, Puente V, et al. Valproate-induced hyperammonemic encephalopathy Acta Neurol Scand, 2006.PMID 16774619
- [18]Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate Ann Intern Med, 2009.PMID 19414839