Psych · Psychopharmacology — SNRIs and NRIs
SNRIs and norepinephrine reuptake inhibitors
Also known as Venlafaxine · Desvenlafaxine · Duloxetine · Milnacipran · Levomilnacipran · Reboxetine · Atomoxetine · Dual reuptake inhibitors · Selective norepinephrine reuptake inhibitors
Exam-exhaustive fellowship pharmacology of SNRIs and selective NRIs — venlafaxine dose-dependent SERT/NET occupancy, desvenlafaxine, duloxetine depression and pain licences, milnacipran class, reboxetine publication-bias evidence, atomoxetine as ADHD NRI pointer, BP monitoring, discontinuation, hyponatraemia, serotonin toxicity, STAR*D switch and Cipriani ranking humility. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
SNRIs are high-yield second-generation antidepressant monographs across FRANZCP, MRCPsych and ABPN. Examiners want dose-dependent dual action, agent-level starts and ceilings, blood-pressure monitoring, discontinuation (especially venlafaxine), duloxetine pain and hepatic niches, and the reboxetine evidence-integrity story — not a brand list or the claim that every SNRI is automatically “stronger than every SSRI.” This leaf topic deepens the antidepressant hub for dual and noradrenergic reuptake drugs.[3][5][11][19]
Definition and classification
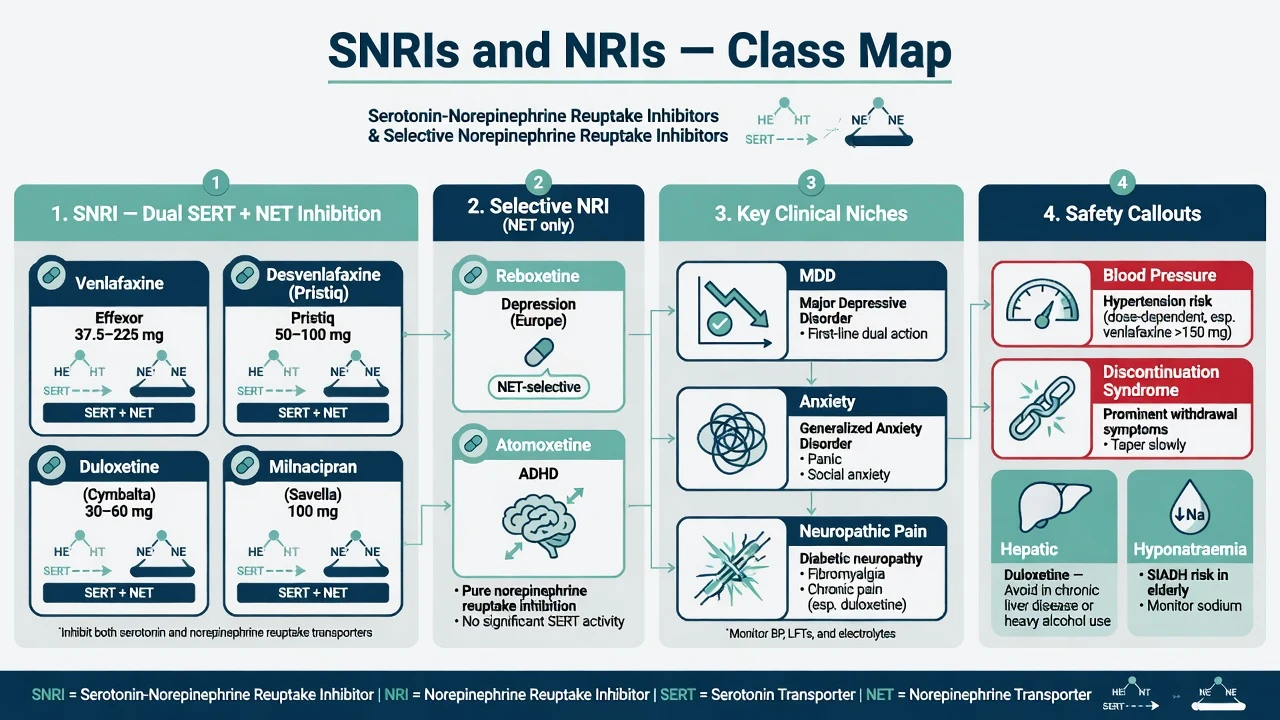
An SNRI (serotonin–norepinephrine reuptake inhibitor) inhibits the serotonin transporter (SERT) and the norepinephrine transporter (NET). A selective NRI inhibits NET with minimal SERT effect at clinical doses — clinically important because reboxetine (depression) and atomoxetine (ADHD) are not interchangeable with venlafaxine or duloxetine in exam answers.[1][11][12]
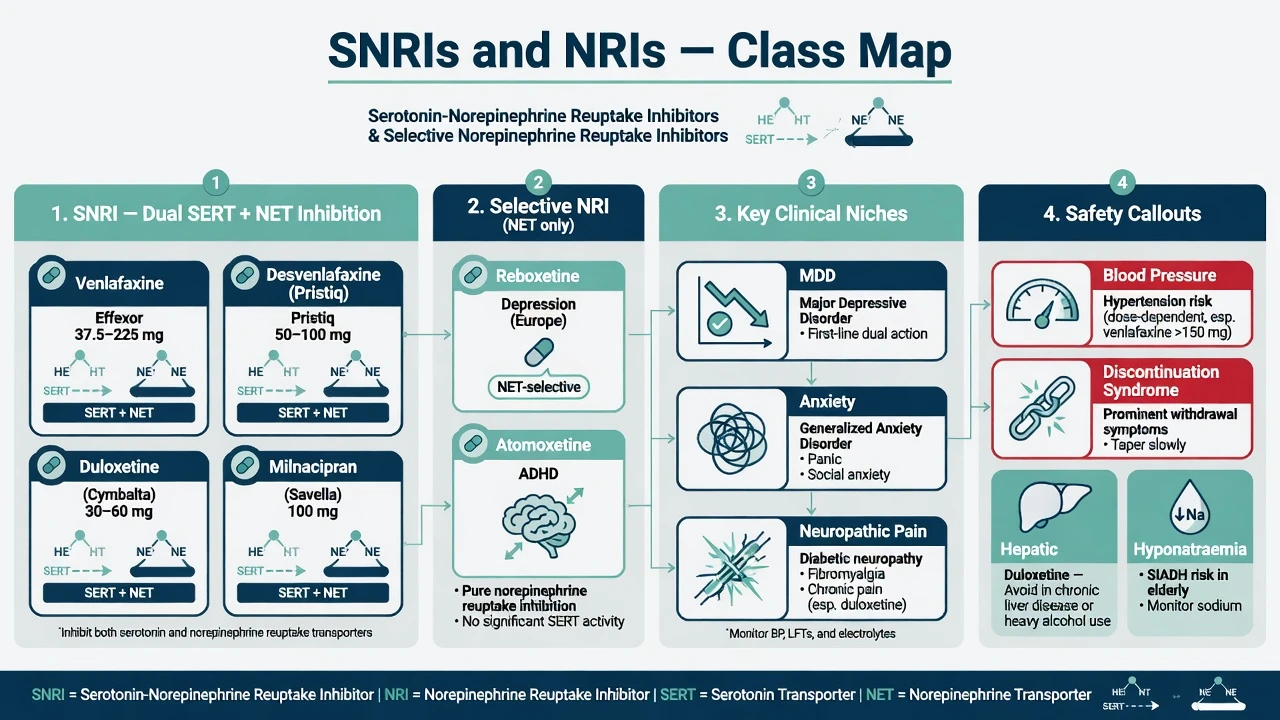
| Group | Core agents | Exam mechanism line | Typical exam niches |
|---|---|---|---|
| SNRI | Venlafaxine (IR/XR), desvenlafaxine | SERT-preferential at lower doses; NET recruited as dose rises | MDD; GAD; switch after SSRI |
| SNRI | Duloxetine | More balanced dual inhibition at usual doses | MDD; GAD; diabetic neuropathy / chronic pain phenotypes |
| SNRI | Milnacipran / levomilnacipran | Dual reuptake; regional availability varies | MDD; milnacipran fibromyalgia in some markets |
| Selective NRI | Reboxetine | NET-selective | Depression — efficacy contested after unpublished-data meta-analysis |
| Selective NRI | Atomoxetine | NET-selective | ADHD (not a first-line unipolar antidepressant) |
| Classification by transporter target beats “dual-action marketing generation” language in viva.[1][5][11][12] |
Mechanisms — the viva core
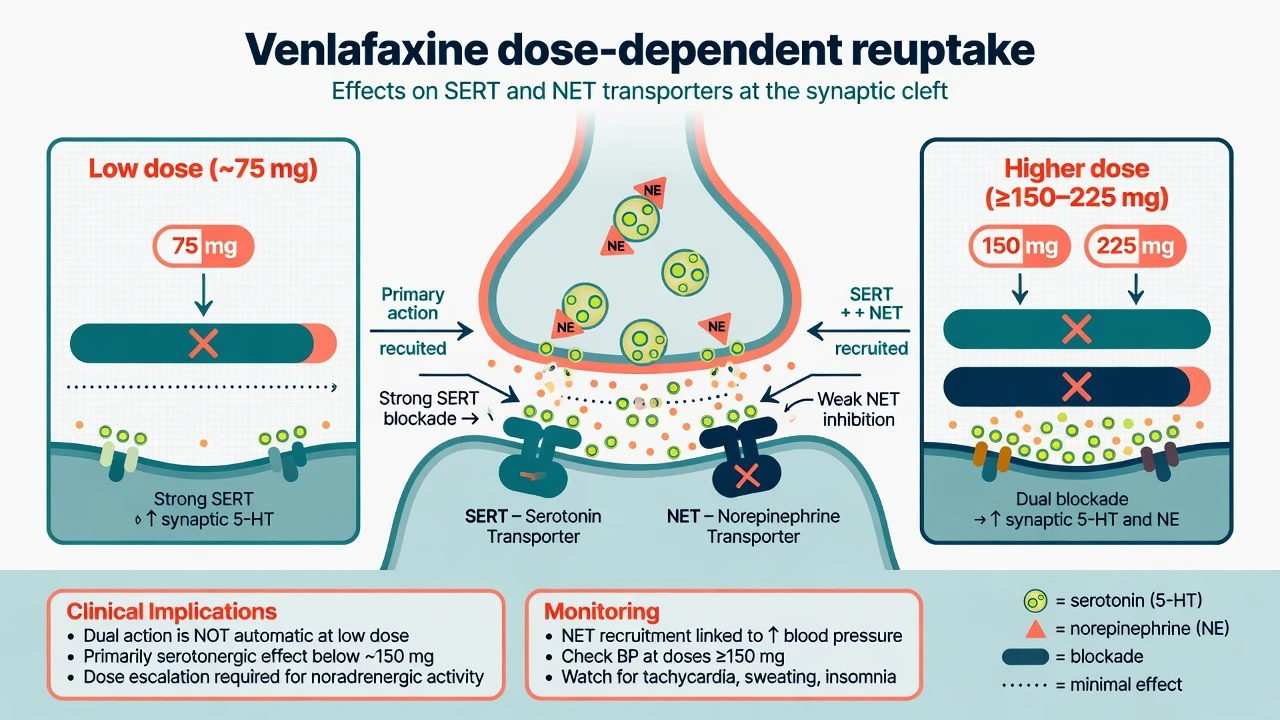
Venlafaxine occupancy teaching point. In healthy-volunteer and clinical physiological studies, lower doses of venlafaxine produce predominantly serotonergic reuptake inhibition, while higher doses recruit noradrenergic reuptake inhibition — Blier and colleagues quantified dose-related effects on SERT and NET function, and Debonnel and colleagues showed differential physiological effects of low versus high doses in major depression.[1][2] Exam translation: starting venlafaxine XR 75 mg is not automatically a “full dual-action” regimen; noradrenergic contribution and BP risk rise as you climb toward 150–225 mg (and specialist higher doses where used).[1][13]
Desvenlafaxine. O-desmethylvenlafaxine is venlafaxine’s major active metabolite; it inhibits both SERT and NET and is typically used at a simpler fixed oral dose (commonly 50 mg daily in outpatients) with placebo-controlled MDD efficacy data at 50 and 100 mg/day ranges.[10]
Duloxetine. Dual SERT/NET inhibition at usual antidepressant doses with RCT support at 60 mg once daily for MDD and broader programme data for painful physical symptoms; pain benefit should not be reduced to “it only works if mood improves” without examining the analgesia literature, but examiners also punish claiming a pure opioid-free panacea.[7][8][9]
Reboxetine. Selective NET inhibition made it the textbook “pure NRI antidepressant.” The 2010 systematic review including unpublished data concluded overall ineffectiveness and potential harm relative to placebo/SSRIs, with published evidence distorted by publication bias — this is an evidence-literacy exam favourite, not an optional history footnote.[11]
Atomoxetine. Selective NET inhibitor with once-daily RCT efficacy in children and adolescents with ADHD; clinical onset is measured in weeks, unlike stimulants. Full ADHD prescribing detail lives in the stimulants topic; here it anchors the NRI class map.[12]
Epidemiology and risk context
SNRIs are widely prescribed for MDD, anxiety disorders and selected pain syndromes. Fellowship risk language focuses on dose-related BP elevation (venlafaxine meta-analysis of thousands of trial patients), discontinuation symptoms with short half-life agents, hyponatraemia (shared SSRI/SNRI association), sexual dysfunction, and rare but catastrophic serotonin toxicity when combined with MAOIs or stacked serotonergics.[13][14][15][16][18]
Evidence anchors examiners expect by name
When to choose an SNRI
RANZCP mood-disorder guidance and CANMAT pharmacological sections place dual-reuptake agents within stepped antidepressant care: first-line options for many adults with moderate–severe MDD include several SSRIs and SNRIs (and other first-line agents) based on prior response, comorbidity, tolerability priorities and local formulary — not a single mandatory brand.[19][20]
Common fellowship selection triggers for SNRI over another first-line class:
- Prior good response to an SNRI or SSRI nonresponse where a cross-class switch is planned (STAR*D switch arm included venlafaxine-XR).[4]
- Comorbid GAD with venlafaxine XR trial evidence in nondepressed outpatients over six months.[6]
- Depressive syndrome with clinically important painful physical symptoms or licensed neuropathic/fibromyalgia indications where duloxetine (or milnacipran where available) is rational.[7][9]
- Need for an agent with different sexual or activation profile after shared decision — still discuss Montejo-level sexual dysfunction risk honestly for serotonergic SNRIs.[16]
Do not choose an SNRI to “force dual action at 37.5 mg,” to treat bipolar I depression as if it were unipolar MDD, or to avoid monitoring. Baseline bipolar screen, suicide risk review and BP remain non-negotiable.[19][13]
Agent-level doses (adult oral exam frameworks)
Ranges are orientation anchors for exams and guidelines teaching. Always check current product information, renal/hepatic labels, and local PBS/authority rules; start lower in older adults and medically frail patients.[19][20]
| Agent | Typical start | Titration / usual range | Killer monitoring notes |
|---|---|---|---|
| Venlafaxine XR | 75 mg orally once daily (some start 37.5 mg if activation/anxiety sensitive) | Increase toward 150–225 mg/day; higher specialist doses used carefully | BP at baseline and after increases; discontinuation risk high if abrupt stop |
| Venlafaxine IR | Divided doses; start low | Same total daily exposure logic | More peak effects; XR preferred for adherence/tolerability in many settings |
| Desvenlafaxine | 50 mg orally once daily | 50 mg often therapeutic; 100 mg studied — little automatic gain for all-comers | BP; nausea; simpler CYP story than parent in teaching talks |
| Duloxetine | 30 mg daily for several days then 60 mg, or start 60 mg if tolerated | 60–120 mg/day usual antidepressant/pain ceiling band | LFT caution; alcohol; pain phenotype documentation |
| Milnacipran / levomilnacipran | Product-specific low start | Labelled MDD (and milnacipran fibromyalgia where licensed) ranges | Availability and brand names vary by region — know the class, not every local trade name |
| Reboxetine | Local product start (often twice-daily historically) | Limited role after evidence reappraisal | Informed consent if still used; Eyding data |
| Atomoxetine (ADHD) | Youth weight-based; adults often 40 mg then 80 mg | Weeks for full trial; max per label (often 100 mg adults) | BP/HR; hepatic warnings; not a stimulant controlled drug |
| Venlafaxine XR placebo-controlled GAD data support long-term outpatient use in nondepressed GAD; duloxetine 60 mg once daily has classic MDD RCT support; desvenlafaxine 50/100 mg outpatient trials support fixed-dose simplicity.[6][7][10][12] |
Landmark evidence every candidate must own
Dose pharmacology. Blier 2007 and Debonnel 2007 are the mechanism pair for “when is venlafaxine dual?” — cite them rather than inventing receptor affinities from memory.[1][2]
Venlafaxine versus SSRIs. Thase’s pooled remission analysis reported higher remission with venlafaxine than SSRIs as a class — historically used to claim SNRI superiority. Cipriani’s 2018 network meta-analysis of 21 antidepressants places efficacy–acceptability differences in a broader, more modest comparative frame: use Thase as history-of-ideas, Cipriani as modern ranking humility, and STAR*D as sequential-care reality.[3][5]
STAR*D Level 2 switch. After citalopram failure, switching to bupropion-SR, sertraline or venlafaxine-XR produced broadly similar remission rates — choose by comorbidity and tolerability, not mythology that venlafaxine is mandatory after every SSRI failure.[4]
Duloxetine programme. Detke and Goldstein RCTs established antidepressant efficacy; Perahia and related analyses address painful symptoms — know both mood and pain exam stems.[7][8][9]
Reboxetine / Eyding. Including unpublished trials overturned the published efficacy narrative — examiners use this to test critical appraisal, not only pharmacology.[11]
Selection algorithm and monitoring
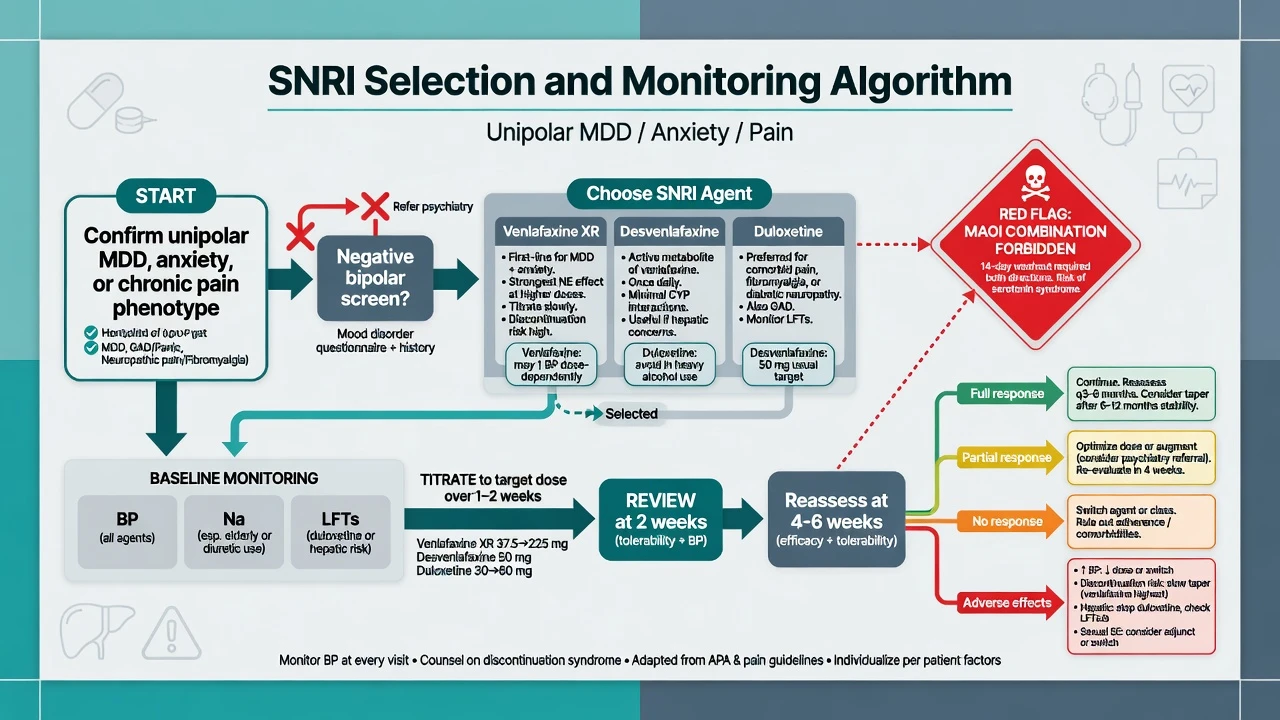
Before first dose (document): unipolar vs bipolar/mixed screen; suicide risk and means; sexual function baseline; concurrent serotonergics (tramadol, triptans, St John’s wort, MAOI history); pregnancy potential; BP and HR; U&E with sodium especially in older adults; LFTs when duloxetine planned or hepatic risk present; alcohol use.[13][15][19][20]
Early follow-up: days to 2 weeks for nausea, activation, akathisia, insomnia and suicidality (especially under 25 and after dose increases); BP after each substantial venlafaxine/desvenlafaxine increase; then efficacy and tolerability at 2–4–6 weeks.[19][14]
Maintenance. Continuation after response reduces relapse risk for antidepressants as a class (Geddes-level teaching lives in the antidepressant hub); plan duration by episode number and residual symptoms, and taper rather than stop cold — especially venlafaxine.[14][19]
RANZCP 2020 mood guidelines frame ANZ practice in formulation-based stepped care with careful antidepressant selection. CANMAT 2016 pharmacological lines (and later updates) are widely used in exams for first-line agent lists that include SNRIs among options. NICE stepped care emphasises review intensity and psychological therapy access. US practice emphasises measurement-based care and product-label ceilings (including venlafaxine and duloxetine pain indications). Formulary and authority rules differ; exam constants are dual-action literacy, BP, taper, and MAOI washouts.[19][20]
Adverse effects and emergencies
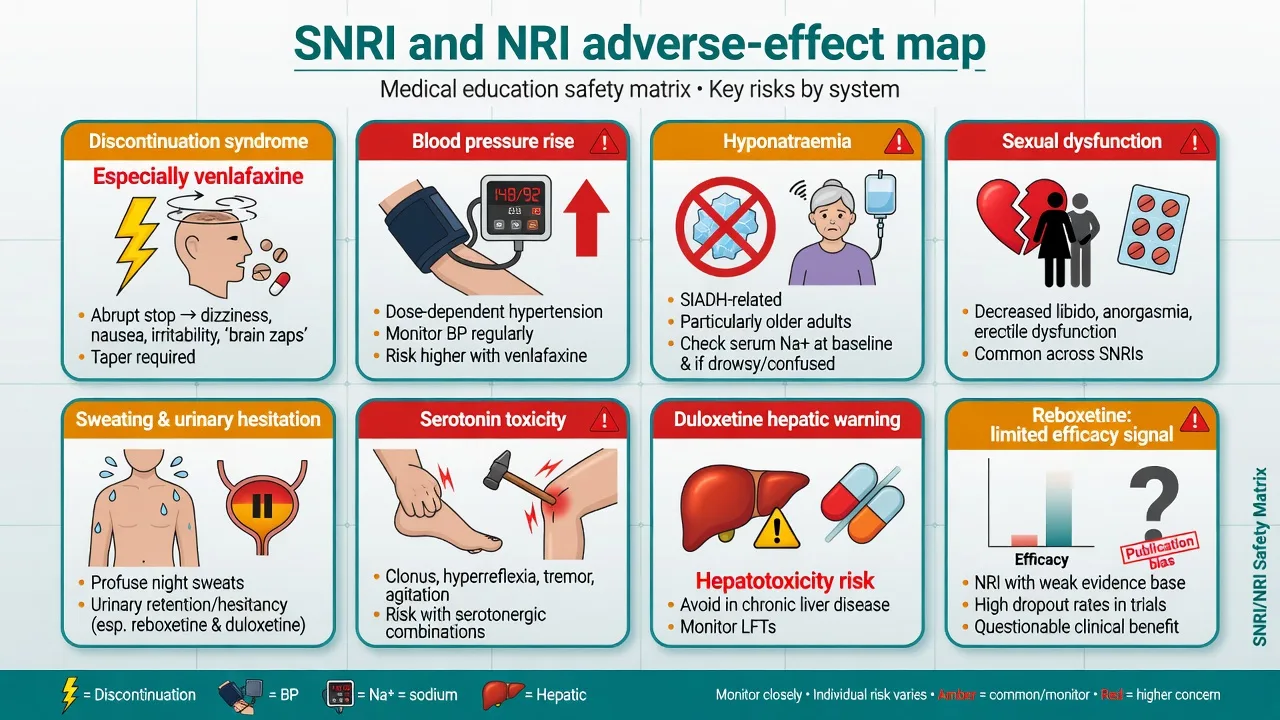
Discontinuation
- Venlafaxine classic short half-life risk with paroxetine
- Dizziness, electric shocks, flu-like, irritability, insomnia
- Taper; reinstate if severe; not framed as addiction
- Counsel before first script
Blood pressure
- Thase meta: venlafaxine BP effects dose-related
- Check baseline and after titration
- Desvenlafaxine and duloxetine also need BP literacy
- Do not escalate into uncontrolled hypertension
Metabolic / electrolyte
- Hyponatraemia association (Movig) — older adults
- Confusion, falls, seizures
- Stop/switch; medical sodium management
Toxicity pathways
- Serotonin toxicity — Hunter criteria
- MAOI + SNRI forbidden
- Duloxetine hepatic injury warnings
- Urinary retention / severe sweating
Blood pressure
Thase’s meta-analysis of original data from 3744 depressed patients is the classic citation for venlafaxine’s blood-pressure effects — clinically, expect dose-related risk of sustained diastolic elevation in a minority and always recheck BP when escalating.[13]
Discontinuation syndrome
Consensus recommendations describe a common, usually time-limited syndrome after abrupt stop or missed doses, worse with short half-life serotonergic agents — venlafaxine is examiners’ favourite SNRI example. Educate at initiation; taper on cessation; distinguish from true depressive relapse that needs separate planning.[14]
Sexual dysfunction and hyponatraemia
Montejo’s prospective multicentre cohort showed high rates of treatment-emergent sexual dysfunction across many antidepressants including dual agents — discuss before prescribing. Movig’s case-control study links antidepressant use with hyponatraemia; SNRI use in older adults demands sodium vigilance like SSRIs.[16][15]
Serotonin toxicity
Clinical diagnosis on the continuum of neuromuscular excitation, autonomic hyperactivity and altered mental status. Apply Hunter Serotonin Toxicity Criteria when a serotonergic agent is present (spontaneous clonus; inducible clonus with agitation or diaphoresis; ocular clonus with agitation or diaphoresis; tremor with hyperreflexia; hypertonia with temperature above 38°C plus ocular or inducible clonus — use the published decision tree precisely).[17][18]
Management: stop serotonergic agents; ABC support; benzodiazepines for agitation; cooling; specialist consideration of cyproheptadine; ICU for severe hyperthermia/rigidity. Never combine irreversible MAOIs with SNRIs; respect washouts (commonly about 2 weeks from most SNRIs to MAOI; longer after fluoxetine if switching the other direction from SSRI pathways).[18][19]
Duloxetine hepatic and other agent-specific issues
Product warnings and clinical teaching emphasise caution or avoidance in substantial hepatic disease and heavy alcohol use; stop for jaundice or significant enzyme rises. Sweating, dry mouth, nausea (early), constipation, and urinary hesitation/retention are noradrenergic-serotonergic mechanism-linked complaints, not mysteries.[7][20]
Switching, augmentation pointers and scenarios
From SSRI to SNRI: cross-taper or direct switch depending on dose, half-life and patient stability; watch for serotonergic overlap symptoms during cross-taper. STAR*D supports venlafaxine-XR as one legitimate switch after SSRI failure, not the only one.[4][14]
Partial response: optimise dose (remember venlafaxine dual-action dose band), confirm adherence, then augment (lithium, atypical antipsychotic, T3) or switch using antidepressant-hub logic — do not stack random serotonergics.[19][20]
Pain-depression overlap: duloxetine 60 mg once daily (titrate as tolerated toward labelled maxima up to 120 mg) is the standard fellowship example; document pain targets separately from mood scores.[7][9]
Anxiety disorders: venlafaxine XR has randomised evidence in GAD without comorbid depression over six months — still use stepped psychological care where indicated.[6]
ADHD NRI path: atomoxetine is the selective NRI for ADHD when stimulants fail, are refused, or diversion risk is high — multi-week trial, BP/HR monitoring (see stimulants topic).[12]
Special populations
Older adults. Start low (e.g. venlafaxine XR 37.5 mg); hyponatraemia and falls; BP; drug interactions; avoid assuming “SNRI is safer than SSRI” for sodium.[15][13]
Youth. Class antidepressant suicidality signal requires close early review; SNRI first-line status is more restricted than in adults in many paediatric pathways — prefer specialist frameworks.[19]
Pregnancy and lactation. Individualised risk–benefit with perinatal psychiatry/obstetrics; untreated depression harms mother and fetus; do not stop abruptly without a plan (discontinuation plus relapse risk).[19]
Hepatic and renal impairment. Duloxetine hepatic caution is high-yield; several SNRIs need renal dose adjustment per label — check product information rather than memorising every eGFR band incorrectly.[20]
Hypertension. Control BP before aggressive venlafaxine titration; choose alternative agents when BP is labile or monitoring will fail.[13]
Prognosis and disposition
Target remission, not mere response; residual symptoms drive relapse. After nonresponse to an optimised SNRI trial, switch or augment using measurement-based care and step up to TRD pathways (including lithium/atypical antipsychotic augmentation or ECT/esketamine interfaces) when severity or risk outstrips outpatient titration speed.[4][5][19]
Evidence, guidelines and controversies
Controversies to handle calmly: how large the true venlafaxine-versus-SSRI remission advantage is; whether higher venlafaxine doses are worth BP and side-effect costs; reboxetine’s residual niche if any; industry influence on dual-action branding. Answer with dose, monitoring and patient values — not slogans.[3][5][11]
Exam pearls
DUAL CHECK before SNRI prescribe
DUALCHECK
References
- [1]Blier P, Saint-André E, Hébert C, et al. Effects of different doses of venlafaxine on serotonin and norepinephrine reuptake in healthy volunteers Int J Neuropsychopharmacol, 2007.PMID 16690005
- [2]Debonnel G, Saint-André E, Hébert C, et al. Differential physiological effects of a low dose and high doses of venlafaxine in major depression Int J Neuropsychopharmacol, 2007.PMID 16690006
- [3]Thase ME, Entsuah AR, Rudolph RL Remission rates during treatment with venlafaxine or selective serotonin reuptake inhibitors Br J Psychiatry, 2001.PMID 11230034
- [4]Rush AJ, Trivedi MH, Wisniewski SR, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression N Engl J Med, 2006.PMID 16554525
- [5]Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis Lancet, 2018.PMID 29477251
- [6]Gelenberg AJ, Lydiard RB, Rudolph RL, et al. Efficacy of venlafaxine extended-release capsules in nondepressed outpatients with generalized anxiety disorder: a 6-month randomized controlled trial JAMA, 2000.PMID 10865302
- [7]Detke MJ, Lu Y, Goldstein DJ, et al. Duloxetine, 60 mg once daily, for major depressive disorder: a randomized double-blind placebo-controlled trial J Clin Psychiatry, 2002.PMID 12000204
- [8]Goldstein DJ, Mallinckrodt C, Lu Y, et al. Duloxetine in the treatment of major depressive disorder: a double-blind clinical trial J Clin Psychiatry, 2002.PMID 11926722
- [9]Perahia DG, Pritchett YL, Desaiah D, et al. Efficacy of duloxetine in painful symptoms: an analgesic or antidepressant effect? Int Clin Psychopharmacol, 2006.PMID 17012978
- [10]Liebowitz MR, Manley AL, Padmanabhan SK, et al. Efficacy, safety, and tolerability of desvenlafaxine 50 mg/day and 100 mg/day in outpatients with major depressive disorder Curr Med Res Opin, 2008.PMID 18507895
- [11]Eyding D, Lelgemann M, Grouven U, et al. Reboxetine for acute treatment of major depression: systematic review and meta-analysis of published and unpublished placebo and selective serotonin reuptake inhibitor controlled trials BMJ, 2010.PMID 20940209
- [12]Michelson D, Allen AJ, Busner J, et al. Once-daily atomoxetine treatment for children and adolescents with attention deficit hyperactivity disorder: a randomized, placebo-controlled study Am J Psychiatry, 2002.PMID 12411225
- [13]Thase ME Effects of venlafaxine on blood pressure: a meta-analysis of original data from 3744 depressed patients J Clin Psychiatry, 1998.PMID 9818630
- [14]Schatzberg AF, Blier P, Delgado PL, et al. Antidepressant discontinuation syndrome: consensus panel recommendations for clinical management and additional research J Clin Psychiatry, 2006.PMID 16683860
- [15]Movig KL, Leufkens HG, Lenderink AW, et al. Association between antidepressant drug use and hyponatraemia: a case-control study Br J Clin Pharmacol, 2002.PMID 11966666
- [16]Montejo AL, Llorca G, Izquierdo JA, et al. Incidence of sexual dysfunction associated with antidepressant agents: a prospective multicenter study of 1022 outpatients J Clin Psychiatry, 2001.PMID 11229449
- [17]Dunkley EJ, Isbister GK, Sibbritt D, et al. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity QJM, 2003.PMID 12925718
- [18]Boyer EW, Shannon M The serotonin syndrome N Engl J Med, 2005.PMID 15784664
- [19]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [20]Kennedy SH, Lam RW, McIntyre RS, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments Can J Psychiatry, 2016.PMID 27486148