Psych · Psychopharmacology — SSRIs
Selective serotonin reuptake inhibitors
Also known as SSRIs · Fluoxetine · Sertraline · Citalopram · Escitalopram · Paroxetine · Fluvoxamine · SSRI discontinuation · Black box antidepressant
Exam-exhaustive fellowship class monograph on selective serotonin reuptake inhibitors — agents, adult doses, pharmacokinetics and CYP differences, licensed indications, black-box early suicide monitoring, sexual dysfunction, hyponatraemia, bleeding, QTc ceilings, serotonin toxicity, discontinuation, switching and MAOI washouts, special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Definition and classification
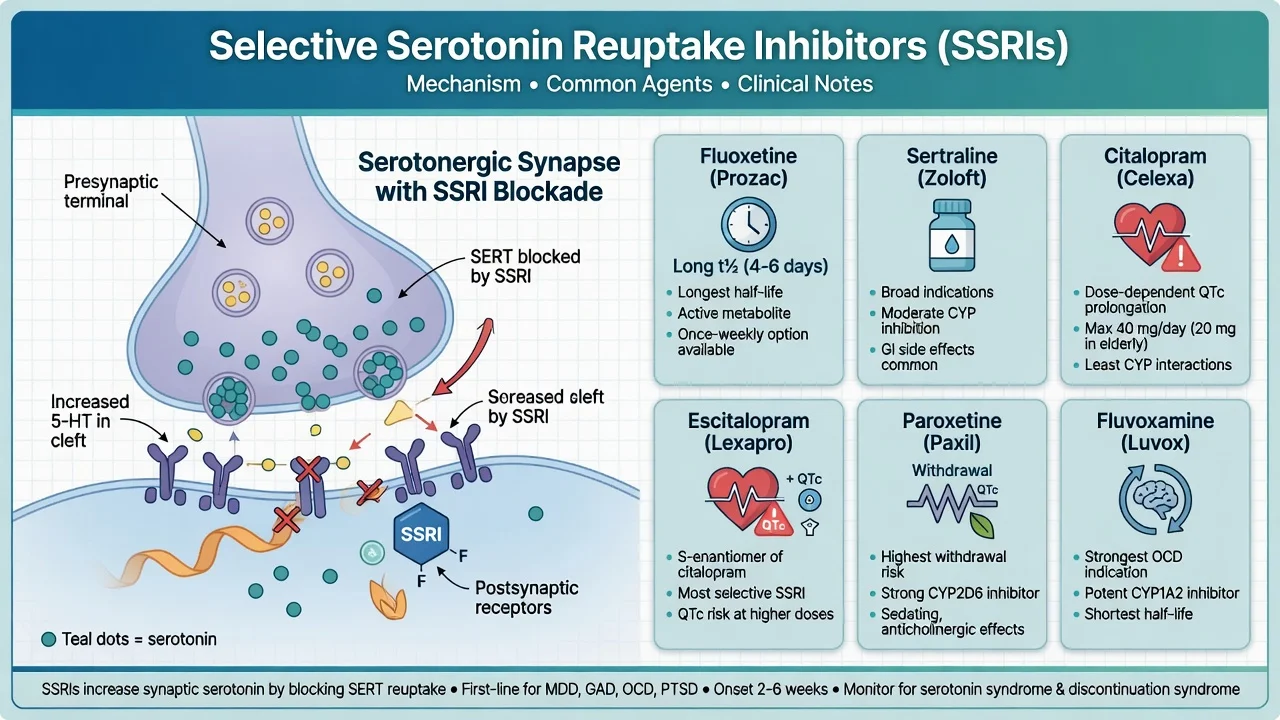
Selective serotonin reuptake inhibitors (SSRIs) are agents whose dominant clinical action is inhibition of the serotonin transporter (SERT), raising synaptic 5-HT with clinically minimal NET/DAT affinity at usual antidepressant doses. They displaced TCAs as first-line outpatient antidepressants because class-level efficacy is comparable while overdose lethality and anticholinergic burden are substantially lower.[1][25]
Core examinable agents: fluoxetine, sertraline, citalopram, escitalopram (S-enantiomer of citalopram), paroxetine, fluvoxamine. Marketing “generation” language is less useful than agent-level half-life, CYP interactions, and toxicity fingerprints.[2][7]
Epidemiology and clinical context
SSRIs are among the most prescribed psychotropics. Absolute suicide risk remains elevated in depressive illness; relative drug-related suicidality signals are age- and time-dependent, strongest in children, adolescents and young adults early after start or dose increase.[9][10] Sexual dysfunction and hyponatraemia are common enough to drive non-adherence and medical harm, not rare textbook footnotes.[11][12] In overdose, SSRIs are far less cardiotoxic than TCAs, though seizures, QTc effects and serotonin toxicity still occur.[25]
Pathophysiology and agent differences
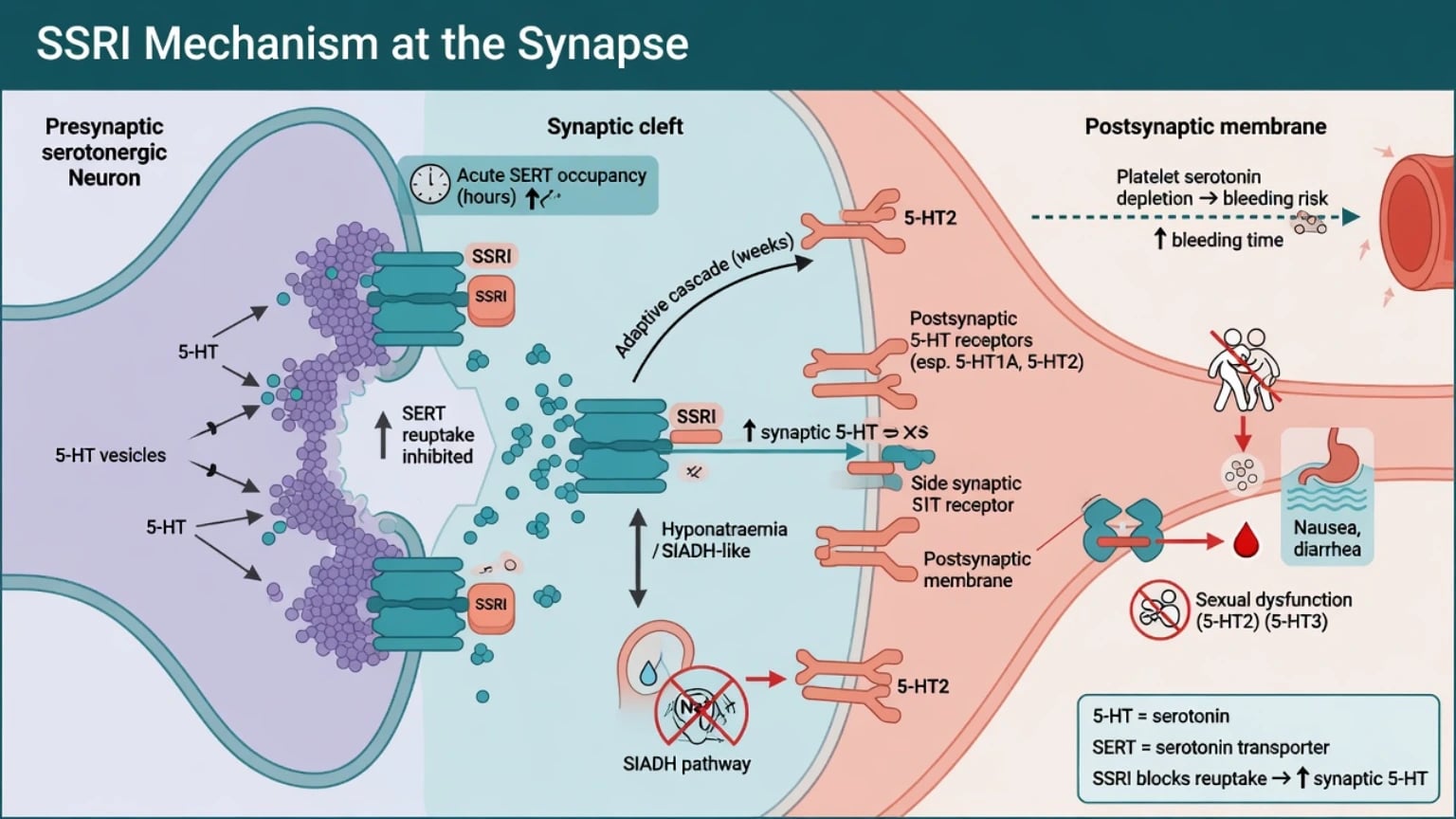
Acute SERT occupancy is rapid; clinical remission is not. Adaptive receptor and network changes over days to weeks track mood and anxiety benefit — do not promise “one tablet, next-day cure.”[1][3]
Side-effect map from serotonergic physiology: GI nausea/diarrhoea (often early); sexual dysfunction (high incidence in prospective data); hyponatraemia / SIADH-like picture especially in older adults; platelet serotonin depletion and upper GI bleeding risk amplified by NSAIDs or anticoagulants; QTc prolongation signal strongest for citalopram/escitalopram among common SSRIs.[11][12][13][14][15]
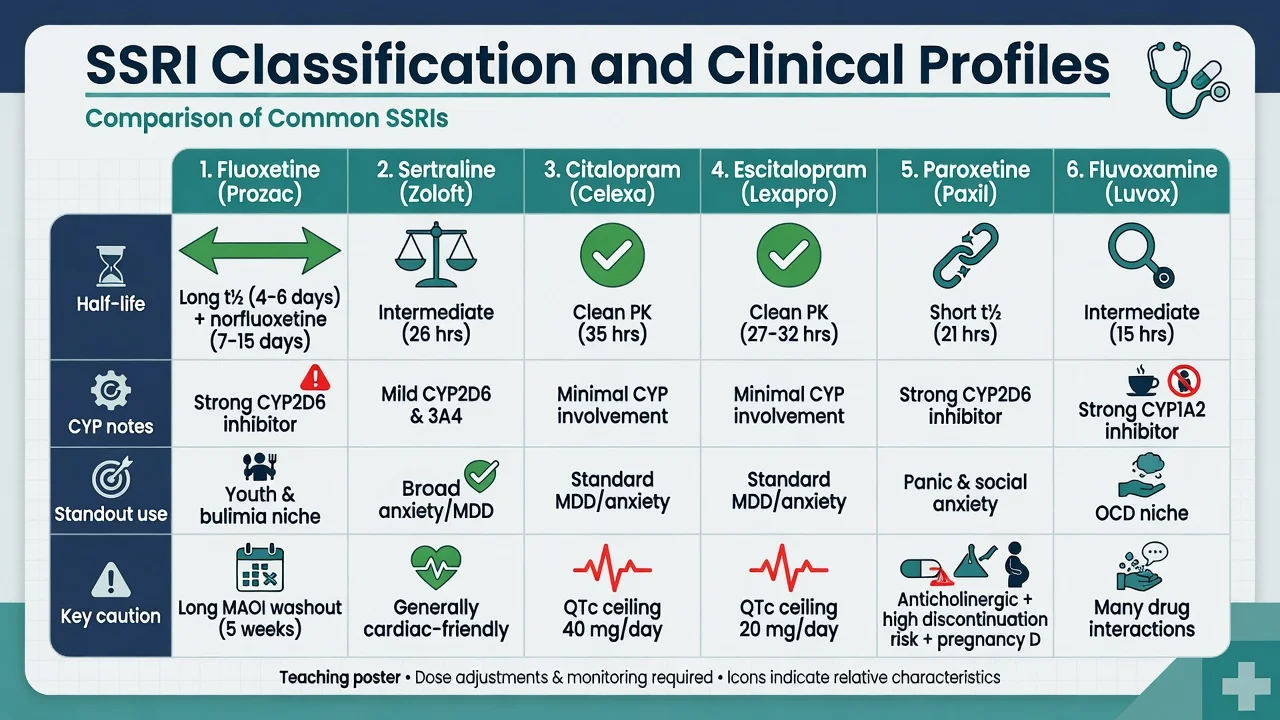
Agent fingerprints examiners reward: fluoxetine (long t½, norfluoxetine, CYP2D6, longest MAOI washout); sertraline (broad MDD/anxiety, often preferred cardiac teaching choice); citalopram/escitalopram (cleaner CYP, QTc dose ceilings); paroxetine (short t½, anticholinergic, worst classic discontinuation); fluvoxamine (CYP1A2/2C19, OCD niche).[3][14][18][20]
Indications beyond “depression tablet”
Major depressive disorder. SSRIs are first-line pharmacological options for moderate–severe unipolar MDD within stepped care; mild illness often starts with psychological therapies and monitoring — Fournier’s patient-level meta-analysis shows average drug–placebo advantage grows with baseline severity.[6][7][27] Network meta-analyses show all common antidepressants beat placebo in adults, with modest between-agent differences in efficacy and acceptability.[1][2]
Anxiety spectrum. Many SSRIs hold indications or guideline roles in GAD, panic disorder, social anxiety disorder and PTSD; start low when activation risk is high.[6][7]
OCD. Serotonin transport inhibitors work as a class; doses often need the upper licensed range and longer trials than depression. Greist meta-analysis established efficacy of SERT inhibitors including SSRIs and clomipramine for OCD.[23]
Other niches. Fluoxetine for bulimia nervosa; selected agents for PMDD; anxiety comorbidity as a choosing factor rather than a reason to avoid the class — place within guideline first-line serotonergic options rather than free-form polypharmacy.[6][7]
Clinical course on treatment
Expect early GI symptoms, possible activation, insomnia or akathisia before mood lift. Delayed benefit over 2–6 weeks is normal; pseudo-resistance includes under-dosing, non-adherence, bipolar miss, substances and medical depression.[3][6] Sexual dysfunction may emerge after mood improves — ask at baseline and follow-up or patients silently stop tablets.[11]
Assessment and investigations
Before first dose: diagnosis and bipolar/mixed screen; suicide risk and means; sexual function baseline; pregnancy potential; NSAID/anticoagulant/antiplatelet use; full serotonergic list (tramadol, triptans, St John’s wort, other ADs, MAOIs); falls risk in elderly.[6][7]
Baseline tests: U&E (sodium); pregnancy test if relevant; ECG when using citalopram/escitalopram at risk doses, known cardiac disease, electrolyte disturbance or QT-prolonging polypharmacy. Routine plasma SSRI levels are not used; measurement-based symptom scores (STAR*D-style) are preferred over vanity drug levels.[3][14][15]
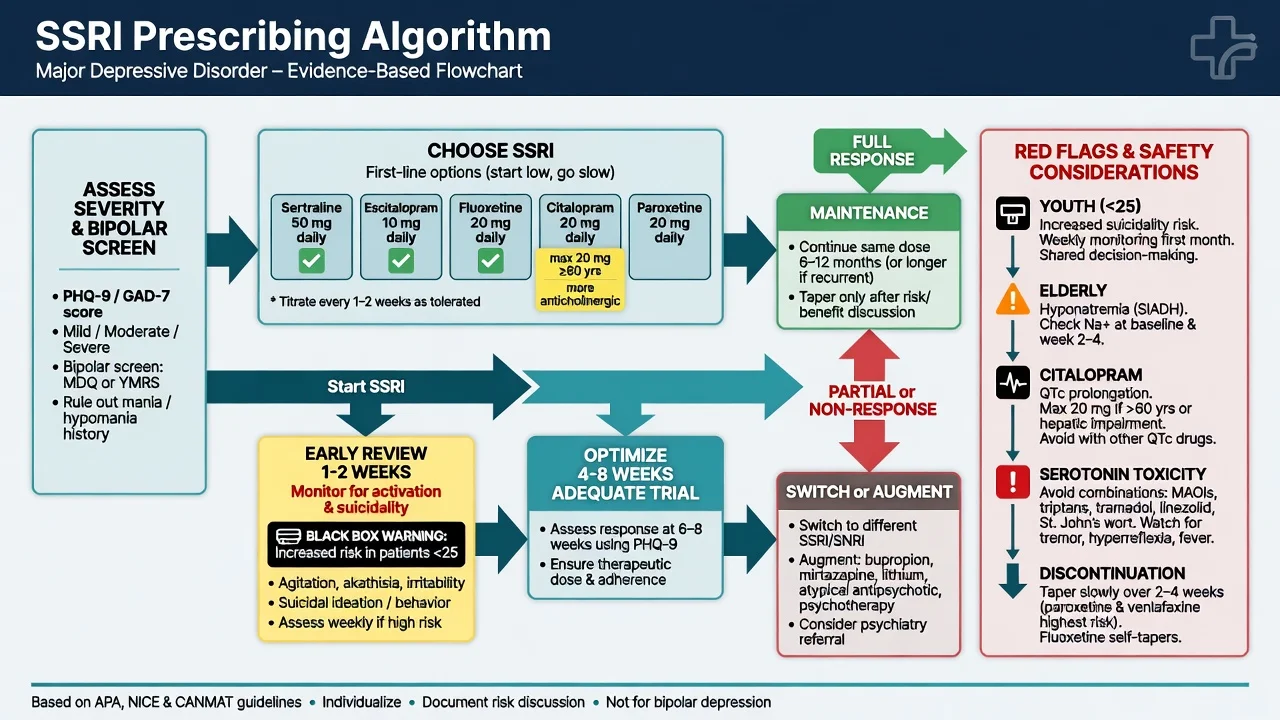
Early review: days to 2 weeks for activation and suicidality (especially under 25), then efficacy/tolerability at 2–4–6 weeks.[9][10]
Adult oral doses and titration (exam scaffolds)
Always individualise; start lower in older adults and anxious/activation-prone patients; confirm current product information and local formulary. Teaching adult oral patterns: sertraline 50 mg daily toward 50–200 mg (anxiety often start 25–50 mg); escitalopram 10 mg toward 10–20 mg (adult max commonly 20 mg, QTc caution); citalopram 20 mg toward max often 40 mg adults (elderly teaching max 20 mg, QTc); fluoxetine 20 mg toward 20–60 mg (higher specialist/OCD/bulimia contexts; long washout before MAOI); paroxetine 20 mg toward 20–50 mg (high discontinuation risk); fluvoxamine 50 mg then titrate (OCD often higher divided doses; CYP burden). Dose optimisation within a structured trial is how STAR*D Level 1 achieved measurable remissions with citalopram under measurement-based care.[3][7][14][15]
Adequate trial: therapeutic dose for typically 4–8 weeks with adherence confirmed before declaring failure.[4][6]
Black-box warning and early suicide risk
FDA analyses of paediatric antidepressant trials showed increased suicidality (ideation/behaviour) versus placebo — the empirical foundation of class black-box warnings and intensive early monitoring practice.[9] Adult proprietary trial meta-analysis demonstrated an age interaction: elevated suicidal behaviour/ideation signal in younger adults, with different patterns in middle and older age groups — never quote one universal relative risk for all ages.[10]
Clinical translation (exam-safe): see patients more often early after start or dose increase; make a safety plan and involve family/carers when appropriate (especially youth); treat activation and akathisia actively; escalating suicidal crisis needs care intensification — not “wait three more weeks for the SSRI”; black-box is monitoring and shared decision, not an absolute ban on youth prescribing when benefit is judged to outweigh risk (TADS context).[9][10][24]
Landmark evidence every candidate must own
SSRI-facing evidence that changes viva answers
STAR*D. Measurement-based citalopram showed structured dose optimisation matters; multi-step outcomes show many patients need more than one step.[3][4] After SSRI failure, switching to sertraline, bupropion-SR or venlafaxine-XR produced broadly similar remission rates — choose by side-effect profile, not mythology of a single strongest switch.[5]
Cipriani NMA. 2009 and 2018 analyses support class efficacy with agent-level rank differences that inform shared decisions without declaring one universal first drug for all humans.[1][2]
Relapse prevention. Continuation antidepressant treatment after response substantially reduces relapse versus stop.[22]
Switching, washouts and combinations
Within/across class: direct switch or cross-taper depending on half-life and withdrawal risk. After nonresponse to one SSRI, another SSRI can work (STAR*D sertraline arm) but partial responders often need augmentation pathways covered in the antidepressants/TRD topics.[5][4]
MAOI red line. Never combine irreversible MAOIs with SSRIs. Typical washout: about 2 weeks from most SSRIs to MAOI; about 5 weeks after fluoxetine because of norfluoxetine. Reverse direction also needs full MAOI washout before SSRI start.[6][17]
Serotonergic polypharmacy: tramadol, pethidine, dextromethorphan, linezolid context, triptans (risk often overstated but not zero), St John’s wort, other SERT inhibitors — document and minimise high-risk stacks.[16][17]
Adverse effects examiners treat as core knowledge
Sexual dysfunction
Montejo’s prospective multicentre study of over a thousand outpatients documented high rates of treatment-emergent sexual dysfunction with many antidepressants including SSRIs. Screen, document, and manage (wait if early and mild, dose reduce if remitted, switch, or add bupropion where appropriate) rather than silence.[11]
Hyponatraemia
Case-control data link antidepressant use with hyponatraemia. Highest vigilance in older adults, female sex, diuretics: baseline Na, recheck if unwell, treat medically and revise the SSRI plan.[12][26]
Bleeding
Population cohort data associate SSRIs with upper GI bleeding; risk rises with concurrent NSAIDs or anticoagulants — gastroprotection or agent review when risk is high.[13]
QTc (citalopram / escitalopram)
EHR and meta-analytic data support SSRI-associated QTc effects with particular regulatory attention to citalopram dose ceilings and escitalopram at higher doses. Respect product maxima (commonly citalopram 40 mg adults / 20 mg many elderly protocols; escitalopram 20 mg adults), check ECG when risk stacks, and avoid casual co-prescription of other QT drugs.[14][15]
Serotonin toxicity
Clinical diagnosis. Boyer and Shannon describe neuromuscular excitation, autonomic hyperactivity and altered mental status. Apply Hunter Serotonin Toxicity Criteria precisely when a serotonergic agent is present (spontaneous clonus; inducible clonus plus agitation or diaphoresis; ocular clonus plus agitation or diaphoresis; tremor plus hyperreflexia; or hypertonia plus temperature above 38°C plus ocular/inducible clonus).[16][17]
Management: stop serotonergic agents; ABC; benzodiazepines; cooling; consider cyproheptadine in specialist protocols; ICU for severe hyperthermia/rigidity. Differentiate from NMS.[17]
Discontinuation / withdrawal syndrome
Abrupt stop or missed doses of short half-life SSRIs (classic paroxetine; also fluvoxamine and others) produce dizziness, electric-shock sensations, flu-like symptoms, irritability, insomnia and sensory disturbances. Randomised interruption data and systematic reviews establish this as a real, usually time-limited syndrome that must be distinguished from relapse; consensus panels recommend education and tapering rather than addiction framing.[18][19][20][28] Fluoxetine’s long half-life often produces milder discontinuation and is sometimes used as a bridge when stopping short-acting agents.[18][28]
Black-box / early risk
- Youth and young adults
- First weeks and after dose rises
- Activation/akathisia
- Intensify review — do not only wait
Sexual / Na / bleed
- Montejo: ask about sex
- Movig: sodium in elderly
- Dalton: GI bleed + NSAIDs
- Adherence and medical safety
QTc agents
- Citalopram ceilings
- Escitalopram higher-dose risk
- ECG if risk stacks
- Sertraline often preferred cardiac teaching
Stop problems
- Paroxetine worst classic
- Taper, do not crash stop
- Fluoxetine smoother
- Discontinuation ≠ relapse always
Special populations
Youth. Elevated relative suicidality signal requires mandatory close review and family engagement. TADS found fluoxetine (especially with CBT) effective for adolescent MDD versus placebo on primary analyses used in exams — evidence supports careful use, not reflexive refusal.[9][24]
Older adults. Start low, go slow; sodium and falls risk; Coupland cohort links antidepressants with adverse outcomes requiring thoughtful selection and monitoring; lower citalopram maxima.[12][26][14]
Pregnancy and lactation. Individualised risk–benefit: untreated depression harms mother and fetus; large meta-analytic data on early SSRI exposure and malformations inform counselling without binary panic or denial. Prefer agents with more reproductive data when possible; coordinate perinatal psychiatry; never crash-stop without a plan (discontinuation plus relapse risk).[21][6]
Hepatic impairment / CYP. Prefer simpler kinetics; mind fluoxetine/paroxetine 2D6 (TCA level spikes; tamoxifen teaching debate) and fluvoxamine 1A2 interactions.[7]
Prognosis and disposition
Response (≥50% symptom reduction) is not enough — remission is the goal because residual symptoms drive relapse.[4] After a first episode, continue months after remission; after recurrent illness, longer maintenance is often justified (Geddes-level evidence).[22] Step up to crisis services, inpatient care, augmentation or ECT pathways when severity or risk outstrips outpatient titration speed.[6]
Regional guideline deltas
RANZCP 2020 mood guidelines anchor ANZ fellowship practice in formulation-based stepped care and careful antidepressant use with safety monitoring.[6] CANMAT 2016/2023 provide granular first-line pharmacological choices and ranks widely used in exams.[7][8] NICE emphasises stepped care and review intensity. APA/FDA black-box framing drives US monitoring language. Thresholds and formulary differ; the exam constant is adequate trial logic, early risk review, and agent-specific safety — not a single global brand preference.
Exam pearls
SSRI SAFE start checklist
SSRISAFE
References
- [1]Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis Lancet, 2018.PMID 29477251
- [2]Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis Lancet, 2009.PMID 19185342
- [3]Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice Am J Psychiatry, 2006.PMID 16390886
- [4]Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report Am J Psychiatry, 2006.PMID 17074942
- [5]Rush AJ, Trivedi MH, Wisniewski SR, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression N Engl J Med, 2006.PMID 16554525
- [6]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [7]Kennedy SH, Lam RW, McIntyre RS, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments Can J Psychiatry, 2016.PMID 27486148
- [8]Lam RW, Kennedy SH, Adams C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder Can J Psychiatry, 2024.PMID 38711351
- [9]Hammad TA, Laughren T, Racoosin J Suicidality in pediatric patients treated with antidepressant drugs Arch Gen Psychiatry, 2006.PMID 16520440
- [10]Stone M, Laughren T, Jones ML, et al. Risk of suicidality in clinical trials of antidepressants in adults: analysis of proprietary data submitted to US Food and Drug Administration BMJ, 2009.PMID 19671933
- [11]Montejo AL, Llorca G, Izquierdo JA, et al. Incidence of sexual dysfunction associated with antidepressant agents: a prospective multicenter study of 1022 outpatients J Clin Psychiatry, 2001.PMID 11229449
- [12]Movig KL, Leufkens HG, Lenderink AW, et al. Association between antidepressant drug use and hyponatraemia: a case-control study Br J Clin Pharmacol, 2002.PMID 11966666
- [13]Dalton SO, Johansen C, Mellemkjaer L, et al. Use of selective serotonin reuptake inhibitors and risk of upper gastrointestinal tract bleeding: a population-based cohort study Arch Intern Med, 2003.PMID 12523917
- [14]Castro VM, Clements CC, Murphy SN, et al. QT interval and antidepressant use: a cross sectional study of electronic health records BMJ, 2013.PMID 23360890
- [15]Beach SR, Kostis WJ, Celano CM, et al. Meta-analysis of selective serotonin reuptake inhibitor-associated QTc prolongation J Clin Psychiatry, 2014.PMID 24922496
- [16]Dunkley EJ, Isbister GK, Sibbritt D, et al. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity QJM, 2003.PMID 12925718
- [17]Boyer EW, Shannon M The serotonin syndrome N Engl J Med, 2005.PMID 15784664
- [18]Schatzberg AF, Blier P, Delgado PL, et al. Antidepressant discontinuation syndrome: consensus panel recommendations for clinical management and additional research J Clin Psychiatry, 2006.PMID 16683860
- [19]Fava GA, Gatti A, Belaise C, et al. Withdrawal Symptoms after Selective Serotonin Reuptake Inhibitor Discontinuation: A Systematic Review Psychother Psychosom, 2015.PMID 25721705
- [20]Rosenbaum JF, Fava M, Hoog SL, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial Biol Psychiatry, 1998.PMID 9646889
- [21]Gao SY, Wu QJ, Sun C, et al. Selective serotonin reuptake inhibitor use during early pregnancy and congenital malformations: a systematic review and meta-analysis of cohort studies of more than 9 million births BMC Med, 2018.PMID 30415641
- [22]Geddes JR, Carney SM, Davies C, et al. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review Lancet, 2003.PMID 12606176
- [23]Greist JH, Jefferson JW, Kobak KA, et al. Efficacy and tolerability of serotonin transport inhibitors in obsessive-compulsive disorder. A meta-analysis Arch Gen Psychiatry, 1995.PMID 7811162
- [24]March J, Silva S, Petrycki S, et al. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents With Depression Study (TADS) randomized controlled trial JAMA, 2004.PMID 15315995
- [25]Whyte IM, Dawson AH, Buckley NA Relative toxicity of venlafaxine and selective serotonin reuptake inhibitors in overdose compared to tricyclic antidepressants QJM, 2003.PMID 12702786
- [26]Coupland C, Dhiman P, Morriss R, et al. Antidepressant use and risk of adverse outcomes in older people: population based cohort study BMJ, 2011.PMID 21810886
- [27]Fournier JC, DeRubeis RJ, Hollon SD, et al. Antidepressant drug effects and depression severity: a patient-level meta-analysis JAMA, 2010.PMID 20051569
- [28]Haddad PM Antidepressant discontinuation syndromes Drug Saf, 2001.PMID 11347722