Psych · Psychopharmacology — stimulants and ADHD medications
Stimulants and ADHD medications
Also known as ADHD stimulants · Methylphenidate · Amphetamines ADHD · Lisdexamfetamine · Atomoxetine · Guanfacine · Clonidine ADHD · ADHD pharmacotherapy
Exam-exhaustive fellowship pharmacology of ADHD medications — methylphenidate and amphetamine formulations with doses and monitoring, atomoxetine, guanfacine and clonidine, DAT/NET mechanisms, MTA and Cortese NMA, cardiovascular safety (Cooper/Habel/Hennissen/Farhat), diversion and misuse, switching, adult versus child pathways. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
ADHD pharmacotherapy is a high-yield drug-class viva across FRANZCP, MRCPsych and ABPN. Examiners expect mechanism maps, agent-level doses, formulation logic, landmark comparative evidence, cardiovascular risk communication, diversion safeguards, and adult-versus-child differences — not brand slogans or undergraduate summaries. This topic is the prescribing spine that the ADHD-across-the-lifespan clinical topic plugs into.[3][22][24]
Definition and classification
ADHD medications are symptomatic treatments that reduce core inattention and/or hyperactivity-impulsivity and related functional impairment. They do not cure the neurodevelopmental syndrome, replace psychoeducation or environmental supports, or license diagnosis from a single rating scale.[22][24]
Working exam taxonomy. Class structure below is the standard fellowship scaffold for choice and monitoring questions.[3][4][5][8][22]
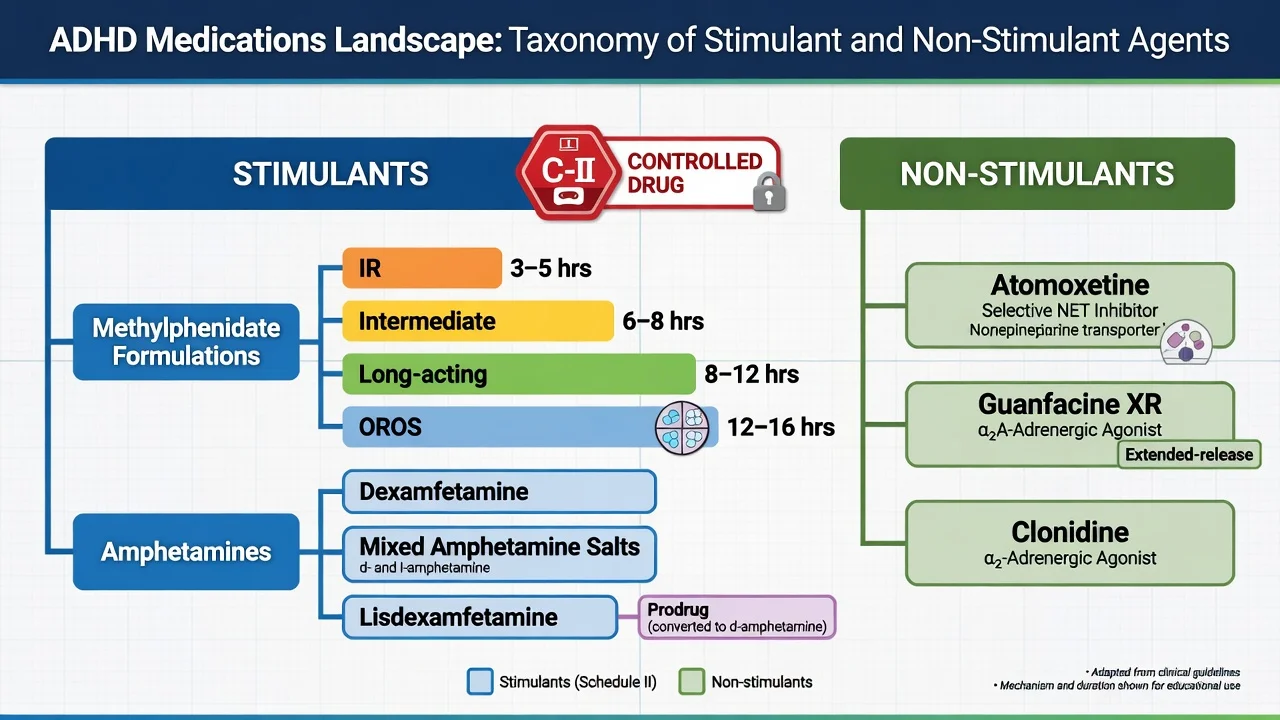
| Class | Core agents (examples) | Exam mechanism line | Controlled-drug issues |
|---|---|---|---|
| Methylphenidate stimulants | IR tablets; intermediate/long-acting products including OROS-style once-daily forms | DAT (and NET) reuptake blockade | Yes — diversion risk |
| Amphetamine stimulants | Dexamfetamine; mixed amphetamine salts; lisdexamfetamine prodrug | Reverse transport / vesicular effects plus reuptake effects | Yes — diversion risk (prodrug relatively less attractive than IR) |
| Atomoxetine | Oral selective NET inhibitor | Continuous noradrenergic tone; delayed clinical onset | Usually not a stimulant controlled drug |
| Alpha-2 agonists | Guanfacine XR; clonidine XR/IR | Postsynaptic alpha-2A (prefrontal) plus autonomic effects | Not stimulants; sedation and BP/HR dominate |
| Incomplete cross-class response and controlled-drug logistics drive formulation choice in practice.[3][27] |
Mechanisms — the viva core
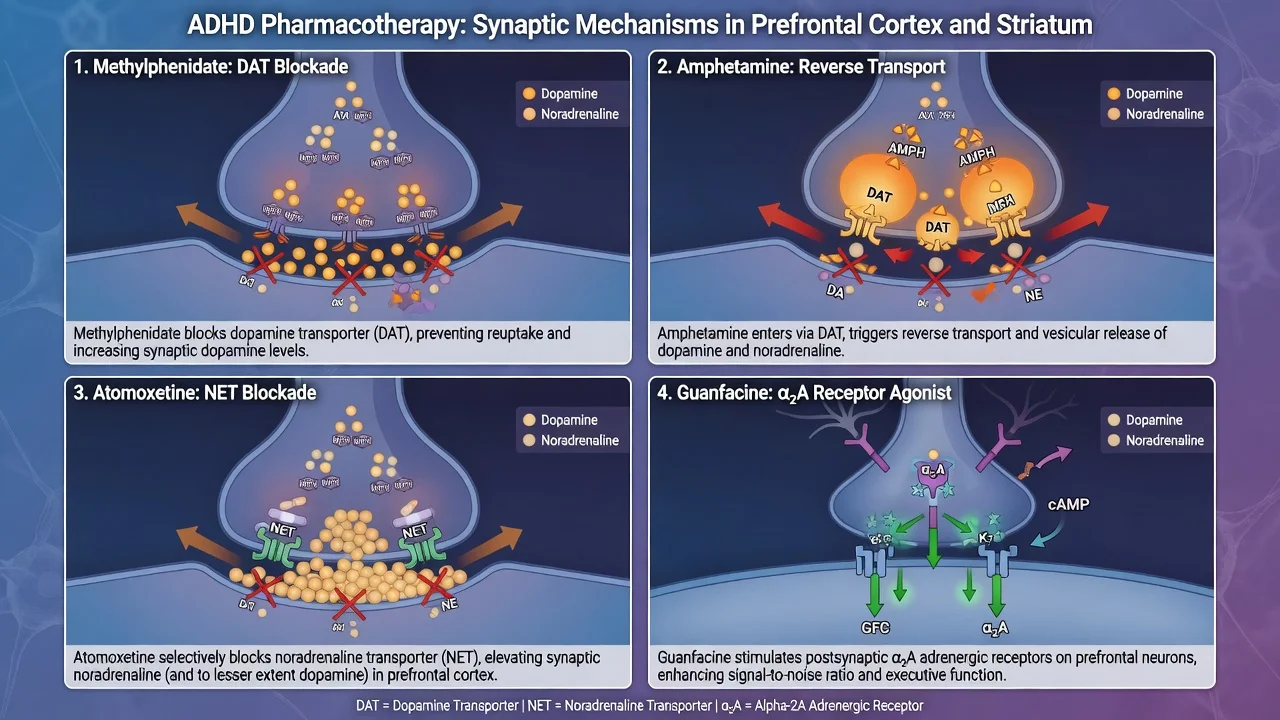
Methylphenidate. Therapeutic oral doses increase extracellular dopamine in the human brain via dopamine transporter (DAT) blockade — the classic PET teaching point from Volkow and colleagues. Clinical onset of core-symptom benefit is often same day at an adequate dose, which is how you judge an early stimulant trial in viva.[4][3]
Amphetamines. Share catecholamine facilitation but are not pharmacologically identical to methylphenidate: reverse transport and vesicular effects contribute, which helps explain cross-class incomplete response (some patients respond to one stimulant class after failing the other).[3][27]
Atomoxetine. Selective noradrenaline reuptake inhibition. Placebo-controlled trials in children/adolescents and adults show separation on ADHD rating scales over weeks, not hours — counsel patients so they do not declare failure on day three.[5][6]
Guanfacine and clonidine. Alpha-2 agonists with prefrontal and autonomic effects. RCT evidence supports guanfacine extended-release as monotherapy versus placebo in youth; clonidine extended-release has monotherapy and stimulant-adjunct data. Sedation, hypotension and bradycardia are mechanism-linked, not surprises.[8][9][10]
Epidemiology and risk context for prescribing
Treated ADHD populations have high rates of medication exposure; examiners care about absolute serious cardiovascular event rates, growth, diversion, and comorbid substance use, not scare headlines alone.[16][17][12]
Numbers that change counselling tone
When to prescribe — clinical use, not diagnosis
Pharmacotherapy is for confirmed ADHD with multi-setting impairment after multi-informant assessment. Behavioural, educational and organisational interventions remain part of multimodal care; medicines are not a substitute for classroom or workplace adjustments.[1][22][24]
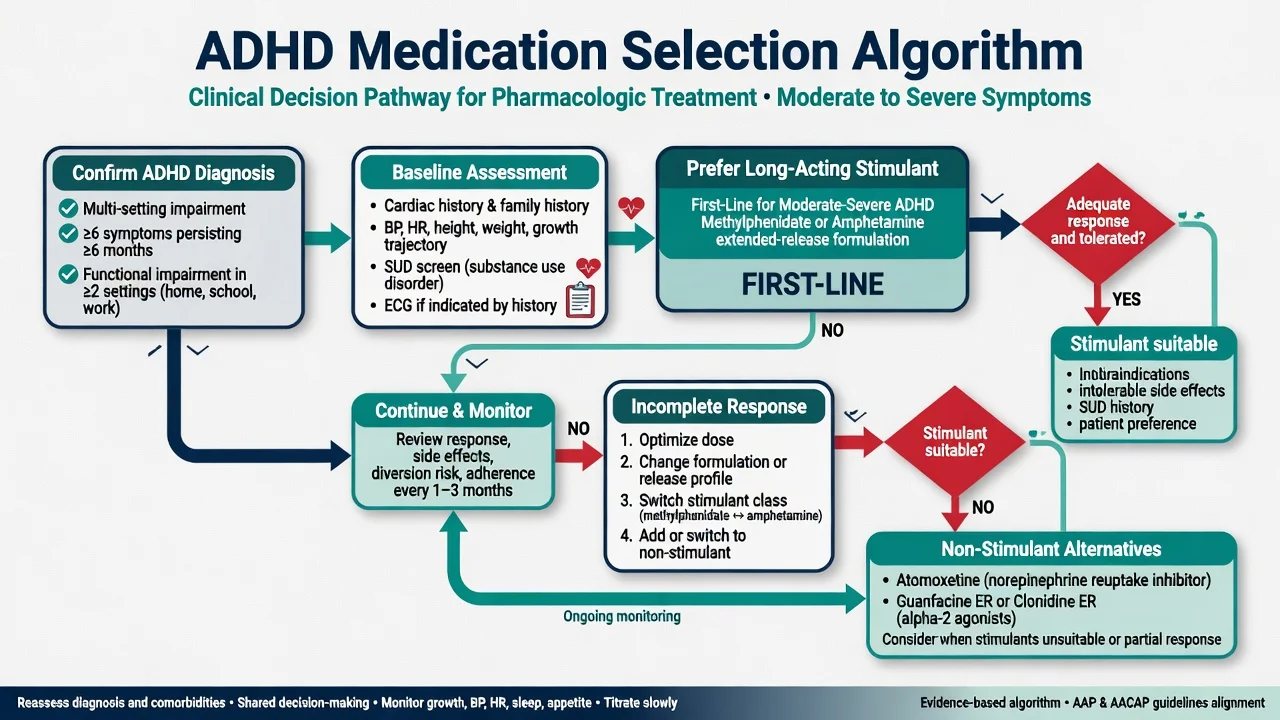
Baseline before first dose (document): personal cardiac history (chest pain, syncope, exercise symptoms, known structural disease), family sudden cardiac death or early cardiomyopathy, resting BP and heart rate, height and weight with growth chart in youth, tics history, mood and bipolar-spectrum screen, substance use and diversion risk, pregnancy potential, concurrent medicines (especially MAOIs), and shared functional targets (schoolwork, relationships, driving, occupational safety).[16][20][22][24]
Agent-level doses and practical notes
Ranges below are typical exam-level starting and titration frameworks. Always individualise for age, formulation, hepatic/renal function and local product information — labels and PBS/authority rules differ by jurisdiction.[3][22][24]
Methylphenidate
| Formulation | Typical start (exam framework) | Titration / usual ceiling notes | Practical pearls |
|---|---|---|---|
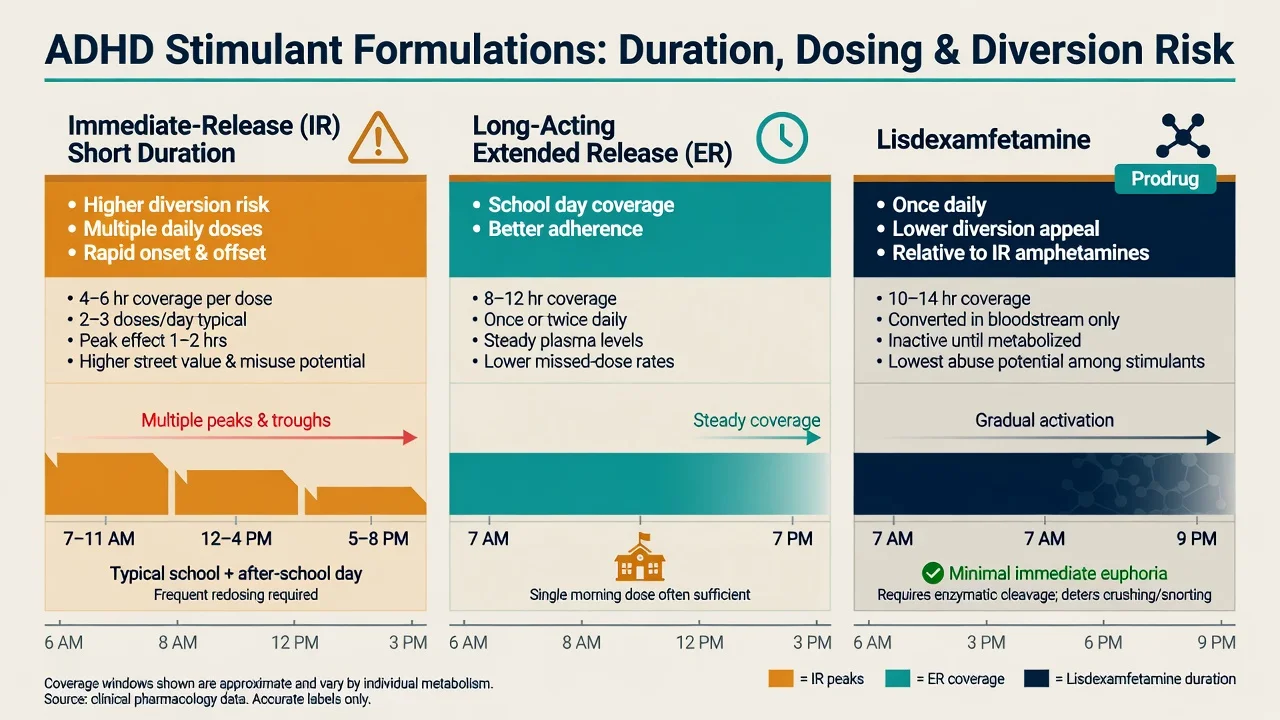
| IR methylphenidate | Child: often 5 mg orally 2–3 times daily | Titrate weekly; many product maxima around 60 mg/day (check label) | Covers short windows; higher diversion risk than long-acting |
| Long-acting / OROS-style | Product-specific morning dose (e.g. mid-teens to adult OROS starts commonly 18 mg once daily in many labels) | Titrate to response and tolerability; adult OROS RCT used dose-escalation designs | Prefer for school/work day coverage and adherence |
| OROS methylphenidate has placebo-controlled adult efficacy and safety data with structured dose escalation; paediatric practice parameters still frame stimulants as highly effective first-line pharmacotherapy when impairment warrants medication.[13][22][3] |
Amphetamines and lisdexamfetamine
| Agent | Typical start (exam framework) | Titration notes | Practical pearls |
|---|---|---|---|
| Dexamfetamine / mixed amphetamine salts IR | Low morning start (often 2.5–5 mg range depending on product/age) | Divide IR doses; titrate weekly | Strong adult efficacy signal historically |
| Mixed amphetamine salts XR | Product-specific morning dose | Titrate within labelled range | Once-daily coverage |
| Lisdexamfetamine | Often 20–30 mg orally each morning | Titrate weekly; common max 70 mg/day on many labels | Prodrug activated after absorption — useful when diversion is a concern |
| Lisdexamfetamine demonstrated efficacy versus placebo in children, with active comparison to mixed amphetamine salts extended-release in a double-blind design. Mixed amphetamine salts have classic adult RCT support.[15][14][3] |
Atomoxetine
| Population | Exam dose framework | Onset / monitoring emphasis |
|---|---|---|
| Children/adolescents | Often 0.5 mg/kg/day for several days, then target around 1.2 mg/kg/day (max commonly 1.4 mg/kg/day or absolute label max — check PI) | Weeks to full effect; GI upset, appetite, mood, BP/HR, hepatic warnings |
| Adults | Often 40 mg/day for several days, then 80 mg/day; some need 100 mg/day | Adult RCTs support efficacy; long-term open-label safety data exist |
| Once-daily atomoxetine separated from placebo in youth; two adult RCTs also showed benefit. Newcorn and colleagues demonstrated that osmotically released methylphenidate was more efficacious on average than atomoxetine in a head-to-head acute comparison, but differential responders exist — failure of one does not forbid trial of the other.[5][6][7][26] |
Guanfacine XR and clonidine
| Agent | Exam dose framework | Key monitoring |
|---|---|---|
| Guanfacine XR | Start 1 mg orally once daily; increase by 1 mg/week as tolerated; common trial range 1–4 mg/day (higher adolescent maxima on some labels) | Sedation, hypotension, bradycardia; taper after prolonged use |
| Clonidine XR | Start 0.1 mg at bedtime or divided; titrate toward 0.1–0.4 mg/day labelled ranges | Sedation more prominent; mono and stimulant-adjunct RCTs |
| Clonidine IR (where used) | Low night-time starts for sleep/tics context | Same autonomic cautions; formulation availability varies |
| Guanfacine XR has placebo-controlled youth efficacy data. Clonidine XR has paediatric monotherapy evidence and add-on-to-stimulant data — examiners like both mono and adjunct framings.[8][9][10] |
Monitoring schedule
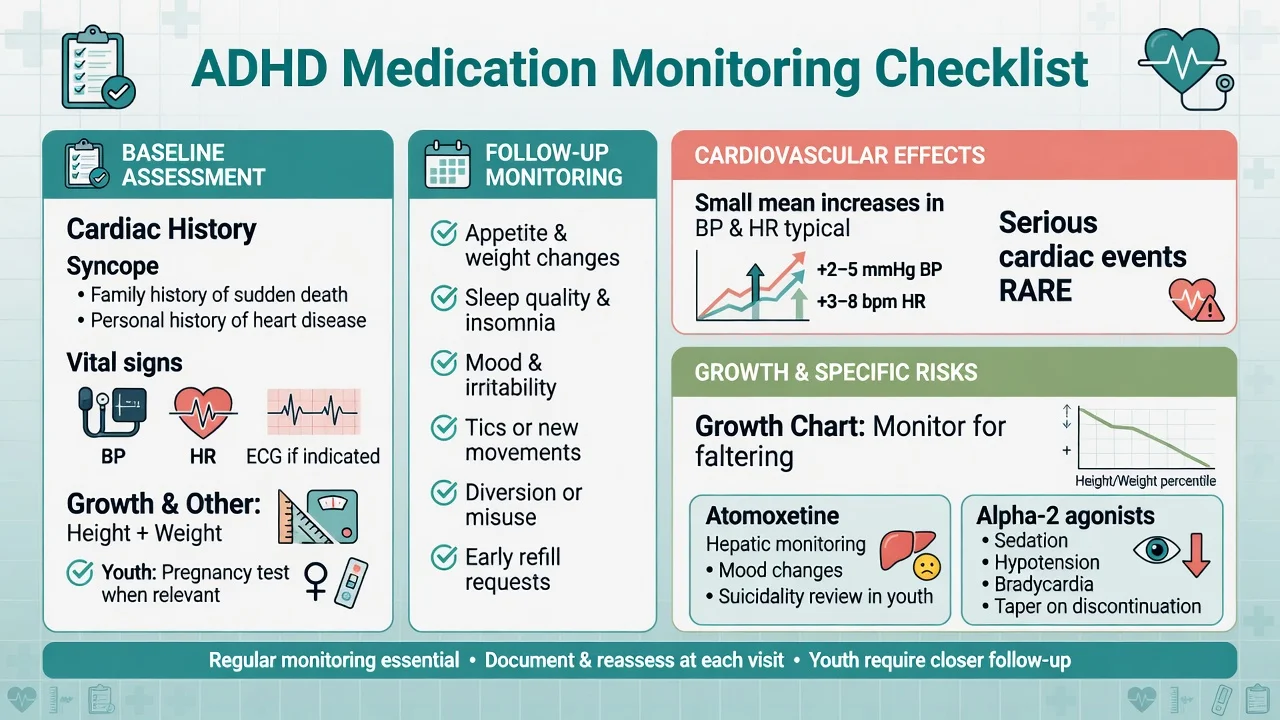
Every visit (minimum): efficacy against pre-agreed functional targets; appetite and weight (plot height/weight in youth); sleep; mood, anxiety, irritability or emotional blunting; tics; BP and HR; adherence; early refill requests or lost prescriptions (diversion flags); driving and substance use review when relevant.[20][21][22]
Cardiovascular communication. Meta-analysis of trials shows small mean increases in blood pressure and heart rate with methylphenidate, amphetamines and atomoxetine. Large observational studies in children/young adults (Cooper) and young/middle-aged adults (Habel) did not find a clear increase in serious cardiovascular events attributable to ADHD drugs in the studied populations — still take personal/family cardiac history seriously and investigate syncope or chest pain rather than escalating the dose.[18][16][17][19]
ECG. Not a universal ritual for every healthy child in every guideline, but document risk-based reasoning; obtain ECG (and cardiology input) when history or examination raises concern.[20][22]
Incomplete response, switching and combination
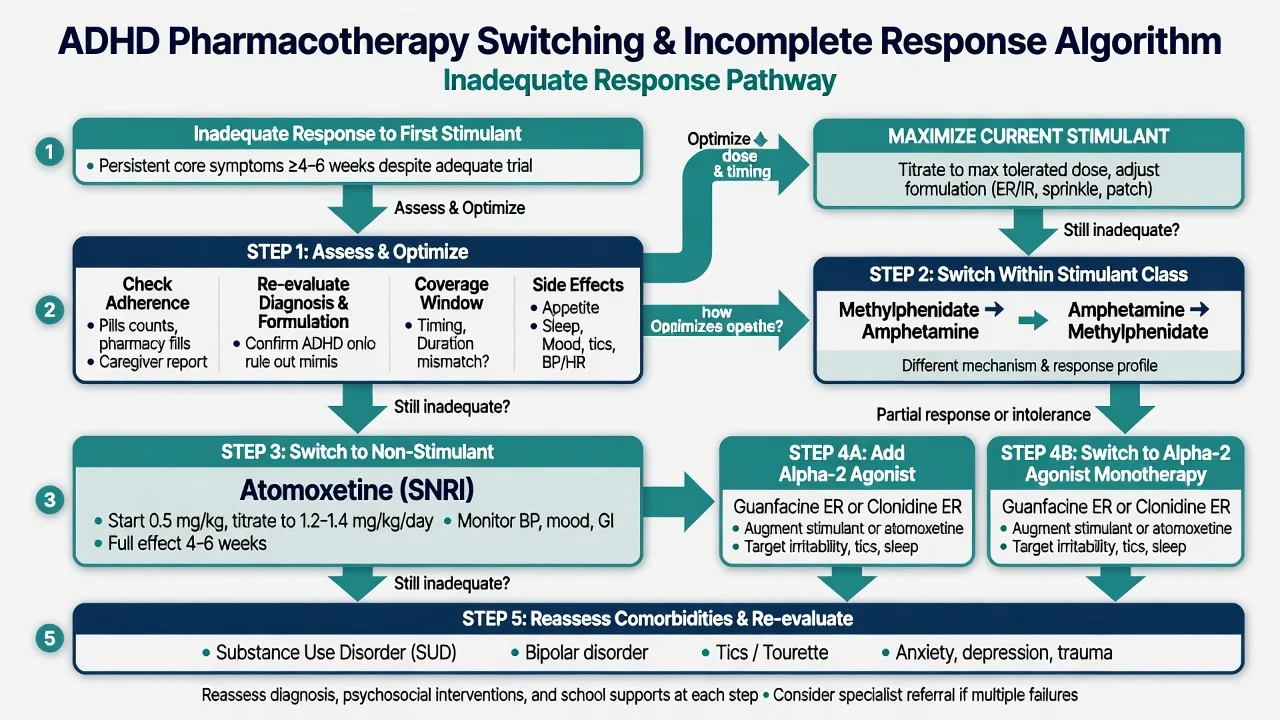
Before declaring failure: confirm diagnosis and multi-setting impairment; adherence; adequate dose and duration; whether the formulation actually covers the problematic hours; sleep deprivation, anxiety, learning disorder, autism features, substances, or bipolar spectrum masquerading as “nonresponse.”[27][22]
Algorithm (exam structure): incomplete-response care is sequential — optimise, switch class, then non-stimulant or adjunct, while repairing multimodal supports.[27][7][3][24]
- Optimise current agent (dose, timing, IR top-up only with a plan, not endless polypharmacy).[27]
- Switch within stimulants (methylphenidate to amphetamine class or reverse) — different pharmacology and incomplete cross-response.[3][27]
- Switch to atomoxetine if stimulants unsuitable or failed, accepting slower onset.[7][5]
- Use guanfacine or clonidine as alternative or adjunct (especially tics, residual hyperarousal, sleep-onset problems) with autonomic monitoring.[8][9][10]
- Revisit multimodal care: CBT/skills for adults, parent training/school strategies for youth.[24]
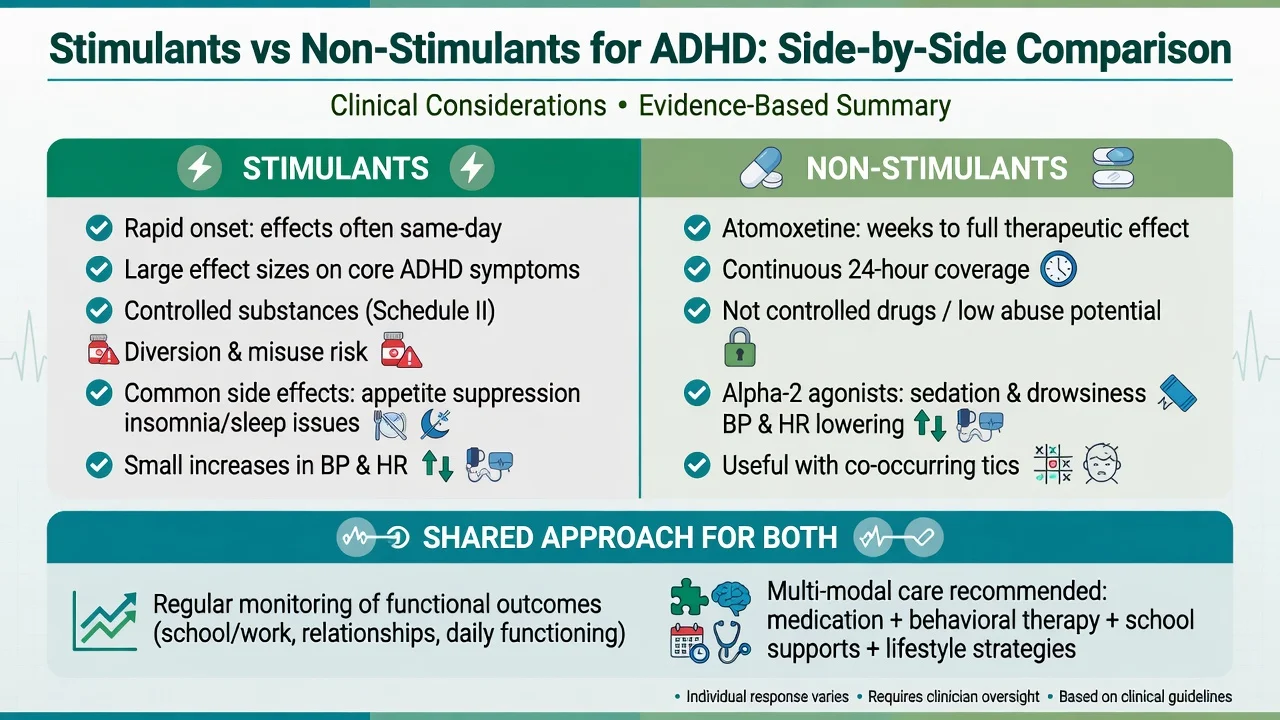
Long-acting stimulant
- Largest short-term effect sizes in NMA
- Same-day onset aids early titration
- Controlled drug logistics and diversion risk
- Appetite/sleep/growth monitoring
Atomoxetine
- Continuous coverage without controlled status
- Weeks to judge full trial
- Useful high diversion/SUD context
- BP/HR, GI, mood, hepatic vigilance
Alpha-2 agonist
- Mono or adjunct evidence in youth
- Tics/sleep/arousal niche
- Sedation and BP/HR lowering
- Taper after prolonged use
Special scenarios
Child and adolescent
MTA 14-month findings: carefully delivered medication management and combined medication-plus-behavioural treatment outperformed behavioural treatment alone and community care for core ADHD symptoms; combination had advantages for some non-ADHD domains and sometimes lower medication dose. At longer follow-up, between-group differences fade as community treatment patterns converge — do not overclaim lifelong superiority of one MTA arm.[1][2]
AACAP-style parameters emphasise comprehensive assessment and multimodal care with stimulants as highly effective first-line pharmacotherapy when impairment warrants medication, plus systematic monitoring of growth and cardiovascular parameters.[22]
Adults
Adult ADHD medication is evidence-based. Cortese NMA and adult meta-analyses support efficacy of stimulants, with amphetamines performing particularly strongly in some adult strata; methylphenidate remains effective; atomoxetine has RCT and longer-term open-label support. European consensus statements emphasise diagnosis quality, comorbidity, driving, and shared decision on formulation.[3][25][13][6][24]
Substance use and diversion
ADHD and SUD frequently co-occur. Meta-analytic work does not support the myth that properly treated stimulant therapy “creates” later substance abuse; some data suggest protective associations, while modern longitudinal MTA-linked analyses require nuanced reading rather than slogans. Practically: prefer long-acting or prodrug formulations, smaller dispensed quantities, supervised dosing, and non-stimulants when diversion risk is high; treat SUD concurrently.[11][12][28]
Tics
Stimulants are often still usable with monitoring. Alpha-2 agonists can help ADHD and tics in selected patients. Do not automatically withhold all stimulants for mild tics.[8][22]
Complications and pitfalls
Common adverse effects and management logic (Graham/Cortese frameworks): appetite suppression and weight loss — dose timing with meals, calorie-dense snacks, growth plots, holidays only if functionally justified; insomnia — earlier last dose, reduce late IR top-ups; emotional lability/irritability — check rebound, dose peak, comorbidity; tics — observe, adjust, consider alpha-2; sexual side-effects less central than in antidepressants but discuss if raised.[20][21]
Absolute interaction pearl: do not combine stimulants or atomoxetine with MAOIs — respect washouts. Alpha-2 pearl: taper after prolonged use to reduce rebound hypertension risk.[20][22]
Classic fails: diagnosing from a questionnaire alone; short-acting stimulants into a diversion network without safeguards; ignoring growth charts; promising cure; missing bipolar before stimulant start; abrupt alpha-2 stop; scaremongering CV risk without absolute-risk numbers, or ignoring cardiac red flags entirely.[16][12][22]
Evidence, guidelines and regional differences
Landmark evidence every candidate must name
Australian and New Zealand practice follows jurisdiction-specific stimulant authority/PBS and controlled-drug rules (state and territory statutes differ — do not invent a single national section number). Specialist initiation and shared care with GPs are common. Always check current local prescribing rules.[22][24]
Special populations
Preschool: specialist territory; behavioural interventions first in most frameworks; medication only with high impairment and specialist oversight.[22]
Pregnancy and lactation: individualised risk–benefit; untreated ADHD can impair driving, work and parenting capacity; involve obstetric and perinatal psychiatry advice rather than reflexive stop or continue slogans. Product-specific data change — check current sources at the time of care.[24][20]
Intellectual disability / complex neurodevelopment: start low, go slow, track behaviour carefully, avoid stacking sedating agents without a plan.[22]
Older adults: rare primary new starts; cardiovascular risk dominates; scrutinise indication and polypharmacy.[17][19]
Prognosis and disposition
Short-term pharmacologic effect sizes for core symptoms are robust. Long-term outcome depends on adherence, comorbidity treatment, education/occupation supports, and substance trajectories — not tablets alone. Medication periods have been associated with reduced criminality in large Swedish registry data (Lichtenstein context is often examined via the ADHD clinical topic; keep functional risk on your script). Plan review intensity higher at initiation and dose changes; step to shared care when stable.[1][2][3][24]
Exam pearls
STIMULATE
- MTA: carefully titrated medication management beat community care for core symptoms at 14 months — quality of titration matters.[1]
- Cortese 2018: most medicines beat placebo short-term; stimulants have the largest average effects; age strata modify preference talk.[3]
- Newcorn: average superiority of OROS MPH over atomoxetine does not abolish ATX as a legitimate next step for nonresponders or special risk groups.[7]
- Serious CV events are rare in large cohorts; small BP/HR rises are real — both statements can be true.[16][17][18]
- Wilens meta: stimulant treatment of ADHD has not been shown to increase later SUD risk in the aggregated literature examined.[11]
Self-test: name three reasons a stimulant 'failed'
Adherence or diversion; inadequate dose or wrong coverage hours; wrong diagnosis/comorbidity (anxiety, learning disorder, bipolar, SUD, sleep apnoea); intolerable side-effects causing covert non-adherence; expectation of personality change rather than functional targets. Fix the process before stacking agents.[27][22]
References
- [1]The MTA Cooperative Group A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. The MTA Cooperative Group. Multimodal Treatment Study of Children with ADHD Arch Gen Psychiatry, 1999.PMID 10591283
- [2]Molina BSG, Hinshaw SP, Swanson JM, et al. The MTA at 8 years: prospective follow-up of children treated for combined-type ADHD in a multisite study J Am Acad Child Adolesc Psychiatry, 2009.PMID 19318991
- [3]Cortese S, Adamo N, Del Giovane C, et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis Lancet Psychiatry, 2018.PMID 30097390
- [4]Volkow ND, Wang G, Fowler JS, et al. Therapeutic doses of oral methylphenidate significantly increase extracellular dopamine in the human brain J Neurosci, 2001.PMID 11160455
- [5]Michelson D, Allen AJ, Busner J, et al. Once-daily atomoxetine treatment for children and adolescents with attention deficit hyperactivity disorder: a randomized, placebo-controlled study Am J Psychiatry, 2002.PMID 12411225
- [6]Michelson D, Adler L, Spencer T, et al. Atomoxetine in adults with ADHD: two randomized, placebo-controlled studies Biol Psychiatry, 2003.PMID 12547466
- [7]Newcorn JH, Kratochvil CJ, Allen AJ, et al. Atomoxetine and osmotically released methylphenidate for the treatment of attention deficit hyperactivity disorder: acute comparison and differential response Am J Psychiatry, 2008.PMID 18281409
- [8]Sallee FR, McGough J, Wigal T, et al. Guanfacine extended release in children and adolescents with attention-deficit/hyperactivity disorder: a placebo-controlled trial J Am Acad Child Adolesc Psychiatry, 2009.PMID 19106767
- [9]Jain R, Segal S, Kollins SH, et al. Clonidine extended-release tablets for pediatric patients with attention-deficit/hyperactivity disorder J Am Acad Child Adolesc Psychiatry, 2011.PMID 21241954
- [10]Kollins SH, Jain R, Brams M, et al. Clonidine extended-release tablets as add-on therapy to psychostimulants in children and adolescents with ADHD Pediatrics, 2011.PMID 21555501
- [11]Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature Pediatrics, 2003.PMID 12509574
- [12]Wilens TE Attention deficit hyperactivity disorder and substance use disorders Am J Psychiatry, 2006.PMID 17151154
- [13]Adler LA, Zimmerman B, Starr HL, et al. Efficacy and safety of OROS methylphenidate in adults with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled, double-blind, parallel group, dose-escalation study J Clin Psychopharmacol, 2009.PMID 19440077
- [14]Spencer T, Biederman J, Wilens T, et al. Efficacy of a mixed amphetamine salts compound in adults with attention-deficit/hyperactivity disorder Arch Gen Psychiatry, 2001.PMID 11483144
- [15]Biederman J, Boellner SW, Childress A, et al. Lisdexamfetamine dimesylate and mixed amphetamine salts extended-release in children with ADHD: a double-blind, placebo-controlled study Biol Psychiatry, 2007.PMID 17631866
- [16]Cooper WO, Habel LA, Sox CM, et al. ADHD drugs and serious cardiovascular events in children and young adults N Engl J Med, 2011.PMID 22043968
- [17]Habel LA, Cooper WO, Sox CM, et al. ADHD medications and risk of serious cardiovascular events in young and middle-aged adults JAMA, 2011.PMID 22161946
- [18]Hennissen L, Bakker MJ, Banaschewski T, et al. Cardiovascular Effects of Stimulant and Non-Stimulant Medication for Children and Adolescents with ADHD: A Systematic Review and Meta-Analysis of Trials of Methylphenidate, Amphetamines and Atomoxetine CNS Drugs, 2017.PMID 28236285
- [19]Farhat LC, Lannes A, Del Giovane C, et al. Comparative cardiovascular safety of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis Lancet Psychiatry, 2025.PMID 40203844
- [20]Graham J, Banaschewski T, Buitelaar J, et al. European guidelines on managing adverse effects of medication for ADHD Eur Child Adolesc Psychiatry, 2011.PMID 21042924
- [21]Cortese S, Holtmann M, Banaschewski T, et al. Practitioner review: current best practice in the management of adverse events during treatment with ADHD medications in children and adolescents J Child Psychol Psychiatry, 2013.PMID 23294014
- [22]Pliszka S; AACAP Work Group on Quality Issues Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder J Am Acad Child Adolesc Psychiatry, 2007.PMID 17581453
- [23]Kooij SJ, Bejerot S, Blackwell A, et al. European consensus statement on diagnosis and treatment of adult ADHD: The European Network Adult ADHD BMC Psychiatry, 2010.PMID 20815868
- [24]Kooij JJS, Bijlenga D, Salerno L, et al. Updated European Consensus Statement on diagnosis and treatment of adult ADHD Eur Psychiatry, 2019.PMID 30453134
- [25]Faraone SV, Glatt SJ A comparison of the efficacy of medications for adult attention-deficit/hyperactivity disorder using meta-analysis of effect sizes J Clin Psychiatry, 2010.PMID 20051220
- [26]Adler LA, Spencer TJ, Williams DW, et al. Long-term, open-label safety and efficacy of atomoxetine in adults with ADHD: final report of a 4-year study J Atten Disord, 2008.PMID 18448861
- [27]Childress AC, Sallee FR Attention-deficit/hyperactivity disorder with inadequate response to stimulants: approaches to management CNS Drugs, 2014.PMID 24402970
- [28]Molina BSG, Kennedy TM, Howard AL, et al. Association Between Stimulant Treatment and Substance Use Through Adolescence Into Early Adulthood JAMA Psychiatry, 2023.PMID 37405756