Psych · Psychopharmacology — TCAs and heterocyclics
Tricyclic and heterocyclic antidepressants
Also known as TCAs · Tricyclic antidepressants · Amitriptyline · Nortriptyline · Clomipramine · Imipramine · Dosulepin · Heterocyclic antidepressants · Trazodone · Maprotiline
Exam-exhaustive fellowship monograph on tricyclic and heterocyclic antidepressants — tertiary vs secondary amines, residual indications (MDD, OCD/clomipramine, neuropathic pain, migraine), adult doses, AGNP-style therapeutic plasma levels, ECG and anticholinergic monitoring, fatal toxicity index, full overdose algorithm (QRS, aVR, sodium bicarbonate, avoid list), heterocyclic relatives, MAOI washouts, special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Definition and classification
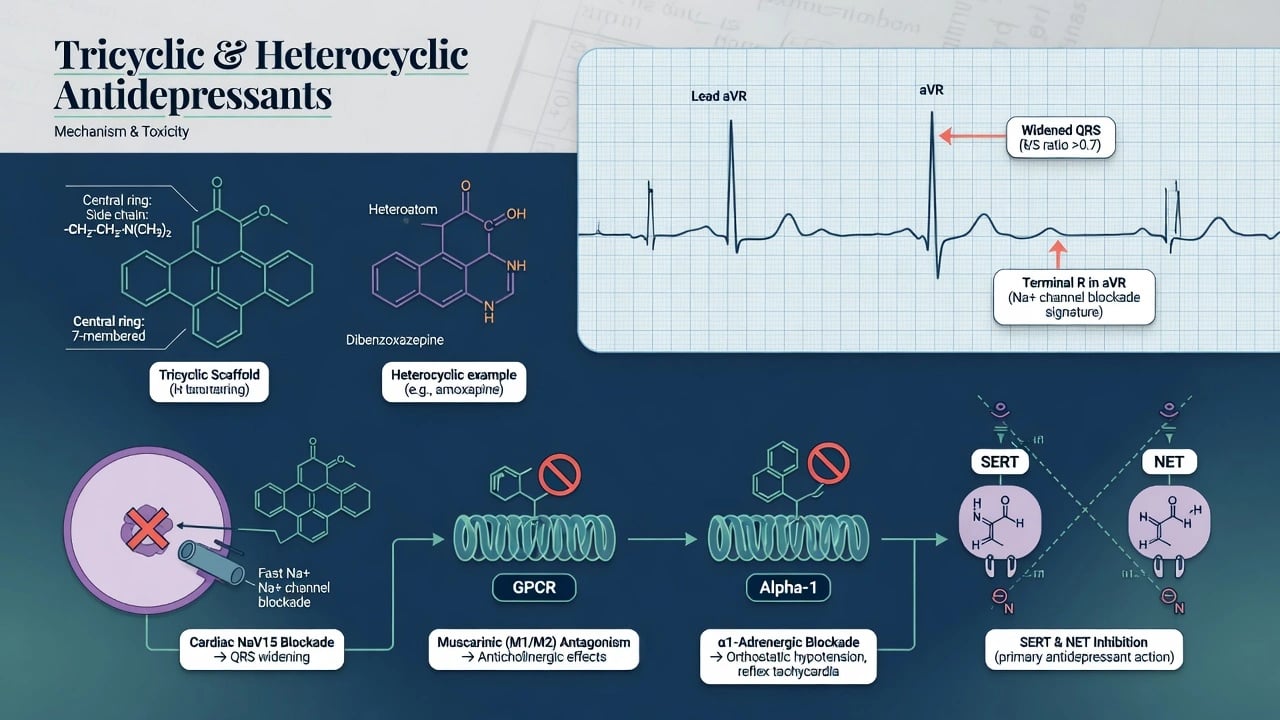
Tricyclic antidepressants are lipophilic three-ring compounds that inhibit the serotonin transporter (SERT) and/or norepinephrine transporter (NET), with clinically dominant off-target blockade at muscarinic M1, histamine H1, alpha-1 adrenergic receptors, and cardiac fast voltage-gated sodium channels.[7] Heterocyclic and related agents (maprotiline, mianserin, trazodone, nefazodone) share historical antidepressant use with different receptor and toxicity profiles; mirtazapine is often taught adjacent but is covered in detail in the multimodal topic.
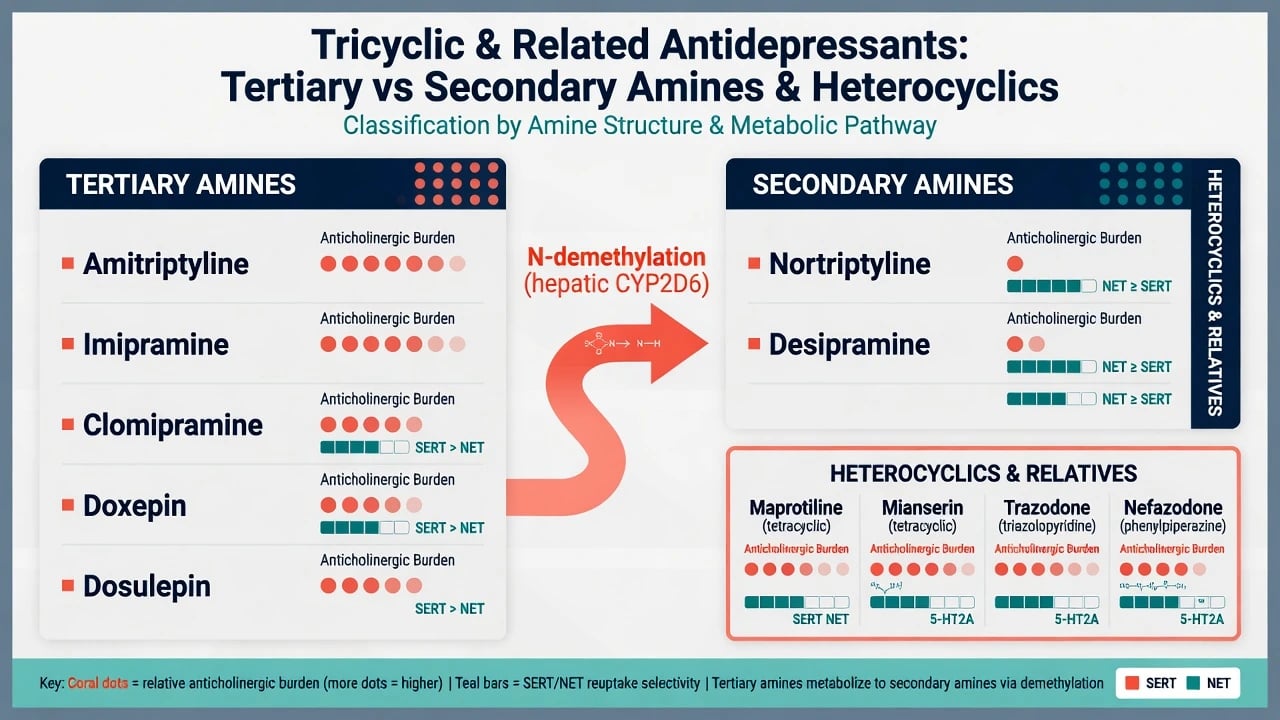
Tertiary amines (amitriptyline, imipramine, clomipramine, doxepin, dosulepin/dothiepin, trimipramine) generally carry heavier anticholinergic/sedative burdens and more serotonergic activity (especially clomipramine). Secondary amines (nortriptyline, desipramine, protriptyline) are demethylated metabolites of tertiary parents, typically more noradrenergic and somewhat better tolerated in older adults when a TCA is still chosen.[2][13]
Epidemiology and fatal toxicity context
TCAs dominated depression treatment for decades, then receded as first-line agents once SSRIs and related drugs offered comparable class-level efficacy with far lower overdose lethality and better acceptability for many patients.[1][2] Relative mortality and fatal toxicity index analyses repeatedly place classical TCAs — particularly amitriptyline and dosulepin/dothiepin — among the most lethal antidepressants per prescription unit.[8][9][10] Comparative toxicology series also show TCAs produce more coma and cardiotoxicity than SSRIs in overdose, which is exactly why means restriction is part of prescribing, not an optional social afterthought.[14]
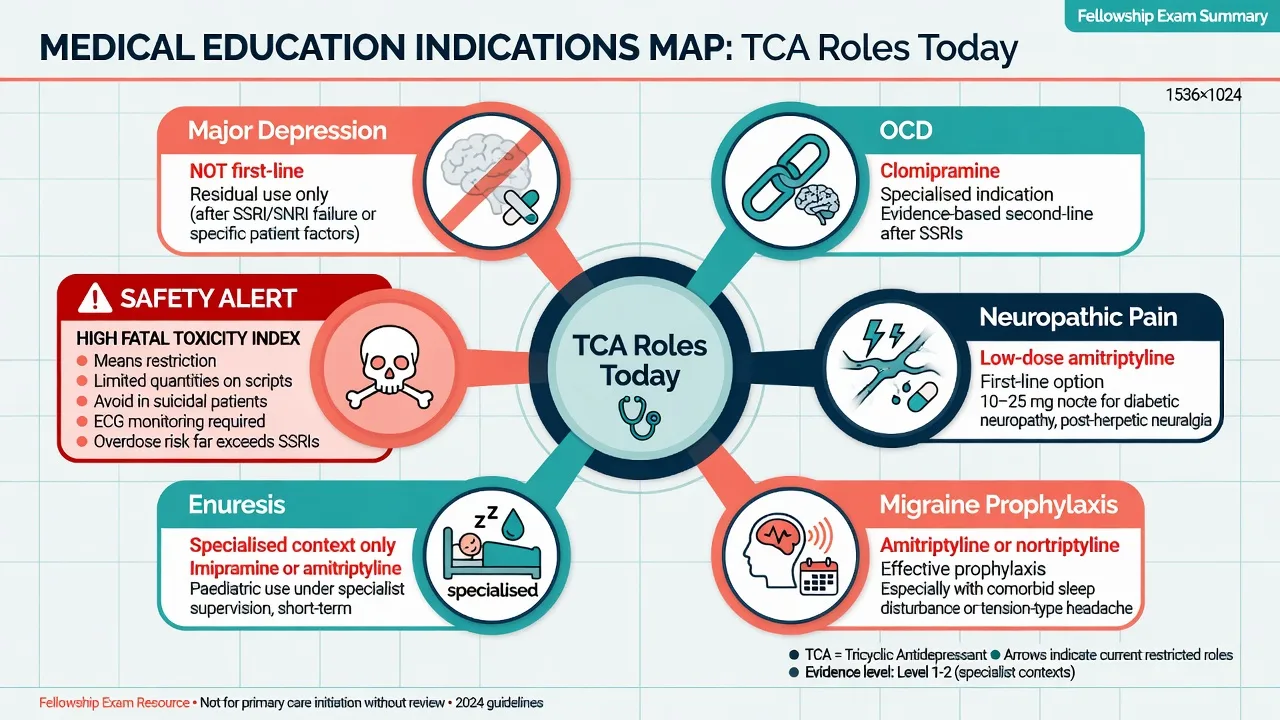
Who still receives them: residual treatment-resistant or melancholic pathways, OCD (clomipramine), neuropathic pain and migraine prophylaxis at often sub-antidepressant doses, enuresis in specialised paediatric contexts, and legacy community scripts that need active review.[15][16][8]
Pathophysiology — therapeutic action and toxicity
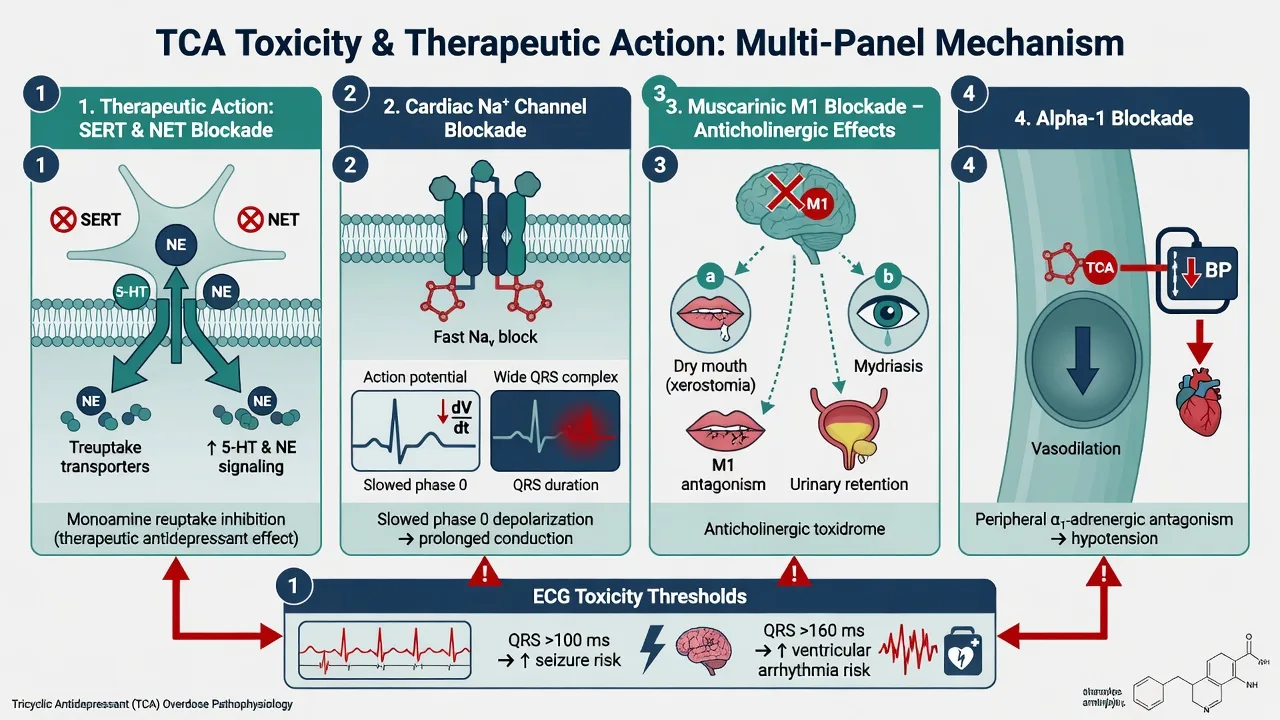
Therapeutic: SERT/NET inhibition initiates adaptive monoaminergic cascades with delayed clinical antidepressant response over weeks, not hours.[1] Off-target H1 blockade drives sedation and appetite; M1 drives the dry-mouth/constipation/blurred-vision package; alpha-1 drives orthostasis.
Toxic (exam core): Cardiac fast Na-channel blockade slows phase-0 depolarisation → QRS widening, rightward terminal forces (tall R in aVR), risk of ventricular arrhythmia, hypotension and seizures.[3][4][7] Anticholinergic features produce the classic toxidrome (tachycardia, dry flushed skin, mydriasis, ileus, urinary retention, delirium). Alpha-1 blockade worsens vasodilatory shock. Clomipramine adds higher serotonergic load and serotonin toxicity potential when combined with other serotonergic drugs.
Indications — residual but real
Major depressive disorder
Modern RANZCP and CANMAT guidance place SSRIs/SNRIs and other better-tolerated agents ahead of TCAs for most first-line outpatient MDD; TCAs remain efficacious options later in stepped care or when prior response and monitoring capacity justify them.[16][17][18] Cipriani network meta-analysis found amitriptyline among the more efficacious acute treatments, with acceptability trade-offs that match clinical experience of drop-outs from anticholinergic and sedative effects.[1] Anderson meta-analysis: overall SSRI vs TCA efficacy similar, with signals favouring some TCAs in inpatients and for amitriptyline comparisons, but SSRIs better tolerated.[2] Relapse prevention principles for antidepressants generally apply once remission is achieved.[20]
OCD — clomipramine niche
Clomipramine is the classic TCA with the strongest OCD evidence among tricyclics; meta-analysis of serotonin transport inhibitors showed all active agents beat placebo, with clomipramine more effective than the SSRIs compared in that era's synthesis — modern practice still often starts SSRIs for tolerability, then escalates to clomipramine or combination strategies under specialist care.[15]
Pain, migraine, other
Low-dose amitriptyline (commonly 10–75 mg oral at night for neuropathic pain teaching ranges) is used for pain and migraine prophylaxis; these doses are not interchangeable with full antidepressant titration and still carry overdose and anticholinergic risk.[16] Nocturnal enuresis is a historical imipramine niche now largely displaced by safer first-line options outside specialist pathways.
Heterocyclics — indication and hazard notes
- Maprotiline: NET-leaning tetracyclic; higher seizure risk teaching point.[7][14]
- Mianserin: alpha-2/5-HT2 related; less classic cardiotoxicity than TCAs in teaching contrasts; blood dyscrasia historical caution.[14]
- Trazodone: 5-HT2A/alpha-1; used as sleep adjunct; counsel priapism.[14]
- Nefazodone: hepatotoxicity risk — avoid when safer options exist.[16]
Clinical presentation on treatment
Expect delayed mood benefit, early sedation (tertiary more than secondary), dry mouth, constipation, blurred vision, orthostatic dizziness, sexual dysfunction and weight gain.[2] Activation or early suicide-risk window still requires same-day review standards as for other antidepressants. Missed bipolar spectrum presents as switch into mania if the TCA is used as if unipolar depression were certain.[16][10]
Differential traps
Anticholinergic delirium is not "worsening depression." Wide-complex tachycardia is not "anxiety tachycardia." Serotonin toxicity (hyperreflexia, clonus, hyperthermia) must be separated from anticholinergic toxidrome and from NMS. Other Na-channel blockers (flecainide, carbamazepine, diphenhydramine) can mimic TCA ECG patterns.[5][7]
Assessment before and during prescribing
Pre-start checklist: MSE and suicide risk with means access (existing tablets at home), bipolar screen, cardiac history and baseline ECG, falls risk, constipation/BPH/glaucoma history, pregnancy potential, full medication review (CYP2D6 inhibitors, other anticholinergics, QT-prolonging agents).[13][16]
On treatment: orthostatic BP, anticholinergic symptom review, weight, sexual function, mood rating scales, adherence, and deliberate discussion of what to do if mood or self-harm risk escalates.[13][16]
Investigations and therapeutic drug monitoring (levels)
Baseline and safety labs/ECG
Obtain baseline ECG (QRS duration, QTc, conduction blocks), U&E, and other tests guided by comorbidity. Repeat ECG if dose escalates substantially, interacting drugs are added, or cardiac symptoms appear.[13]
Plasma levels — when and what they mean
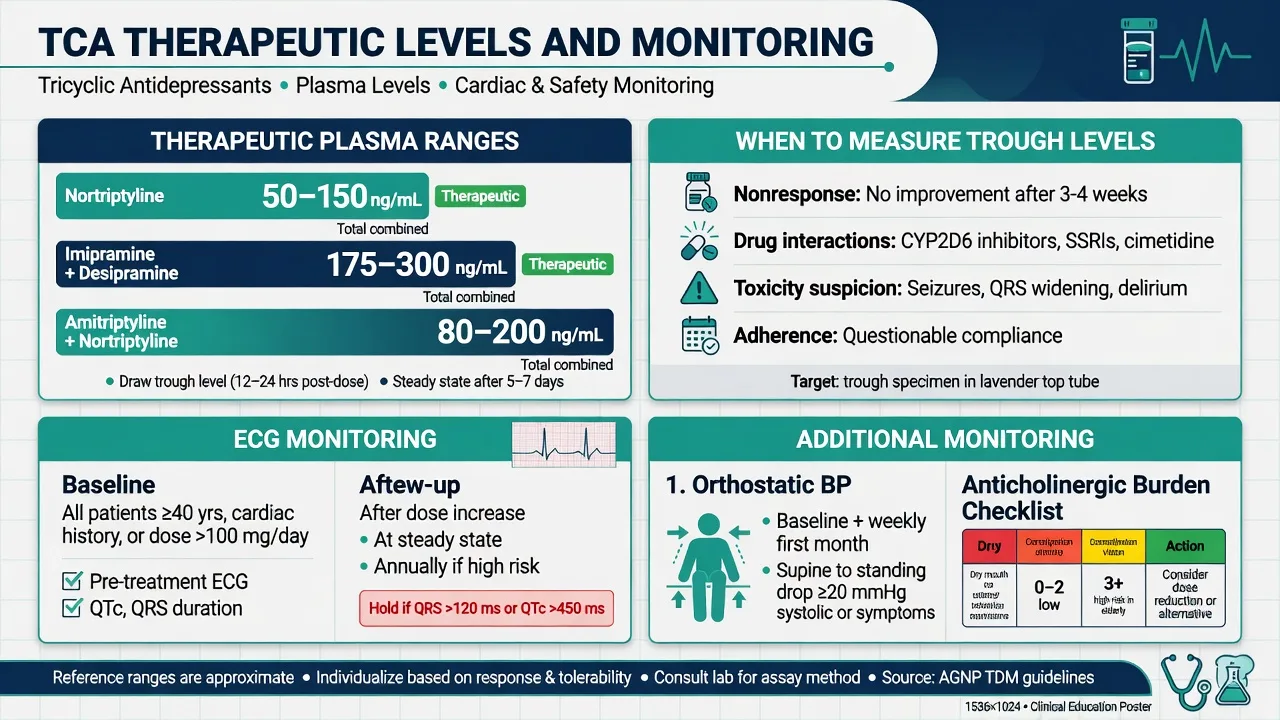
Unlike most SSRIs, classic TCAs have concentration–response data and AGNP-level recommendation for therapeutic drug monitoring.[11][12][13] Measure trough concentrations at steady state (typically after about five half-lives on a stable dose; many TCAs about 1 week, agent-dependent).[13]
Teaching reference bands (confirm local lab units — ng/mL vs µg/L are numerically equal): Nortriptyline ~50–150 ng/mL; imipramine + desipramine ~175–300 ng/mL; amitriptyline + nortriptyline ~80–200 ng/mL (lab-specific); clomipramine + desmethylclomipramine lab-specific (monitor parent and metabolite). These ranges are AGNP- and classic TDM teaching scaffolds and must be interpreted with the local laboratory method.[11][13]
Perry and colleagues estimated that response rates are substantially higher inside published therapeutic ranges than outside them — levels are a tool for non-response, adherence, interactions and toxicity, not a vanity number.[11] Glassman's imipramine work helped establish that plasma concentration relates to clinical outcome and that fixed milligram doses produce wide interindividual levels.[12] Hiemke AGNP 2017 consensus codifies recommended ranges, laboratory alert levels and recommendation grades for neuropsychopharmacology TDM, with TCAs among agents where monitoring is strongly supported.[13]
Critical exam contrast: in acute overdose, serial ECG (not waiting for a TCA plasma level) drives bicarb decisions; Boehnert showed QRS duration outperforms serum drug level for predicting seizures and ventricular arrhythmias.[3]
Acute management — overdose resuscitation
TCA overdose remains a high-lethality medical emergency defined by Na-channel cardiotoxicity, anticholinergic and CNS toxicity.[5][7]
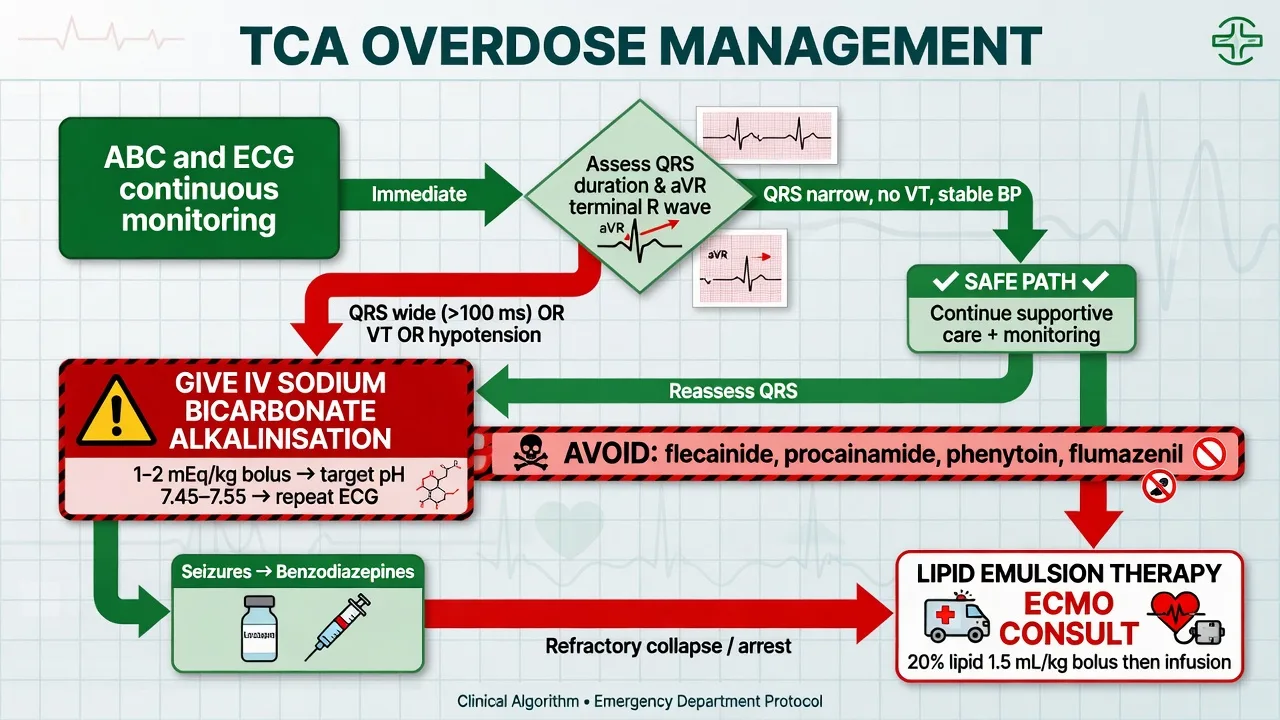
Immediate: ABC with early airway protection if coma or seizure risk, IV access, continuous cardiac monitoring, capillary glucose, temperature, serial ECGs, discuss early with toxicology/ED/ICU.[5][19]
ECG risk thresholds (classic teaching): QRS greater than 100 ms — increased seizure risk; QRS greater than 160 ms — high ventricular arrhythmia risk; terminal R in aVR of 3 mm or more (or elevated R/S in aVR) — additional marker of Na-channel toxicity. These thresholds come from Boehnert and Liebelt and remain viva staples.[3][4]
Sodium bicarbonate is the specific intervention for wide-complex cardiotoxicity, ventricular arrhythmia or refractory hypotension: hypertonic sodium load plus alkalinisation reduces Na-channel blockade; aim clinically for QRS narrowing and controlled alkalinisation (commonly taught target pH around 7.45–7.55, avoiding extreme alkalosis).[5][6] Seizures: benzodiazepines. Avoid class Ia/Ic antiarrhythmics, avoid relying on phenytoin for TCA arrhythmia, and avoid flumazenil in mixed overdoses that may unmask seizures.[5][7] Refractory cardiovascular collapse: involve ICU/toxicology for lipid emulsion and advanced support pathways consistent with contemporary poisoning guidance.[19]
Disposition follows local protocol (GEMNet-style observation logic: prolonged monitoring if any ECG abnormality or significant ingestion; do not discharge on a normal single snapshot after large deliberate self-harm).[5]
Definitive management — doses, titration, switching
Adult oral dose scaffolds (always individualise; start low in elderly)
| Drug | Typical adult oral range (depression context) | Notes |
|---|---|---|
| Amitriptyline | Start 25–50 mg at night; titrate toward 75–150 mg/day (max often 150–200 mg/day supervised) | Pain doses often 10–75 mg |
| Nortriptyline | Start 10–25 mg; usual 50–100 mg/day; max often 150 mg/day | Best TDM scaffolding among common TCAs |
| Imipramine | Start 25 mg; usual 75–150 mg/day | Parent + desipramine levels |
| Clomipramine | Start 25 mg; OCD often needs higher gradual titration toward 100–250 mg/day specialist ranges | ECG and seizure risk awareness |
| Dosulepin | Avoid new starts when alternatives exist | High FTI |
| Individualise all of the above adult oral scaffolds; efficacy exists but tolerability and lethality constrain use.[1][2][8][9][13][16] |
Adequate trial: therapeutic dose (level-guided when available) for about 4–6 weeks with adherence checked before declaring failure.[11][16]
Switching: cross-taper with ECG and side-effect vigilance. Never combine with irreversible MAOIs; respect prolonged washouts (classically about 2 weeks after most TCAs before MAOI; longer after agents with long-lived active metabolites as per product information). Adding fluoxetine, paroxetine or bupropion can spike TCA levels via CYP2D6 inhibition — reduce dose and re-level.[13]
Means restriction: small quantities, blister packs, carer administration, lock-box, and document lethality counselling whenever suicide risk is material.[10]
Subtypes and clinical scenarios
- Inpatient melancholic depression: historical TCA strength; still not automatic if safer intensive options (including ECT pathways) fit better.[2]
- OCD: clomipramine after or alongside SSRI strategy.[15]
- Neuropathic pain / migraine: low-dose amitriptyline; separate consent for off-target risks.[16]
- Legacy dosulepin review: switch unless clear ongoing benefit and risk is tightly managed.[8][9]
- Trazodone sleep adjunct: counsel priapism; do not assume "safe TCA alternative" without reviewing hypotension and interactions.[14]
Complications and pitfalls
Cardiotoxicity in overdose; therapeutic-dose conduction risk in vulnerable hearts; anticholinergic delirium and urinary retention; severe constipation; orthostatic falls; seizures (maprotiline and overdose); CYP2D6-mediated level spikes; additive anticholinergic or QT polypharmacy; serotonin toxicity with serotonergic combinations (clomipramine high risk).[7][13][14]
Prognosis and disposition
Therapeutic prognosis tracks depression severity, adherence, comorbidity and whether a true therapeutic level was reached.[11][20] Overdose prognosis is ECG- and physiology-guided; early bicarb and airway care change outcomes.[5][6] Stop or switch TCAs when high suicide risk meets free access to a lethal tablet supply, when significant conduction disease appears, or when safer agents can deliver the same goal.[9][10][16]
Special populations
Older adults: prefer secondary amines if a TCA is unavoidable; start very low (for example nortriptyline 10 mg oral); prioritise falls, cognition, constipation and drug interactions.[13][16] Youth: generally not first-line; overdose lethality is decisive.[9][10] Pregnancy/lactation: individualised perinatal psychiatry decision — do not default to TCA nostalgia.[16] Cardiac disease, narrow-angle glaucoma, significant BPH, dementia: relative contraindications or intensified monitoring.[7][13] Hepatic disease: lower doses; avoid nefazodone.[13][16]
Evidence, guidelines and regional deltas
| Source | Fellowship take-home |
|---|---|
| Cipriani 2018 NMA | Amitriptyline efficacious; acceptability trade-off[1] |
| Anderson 2000 | SSRI ≈ TCA efficacy overall; SSRIs better tolerated[2] |
| Boehnert / Liebelt / GEMNet / Bradberry | QRS/aVR and bicarbonate dominate OD care[3][4][5][6] |
| Henry / Buckley / Hawton / Whyte | TCAs high relative lethality in overdose[8][9][10][14] |
| Perry / Glassman / Hiemke AGNP | Levels matter for therapeutic use[11][12][13] |
| Greist 1995 | Clomipramine strong OCD signal among SERT inhibitors of that era[15] |
| RANZCP 2020 / CANMAT 2016–2023 | TCAs not routine first-line MDD; residual and specialist roles[16][17][18] |
| AHA 2023 poisoning update | Life-threatening Na-channel toxicity pathways including advanced support concepts[19] |
ANZ delta: active review of high-FTI agents (dosulepin), small-quantity dispensing under high risk, and toxicology/ED partnership for OD. NICE/APA-aligned teaching: prefer safer first-line antidepressants for uncomplicated MDD; reserve TCAs with monitoring capacity.[8][9][16][5]
Exam pearls
References
- [1]Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis Lancet, 2018.PMID 29477251
- [2]Anderson IM Selective serotonin reuptake inhibitors versus tricyclic antidepressants: a meta-analysis of efficacy and tolerability J Affect Disord, 2000.PMID 10760555
- [3]Boehnert MT, Lovejoy FH Jr Value of the QRS duration versus the serum drug level in predicting seizures and ventricular arrhythmias after an acute overdose of tricyclic antidepressants N Engl J Med, 1985.PMID 4022081
- [4]Liebelt EL, Francis PD, Woolf AD ECG lead aVR versus QRS interval in predicting seizures and arrhythmias in acute tricyclic antidepressant toxicity Ann Emerg Med, 1995.PMID 7618783
- [5]Body R, Bartram T, Azam F, Mackway-Jones K Guidelines in Emergency Medicine Network (GEMNet): guideline for the management of tricyclic antidepressant overdose Emerg Med J, 2011.PMID 21436332
- [6]Bradberry SM, Thanacoody HK, Watt BE, Thomas SH, Vale JA Management of the cardiovascular complications of tricyclic antidepressant poisoning: role of sodium bicarbonate Toxicol Rev, 2005.PMID 16390221
- [7]Kerr GW, McGuffie AC, Wilkie S Tricyclic antidepressant overdose: a review Emerg Med J, 2001.PMID 11435353
- [8]Buckley NA, McManus PR Fatal toxicity of serotoninergic and other antidepressant drugs: analysis of United Kingdom mortality data BMJ, 2002.PMID 12468481
- [9]Henry JA, Alexander CA, Sener EK Relative mortality from overdose of antidepressants BMJ, 1995.PMID 7866123
- [10]Hawton K, Bergen H, Simkin S, et al. Toxicity of antidepressants: rates of suicide relative to prescribing and non-fatal overdose Br J Psychiatry, 2010.PMID 20435959
- [11]Perry PJ, Zeilmann C, Arndt S Tricyclic antidepressant concentrations in plasma: an estimate of their sensitivity and specificity as a predictor of response J Clin Psychopharmacol, 1994.PMID 7962678
- [12]Glassman AH, Perel JM, Shostak M, et al. Clinical implications of imipramine plasma levels for depressive illness Arch Gen Psychiatry, 1977.PMID 843179
- [13]Hiemke C, Bergemann N, Clement HW, et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017 Pharmacopsychiatry, 2018.PMID 28910830
- [14]Whyte IM, Dawson AH, Buckley NA Relative toxicity of venlafaxine and selective serotonin reuptake inhibitors in overdose compared to tricyclic antidepressants QJM, 2003.PMID 12702786
- [15]Greist JH, Jefferson JW, Kobak KA, et al. Efficacy and tolerability of serotonin transport inhibitors in obsessive-compulsive disorder. A meta-analysis Arch Gen Psychiatry, 1995.PMID 7811162
- [16]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [17]Kennedy SH, Lam RW, McIntyre RS, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments Can J Psychiatry, 2016.PMID 27486148
- [18]Lam RW, Kennedy SH, Adams C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder Can J Psychiatry, 2024.PMID 38711351
- [19]Lavonas EJ, Akpunonu PD, Arens AM, et al. 2023 American Heart Association Focused Update on the Management of Patients With Cardiac Arrest or Life-Threatening Toxicity Due to Poisoning Circulation, 2023.PMID 37721023
- [20]Geddes JR, Carney SM, Davies C, et al. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review Lancet, 2003.PMID 12606176