Psych · Psychopharmacology — rTMS, VNS and DBS
rTMS, VNS and deep brain stimulation
Also known as repetitive transcranial magnetic stimulation · rTMS · iTBS · theta burst stimulation · vagus nerve stimulation · VNS · deep brain stimulation depression · subcallosal cingulate DBS · SAINT · SNT · neurostimulation psychiatry
Exam-exhaustive fellowship reference on rTMS/iTBS, implanted vagus nerve stimulation, and deep brain stimulation for treatment-resistant depression — protocols, safety, landmark trials (O'Reardon, George, THREE-D, SAINT/SNT, Rush VNS, Mayberg/Holtzheimer/Dougherty DBS), evidence ladder versus ECT, and regional access. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Device-based neurostimulation sits beside ECT and rapid-acting pharmacology on the treatment-resistant depression (TRD) ladder. Fellowship examiners test indication discipline, protocol literacy, honest trial reading (especially negative or delayed signals), and safety screening — not device brand names or local funding codes as universal law.[9][12]
Definition and place in care
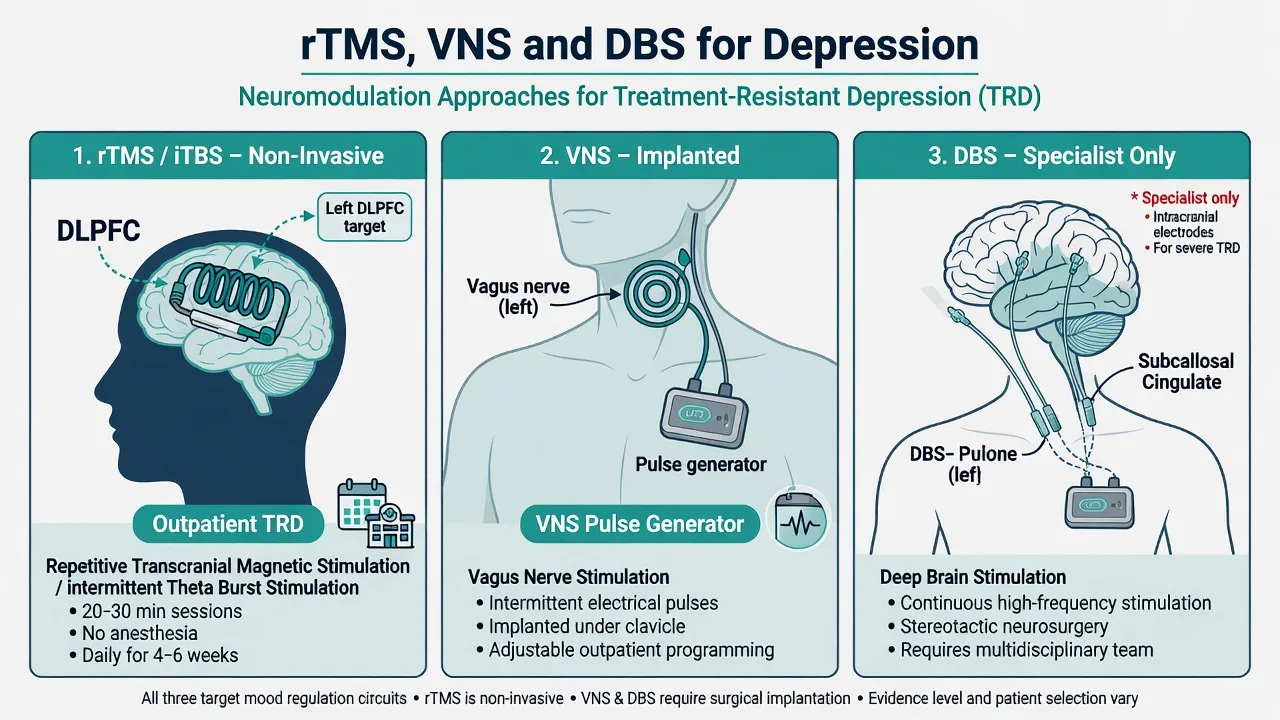
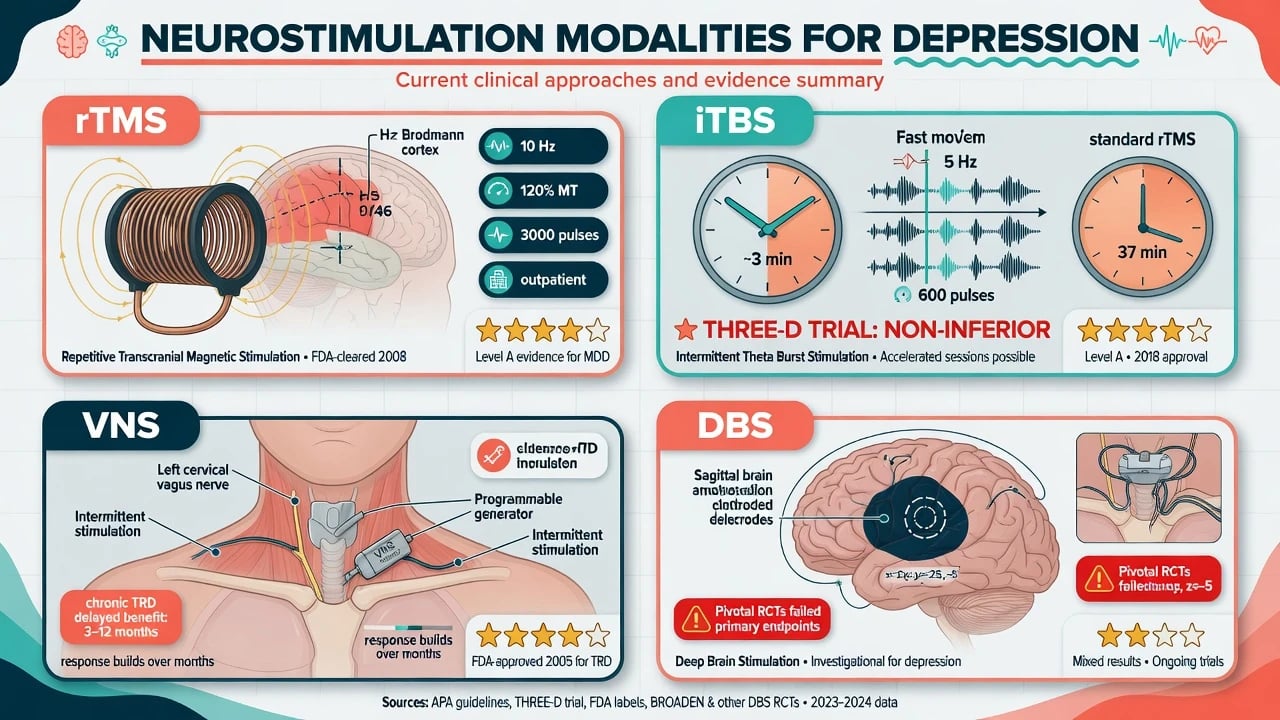
Repetitive transcranial magnetic stimulation (rTMS) delivers pulsed magnetic fields through a scalp coil to induce focal cortical currents without anaesthesia or seizure (contrast with ECT). Common antidepressant teaching target is the left dorsolateral prefrontal cortex (DLPFC). Intermittent theta-burst stimulation (iTBS) is a patterned rTMS protocol delivering bursts that markedly shorten session length while matching efficacy of standard high-frequency rTMS in a large non-inferiority trial.[1][2][6]
Vagus nerve stimulation (VNS) for depression uses a surgically implanted pulse generator (typically left chest) with a lead to the left cervical vagus nerve, delivering intermittent electrical pulses as a chronic adjunct to ongoing treatments.[13][14]
Deep brain stimulation (DBS) places stereotactic intracranial electrodes (examples in depression research: subcallosal cingulate / Brodmann area 25 white matter, ventral capsule/ventral striatum (VC/VS)) connected to an implanted generator. For depression this remains specialist/research-tier, not a routine community step after two failed antidepressants.[16][17][18]
Classification and evidence ladder
| Modality | Invasiveness | Typical role | Exam one-liner on evidence |
|---|---|---|---|
| rTMS / iTBS | Non-invasive | Outpatient TRD after failed ADs | Sham RCTs positive (O'Reardon, George); iTBS non-inferior (THREE-D) |
| ECT | Anaesthetised seizure | Severe, psychotic, catatonic, urgent | Highest acute efficacy for severe depression — separate topic depth |
| VNS | Peripheral implant | Chronic multi-year TRD | Acute sham primary failed; longer-term comparative data friendlier |
| DBS | Intracranial implant | Ultra-refractory research centres | Open-label hope; pivotal SCC and VC/VS RCTs failed primary endpoints |
The ladder above compresses the exam hierarchy: rTMS/iTBS outpatient sham-RCT support, ECT for high-acuity syndromes, VNS for chronic multi-failure TRD with delayed benefit, and DBS as specialist/research after negative pivotal primary endpoints.[1][6][12][13][17][18]
CANMAT neurostimulation guidance situates rTMS as an evidence-based option in stepped care for MDD, with other devices tiered by evidence and practicality.[12] Lefaucheur evidence-based rTMS guidelines (2014 and 2020 update) grade therapeutic recommendations by indication and protocol class.[4][5]
Epidemiology and clinical need
TRD drives disproportionate disability, rehospitalisation, and suicide risk. Device therapies matter for people who remain ill after adequate medication and psychological trials, or who cannot tolerate further pharmacotherapy. Meta-analysis of high-frequency rTMS sham RCTs shows clinically relevant response and remission advantages over sham with relatively low drop-out, supporting outpatient programmes when access exists.[3]
Implant rates for VNS/DBS depression are far lower than rTMS course numbers: candidacy, surgical risk, cost, and evidence nuance constrain use. Aaronson five-year observational comparative data illustrate why long-horizon outcomes (response, remission, suicidality measures) dominate VNS discussions more than the 10-week acute RCT snapshot.[15]
Pathophysiology and mechanisms
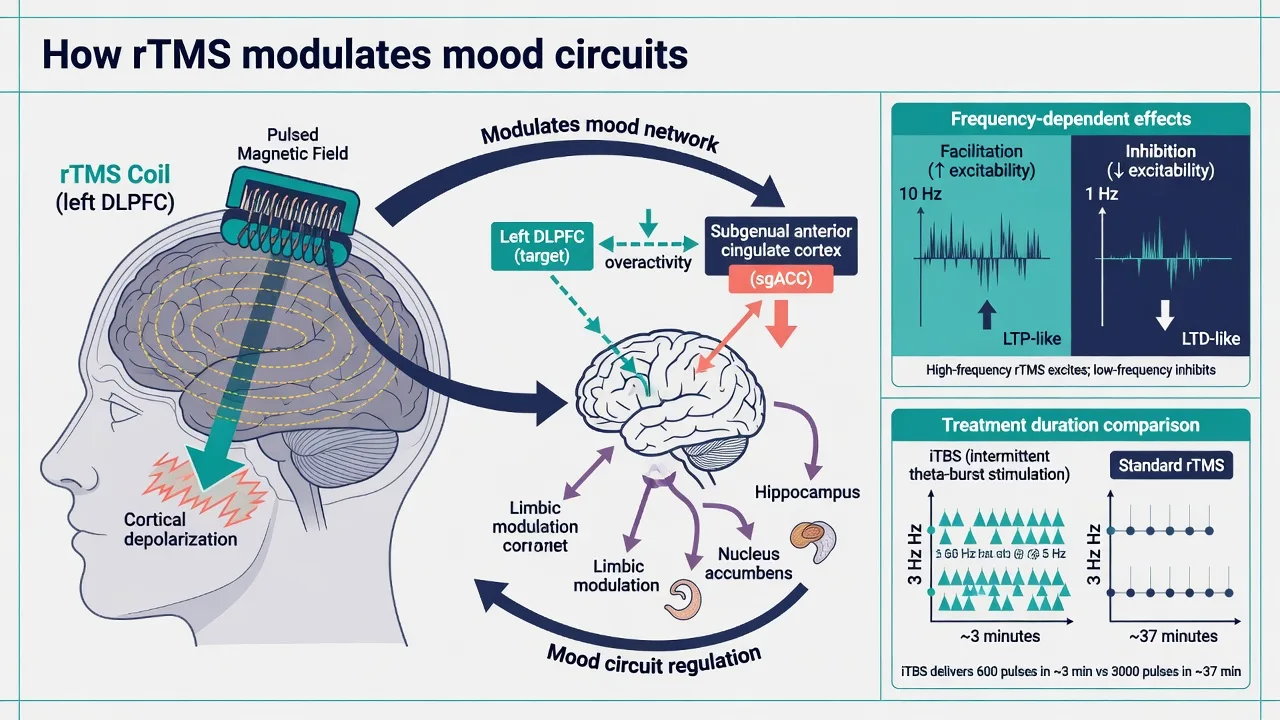
rTMS teaching model. Rapid magnetic flux induces electrical current in superficial cortex under the coil. High-frequency protocols over left DLPFC are framed as facilitatory; low-frequency right DLPFC as inhibitory — a useful viva scaffold linked to prefrontal asymmetry hypotheses, acknowledging individual variability.[4][5] Network effects extend beyond the stimulation site, including connectivity with subgenual anterior cingulate circuitry relevant to depression. Connectivity-guided targeting (DLPFC site most anticorrelated with sgACC) underpins accelerated intelligent protocols (SAINT/SNT).[7][8]
iTBS delivers triplets of pulses at gamma-like frequencies nested in theta-like rhythms (classic teaching: 50 Hz bursts repeated at 5 Hz), achieving therapeutic pulse counts in roughly 3 minutes versus half-hour-plus standard 10 Hz sessions in THREE-D.[6]
VNS engages ascending vagal afferents to nucleus tractus solitarius and widespread brainstem–limbic–cortical modulation; clinical benefit in TRD often accrues over months, matching a plasticity/network re-equilibration story rather than a same-day monoamine boost.[14][15]
DBS delivers continuous (or programmed) high-frequency stimulation to white-matter or grey targets to modulate dysfunctional mood networks. Mayberg open-label subcallosal cingulate work catalysed the field; subsequent controlled trials force humility about target, trial design, and placebo/expectation in device research.[16][17]
Clinical assessment before stimulation
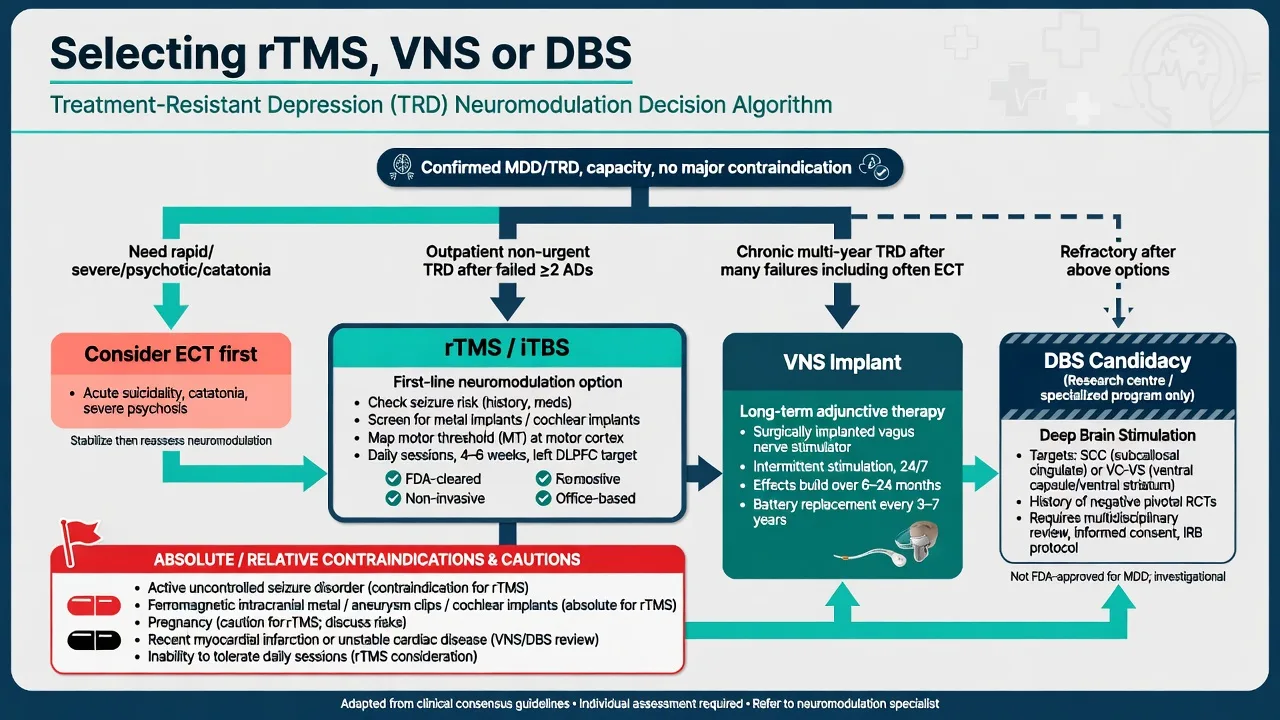
Confirm MDD/TRD diagnosis, document adequate failed antidepressant trials (dose, duration, adherence), and exclude pseudo-resistance (bipolar spectrum, substances, organic depression, non-adherence). Screen for psychosis, catatonia, and acute risk that would re-route to ECT or hospital care.[9][12]
rTMS safety screen (exam essentials). History of epilepsy/seizures, intracranial ferromagnetic implants, cochlear implants, recent stroke in target territory, pregnancy, substance withdrawal (seizure risk), and medications that substantially lower seizure threshold. Determine resting motor threshold (MT) and map the target (Beam F3 methods or neuronavigation). Hearing protection is standard. Rossi consensus guidelines (2009 and 2021 update) frame screening, parameter safety, operator training, and rare seizure management.[9][10][11]
VNS/DBS pre-surgical assessment. Multidisciplinary psychiatric stability and realistic goals, surgical fitness, imaging for stereotaxy (DBS), discussion of irreversible surgical risk, device MRI-conditional rules, and capacity/consent (or substitute decision-making under local law).[15][17]
rTMS and iTBS protocols
Landmark efficacy. O'Reardon multisite RCT established antidepressant benefit of daily left prefrontal rTMS versus sham in medication-free MDD with prior failure, underpinning early regulatory clearances.[1] George and colleagues' OPT-TMS NIMH-sponsored sham-controlled trial reinforced daily left prefrontal rTMS efficacy and safety messaging for major depression.[2]
iTBS (THREE-D). Blumberger randomised 10 Hz rTMS versus iTBS to left DLPFC: iTBS was non-inferior on depression symptom reduction, with similar tolerability — transforming clinic throughput (session minutes, not efficacy class).[6]
Accelerated protocols (SAINT/SNT). Cole open-label Stanford Accelerated Intelligent Neuromodulation Therapy reported high remission rates after an intensive multi-session/day iTBS schedule with functional connectivity-guided targeting.[7] The subsequent double-blind sham-controlled SNT trial supported superiority of active accelerated therapy over sham in TRD — powerful but specialist, resource-intensive, and not yet the default community protocol everywhere.[8]
Adverse effects. Common: scalp pain, headache, facial muscle twitching, transient discomfort. Serious but uncommon: seizure. McClintock consensus recommendations cover practical application standards for depression rTMS programmes.[9][10]
Vagus nerve stimulation
Procedure. Surgical implant of generator and left cervical vagus lead under anaesthetic; outpatient parameter titration follows (output current, pulse width, frequency, on/off duty cycle) while continuing psychotropics and psychosocial care.[13][14]
Evidence nuance (exam gold). Rush acute-phase randomised controlled trial of adjunctive VNS versus sham over about 10 weeks did not show a significant difference on the primary HRSD response endpoint (active about 15 percent vs sham about 10 percent), though a secondary self-report measure favoured active stimulation — know this honest reading.[13] Twelve-month naturalistic follow-up suggested growing benefit and acceptable tolerability over longer horizons.[14] Aaronson five-year observational comparison of VNS versus treatment-as-usual in TRD reported advantages in response, remission, and suicidality-related outcomes — compelling for chronic TRD counselling, still not a substitute for acute RCT perfection.[15]
Adverse effects. Voice alteration/hoarseness, cough, paraesthesia, dyspnoea during on-time, surgical infection, lead fracture, need for battery replacement. Counsel delayed onset of benefit (often months).[14][15]
Deep brain stimulation
Open-label catalyst. Mayberg and colleagues reported striking improvement in highly refractory depression with bilateral subcallosal cingulate white-matter DBS, launching modern psychiatric DBS research.[16]
Pivotal humility. Holtzheimer multisite randomised sham-controlled trial of subcallosal cingulate DBS for TRD failed its primary efficacy endpoint — essential viva fact countering pure open-label enthusiasm.[17] Dougherty randomised sham-controlled trial of VC/VS DBS for chronic TRD likewise found no significant difference in response rates in the blinded phase.[18]
Exam stance: DBS for depression is not a routine third-line tablet replacement. Offer only via centres of excellence/research protocols, with consent that explicitly includes negative pivotal data, surgical risks (haemorrhage, infection, hardware failure), and possible stimulation-related psychiatric effects (mood elevation, impulsivity depending on target/parameters).[17][18]
Acute problems and definitive management algorithm
Peri-rTMS seizure. Stop stimulation immediately; protect airway and safety; supportive care; medical evaluation; document parameters; revise risk–benefit before any future session. Do not complete remaining trains the same day after a clinical seizure.[10][11]
Definitive sequencing (teaching scaffold).
- Confirm diagnosis and true resistance; optimise meds and evidence-based psychotherapy access.[12]
- If severe/urgent/psychotic/catatonic → ECT discussion early.[12]
- If outpatient TRD, able to attend daily sessions, no major contraindications → rTMS/iTBS course with MT-based dosing.[1][6][9]
- If multi-year ultra-chronic TRD after many modalities (often including ECT courses) → VNS candidacy discussion with delayed-benefit consent.[15]
- If still refractory and motivated for research neurosurgery → DBS centre evaluation with full negative-RCT disclosure.[17][18]
Continue suicide risk management, social supports, and pharmacotherapy throughout — devices are not a licence to abandon formulation and risk planning.[9][12]
Subtypes and special scenarios
Bipolar depression. Limited evidence relative to unipolar TRD; switch risk and protocol heterogeneity — specialist only, careful mood-stabiliser coverage.[9]
OCD and other indications. Separate device clearances and protocols (including some deep TMS programmes) exist; do not import depression parameters blindly into OCD stems without stating indication shift.[5]
Maintenance. After rTMS response, individualised booster/maintenance sessions plus continued AD therapy reduce relapse risk for some patients — plan disposition at course start, not at discharge day only.[9]
Complications and pitfalls
| Domain | Complications | Exam pitfall |
|---|---|---|
| rTMS | Headache, pain, rare seizure | Skipping MT and metal screen |
| VNS | Hoarseness, infection, delayed benefit | Quoting only open-label while ignoring acute sham primary failure |
| DBS | Surgical/neuropsychiatric AEs | Presenting DBS as proven routine after Holtzheimer/Dougherty |
| System | Access inequity | Promising timelines you cannot deliver |
Common rTMS adverse effects are mostly local and transient, with seizure uncommon under standard parameters; VNS adds surgical and voice-related risks; DBS adds intracranial surgical risk — and overselling any implant without citing negative controlled data is the classic exam fail.[9][10][13][17][18]
Prognosis and disposition
rTMS responders often need ongoing pharmacotherapy and sometimes maintenance stimulation; non-responders should be re-formulated toward ECT, ketamine-class pathways, or further augmentation rather than endless identical courses without strategy change.[3][9][12] VNS and DBS demand long-term device clinic follow-up, battery/hardware surveillance, and psychiatric co-management.[15][17]
Special populations
Older adults. rTMS is used; cognitive burden often lower than ECT in shared decisions — still individualise vascular risk and logistics of daily attendance.[9][12]
Youth. Largely outside standard adult depression device pathways; specialist/research frameworks only — do not import adult rTMS parameters as free-standing community paediatric practice without local governance.[9][12]
Pregnancy and lactation. Prefer specialist perinatal psychiatry; for severe perinatal TRD, ECT frequently remains the somatic treatment with the deepest clinical tradition — do not default to experimental implants.[12]
Implanted electronic devices. Compatibility is device- and protocol-specific; never assume "all metals are fine" or "all implants forbid all TMS."[10][11]
Evidence, guidelines and regional deltas
ANZ: rTMS services expanding but access and public funding vary by jurisdiction; VNS/DBS depression pathways are highly selective. Pair device discussions with RANZCP-aligned overall depression and ECT professional practice context rather than inventing universal Medicare item rules in viva answers.[12] UK: NICE technology appraisals and local commissioning shape TMS access; implant therapies tightly controlled.[12] USA: Multiple FDA clearances for rTMS systems and iTBS protocols; VNS has a depression regulatory history; DBS depression remains constrained relative to movement-disorder indications.[1][6][13][17] Canada: CANMAT Section 4 remains a high-yield structured neurostimulation syllabus for exams.[12]
Named trials/guidelines to carry: O'Reardon 2007; George 2010; Berlim 2014; Lefaucheur 2014/2020; THREE-D 2018; SAINT 2020 / SNT 2022; McClintock 2018; Rossi safety 2009/2021; CANMAT 2016; Rush VNS 2005 acute and 12-month; Aaronson 2017; Mayberg 2005; Holtzheimer 2017; Dougherty 2015.[1][2][3][6][8][13][15][17][18]
Exam pearls
References
- [1]O'Reardon JP, Solvason HB, Janicak PG, et al. Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: a multisite randomized controlled trial Biol Psychiatry, 2007.PMID 17573044
- [2]George MS, Lisanby SH, Avery D, et al. Daily left prefrontal transcranial magnetic stimulation therapy for major depressive disorder: a sham-controlled randomized trial Arch Gen Psychiatry, 2010.PMID 20439832
- [3]Berlim MT, van den Eynde F, Tovar-Perdomo S, et al. Response, remission and drop-out rates following high-frequency repetitive transcranial magnetic stimulation (rTMS) for treating major depression: a systematic review and meta-analysis of randomized, double-blind and sham-controlled trials Psychol Med, 2014.PMID 23507264
- [4]Lefaucheur JP, André-Obadia N, Antal A, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS) Clin Neurophysiol, 2014.PMID 25034472
- [5]Lefaucheur JP, Aleman A, Baeken C, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014-2018) Clin Neurophysiol, 2020.PMID 31901449
- [6]Blumberger DM, Vila-Rodriguez F, Thorpe KE, et al. Effectiveness of theta burst versus high-frequency repetitive transcranial magnetic stimulation in patients with depression (THREE-D): a randomised non-inferiority trial Lancet, 2018.PMID 29726344
- [7]Cole EJ, Stimpson KH, Bentzley BS, et al. Stanford Accelerated Intelligent Neuromodulation Therapy for Treatment-Resistant Depression Am J Psychiatry, 2020.PMID 32252538
- [8]Cole EJ, Phillips AL, Bentzley BS, et al. Stanford Neuromodulation Therapy (SNT): A Double-Blind Randomized Controlled Trial Am J Psychiatry, 2022.PMID 34711062
- [9]McClintock SM, Reti IM, Carpenter LL, et al. Consensus Recommendations for the Clinical Application of Repetitive Transcranial Magnetic Stimulation (rTMS) in the Treatment of Depression J Clin Psychiatry, 2018.PMID 28541649
- [10]Rossi S, Hallett M, Rossini PM, Pascual-Leone A; Safety of TMS Consensus Group Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research Clin Neurophysiol, 2009.PMID 19833552
- [11]Rossi S, Antal A, Bestmann S, et al. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines Clin Neurophysiol, 2021.PMID 33243615
- [12]Milev RV, Giacobbe P, Kennedy SH, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 4. Neurostimulation Treatments Can J Psychiatry, 2016.PMID 27486154
- [13]Rush AJ, Marangell LB, Sackeim HA, et al. Vagus nerve stimulation for treatment-resistant depression: a randomized, controlled acute phase trial Biol Psychiatry, 2005.PMID 16139580
- [14]Rush AJ, Sackeim HA, Marangell LB, et al. Effects of 12 months of vagus nerve stimulation in treatment-resistant depression: a naturalistic study Biol Psychiatry, 2005.PMID 16139581
- [15]Aaronson ST, Sears P, Ruvuna F, et al. A 5-Year Observational Study of Patients With Treatment-Resistant Depression Treated With Vagus Nerve Stimulation or Treatment as Usual: Comparison of Response, Remission, and Suicidality Am J Psychiatry, 2017.PMID 28359201
- [16]Mayberg HS, Lozano AM, Voon V, et al. Deep brain stimulation for treatment-resistant depression Neuron, 2005.PMID 15748841
- [17]Holtzheimer PE, Husain MM, Lisanby SH, et al. Subcallosal cingulate deep brain stimulation for treatment-resistant depression: a multisite, randomised, sham-controlled trial Lancet Psychiatry, 2017.PMID 28988904
- [18]Dougherty DD, Rezai AR, Carpenter LL, et al. A Randomized Sham-Controlled Trial of Deep Brain Stimulation of the Ventral Capsule/Ventral Striatum for Chronic Treatment-Resistant Depression Biol Psychiatry, 2015.PMID 25726497