Psych · Psychopharmacology — valproate
Valproate
Also known as Sodium valproate · Valproic acid · Divalproex · Depakote · Epilim · Semisodium valproate · VPA
Exam-exhaustive fellowship psychopharmacology of valproate/divalproex — acute mania and oral loading, trough levels, BALANCE maintenance limits versus lithium, pregnancy-prevention hierarchy (EURAP, NEAD, ASD risk), PCOS-like endocrine effects, hyperammonaemic encephalopathy, LFT/platelet monitoring, and lamotrigine interaction. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Valproate (valproic acid / sodium valproate / divalproex) is high-weight psychopharmacology across FRANZCP, MRCPsych and ABPN because examiners test pregnancy hierarchy, levels and loads, ammonia, reproductive endocrine effects, and trial literacy in one station. This leaf topic deepens the mood-stabiliser spine into a single-agent monograph you can teach from cold.[1][2][12]
Definition and place in treatment
Valproate is a branched-chain carboxylic acid anticonvulsant used as a mood stabiliser. Formulations include valproic acid, sodium valproate and divalproex (semisodium) salts; exam teaching treats them as related active species with product-specific kinetics and local brand names (e.g. Epilim, Depakote) rather than interchangeable marketing myths.[1][12]
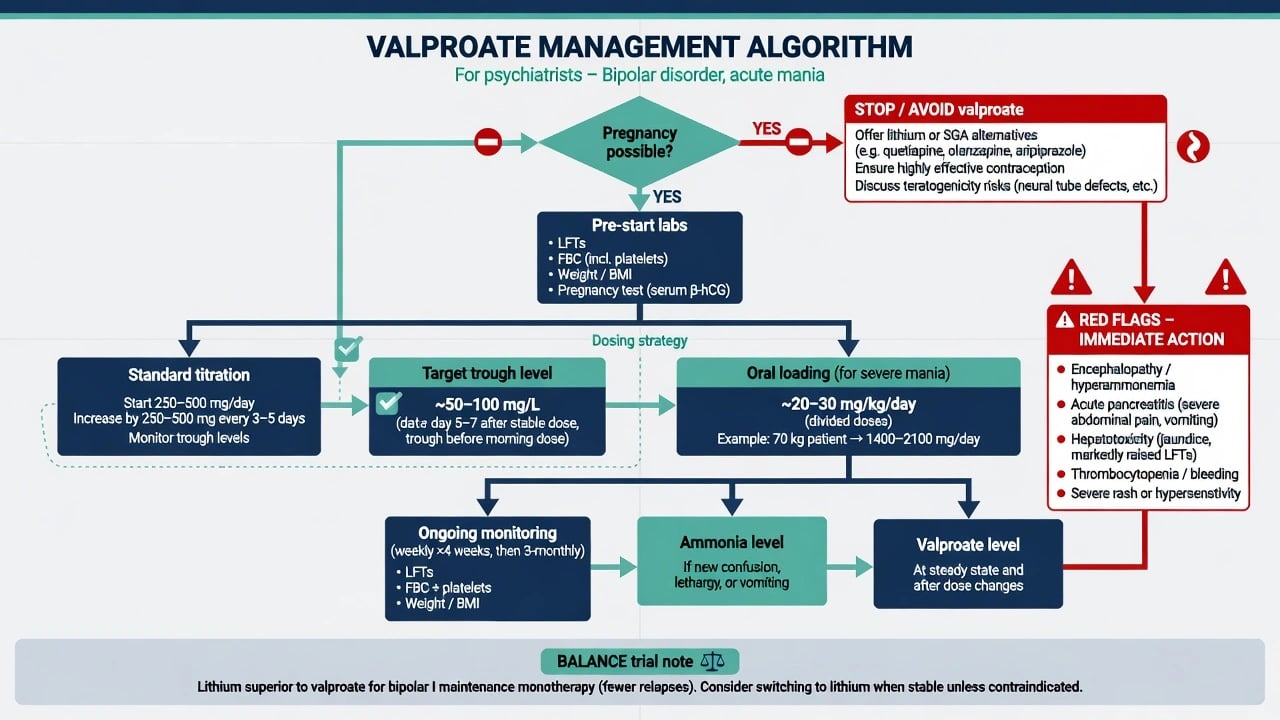
Psychiatric pole fit. Strongest evidence is acute mania (and clinically for mixed features in many algorithms). Maintenance monotherapy is not lithium-equivalent: BALANCE showed lithium superior to valproate monotherapy for bipolar I relapse prevention, with combination also effective.[1][2][3][4]
| Use case | Exam stance |
|---|---|
| Acute mania / mixed | Rational option when pregnancy potential excluded or tightly controlled |
| Bipolar I maintenance monotherapy | Inferior to lithium in BALANCE; do not market as equal |
| Lithium + valproate combination | Effective arm in BALANCE for selected severe/recurrent illness |
| People who can become pregnant | Avoid as routine; pregnancy-prevention framework if exceptional |
| Clozapine seizure cover | Common adjunct — document myocarditis risk trade-offs elsewhere |
| Valproate is a tool, not a default for every bipolar chart.[2][12] |
Mechanisms — viva depth without fluff
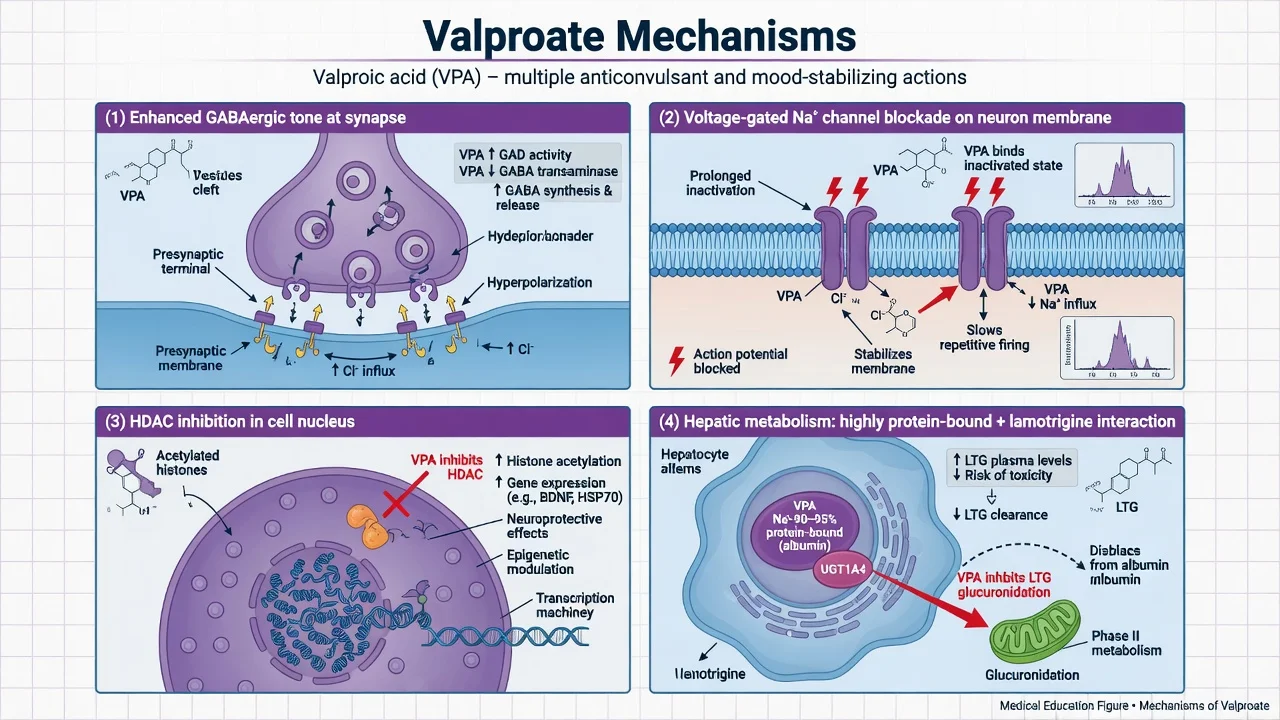
GABAergic enhancement. Valproate increases GABAergic tone through effects on synthesis, degradation and related pathways — a classic antimanic/antiseizure teaching package rather than a single receptor agonist story.[1]
Voltage-gated sodium channel blockade. Use-dependent Na channel effects contribute to antiseizure and mood-stabilising actions shared with other anticonvulsant mood stabilisers.[1]
HDAC inhibition. Histone deacetylase inhibition is a modern mechanistic hook examiners may invite; it also features in teratogenicity hypotheses without claiming a single causal pathway for every birth defect.[5][7]
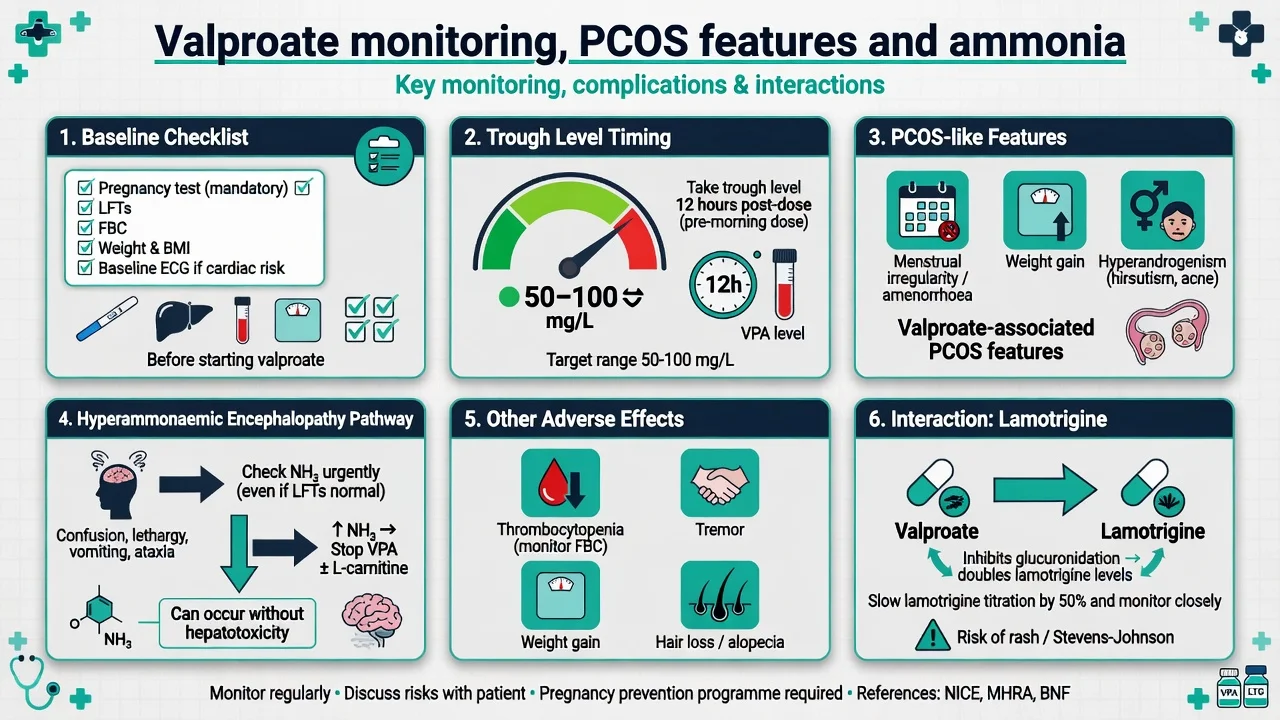
Kinetics and interactions. Highly protein-bound; hepatic metabolism (including glucuronidation and CYP pathways). Critical co-prescription: valproate inhibits lamotrigine metabolism, raising lamotrigine levels — slow LTG titration and lower target doses when combined. Free fraction rises when albumin is low, so total levels can mislead in critical illness.[12][16]
Landmark evidence every candidate must own
Trials and registries that change viva answers
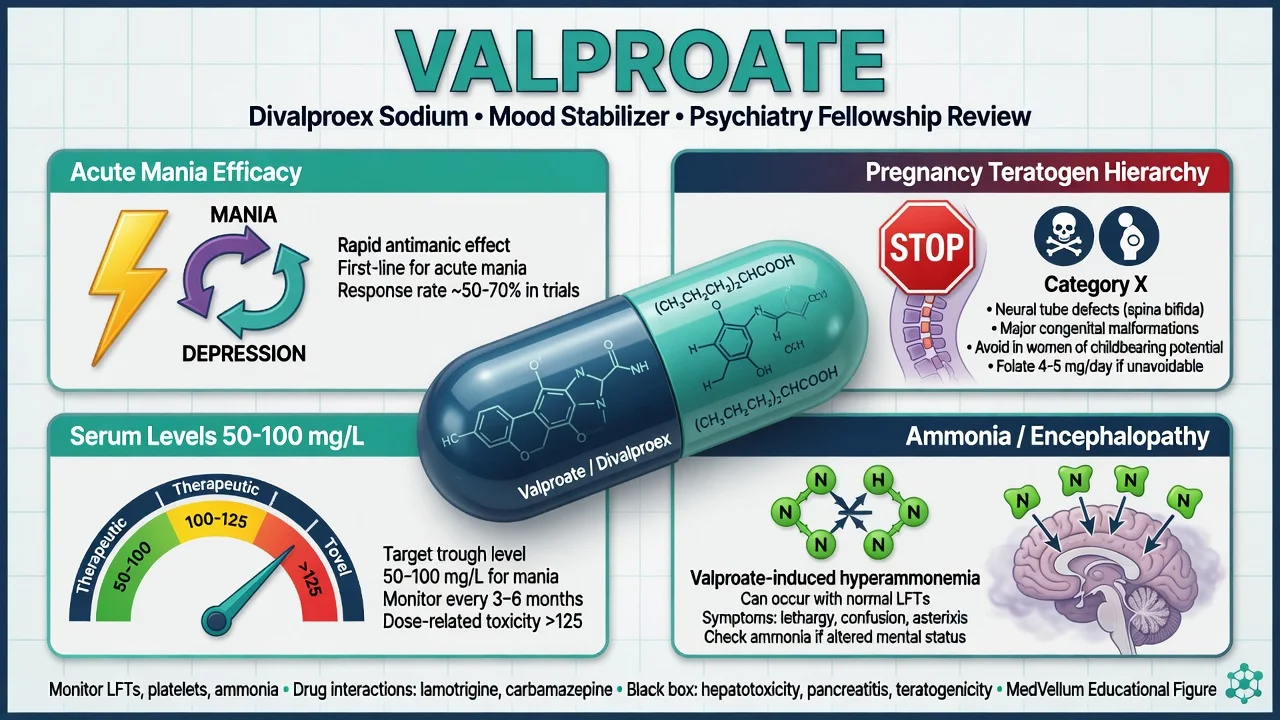
Bowden 1994. Landmark double-blind trial: divalproex was superior to placebo in acute mania and established valproate as a core antimanic option alongside lithium.[1]
Oral loading lineage. Hirschfeld and colleagues showed accelerated oral loading of divalproex can safely reach therapeutic serum concentrations rapidly in acute mania; McElroy randomised oral loading against haloperidol with comparable early antimanic effect in psychotic mania — the exam point is loading is feasible when oral intake, monitoring and consent allow, not reckless megadosing without labs.[11][15]
Allen concentration–response. Analyses support a relationship between higher serum concentrations and greater antimanic response, informing why levels are checked after loading and in non-response rather than treated as optional decoration.[14]
BALANCE. Lithium monotherapy outperformed valproate monotherapy for bipolar I relapse prevention; lithium–valproate combination was also effective. This is the lever against casual long-term valproate-for-all maintenance.[2]
Network meta-analyses. Cipriani places valproate among effective antimanics; Miura frames comparative maintenance options where lithium remains a standout dual-pole agent — use these names, not vague “guidelines say.”[3][4]
Clinical selection algorithm
Prefer valproate for acute mania when: lithium is unsuitable or previously ineffective/intolerable, mixed features dominate local algorithm choice, oral loading is attractive for speed, prior clear VPA response, and pregnancy potential is excluded or managed under an exceptional framework.[1][11][12]
Prefer alternatives when: the person can become pregnant and bipolar maintenance is the question (lithium shared decision, selected SGAs, lamotrigine for depression-pole courses); depression-predominant bipolar without acute mania need; inability to monitor LFT/FBC; active liver disease or pancreatitis history.[2][5][12]
Dosing, loading and levels
Teaching ranges and schedules always yield to local product information and hospital protocols; TDM and dose scaffolds below are exam orientation, not a substitute for the SmPC.[16][12]
Standard adult initiation (scaffold). Many adults start around 500–1000 mg/day in divided doses (or night-weighted extended-release products where available), titrating by clinical response and levels over days. Typical total daily maintenance bands often land in roughly 1000–2000 mg/day for many psychiatric uses, individualised by weight, tolerability and serum concentration.[12][16]
Oral loading for acute mania. Evidence-based loading frameworks commonly teach approximately 20–30 mg/kg/day oral loading strategies (e.g. ~20 mg/kg then adjustment, or ~30 mg/kg/day short protocols in studies) to reach therapeutic serum levels within about a day when the patient can swallow and is monitored. Confirm formulation, renal/hepatic status, and interaction list before loading.[11][15]
Serum levels. Draw trough samples at steady state (commonly ~12 hours after last dose for many BD regimens; once-daily ER products may use product-specific timing). Class teaching therapeutic windows for bipolar use often cite about 50–100 mg/L (µg/mL); acute mania response analyses support aiming toward the upper part of the range when tolerated, with some teaching ceilings near ~125 mg/L before side-effect risk rises disproportionately — individualise, do not worship a single number.[14][16]
When levels matter most: after loading, non-response, suspected toxicity, adherence questions, interacting drug changes, hypoalbuminaemia, and pregnancy-exceptional continuing therapy under specialist care.[14][16]
Pre-start assessment and monitoring
Baseline before first dose: pregnancy test when relevant; contraception and fertility plans; LFT; FBC including platelets; weight/BMI; alcohol and liver risk; full drug list (lamotrigine, topiramate, carbapenems, highly protein-bound drugs, enzyme inducers); capacity for follow-up bloods; documented teratogen counselling.[5][12]
Ongoing: clinical review for tremor, sedation, GI symptoms, cognition; weight trajectory; periodic LFT and FBC/platelets; levels when indicated; ammonia if new confusion or reduced alertness even when transaminases look modest.[13][16]
Pregnancy and teratogenicity hierarchy — highest exam stakes
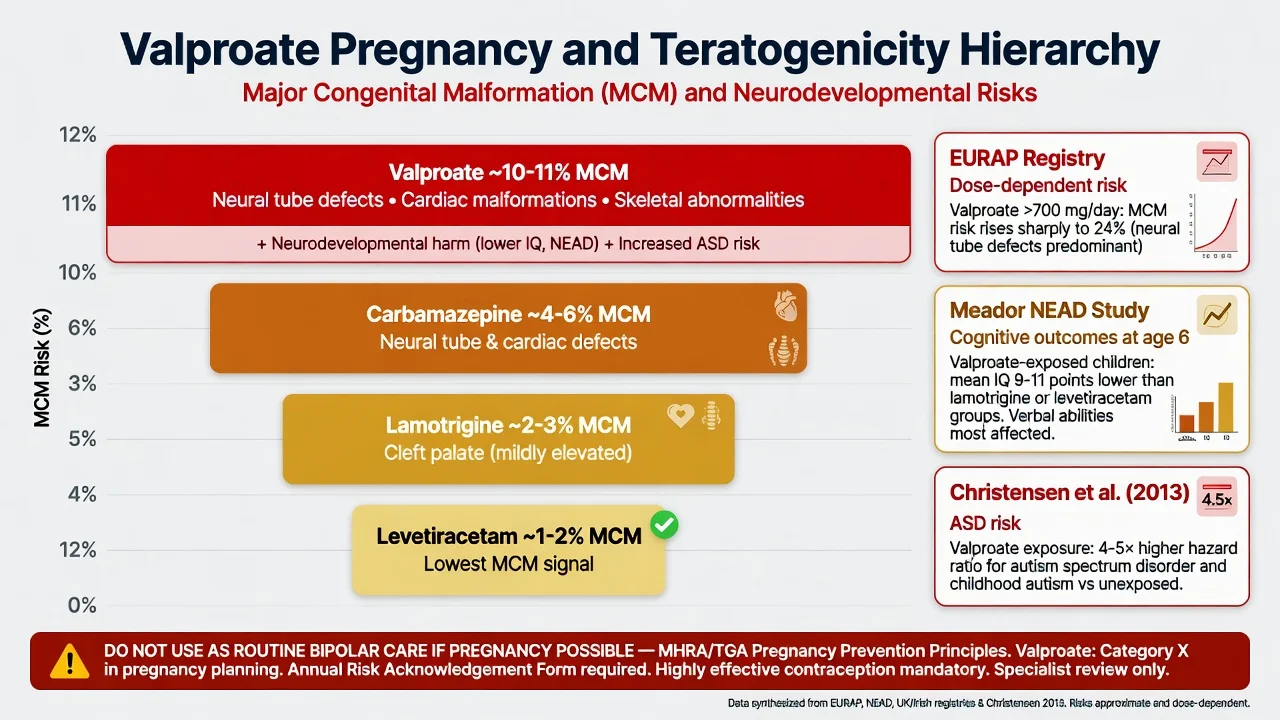
Do not use valproate as routine mood stabilisation in people who can become pregnant. This is not optional soft advice: major congenital malformation risk is high and dose-dependent in EURAP analyses, and comparative registry data place valproate among the highest-risk commonly used antiseizure medicines for MCM.[5][6]
Neurodevelopment. NEAD showed lower cognitive outcomes after fetal valproate exposure at 3 years and again at 6 years versus several comparators — examiners want cognition named, not only structural anomalies.[7][8]
Autism spectrum risk. Population data associate prenatal valproate with increased risk of autism spectrum disorder and childhood autism, including after adjustment for maternal epilepsy in key analyses — quote direction and seriousness, not invented percentages in a viva unless you have them memorised accurately.[9]
Practical hierarchy for bipolar care: prefer non-valproate strategies (lithium shared decision, selected SGAs, lamotrigine for depression-pole, psychosocial anchors); if already on valproate with pregnancy possible, urgently review contraception and plan specialist switch without abrupt stop mid-mania/seizure risk; exceptional continuing use (e.g. refractory epilepsy dual indication) requires specialist framework, highly effective contraception, folic acid per local guidance, lowest effective dose, and documented counselling — not a casual restart after one manic night.[5][6][12]
PCOS-like features and reproductive endocrine effects
Isojärvi and colleagues reported high rates of polycystic ovaries and hyperandrogenism among women taking valproate for epilepsy, embedding a reproductive-endocrine caution into every fellowship discussion of long-term VPA in women and people with ovaries. Counsel about menstrual irregularity, weight gain, hyperandrogenism and metabolic risk; monitor weight; do not dismiss oligomenorrhoea as “stress only.” Causation debates exist in the epilepsy literature, but the clinical duty to screen and counsel stands.[10][12]
Hyperammonaemic encephalopathy
Valproate-induced hyperammonaemic encephalopathy presents with progressive confusion, lethargy, vomiting, ataxia or reduced consciousness and may occur with relatively preserved liver enzymes. Check serum ammonia, stop or hold valproate, support ABC, exclude other causes, involve medical/toxicology partners; L-carnitine is used in severe cases in toxicology pathways. Risk rises with urea-cycle disorders, polypharmacy and high exposures, but can be idiosyncratic — exam pearl: confusion on valproate → ammonia.[13]
Other complications and pitfalls
| Problem | First move |
|---|---|
| Tremor, sedation, GI upset | Level check, dose adjust, formulation review |
| Weight gain / metabolic | Lifestyle, metabolic panel, reconsider long-term choice |
| Thrombocytopenia / bleeding | FBC, hold/reduce, avoid stacking antiplatelets casually |
| Suspected pancreatitis | Stop valproate, lipase/imaging, surgical review |
| Hepatotoxicity | Stop, LFTs, synthetic function, never shrug “mild rise” if sick |
| Lamotrigine rash risk | Slow LTG; educate stop rules for concerning rash |
| Common adverse effects and red-flag pathways for viva speed.[12][13][16] |
Pitfalls that fail stations: starting without pregnancy test; calling valproate “safer than lithium for pregnancy”; ignoring BALANCE when debating maintenance; random non-trough levels used as gospel; full-dose lamotrigine start on VPA; missing ammonia in encephalopathy; loading without baselines or oral intake assessment.[2][5][11][13]
Special populations
People who can become pregnant. Highest priority section — hierarchy above; MHRA-style pregnancy prevention programmes in the UK and analogous TGA/local frameworks shape consent and documentation. NICE and RANZCP-aligned bipolar care treat valproate avoidance as a quality standard, not a footnote.[5][6][12]
Lactation. Specialist perinatal advice; many teams prefer alternatives when feasible; if continued, monitor infant sedation/feeding and maternal levels as indicated.[12]
Older adults. Lower starting doses, fall and sedation risk, hepatic reserve, polypharmacy interactions, platelet and cognitive vigilance.[12]
Youth. Specialist initiation; endocrine and weight monitoring; start pregnancy-prevention conversations early when developmentally appropriate.[12]
Hepatic disease / alcohol use disorder. Caution or avoid; baseline and frequent LFTs if unavoidable; discuss alternatives first.[12]
Intellectual disability / epilepsy dual care. Multidisciplinary; teratogen rules still apply to any person who can become pregnant; do not assume “epilepsy needs VPA forever” without review.[5][12]
Prognosis and disposition
Acute mania often improves over days to 1–2 weeks once levels are adequate and sleep/agitation are controlled (often with short-term antipsychotic or benzo cover per mania protocols). Long-term: if the only reason for staying on valproate is inertia, re-evaluate against lithium and SGA maintenance options using BALANCE and network evidence. Admit for severe mania risk, encephalopathy, pancreatitis or hepatic failure pathways.[1][2][13]
Evidence, guidelines and regional differences
| Source | Exam take-home |
|---|---|
| Bowden 1994 | Divalproex antimanic efficacy vs placebo |
| Hirschfeld / McElroy | Oral loading feasible and effective frameworks |
| Allen 2006 | Concentration–response in acute mania |
| BALANCE 2010 | Lithium better than VPA monotherapy maintenance |
| Cipriani / Miura NMA | Antimanic and maintenance comparative fields |
| EURAP Tomson | Dose-dependent and comparative MCM risk |
| NEAD Meador | Cognitive outcomes after fetal exposure |
| Christensen 2013 | ASD/autism association with prenatal VPA |
| Isojärvi 1993 | PCOS/hyperandrogenism association signal |
| CANMAT/ISBD 2018 | Algorithmic bipolar placement with safety gates |
| Landmark synthesis for viva speed.[1][2][3][4][5][7][9][10][11][12][14] |
ANZ: TGA and RANZCP-aligned practice treat valproate as high-teratogen; document contraception and prefer alternatives in people who can become pregnant. UK: MHRA valproate pregnancy prevention programme culture is examinable; NICE bipolar guidance avoids valproate in this group. US: FDA boxed warnings for hepatotoxicity, pancreatitis and fetal risk; APA bipolar principles emphasise shared decision with strong teratogen caution. Europe: EURAP registry culture and strong regulatory restrictions. Exact legal forms differ — the clinical hierarchy does not.[5][6][12]
Exam pearls
Acute mania
- Bowden efficacy
- Oral loading option
- Levels guide response
- Often + SGA if severe
Maintenance
- BALANCE: weaker than Li mono
- Combination Li+VPA option
- Reassess inertia
- Polarity + pregnancy review
Pregnancy gate
- Avoid if pregnancy possible
- EURAP MCM risk
- NEAD cognition
- Christensen ASD signal
Safety board
- Ammonia if confused
- LFT + platelets
- PCOS-like features
- Slow LTG with VPA
References
- [1]Bowden CL, Brugger AM, Swann AC, et al. Efficacy of divalproex vs lithium and placebo in the treatment of mania. The Depakote Mania Study Group JAMA, 1994.PMID 8120960
- [2]BALANCE investigators and collaborators, Geddes JR, Goodwin GM, et al. Lithium plus valproate combination therapy versus monotherapy for relapse prevention in bipolar I disorder (BALANCE): a randomised open-label trial Lancet, 2010.PMID 20092882
- [3]Cipriani A, Barbui C, Salanti G, et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis Lancet, 2011.PMID 21851976
- [4]Miura T, Noma H, Furukawa TA, et al. Comparative efficacy and tolerability of pharmacological treatments in the maintenance treatment of bipolar disorder: a systematic review and network meta-analysis Lancet Psychiatry, 2014.PMID 26360999
- [5]Tomson T, Battino D, Bonizzoni E, et al. Dose-dependent risk of malformations with antiepileptic drugs: an analysis of data from the EURAP epilepsy and pregnancy registry Lancet Neurol, 2011.PMID 21652013
- [6]Tomson T, Battino D, Bonizzoni E, et al. Comparative risk of major congenital malformations with eight different antiepileptic drugs: a prospective cohort study of the EURAP registry Lancet Neurol, 2018.PMID 29680205
- [7]Meador KJ, Baker GA, Browning N, et al. Cognitive function at 3 years of age after fetal exposure to antiepileptic drugs N Engl J Med, 2009.PMID 19369666
- [8]Meador KJ, Baker GA, Browning N, et al. Fetal antiepileptic drug exposure and cognitive outcomes at age 6 years (NEAD study): a prospective observational study Lancet Neurol, 2013.PMID 23352199
- [9]Christensen J, Grønborg TK, Sørensen MJ, et al. Prenatal valproate exposure and risk of autism spectrum disorders and childhood autism JAMA, 2013.PMID 23613074
- [10]Isojärvi JI, Laatikainen TJ, Pakarinen AJ, et al. Polycystic ovaries and hyperandrogenism in women taking valproate for epilepsy N Engl J Med, 1993.PMID 8413434
- [11]Hirschfeld RM, Allen MH, McEvoy JP, et al. Safety and tolerability of oral loading divalproex sodium in acutely manic bipolar patients J Clin Psychiatry, 1999.PMID 10665626
- [12]Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder Bipolar Disord, 2018.PMID 29536616
- [13]Segura-Bruna N, Rodriguez-Campello A, Puente V, et al. Valproate-induced hyperammonemic encephalopathy Acta Neurol Scand, 2006.PMID 16774619
- [14]Allen MH, Hirschfeld RM, Wozniak PJ, et al. Linear relationship of valproate serum concentration to response and optimal serum levels for acute mania Am J Psychiatry, 2006.PMID 16449481
- [15]McElroy SL, Keck PE, Stanton SP, et al. A randomized comparison of divalproex oral loading versus haloperidol in the initial treatment of acute psychotic mania J Clin Psychiatry, 1996.PMID 8601548
- [16]Haymond J, Ensom MH Does valproic acid warrant therapeutic drug monitoring in bipolar affective disorder? Ther Drug Monit, 2010.PMID 19901867