Psych · psychotherapy
Acceptance and commitment therapy
Also known as ACT · Acceptance & commitment therapy · Acceptance-based behaviour therapy · Contextual CBT · Hexaflex therapy · Psychological flexibility therapy · Third-wave ACT
Exam-exhaustive fellowship reference on acceptance and commitment therapy (ACT): psychological flexibility and the hexaflex, experiential avoidance and fusion, techniques, indication-specific evidence (anxiety, depression, OCD, psychosis adjunct, chronic pain), comparison with CBT/DBT/MBCT/ERP, AAQ-II, combined care, and CASC/MEQ pearls. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship examiners expect you to name the hexaflex, contrast ACT with traditional CBT / ERP / DBT, explain experiential avoidance and fusion, outline a session sequence, cite meta-analyses and indication trials, and state when ACT is not the priority (acute risk, mania, medical emergency).[1][2][3]
Definition and classification
ACT is grounded in functional contextualism and Relational Frame Theory (RFT) accounts of language: verbal humans can problem-solve brilliantly and also get trapped in rule-governed rigidity, reason-giving, and struggle with private events.[1] It is transdiagnostic in intent, with manuals and evidence density varying by disorder (anxiety, depression, OCD spectrum, psychosis adjuncts, chronic pain, workplace stress, stigma).[3][4]
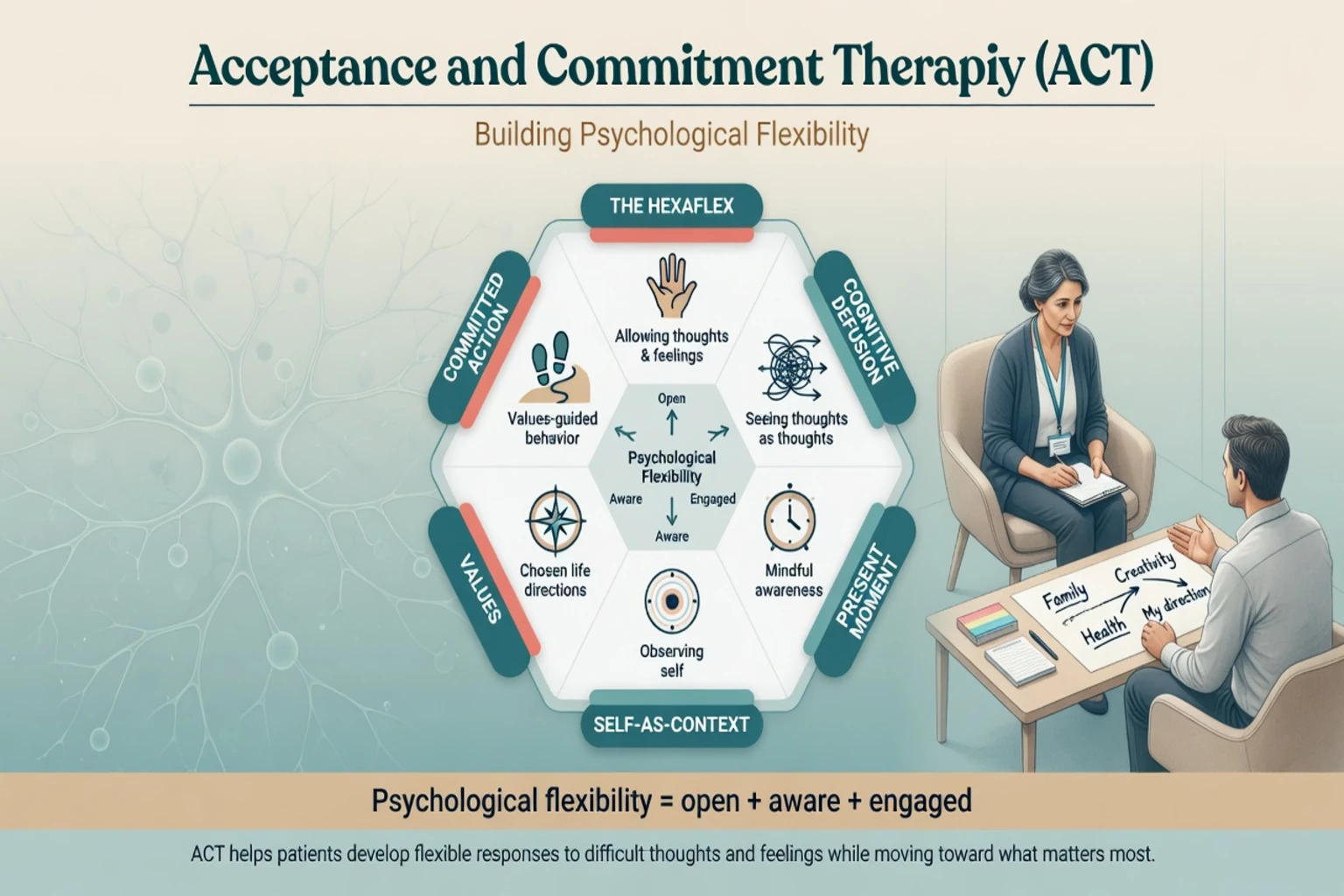
Psychological flexibility (exam definition)
The ability to contact the present moment as a conscious human being, and to change or persist in behaviour when doing so serves valued ends.[1]
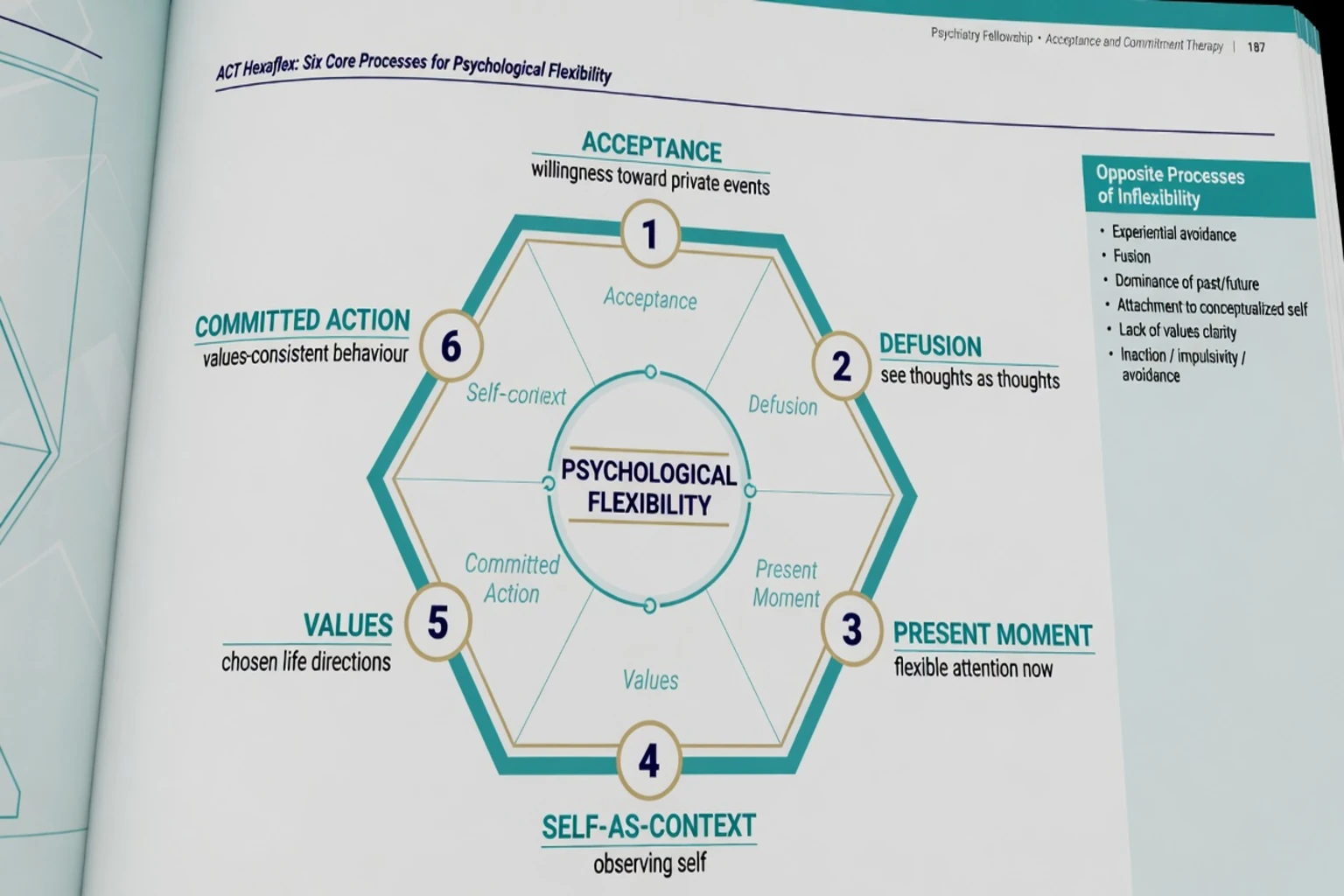
Hexaflex — six processes
| Process | Clinical gloss |
|---|---|
| Acceptance | Willingness to experience private events without unnecessary struggle |
| Cognitive defusion | Seeing thoughts as thoughts (events in mind), not literal commands |
| Present-moment contact | Flexible attention to here-and-now |
| Self-as-context | Observing self — perspective-taking beyond the story of "I am X" |
| Values | Chosen life directions (not goals that finish) |
| Committed action | Values-consistent behaviour, including graded activation and exposure-with-willingness |
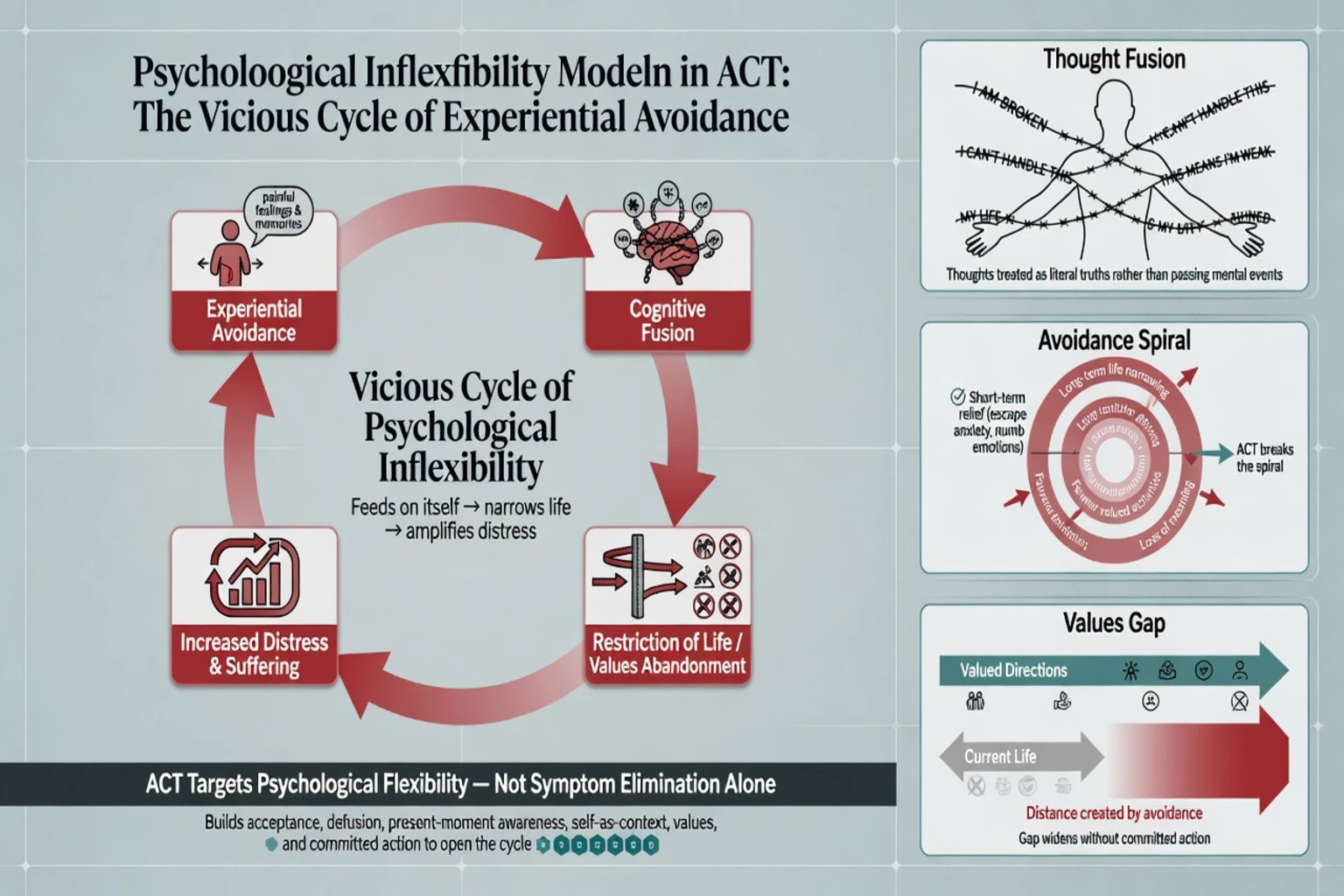
Six processes of inflexibility (mirror map)
Experiential avoidance; cognitive fusion; dominance of conceptualised past/feared future; attachment to conceptualised self; lack of values clarity; inaction, impulsivity, or persistent avoidance patterns.[1][2]
Mechanisms (pathophysiology of inflexibility)
Experiential avoidance — efforts to avoid, suppress, or escape unwanted thoughts, feelings, memories, or sensations — can reduce distress short-term while narrowing life long-term (cancelled relationships, avoided exposure, abandoned roles). Hayes and colleagues framed experiential avoidance as a functional dimension across behavioural disorders, not a single DSM diagnosis.[2]
Cognitive fusion treats verbal products as absolute reality ("I am a failure" → behavioural compliance with that rule). Defusion changes the function of the thought without requiring belief change as the first move.[1]
ACT therefore targets process (flexibility) rather than only content (thought accuracy). Traditional CBT more often works cognitive content, behavioural experiments, and exposure for extinction/new learning; ACT often uses exposure-like contact with private events under a willingness and values frame.[1][10]
Epidemiology and evidence positioning
Multiple meta-analyses place ACT as more effective than waitlist/placebo/TAU for clinically relevant mental and physical health problems, with often comparable effects to established treatments including CBT in several comparisons — though study quality and bias risk vary and are examinable.[3][4][5][6]
Öst's third-wave and ACT-specific reviews are critical landmarks: they support efficacy signals while highlighting methodological limitations in parts of the literature — do not present ACT evidence as uniformly gold-standard or as always superior to CBT.[5][6]
Depression-specific synthesis (Bai and colleagues) supports ACT for depressive symptoms versus control conditions in systematic review/meta-analysis framing.[14] Anxiety and OCD spectrum reviews support a growing ACT evidence base with heterogeneity by protocol and comparator.[15]
Access reality: fewer ACT-specialist therapists than CBT in many public systems; training and fidelity matter as much as brand name.[3][5]
Clinical presentation — what ACT looks like
Good ACT is experiential, not a pure lecture on philosophy. Sessions typically mix mapping the control agenda, willingness practices, defusion of sticky thoughts, values clarification (relationships, work/education, health, recreation, culture/spirituality as the patient defines), committed action homework that is specific, graded, and scheduled, and present-moment/self-as-context work when attention is stuck in rumination/worry or self-story.[1]
Patient experience often feels counterintuitive: make room for discomfort while doing what matters, rather than waiting to feel motivated or symptom-free.[1]
Differential: ACT among therapies
| Modality | Primary target | Contrast with ACT |
|---|---|---|
| Traditional CBT/CT | Thought content, behavioural experiments, skill teaching | ACT prioritises function of private events and values-based action |
| ERP (OCD) | Habituation/inhibitory learning via exposure without rituals | ERP remains core for many OCD pathways; ACT may aid engagement |
| DBT | Emotion dysregulation, self-harm hierarchy, multi-modal skills | Different structure; acceptance–change dialectic is related but not identical package |
| MBCT | Mindfulness curriculum, classically depression relapse prevention | ACT is broader values/action package, not only meditation classes |
| Behavioural activation | Reinforcement and anti-avoidance activation | ACT adds defusion/self-as-context and explicit values framing |
Assessment
- Confirm syndrome (depression, anxiety, OCD, psychosis, pain–psychiatry interface) and severity.
- Full risk assessment; substance use; bipolar screen when activating behaviourally.
- Map avoidance/fusion: what is being avoided, at what life cost?
- Values assessment — co-created, culturally humble.
- Suitability: alliance capacity; not solely crisis stabilisation.
- Measures: disorder-specific scales plus process measures such as the Acceptance and Action Questionnaire-II (AAQ-II) for psychological inflexibility where used — AAQ-II is not a diagnostic test.[13]
Investigations are those of the underlying syndrome (medical differentials for mood/psychosis, baseline labs/ECG if starting psychotropics). No biomarker selects ACT candidacy.[1][13]
Acute and emergency limits
[1] [7]Definitive management
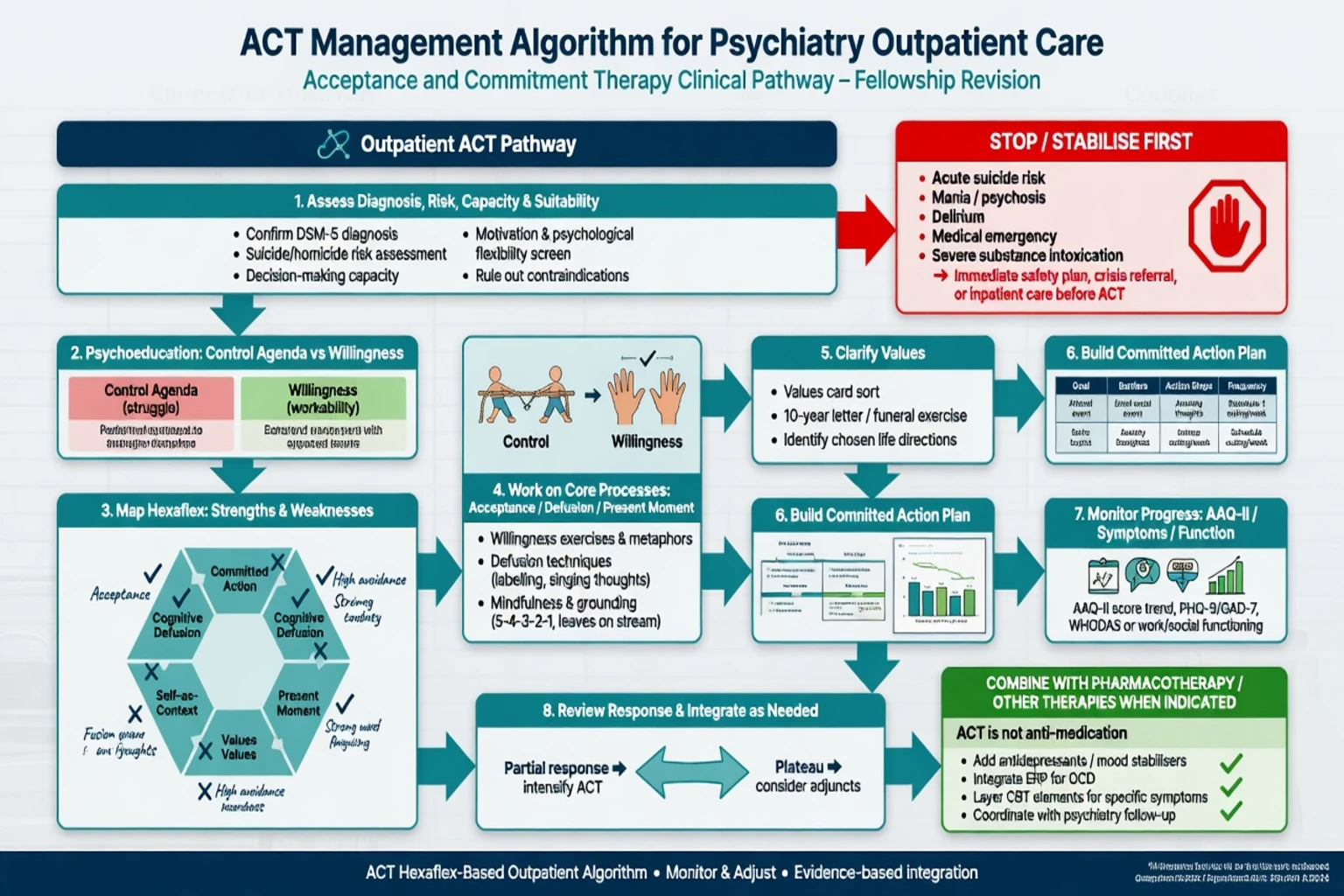
Core sequence (exam-ready)
- Engage; explain control agenda and creative hopelessness (costs of struggle) carefully and compassionately.
- Build willingness/acceptance skills.
- Train defusion (e.g. "I am having the thought that…", distancing metaphors used judiciously).
- Strengthen present-moment and self-as-context.
- Clarify values (directions, not finishable goals).
- Design committed action plans (graded, scheduled, reviewed).
- Integrate exposure-with-willingness when anxiety/OCD formulation requires contact with feared cues.
- Review outcome: symptoms, function, flexibility (AAQ-II optional), homework fidelity.[1][13]
Session skeleton (CASC-friendly)
Check-in and measures → homework review (what was tried, what got in the way) → brief experiential exercise → values/action planning → written commitment and risk check.[1]
Format and dose
Protocols vary: e.g. about eight weekly sessions in a major OCD ACT RCT versus progressive relaxation; longer courses for complex comorbidity; group and workplace protocols exist.[9][4] State the planned course and review points rather than endless open-ended "ACT chat."
Combining with medication and ERP
ACT is not anti-medication. For moderate–severe depression or anxiety, antidepressants follow usual pathways (example pattern: SSRI such as sertraline starting low, e.g. sertraline 50 mg oral daily, titrate toward a therapeutic range with review of response, activation/agitation, GI and sexual effects, and suicide risk early in treatment — always per local formulary and product information, not as a universal script).[11][14]
For OCD, ERP remains a behavioural cornerstone in many guidelines; Twohig and colleagues tested ACT versus relaxation and later ACT added to ERP — use ACT to reduce fusion/avoidance that blocks exposure, not as an ideological replacement when ERP is indicated and accessible.[9][16]
FLEXACT
Subtypes and scenarios
| Scenario | ACT emphasis | Landmark anchors |
|---|---|---|
| Mixed anxiety | Flexibility vs control of anxiety; comparative CBT trials | Arch 2012; Bluett review |
| Depression | Willingness + values-based activation | Forman 2007; Bai 2020 |
| OCD | Defusion from obsessions; exposure-with-willingness; ACT±ERP | Twohig 2010; Twohig 2018 |
| Psychosis (adjunct) | Reduce struggle/believability; functioning; not "delete voices" | Bach and Hayes 2002; Gaudiano 2006; Shawyer 2017 |
| Chronic pain | Function and acceptance; interference reduction | Wetherell 2011 pain RCT |
| Older adult GAD | Adapted ACT package | Wetherell 2011 GAD pilot |
| Workplace stress | Values and psychological flexibility at work | Bond lineage in process literature |
Psychosis note (exam-careful)
Brief ACT reduced rehospitalisation and changed relationship to symptoms in early inpatient work (Bach and Hayes; Gaudiano and Herbert pilot). Larger outpatient RCTs (e.g. Shawyer) require nuanced reading — do not claim ACT replaces antipsychotic care or early intervention packages.[7][8][17]
Complications and pitfalls
| Pitfall | Correction |
|---|---|
| Acceptance = resignation | Willingness in service of values; safety planning for abuse |
| Values imposition | Co-create; cultural humility |
| Mindfulness-only homework | Always couple with committed action |
| Pure ACT ideology | Combine meds/ERP when indicated |
| Premature deep work | Stabilise risk first |
| Endless therapy without goals | Time-box, review function |
Prognosis and disposition
Meta-analytic signals support clinically meaningful benefit versus inactive controls across several problem domains, with frequent rough parity versus active CBT comparators in anxiety, pain, and related areas — exact effect sizes depend on population, control type, and study quality.[3][4][5][10][12]
Disposition: outpatient individual or group pathways; stepped care from guided self-help to specialist ACT; CMHT shared care when risk or severity is high; brief inpatient ACT-consistent work only when medically/psychiatrically stable enough.[3][1]
Step up when non-response follows adequate dose/fidelity, when trauma-focused or DBT programmes better fit the formulation, or when risk escalates. Step down to self-management with a written values–action plan when stable.[1][3]
Special populations
- Youth: concrete values language; caregiver scaffolding; growing but mixed evidence — claim carefully.[3]
- Older adults: Wetherell GAD pilot supports feasibility; medical pacing of committed action.[18]
- Pregnancy/lactation: psychological therapies including acceptance-based approaches may be preferred or combined depending on severity; medication decisions are separate risk–benefit discussions.[14]
- Intellectual disability: simplify metaphors; behavioural committed action; carer involvement.[1]
- Cultural diversity: values are patient-defined; metaphors must be culturally adapted.[1]
- Chronic medical illness/pain: function-first outcomes are natural ACT targets.[12]
Evidence and guidelines
Must-name landmarks
- Hayes 2006 process/outcome model; Hayes 1996 experiential avoidance.[1][2]
- Powers 2009; A-Tjak 2015 metas; Öst 2008/2014 critical third-wave/ACT reviews.[3][4][5][6]
- Bach and Hayes 2002; Gaudiano and Herbert 2006; Shawyer 2017 psychosis line.[7][8][17]
- Twohig 2010/2018 OCD; Arch 2012 mixed anxiety CBT vs ACT; Forman 2007 ACT vs CT; Bai 2020 depression meta; Bluett 2014 anxiety/OCD review.[9][10][11][14][15][16]
- Wetherell 2011 chronic pain RCT and older adult GAD pilot; Bond 2011 AAQ-II.[12][13][18]
Regional framing
Exam pearls
[1] [5] [9] [10]CASC micro-skills
Collaborative tone; avoid jargon pile-up (hexaflex can wait until after plain language); give a one-sentence definition of flexibility; practise one defusion of a sticky thought without arguing content; co-create one values-consistent action for the next 48 hours; and close with an explicit safety-net if mood or risk worsens.[1]
Rapid revision table
| Domain | Anchor |
|---|---|
| Aim | Psychological flexibility |
| Map | Hexaflex (six processes) |
| Core problems | Experiential avoidance + fusion |
| Technique core | Willingness, defusion, values, committed action |
| Process measure | AAQ-II (not diagnostic) |
| Broad metas | Powers 2009; A-Tjak 2015; Öst critical updates |
| OCD | Twohig 2010; ACT+ERP 2018 |
| Psychosis adjunct | Bach/Hayes; Gaudiano; Shawyer |
| Safety | Stabilise risk/mania/medical first |
| Not the same as | Mindfulness-only apps or pure CBT content work |
References
- [1]Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J Acceptance and commitment therapy: model, processes and outcomes Behav Res Ther, 2006.PMID 16300724
- [2]Hayes SC, Wilson KG, Gifford EV, Follette VM, Strosahl K Experiential avoidance and behavioral disorders: a functional dimensional approach to diagnosis and treatment J Consult Clin Psychol, 1996.PMID 8991302
- [3]A-Tjak JG, Davis ML, Morina N, Powers MB, Smits JA, Emmelkamp PM A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems Psychother Psychosom, 2015.PMID 25547522
- [4]Powers MB, Zum Vorde Sive Vording MB, Emmelkamp PM Acceptance and commitment therapy: a meta-analytic review Psychother Psychosom, 2009.PMID 19142046
- [5]Ost LG The efficacy of Acceptance and Commitment Therapy: an updated systematic review and meta-analysis Behav Res Ther, 2014.PMID 25193001
- [6]Ost LG Efficacy of the third wave of behavioral therapies: a systematic review and meta-analysis Behav Res Ther, 2008.PMID 18258216
- [7]Bach P, Hayes SC The use of acceptance and commitment therapy to prevent the rehospitalization of psychotic patients: a randomized controlled trial J Consult Clin Psychol, 2002.PMID 12362963
- [8]Gaudiano BA, Herbert JD Acute treatment of inpatients with psychotic symptoms using Acceptance and Commitment Therapy: pilot results Behav Res Ther, 2006.PMID 15893293
- [9]Twohig MP, Hayes SC, Plumb JC, et al. A randomized clinical trial of acceptance and commitment therapy versus progressive relaxation training for obsessive-compulsive disorder J Consult Clin Psychol, 2010.PMID 20873905
- [10]Arch JJ, Eifert GH, Davies C, et al. Randomized clinical trial of cognitive behavioral therapy (CBT) versus acceptance and commitment therapy (ACT) for mixed anxiety disorders J Consult Clin Psychol, 2012.PMID 22563639
- [11]Forman EM, Herbert JD, Moitra E, Yeomans PD, Geller PA A randomized controlled effectiveness trial of acceptance and commitment therapy and cognitive therapy for anxiety and depression Behav Modif, 2007.PMID 17932235
- [12]Wetherell JL, Afari N, Rutledge T, et al. A randomized, controlled trial of acceptance and commitment therapy and cognitive-behavioral therapy for chronic pain Pain, 2011.PMID 21683527
- [13]Bond FW, Hayes SC, Baer RA, et al. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance Behav Ther, 2011.PMID 22035996
- [14]Bai Z, Luo S, Zhang L, Wu S, Chi I Acceptance and Commitment Therapy (ACT) to reduce depression: A systematic review and meta-analysis J Affect Disord, 2020.PMID 31563072
- [15]Bluett EJ, Homan KJ, Morrison KL, Levin ME, Twohig MP Acceptance and commitment therapy for anxiety and OCD spectrum disorders: an empirical review J Anxiety Disord, 2014.PMID 25041735
- [16]Twohig MP, Abramowitz JS, Smith BM, et al. Adding acceptance and commitment therapy to exposure and response prevention for obsessive-compulsive disorder: A randomized controlled trial Behav Res Ther, 2018.PMID 29966992
- [17]Shawyer F, Farhall J, Thomas N, et al. Acceptance and commitment therapy for psychosis: randomised controlled trial Br J Psychiatry, 2017.PMID 27979820
- [18]Wetherell JL, Afari N, Ayers CR, et al. Acceptance and Commitment Therapy for generalized anxiety disorder in older adults: a preliminary report Behav Ther, 2011.PMID 21292059