Psych · Psychotherapy
Cognitive analytic therapy
Also known as CAT · Cognitive-analytic therapy · Cognitive Analytical Therapy · Ryle CAT · Sequential diagrammatic reformulation · Reciprocal role procedures
Exam-exhaustive fellowship reference on cognitive analytic therapy (CAT): Ryle integrative model, reciprocal roles, traps/dilemmas/snags, reformulation letter and SDR map, recognition–revision–ending structure, landmark Chanen/Clarke/Treasure/Fosbury evidence, meta-analytic acceptability, and differentials versus CBT, MBT, schema, and IPT. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship exams test whether you can define CAT tools and phases, name RRPs and traps/dilemmas/snags, outline a brief contract, differentiate CAT from CBT/MBT/schema/IPT, and cite landmark trials honestly without overclaiming.[1][2][3]
Definition and classification
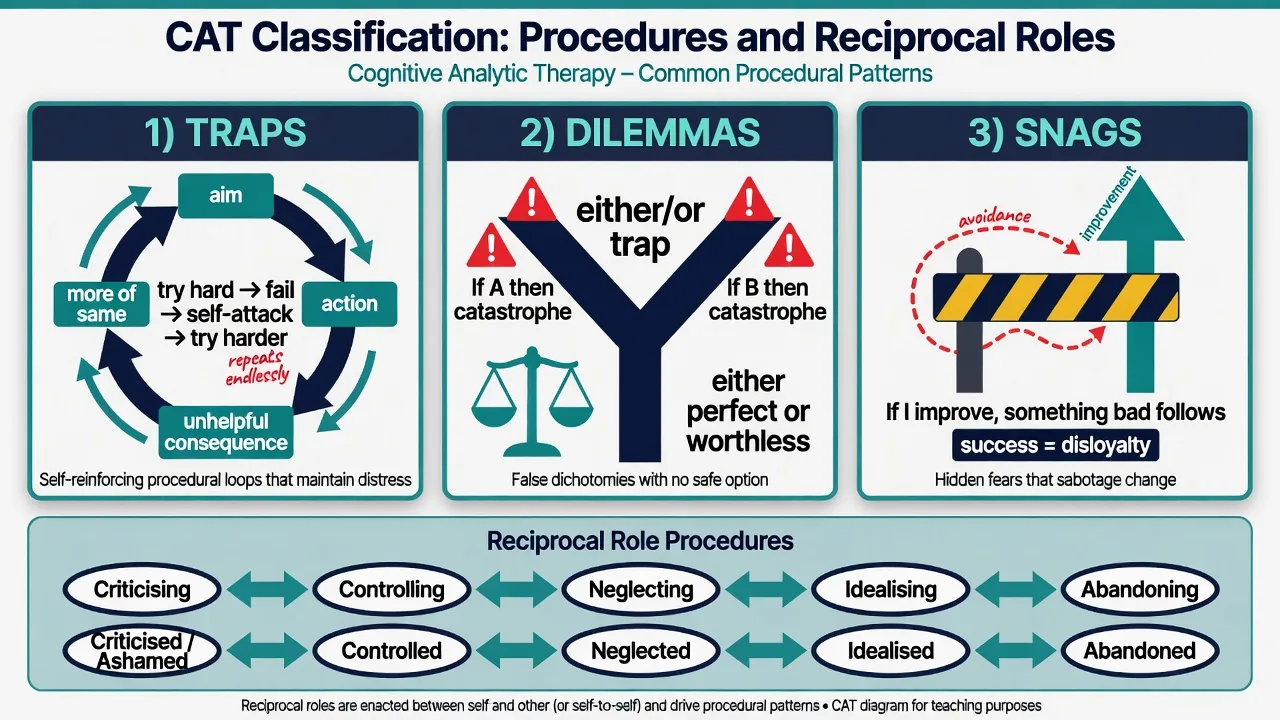
CAT is not “CBT with a letter.” It is a relational procedural model: early and current relationships are internalised as reciprocal roles (linked self–other positions such as criticising–criticised, abandoning–abandoned, controlling–controlled, idealising–idealised). These roles organise feeling, thinking, and action in procedures that become self-maintaining.[11]
| Tool / construct | Exam definition | Clinical use |
|---|---|---|
| Reciprocal role procedure (RRP) | Linked pair of positions (self ↔ other or self ↔ self) that can switch under stress | Name enactments in relationships and therapy |
| Target problem procedure (TPP) | The specific sequence maintaining the complaint | Focus of recognition and exits |
| Traps | Circular procedures where efforts to solve worsen the problem | E.g. try hard → fail → self-attack → try harder |
| Dilemmas | False either/or polarities | E.g. either perfect or worthless; either close and controlled or free and alone |
| Snags | Covert bans on improvement (“if I get better, something bad follows”) | Guilt, loyalty binds, fear of success |
| Psychotherapy file | Structured self-report of common patterns | Seeds early reformulation |
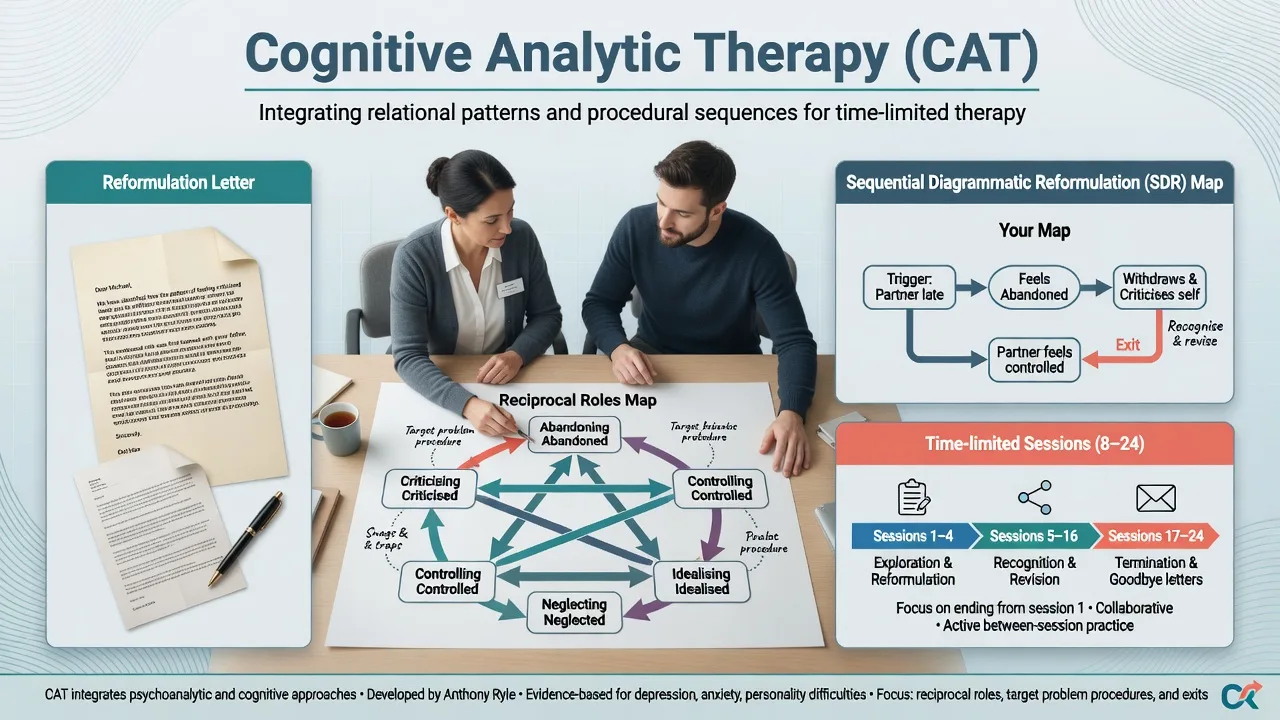
| Reformulation letter | Written narrative reformulation from therapist (shared and revised) | Humanises pattern without pejorative labelling |
| SDR / map | Sequential diagrammatic reformulation of key roles and procedures | Shared visual tool for recognition |
| Exits | Alternative procedures and role experiments | Revision-phase change methods |
| Goodbye letter | Ending letter(s) consolidating learning and marking separation | Manages ending as a role event |
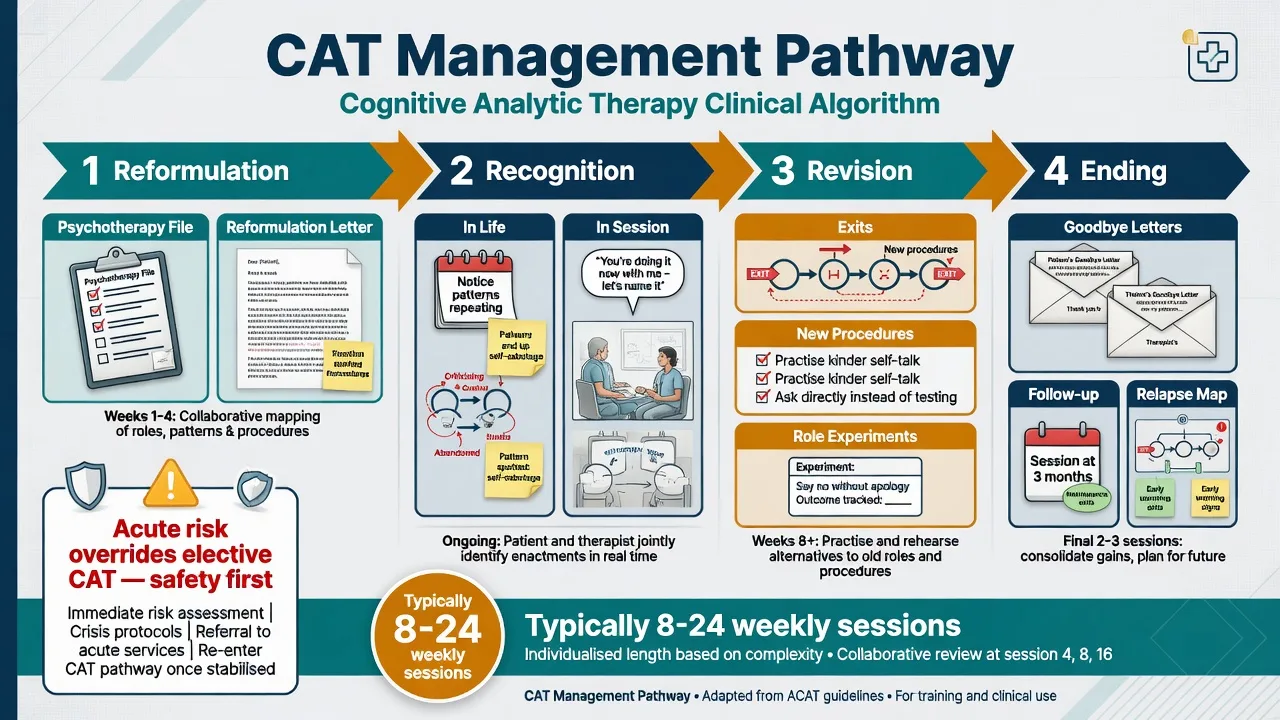
Course structure. Typical adult CAT is weekly and time-limited: often 8–16 sessions for focal problems and about 16–24 sessions for more complex personality-related presentations (trial protocols vary; Clarke used 24 sessions). Phases are classically reformulation → recognition → revision, with explicit ending and follow-up.[2][3][5]
Mechanism: roles, procedures, self-states
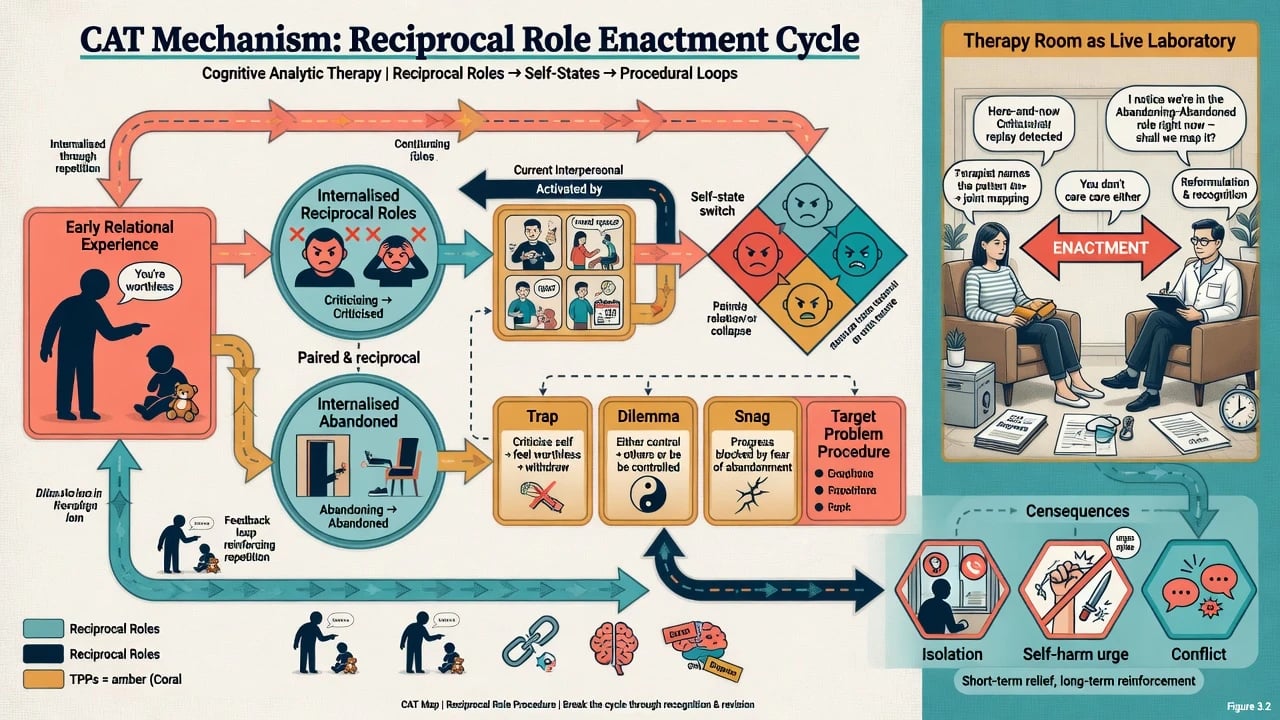
Ryle’s procedural sequence model describes how aims lead to actions, consequences, evaluations, and revised aims. Unhelpful sequences become automatic procedures. In personality pathology, multiple self-states may be partially dissociated and linked by rapid role switches, producing identity instability and chaotic relationships. Mapping aims to make the system visible, shared, and revisable rather than only listing DSM criteria.[6][11]
The therapy relationship is a live laboratory: the same RRPs that organise outside life can be enacted with the therapist (e.g. patient expects abandonment; therapist feels pushed to over-rescue or cut off). CAT names these enactments collaboratively rather than interpreting them as secret truth only the therapist owns.[5][11]
Clinical presentation and bedside assessment
Typical referrals: complex interpersonal patterns, personality-disorder features with role switches, recurrent self-harm after perceived abandonment or criticism, chronic depression entangled with relational traps, eating-disorder control/surrender roles, or long-term illness self-care sabotage (e.g. diabetes).[1][2][7][9]
What good CAT looks like at the bedside: a stated time limit, early psychotherapy file themes, a shared reformulation letter, a map that both parties can point to, recognition homework, explicit exits, and a planned ending. Absence of these tools is a fidelity red flag.[3][5]
Always assess first: suicide/self-harm risk; violence risk; substance use; bipolar/psychosis screen; medical status in eating disorders and diabetes; trauma load; cultural models of roles and shame; practical ability to attend a time-limited course; and whether the person wants collaborative written reformulation versus only crisis contact.[1][6][9]
Investigations do not diagnose reciprocal roles. Track outcomes with symptom scales, self-harm frequency, interpersonal crises, and — in medical adaptations — HbA1c, weight, or electrolytes as indicated. Research settings may rate therapist competence/fidelity.[5][9]
Acute care and definitive management
Acute / resuscitation of the frame
Medical stabilisation and standard risk assessment outrank mapping after overdose, high-lethality self-harm, unstable medical eating disorder, severe hypoglycaemia, mania, or delirium. Once safe, help the person notice the role–procedure sequence of the crisis without blame, and do not force deep shaming-role work in an uncontained crisis.[1][6]
Definitive CAT pathway
| Phase | Tasks | Examiner anchors |
|---|---|---|
| Reformulation | History, psychotherapy file, draft letter, collaborative SDR map | Shared ownership; revise language that shames |
| Recognition | Notice TPPs/RRPs in daily life and in session | “What just happened between us on the map?” |
| Revision | Exits, role experiments, self-to-self care, break traps/dilemmas/snags | Change is procedural, not insight alone |
| Ending | Goodbye letters, anticipate abandonment/rejection enactments, follow-up | Ending is treatment, not admin |
Combined care. Treat comorbid depression, anxiety, ADHD, substance use, sleep, and medical illness with usual evidence-based medical care. CAT is not a reason to withhold indicated antidepressants or medical monitoring.[4][8]
Team/contextual CAT. Reciprocal-role maps can describe staff–patient and team patterns (rescue–abandon; control–revolt) that maintain iatrogenic cycles in complex care — an examinable systems application beyond individual sessions.[11]
Comparators and differentials
- Reciprocal roles + traps/dilemmas/snags
- Letter + SDR map + goodbye
- Brief collaborative contract (often 8–24 sessions)
- Automatic thoughts, behaviours, experiments
- Thought records / behavioural activation tools
- Less emphasis on RRP letters by default
- Primary aim: restore mentalising under arousal
- Not-knowing stance; pre-mentalising modes
- Classic dual individual + group format
Also distinguish schema therapy (early maladaptive schemas/modes, often longer) and IPT (medical-model four problem areas for mood) — related interpersonal aims, different manuals and tools.[3]
Landmark evidence
Personality disorder and early intervention
- Chanen et al. 2008 (BJP): RCT of CAT versus manualised good clinical care (GCC) within a specialised early-intervention service for adolescents with subthreshold or full borderline personality features. Both arms improved; CAT was associated with more rapid improvement on some trajectories — teach “both structured approaches help; CAT may accelerate change,” not “CAT always uniquely wins.”[1]
- Clarke et al. 2013 (BJP): RCT of 24-session CAT versus treatment-as-usual for personality disorder — CAT superior on key outcomes in the trial analysis for this complex adult group.[2]
- Ryle and Golynkina 2000: open effectiveness of time-limited CAT for BPD with factors associated with outcome — foundational practice-based evidence.[6]
- Kellett et al. 2013: competence and therapeutic effectiveness of CAT for BPD in routine practice, with fidelity attention — bridges research to real services.[5]
- Ryle 2004: model paper on CAT’s contribution to BPD treatment and management, including self-state mapping language.[11]
Eating disorders, medical illness, synthesis
- Treasure et al. 1995: pilot randomised comparison of CAT versus educational behavioural treatment for adult anorexia nervosa — early specialised psychotherapy signal.[7]
- Dare et al. 2001: multi-arm outpatient psychotherapy RCT for adult anorexia nervosa (includes specialist psychotherapies in the historical CAT-relevant landscape) — know adult AN needs structured psychological treatment plus medical care.[8]
- Fosbury et al. 1997 (Diabetes Care): CAT versus diabetes specialist nurse education in poorly controlled type 1 diabetes — relational procedures can affect self-management outcomes.[9]
- Calvert and Kellett 2014: structured review of CAT outcome evidence quality and gaps.[3]
- Hallam et al. 2021: systematic review and meta-analysis supporting acceptability, effectiveness, and durability signals across presentations, with acknowledged heterogeneity and need for more high-quality trials.[4]
- Simmonds-Buckley et al. 2022: meta-analysis of refusal and dropout — CAT often shows relatively favourable engagement (dropout on the order of the high teens percent in pooled estimates; lower than some comparators in head-to-heads).[10]
Pitfalls, special populations, prognosis
Special populations. Adolescents: HYPE-style early intervention with CAT is examinable in ANZ teaching.[1] Perinatal: prioritise safety, bonding, and sleep; map roles carefully. Cultural care: co-create role language that respects kinship and collective selfhood. Neurodivergence: simplify maps; do not confuse lifelong communication difference with procedural traps alone. Medical illness: keep physicians in the loop (diabetes, eating disorders).[7][9]
Prognosis and disposition. Meta-analytic and trial data support clinically meaningful gains for many completers, with durability signals in synthesis, but response is individual. Engagement, alliance, substance use, medical stability, and therapist competence influence outcome. Plan step-down, crisis pathways, and honest waitlist discussion when CAT is scarce.[4][10]
Regional practice notes
ANZ (FRANZCP). CAT appears in some public psychotherapy and youth early-intervention (HYPE-influenced) pathways. Examiners expect: define tools/phases, cite Chanen thoughtfully, offer structured alternatives when CAT unavailable, and avoid inventing Mental Health Act section numbers.[1][3]
UK (MRCPsych). CAT is a familiar UK-origin model (ACAT training tradition). CASC stations often test plain-language explanation of the map, collaborative stance, and ending. NICE emphasises structured psychological therapies for PD and depression; CAT may be available locally without being the only named first-line brand everywhere.[2][3][4]
US (ABPN). CAT is less ubiquitous than CBT/DBT/MBT in many services. Know the model as an integrative brief relational therapy with growing evidence, and match available specialised programmes to formulation and preference.[3][4]
Exam pearls
CAT core package
Target procedures
Do not confuse CAT with CBT because both contain “cognitive.” Quote Chanen 2008 (youth early intervention; both CAT and GCC help) and Clarke 2013 (adult PD CAT vs TAU). Mention Hallam 2021 and Simmonds-Buckley 2022 for synthesis and engagement. Ending is high-yield: goodbye letters prevent unprocessed abandonment enactments. Safety always overrides elective mapping.[1][2][4][10]
References
See frontmatter PMIDs (title/year verified). Landmark anchors: Chanen 2008; Clarke 2013; Calvert and Kellett 2014; Hallam 2021; Kellett 2013; Ryle and Golynkina 2000; Treasure 1995; Dare 2001; Fosbury 1997; Simmonds-Buckley 2022; Ryle 2004.[1][2][4]
References
- [1]Chanen AM, Jackson HJ, McCutcheon LK, et al. Early intervention for adolescents with borderline personality disorder using cognitive analytic therapy: randomised controlled trial Br J Psychiatry, 2008.PMID 19043151
- [2]Clarke S, Thomas P, James K Cognitive analytic therapy for personality disorder: randomised controlled trial Br J Psychiatry, 2013.PMID 23222038
- [3]Calvert R, Kellett S Cognitive analytic therapy: a review of the outcome evidence base for treatment Psychol Psychother, 2014.PMID 24610564
- [4]Hallam C, Simmonds-Buckley M, Kellett S, et al. The acceptability, effectiveness, and durability of cognitive analytic therapy: Systematic review and meta-analysis Psychol Psychother, 2021.PMID 32543107
- [5]Kellett S, Bennett D, Ryle T, Thake A Cognitive analytic therapy for borderline personality disorder: therapist competence and therapeutic effectiveness in routine practice Clin Psychol Psychother, 2013.PMID 22109975
- [6]Ryle A, Golynkina K Effectiveness of time-limited cognitive analytic therapy of borderline personality disorder: factors associated with outcome Br J Med Psychol, 2000.PMID 10874479
- [7]Treasure J, Todd G, Brolly M, et al. A pilot study of a randomised trial of cognitive analytical therapy vs educational behavioural therapy for adult anorexia nervosa Behav Res Ther, 1995.PMID 7755523
- [8]Dare C, Eisler I, Russell G, et al. Psychological therapies for adults with anorexia nervosa: randomised controlled trial of out-patient treatments Br J Psychiatry, 2001.PMID 11230031
- [9]Fosbury JA, Bosley CM, Ryle A, et al. A trial of cognitive analytic therapy in poorly controlled type I patients Diabetes Care, 1997.PMID 9167106
- [10]Simmonds-Buckley M, Osivwemu EO, Kellett S, Taylor C The acceptability of cognitive analytic therapy (CAT): Meta-analysis and benchmarking of treatment refusal and treatment dropout rates Clin Psychol Rev, 2022.PMID 35914380
- [11]Ryle A The contribution of cognitive analytic therapy to the treatment of borderline personality disorder J Pers Disord, 2004.PMID 15061342