Psych · psychotherapy
Combining psychotherapy and pharmacotherapy
Also known as Combined treatment · Combination therapy psychiatry · Integrated psychotherapy pharmacotherapy · Sequential treatment residual depression · Adjunctive CBT · Concurrent medication and therapy
Exam-exhaustive fellowship reference on combining psychotherapy and pharmacotherapy — concurrent vs sequential models, landmark trials (Keller CBASP, TADS, CAMS, POTS, CoBalT, STEP-BD), meta-analytic evidence, care models, pitfalls, and shared decision-making. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Examiners (FRANZCP MEQ/clinical, MRCPsych Paper B/CASC, ABPN, MD/DNB viva) test whether you can hold both medical and psychological frames: when monotherapies are equivalent, when combination is superior, when sequential residual-symptom work is smarter than more polypharmacy, and when acute risk makes elective therapy secondary.[8][9][15]
Definition and models
What counts as combination
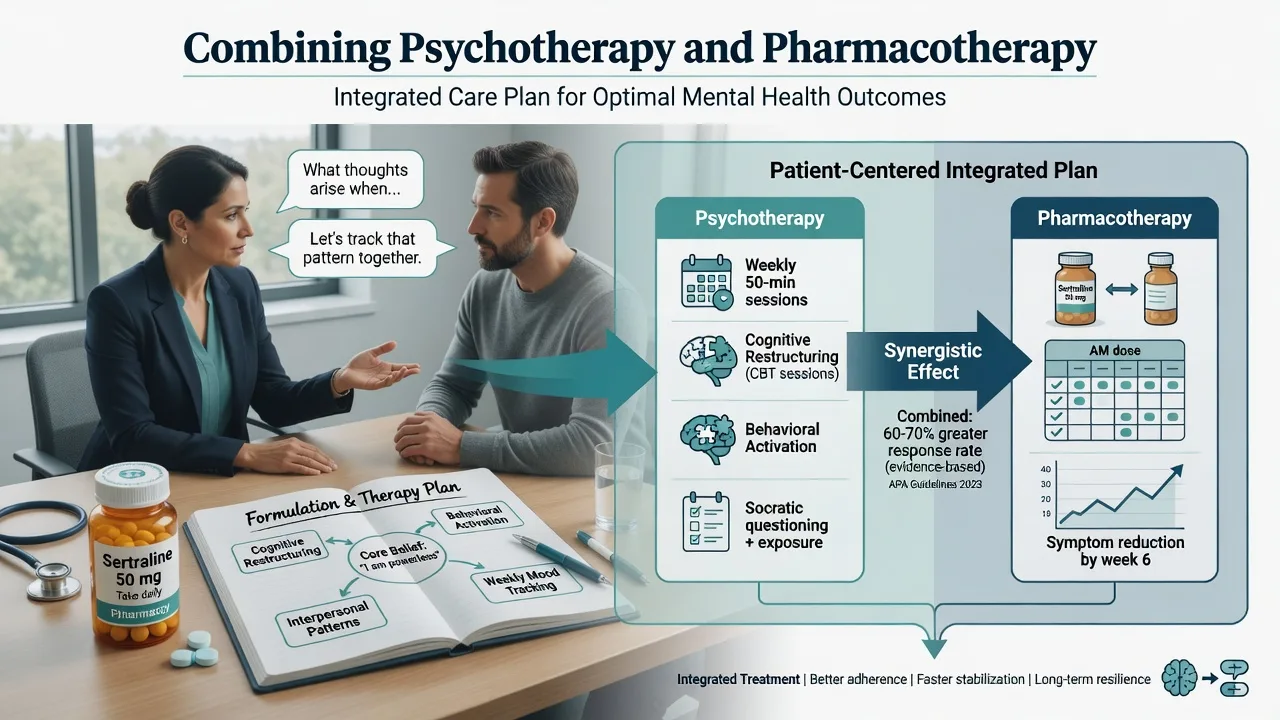
True combination requires an evidence-informed psychological intervention (for example CBT, IPT, CBASP, ERP, family intervention, CBTp) plus pharmacotherapy with adequate dose, duration, and monitoring. Monthly unstructured support while prescribing is not exam-standard “combined CBT.”[3][5]
| Model | Core idea | Typical use |
|---|---|---|
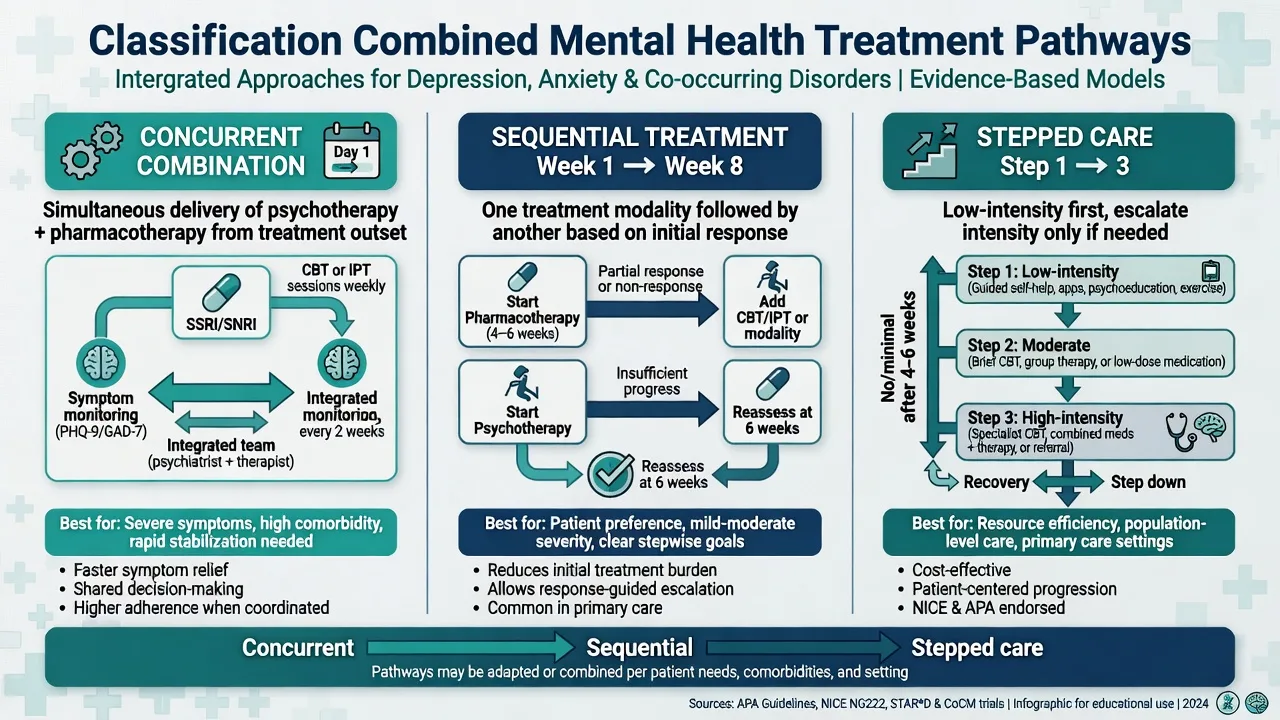
| Concurrent | Both start (or run) in the same acute phase | Moderate–severe MDD, chronic depression, youth anxiety/depression/OCD |
| Sequential | One modality first; second targets residual symptoms, well-being, or relapse prevention after response | After antidepressant response with residual symptoms; step-down from intensive care |
| Stepped care | Intensity rises with severity/non-response | Mild → guided self-help/therapy; higher steps → meds ± therapy |
| Integrated/collaborative | Shared formulation, measures, and team communication | Primary care collaborative care; CMHT packages |
Intent of combination (name it in viva)
- Acute efficacy — higher response/remission than one modality alone.[1][3][4]
- Adherence and engagement — therapy supports medication use and vice versa.
- Relapse prevention — skills after acute response; maintenance medication when recurrence risk is high.[9][16]
- Residual symptoms / functioning — sequential psychotherapy after pharmacologic response.[15][18][20]
- Disorder-specific non-negotiables — mood stabiliser backbone in bipolar; antipsychotics primary in schizophrenia with psychosocial adjuncts.[14][17]
Mechanisms (complementary framing)
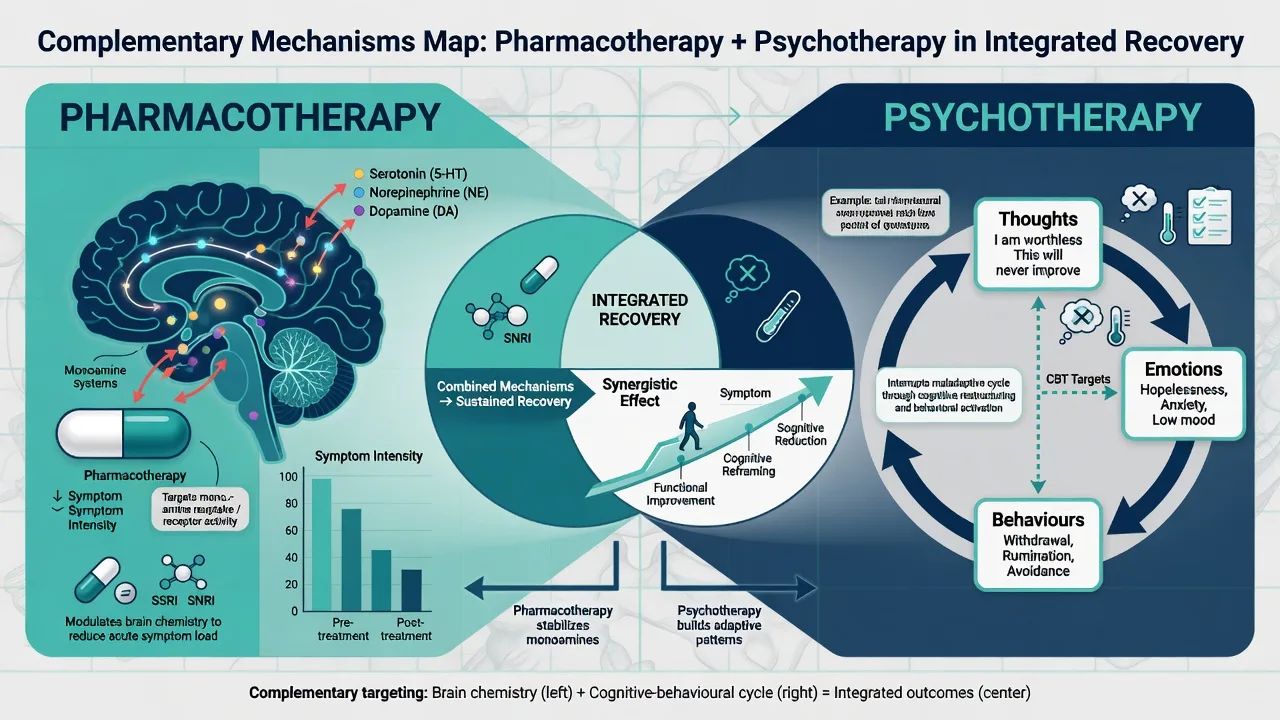
Pharmacotherapy typically reduces symptom intensity, sleep/appetite disruption, and physiological arousal that can make psychological work possible. Psychotherapy targets maintaining cycles: avoidance, safety behaviours, rumination, interpersonal patterns, skill deficits, trauma memory processing, and relapse-prevention repertoires. Examiners want this complementary map — not speculative neurobabble about “rewiring the brain” as doctrine.[5][19]
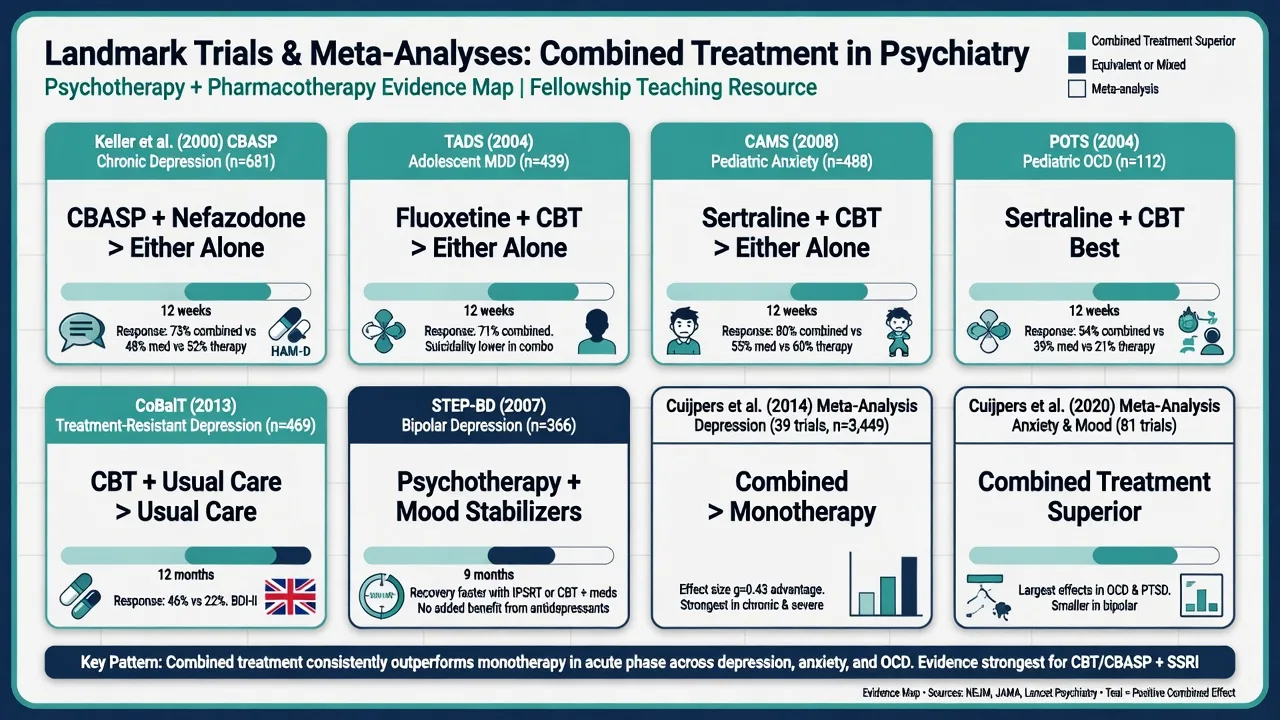
In chronic depression, CBASP specifically targets interpersonal–environmental maintaining factors while antidepressant treatment addresses neurovegetative burden; combination outperformed either alone in the landmark Keller trial.[1] In anxiety, SSRIs/SNRIs may lower baseline anxiety while exposure/ERP drives inhibitory learning; standing benzodiazepines often function as safety behaviours that prevent disconfirmation of threat beliefs.[19]
Epidemiology and practice reality
Combined regimens are common once severity, chronicity, or partial response rise. Access barriers to high-fidelity psychotherapy mean many patients receive medication monotherapy by default — an access problem, not evidence that therapy is unnecessary.[3][4] Incomplete delivery (subtherapeutic SSRI dose/duration; “CBT” without agenda, homework, or exposure) is frequently misread as combination failure.[5]
Assessment for combined care
Clinical questions that change the plan
- Diagnosis and differential — unipolar vs bipolar, substance, organic, personality, psychosis.
- Severity and risk — suicide, self-neglect, mania, incapacity.
- Chronicity and residual symptoms — Keller and sequential-model territory.[1][15]
- Prior trials — which drugs, dose, duration, side effects; which therapy, modality, fidelity, homework.
- Preference, culture, literacy, access, cost.
- Care model — single provider vs split care communication plan.
Measures and documentation
Use disorder-appropriate scales (PHQ-9, GAD-7, Y-BOCS, CDRS-R, etc.) and who owns the review. Document: shared goals; current regimen with dose/route; therapy modality and session structure; homework/exposure tasks; side effects; risk plan.[13][18]
Acute / emergency priorities
Elective combination planning does not override medical emergencies or acute risk containment: high suicide risk needing secure care, severe self-neglect, mania, catatonia, NMS, serotonin syndrome, lithium toxicity, delirium. Stabilise first; short problem-solving and safety planning can run in parallel with acute pharmacologic care. Do not delay emergency intervention to finish a thought record. Acute risk always outranks elective session structure in combined-care planning.[13][14]
Definitive management by syndrome
Adult major depression
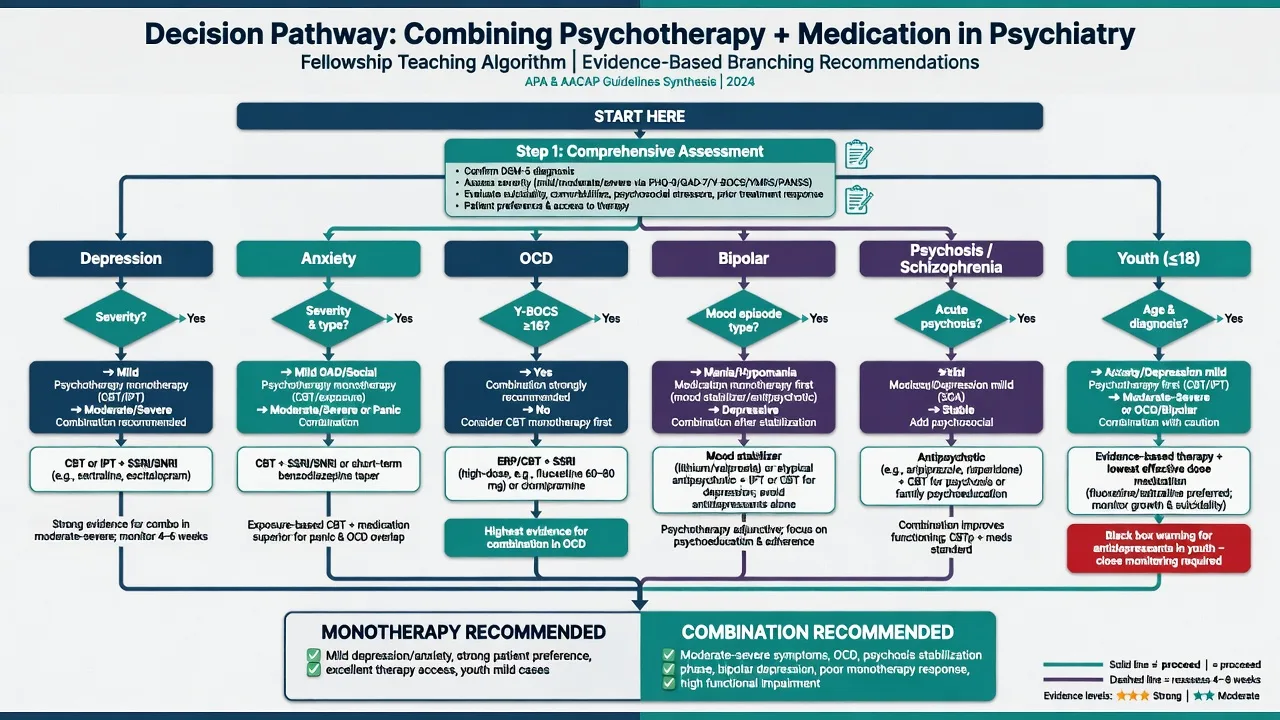
Acute moderate–severe MDD. Cognitive therapy can match medications for initial treatment when delivered competently.[8] After response, patients discontinuing medication relapse more than those who received CT and then discontinue active treatment — durable skills matter.[9]
Adding therapy to antidepressants. Meta-analysis shows combined treatment more effective than antidepressant medication alone across depression and several anxiety disorders.[3] Network meta-analysis finds combination superior to psychotherapy alone and pharmacotherapy alone for adult depression.[4] Earlier systematic review similarly favoured combination for improvement rates, with longer treatments mattering.[7] Large CBT syntheses position CBT among first-line psychological options and place combined treatment in the high-efficacy set for depression.[5] Functioning and quality of life also improve, with combination often superior.[18]
Treatment-resistant depression in primary care. CoBalT: CBT as an adjunct to usual care including antidepressants improved outcomes versus usual care alone for patients with inadequate antidepressant response.[13]
Example prescribing context (illustrative, cite nearby). For a first-line SSRI pathway in moderate–severe MDD, a common adult start is sertraline 50 mg oral daily, titrate by clinical response and tolerability toward an effective range (often 50–200 mg daily), review side effects, suicide risk early in treatment, and sexual/gastrointestinal effects, with planned duration and therapy goals documented — combination does not waive monitoring standards.[8][13]
Chronic / persistent depression
Keller and colleagues randomised chronic nonpsychotic major depression to nefazodone, CBASP, or both. Combination produced substantially higher remission/response rates than either monotherapy at 12 weeks — the classic exam anchor for chronic depression combination.[1] For non-responders, switching modality (medication ↔ CBASP) can still help.[2] (Nefazodone itself is largely historical because of hepatotoxicity; the design lesson — structured chronic-depression psychotherapy plus antidepressant strategy — remains examinable.)
Sequential residual-symptom model
After pharmacologic response, residual symptoms predict relapse. Sequential addition of psychotherapy (including well-being-oriented approaches in the Fava–Guidi tradition) reduces residual burden and recurrence risk compared with clinical management alone in meta-analytic synthesis.[15][20] This is the answer when the examiner asks: “response on meds, still not well — more polypharmacy or something else?”
Maintenance after recurrent depression
Classic Pittsburgh maintenance work: full-dose maintenance imipramine was highly effective against recurrence; monthly maintenance IPT had intermediate benefit; combination of full-dose imipramine plus IPT was among the strongest conditions in the three-year design — teaching point that maintenance pharmacotherapy dose and psychological maintenance both matter after highly recurrent illness.[16]
Anxiety disorders
Direct comparisons of psychotherapy vs antidepressants show broadly similar efficacy for many anxiety presentations; choice often turns on preference, access, comorbidity, and prior response.[6] Adding pharmacotherapy to CBT can improve short-term severity versus CBT plus placebo, with less clear durable advantage at follow-up — useful nuance for viva.[19] Prefer SSRIs/SNRIs over chronic benzodiazepines when combining with exposure-based CBT.
Youth depression (TADS)
Four arms: fluoxetine, CBT, combination, placebo. Combination offered the best benefit–risk trade-off; fluoxetine alone beat CBT alone acutely; CBT-containing arms were relevant to suicidal thinking trajectories in the programme narrative.[10] Fluoxetine dosing in TADS was in the 10–40 mg oral daily range under protocol titration — always couple youth prescribing with risk monitoring and family engagement.[10]
Youth anxiety (CAMS)
CBT, sertraline (up to 200 mg oral daily in protocol), combination, or placebo. Combination had the highest response rates; both monotherapies beat placebo.[11]
Youth OCD (POTS)
CBT, sertraline, combination, placebo. Combination and CBT were superior; sertraline alone intermediate — supports prioritising CBT/ERP access and combining when severity or partial response demands.[12]
Bipolar depression
Intensive psychosocial treatments (family-focused therapy, IPSRT, CBT) as adjuncts to pharmacotherapy improved recovery from bipolar depression versus brief collaborative care in the Systematic Treatment Enhancement Program bipolar trial — psychotherapy is additive, not alternative, to mood-stabilising medication.[14]
Psychosis
CBTp has modest beneficial effects on positive symptoms in meta-analysis and is adjunctive; family intervention and other psychosocial packages sit alongside antipsychotics. Do not frame psychological therapy as licence to stop indicated antipsychotic treatment.[17]
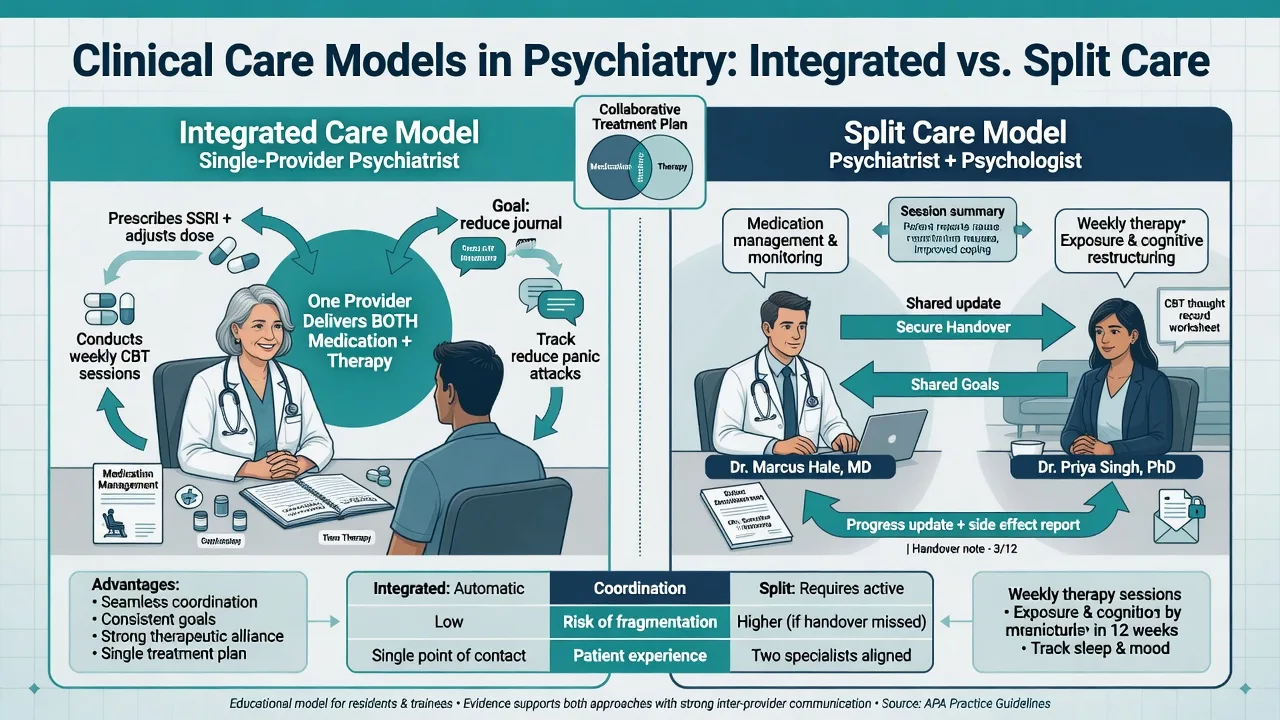
Care models: single provider vs split care
| Issue | Single psychiatrist | Split (prescriber + therapist) |
|---|---|---|
| Formulation | One mind; risk of medical or therapy bias | Must be shared in writing |
| Communication | Internal | Explicit: goals, risk, side effects, homework conflicts |
| Boundary | Dual role intensity | Role clarity protects frame |
| Failure mode | Over-medicalising or under-prescribing | Conflicting messages; no one owns risk |
Patients need one coherent story: what the tablets do, what the sessions train, how progress is measured, and what to do in crisis.[13][14]
Complications and pitfalls
- False dichotomy — “meds or therapy.” Evidence supports both monotherapies and combination as context-dependent tools.[6][4]
- Pseudo-combination — prescribing plus non-specific support labelled as CBT.[5]
- Benzodiazepine talismans during exposure.[19]
- Premature polypharmacy when high-fidelity therapy was never tried (or the reverse: endless therapy without indicated medication in severe illness).[3][13]
- Ignoring residual symptoms after numeric “response.”[15][20]
- CBTp or bipolar psychosocial care without medical backbone.[14][17]
- Cultural meanings — medication as weakness; therapy as only for the “psychologically minded.”
Prognosis and disposition
Combined treatment often improves acute outcomes and functioning versus monotherapy pathways in depression syntheses.[3][4][18] Disposition ladders: GP collaborative care → outpatient combined specialist care → CMHT for complexity/risk → brief admission for acute risk. Step-down: continue the modality carrying relapse-prevention value (maintenance meds after multiple recurrences; booster therapy sessions; sequential residual work).[15][16]
Special populations
Youth. Use TADS/CAMS/POTS hierarchies; involve caregivers; monitor activation and suicidal ideation when starting antidepressants.[10][11][12]
Older adults. Medical comorbidity, drug–drug interactions, slower titration; psychotherapy adaptations for pacing and sensory load. Combined treatment principles still apply with higher interaction vigilance.[3][18]
Perinatal. Shared decision-making; accessible psychotherapy is often prioritised when mild–moderate and available; medication risk–benefit for moderate–severe illness remains a medical decision.[3][6]
Intellectual disability / neurodevelopmental. Behavioural emphasis, carer coaching, simplified cognitive work, careful dosing; combination still requires clear goals and monitoring.[5]
Indigenous and culturally diverse communities. Cultural formulation of both medication and therapy meanings; interpreter use; community supports; avoid assuming one Western model fits all.[3]
Evidence and guideline deltas
NICE-style stepped care emphasises psychological therapies early for many common mental disorders and combination or more intensive packages as severity/complexity rises. APA guidance supports evidence-based psychotherapies and pharmacotherapies, with combination for selected presentations. RANZCP training expects competence across biological treatment and psychological therapies — examiners dislike one-track answers. ANZ service reality: waiting lists for CBT/ERP often drive interim medication; document the plan to add therapy, not pretend access equals non-indication.[3][4][5]
Landmark set for recall: Keller CBASP combination; Schatzberg switch; Cuijpers direct, add-on, network, and CBT mega-analyses; Pampallona; DeRubeis/Hollon; CoBalT; Guidi–Fava sequential; Frank maintenance; TADS; CAMS; POTS; Miklowitz bipolar psychosocial trial; Hofmann anxiety add-on; Wykes CBTp; Kamenov functioning.[1][3][4][10][11][12][13][14][15]
Exam pearls
- Combination is a named strategy with intent (acute boost, residual symptoms, relapse prevention, adherence), not a reflex.[3][4]
- Keller = chronic depression, combination wins.[1]
- DeRubeis = CT ≈ meds acutely moderate–severe; Hollon = CT more durable after discontinuation of active treatment.[8][9]
- CoBalT = adjunctive CBT for antidepressant-resistant primary-care depression.[13]
- Guidi–Fava = sequential psychotherapy after pharmacologic response.[15]
- TADS / CAMS / POTS = youth combination hierarchies.[10][11][12]
- Miklowitz bipolar psychosocial trial = intensive therapy adjunct to meds for bipolar depression.[14]
- Never drop antipsychotics for CBTp; never mood-stabiliser-free bipolar “therapy only.”[14][17]
- Inadequate fidelity is not evidence against combination.[5]
References
- [1]Keller MB, McCullough JP, Klein DN, et al. A comparison of nefazodone, the cognitive behavioral-analysis system of psychotherapy, and their combination for the treatment of chronic depression N Engl J Med, 2000.PMID 10816183
- [2]Schatzberg AF, Rush AJ, Arnow BA, et al. Chronic depression: medication (nefazodone) or psychotherapy (CBASP) is effective when the other is not Arch Gen Psychiatry, 2005.PMID 15867104
- [3]Cuijpers P, Sijbrandij M, Koole SL, et al. Adding psychotherapy to antidepressant medication in depression and anxiety disorders: a meta-analysis World Psychiatry, 2014.PMID 24497254
- [4]Cuijpers P, Noma H, Karyotaki E, et al. A network meta-analysis of the effects of psychotherapies, pharmacotherapies and their combination in the treatment of adult depression World Psychiatry, 2020.PMID 31922679
- [5]Cuijpers P, Miguel C, Harrer M, et al. Cognitive behavior therapy vs. control conditions, other psychotherapies, pharmacotherapies and combined treatment for depression: a comprehensive meta-analysis including 409 trials with 52,702 patients World Psychiatry, 2023.PMID 36640411
- [6]Cuijpers P, Sijbrandij M, Koole SL, et al. The efficacy of psychotherapy and pharmacotherapy in treating depressive and anxiety disorders: a meta-analysis of direct comparisons World Psychiatry, 2013.PMID 23737423
- [7]Pampallona S, Bollini P, Tibaldi G, et al. Combined pharmacotherapy and psychological treatment for depression: a systematic review Arch Gen Psychiatry, 2004.PMID 15237083
- [8]DeRubeis RJ, Hollon SD, Amsterdam JD, et al. Cognitive therapy vs medications in the treatment of moderate to severe depression Arch Gen Psychiatry, 2005.PMID 15809408
- [9]Hollon SD, DeRubeis RJ, Shelton RC, et al. Prevention of relapse following cognitive therapy vs medications in moderate to severe depression Arch Gen Psychiatry, 2005.PMID 15809409
- [10]March J, Silva S, Petrycki S, et al. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents With Depression Study (TADS) randomized controlled trial JAMA, 2004.PMID 15315995
- [11]Walkup JT, Albano AM, Piacentini J, et al. Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety N Engl J Med, 2008.PMID 18974308
- [12]Pediatric OCD Treatment Study (POTS) Team Cognitive-behavior therapy, sertraline, and their combination for children and adolescents with obsessive-compulsive disorder: the Pediatric OCD Treatment Study (POTS) randomized controlled trial JAMA, 2004.PMID 15507582
- [13]Wiles N, Thomas L, Abel A, et al. Cognitive behavioural therapy as an adjunct to pharmacotherapy for primary care based patients with treatment resistant depression: results of the CoBalT randomised controlled trial Lancet, 2013.PMID 23219570
- [14]Miklowitz DJ, Otto MW, Frank E, et al. Psychosocial treatments for bipolar depression: a 1-year randomized trial from the Systematic Treatment Enhancement Program Arch Gen Psychiatry, 2007.PMID 17404119
- [15]Guidi J, Fava GA Sequential Combination of Pharmacotherapy and Psychotherapy in Major Depressive Disorder: A Systematic Review and Meta-analysis JAMA Psychiatry, 2021.PMID 33237285
- [16]Frank E, Kupfer DJ, Perel JM, et al. Three-year outcomes for maintenance therapies in recurrent depression Arch Gen Psychiatry, 1990.PMID 2244793
- [17]Wykes T, Steel C, Everitt B, Tarrier N Cognitive behavior therapy for schizophrenia: effect sizes, clinical models, and methodological rigor Schizophr Bull, 2008.PMID 17962231
- [18]Kamenov K, Twomey C, Cabello M, et al. The efficacy of psychotherapy, pharmacotherapy and their combination on functioning and quality of life in depression: a meta-analysis Psychol Med, 2017.PMID 27780478
- [19]Hofmann SG, Sawyer AT, Korte KJ, Smits JA Is it Beneficial to Add Pharmacotherapy to Cognitive-Behavioral Therapy when Treating Anxiety Disorders? A Meta-Analytic Review Int J Cogn Ther, 2009.PMID 19714228
- [20]Fava GA, Tomba E New modalities of assessment and treatment planning in depression: the sequential approach CNS Drugs, 2010.PMID 20443645