Psych · psychotherapy
Couples therapy
Also known as Couple therapy · Marital therapy · Relationship therapy · Conjoint therapy · Behavioural couples therapy · BCT · IBCT · TBCT · Emotionally focused couple therapy · EFT for couples
Exam-exhaustive fellowship reference on couples therapy — major models (TBCT, IBCT, CBCT, EFT, insight-oriented), assessment and IPV safety rules, bidirectional link with psychopathology, landmark evidence for relationship distress, depression, SUD and PTSD conjoint packages, combined care, and CASC/MEQ technique. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Examiners want you to screen for safety, choose a model for formulation, cite meta-analytic and landmark RCT evidence, and know when conjoint work is contraindicated — especially active IPV, acute high risk, or untreated severe individual illness needing medical priority.[2][8][13]

Definition and scope
Couples therapy is not mediation, legal counselling, or unstructured advice-giving. It is a clinical intervention with assessment, formulation, session structure, homework or between-session experiments, and outcome monitoring. Historical labels include marital therapy and behavioural marital therapy (BMT); contemporary language prefers couple or relationship therapy to include cohabiting, same-sex, and gender-diverse partnerships without pathologising identity.[1][15]
Two clinical targets (exam-critical)
- Primary relationship distress — dissatisfaction, conflict, consideration of separation, sexual/intimacy problems, attachment injuries (e.g. after betrayal).
- Disorder-specific conjoint work — partner included deliberately to treat depression, alcohol/other substance use disorders, PTSD, or other syndromes while also improving the relationship.[16][7][10]
What couples therapy is and is not
| Couples therapy is | Couples therapy is not |
|---|---|
| Dual-client structured treatment | One partner “fixing” the other while the therapist takes sides |
| Compatible with individual therapy and medication | A substitute for acute risk containment or mania treatment |
| Model-based (behavioural, integrative, attachment, cognitive) | Purely legal separation coaching |
| Dependent on safety and consent of both | Standard care when active IPV makes conjoint problem-solving dangerous |
| Outcome-measurable (DAS/CSI + symptom scales) | Endless unfocused chat without mid-course review |
Epidemiology and the psychopathology link
Population data show marital distress is associated with elevated rates of mood, anxiety, and substance use disorders — not a trivial lifestyle complaint sitting outside psychiatry.[13] Relationship discord and depressive symptoms show a bidirectional association: discord precipitates and maintains depression; depression degrades role performance, intimacy, and problem-solving, worsening discord.[13][7]
Access reality: fewer clinicians have supervised couple therapy competence than individual CBT competence in many public services; fidelity and waiting lists matter for realistic disposition plans.[15]
Mechanisms (pathophysiology of distress)
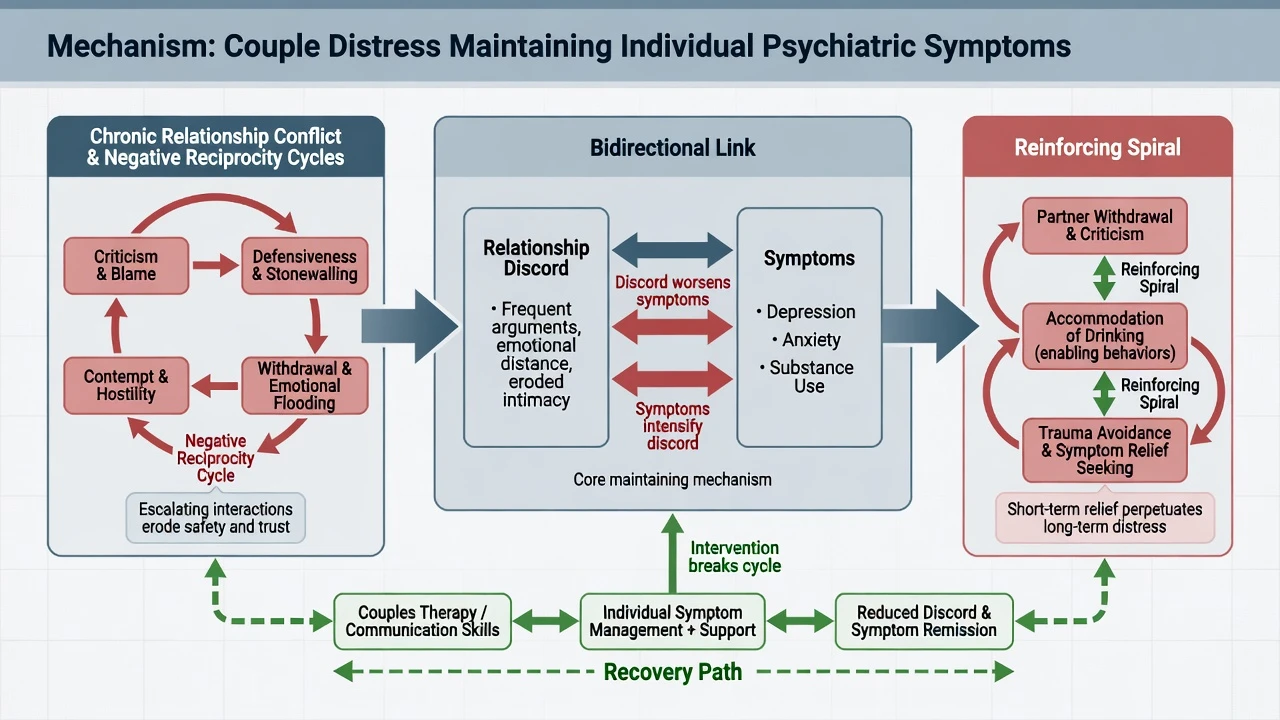
Behavioural / social learning (TBCT frame)
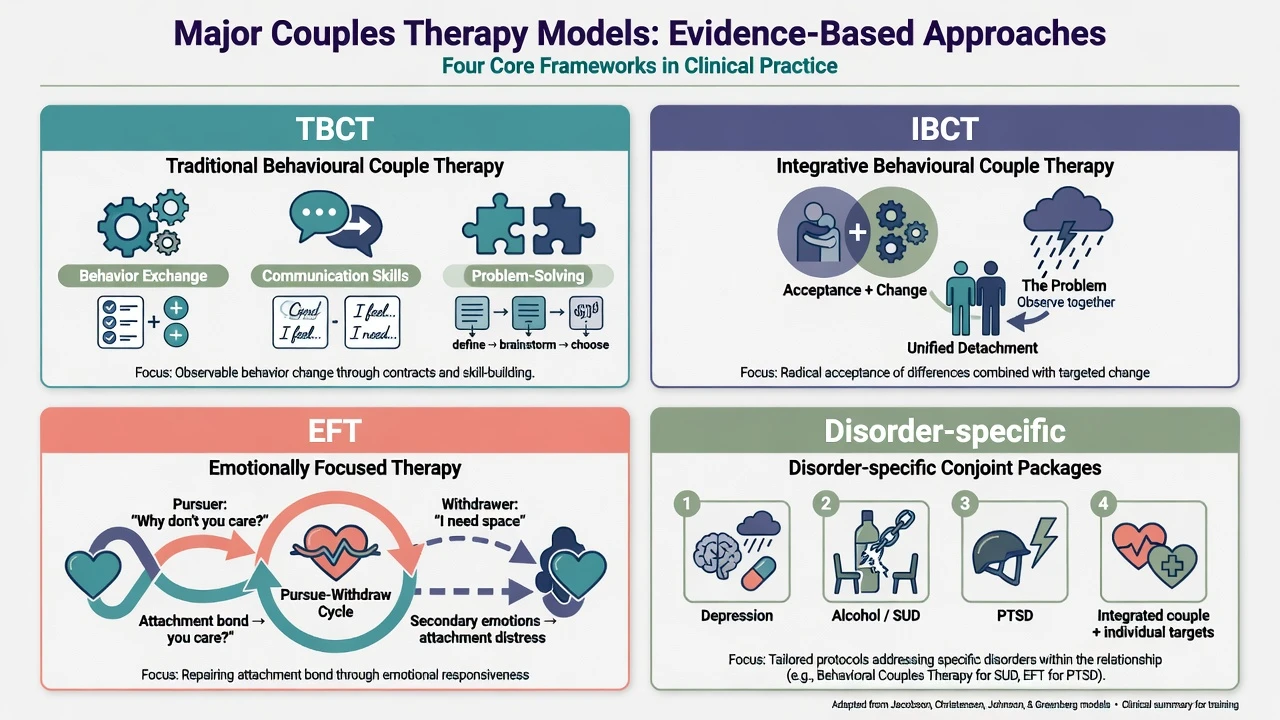
Distressed couples show low rates of positive reinforcement, negative reciprocity (criticism begets counter-attack), and coercive cycles. Traditional behavioural couple therapy builds behaviour exchange, communication skills, and problem-solving to increase positive exchange and reduce aversive sequences.[1][3]
IBCT: acceptance plus change
Integrative behavioural couple therapy retains change strategies but adds acceptance processes: empathic joining around soft emotions, unified detachment (observing the pattern as a shared problem), and tolerance of differences that will not fully change. Polarisation and the “mutual trap” are central clinical metaphors.[4][5]
Attachment / EFT
Emotionally focused couple therapy targets pursue–withdraw cycles: secondary reactive anger or shutdown masks primary attachment fears. Stages move from de-escalation of the negative cycle → restructuring bonding interactions → consolidation of a more secure bond.[14]
Cognitive couple models
Partners of distressed couples often show hostile attributions (“they meant to hurt me”), selective attention to negatives, and rigid dyadic rules. Cognitive-behavioural couple therapy works these appraisals alongside behavioural skills.[1][16]
Major models (classification)
| Model | Core emphasis | Exam pearl |
|---|---|---|
| TBCT / BMT | Behaviour exchange, communication, problem-solving | Strong RCT/meta-analytic support for distress.[3][1] |
| IBCT | Acceptance + targeted change; unified detachment | RCT vs TBCT in chronically distressed couples; long follow-up.[4][5] |
| CBCT | Cognitions + behavioural skills | Overlaps TBCT; used broadly and in disorder packages.[16] |
| EFT | Attachment bonding, cycle de-escalation | Attachment-process evidence base summarised in reviews.[14] |
| Insight-oriented marital therapy | Affective insight, developmental themes | Classic comparison with BMT; long-term follow-up data.[6] |
| Disorder-specific | Depression-focused, BCT-SUD, CBCT-PTSD | Partner as co-therapist of recovery, not only of “marriage.”[8][11][12] |
Assessment bedside checklist
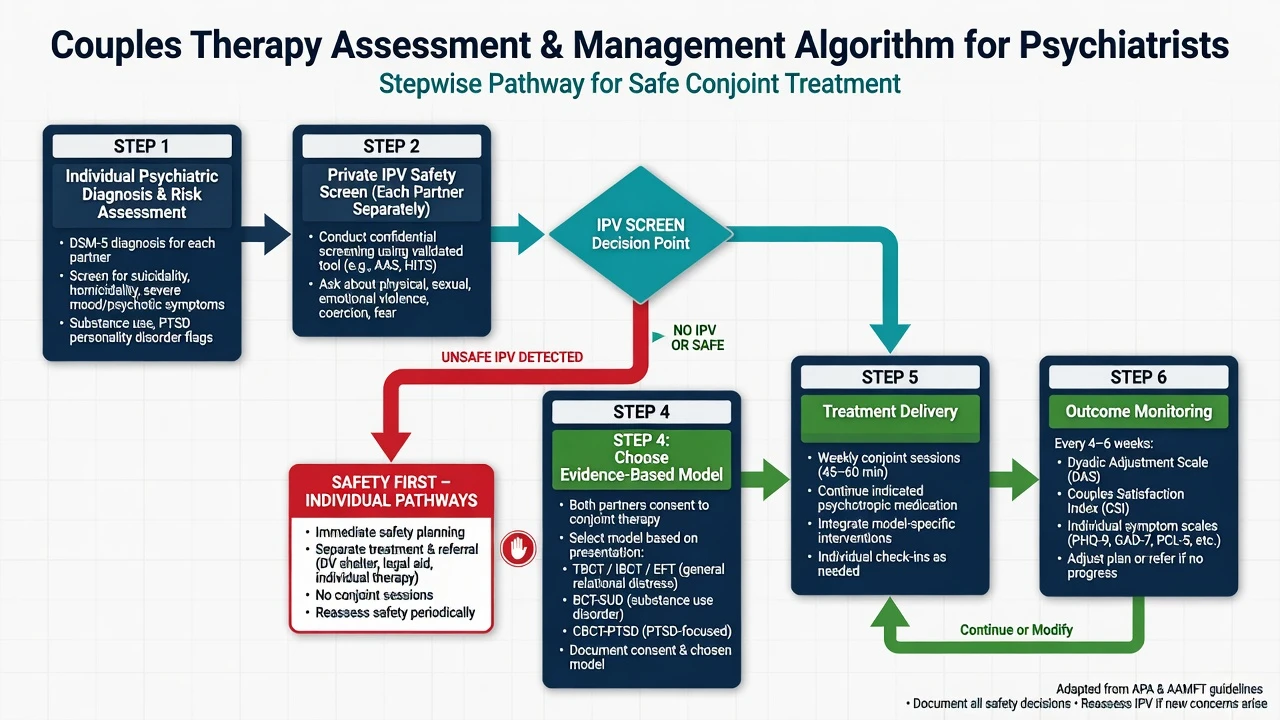
- Individual psychiatric diagnosis for each partner (mood, anxiety, psychosis, personality, neurocognitive).
- Risk: suicide, violence, self-neglect, safeguarding, children at risk.
- Private IPV/coercive control screen — each partner alone before committing to conjoint problem-solving.
- Substance use including partner accommodation (covering, buying, arguing as maintenance).
- Relationship history: courtship, strengths, conflict topography, affairs, separations, sexual intimacy, parenting.
- Goals and commitment: both agendas; separation ambivalence; secrets policy (what is confidential if one emails alone).
- Measures: relationship (e.g. DAS, CSI) and symptoms (PHQ-9, GAD-7, AUDIT, PCL-5 as indicated).
- Cultural formulation: gender roles, religion, family hierarchy, minority stress, migration strain.[15][13][16]
Acute / emergency priorities
- Active IPV with ongoing threat, stalking, or fear of severe retaliation → individual safety planning and domestic-violence pathways; do not run standard assertiveness homework that increases danger.[15]
- High suicide risk, mania/mixed states, delirium, severe intoxication → medical/psychiatric containment first.
- If a partner discloses violence privately, do not force confrontation in the joint room that day; document, safety-plan, follow local reporting rules.[15]
Definitive management algorithm
Frame and “dose”
Typical outpatient courses use weekly conjoint sessions over months (often roughly 8–20+ depending on model and severity), with mid-course review. State goals, approximate length, homework expectations, and cancellation rules. Parallel individual therapy is common when one partner has moderate–severe illness.[15][1]
Model techniques (high-yield)
- TBCT: increase positive behaviours (caring days, behaviour exchange contracts); speaker–listener communication skills; structured problem-solving (define → brainstorm → choose → implement → review).[3]
- IBCT: formulate polarisation; foster empathic joining; teach unified detachment (“the pattern is the enemy”); selective change strategies for solvable problems.[4]
- EFT: map the negative cycle; access primary emotions; create new bonding events; consolidate.[14]
- BCT for SUD: daily sobriety trust discussion, recovery contract, shared activities incompatible with use, communication/problem-solving around recovery stressors — not only “talk about feelings.”[10][11]
- CBCT for PTSD: structured conjoint protocol targeting PTSD symptoms and relationship functioning together (Monson package).[12]
Combined care with medication
Couples therapy is compatible with antidepressants, anti-craving agents, mood stabilisers, and PTSD pharmacotherapy. Do not stop indicated medication because couple sessions start. For moderate–severe depression, treat the syndrome (medication and/or individual evidence-based therapy) and address discord when present.[8][9][16]
Evidence base (landmarks)
Relationship distress overall
Meta-analytic reviews of marital and family interventions support efficacy for distressed couples, with clinically meaningful recovery rates in a substantial minority to half of treated cases in classic syntheses; differences among bona fide models are often modest at the meta-analytic level.[2][1] Behavioural marital therapy has a dedicated RCT meta-analysis supporting benefit versus no-treatment controls.[3] Contemporary status reviews reaffirm that cognitive-behavioural, integrative behavioural, and emotionally focused approaches each have sufficient evidence to be considered well-established for relationship distress.[15]
TBCT vs IBCT (Christensen)
In significantly and chronically distressed married couples, a randomised trial compared TBCT and IBCT — both improved satisfaction substantially; process and trajectory differences inform model choice more than a slogan of “one always wins.”[4] Five-year follow-up found large pre-to-follow-up effect sizes for both, with IBCT showing significantly but not dramatically superior outcomes through early follow-up years and convergence over longer horizons; divorce/separation rates remained non-trivial in both arms — set realistic expectations in viva.[5]
Behavioural vs insight-oriented (Snyder)
A controlled comparison with four-year follow-up is a classic exam landmark for long-term marital status and accord after behavioural versus insight-oriented marital therapy — know that long-term outcome research exists beyond post-treatment satisfaction scores.[6]
Depression
Meta-analysis found no difference between couple therapy and individual psychotherapy on depressive symptoms, with greater reduction in relationship distress for couple therapy when that domain is measured — the dual-outcome logic for depressed patients with discord.[7] Cochrane synthesis and subsequent clinical implications papers support couple therapy as improving depressive symptoms comparably to individual psychotherapy, with relationship benefits as a key differentiator when discord coexists.[8][9]
Substance use disorders
Narrative and meta-analytic evidence supports behavioural couples therapy for married/cohabiting patients with alcohol or drug use disorders: better abstinence-related outcomes and relationship functioning than individual-based treatment alone in synthesis.[10][11]
PTSD
A randomised trial of cognitive-behavioural conjoint therapy versus wait-list showed decreased PTSD symptom severity and benefits for patient comorbid symptoms — know CBCT as a disorder-specific couple package, not the only PTSD first-line option globally.[12]
EFT
Research reviews summarise EFT as an attachment-based brief couple therapy with a body of outcome and process research supporting reduced distress and improved bonding for many couples.[14]
Differential and modality choice
- Couple vs individual IPT/CBT for depression: if discord is high and both partners engage safely, couple therapy can treat depression and discord; if discord is low, individual IPT/CBT remains excellent first-line psychological care.[7][8]
- EFT vs IBCT vs TBCT: attachment injury and emotional disconnection may favour EFT; chronic polarisation with unsolvable differences may favour IBCT acceptance work; skill deficits and low positive exchange may favour TBCT skill training — all can help; competence and preference matter.[4][14]
- BCT-SUD vs individual SUD treatment: prefer BCT when a supportive cohabiting partner will engage and violence is not a barrier.[11]
- Family therapy: multi-member systems (parents + adolescent, multi-generational) differ from dyadic couple work.
Subtypes and scenarios
- Primary discord without major Axis I disorder.
- Depression with marital discord (dual outcome target).[8]
- Alcohol/drug use with cohabiting partner (BCT).[10]
- PTSD with partner accommodation or secondary trauma (CBCT).[12]
- Infidelity recovery (stabilisation → disclosure/processing per protocol → rebuild trust).
- Same-sex and gender-diverse couples — adapt skills without pathologising identity; address minority stress when relevant.[15]
- Perinatal couples — sleep, role transition, postpartum depression interface.
- Later-life couples — medical illness roles, caregiving, sexual changes, grief.
Complications and pitfalls
- IPV escalation from poorly timed homework.
- Therapist triangulation or collusion with an abuser narrative.
- Secrets policy violations and dual-client ethics failures.
- Minimising treatable individual illness as “just the marriage.”
- Endless unfocused sessions without measures or termination criteria.[15][1]
Prognosis and disposition
Many couples improve with evidence-based therapy; a substantial minority still separate over multi-year follow-up even after good acute gains — counsel honestly.[5][15] Disposition ladder: outpatient couple pathway when both engage and safety allows → parallel CMHT/individual care for moderate–severe individual illness → step-up admission for risk → specialist domestic-violence services when conjoint therapy is unsafe.
Regional guidance language
NICE-style depression pathways include couple interventions among psychological options when relationship problems maintain depression; APA and contemporary reviews endorse evidence-based couple treatments for distress and selected disorders; FRANZCP training expects formulation-based psychotherapy competence and safe practice boundaries rather than brand loyalty. Match local supervision and service access.[8][15][1]
Special populations
- Youth/young adults: emerging adult couples; still screen IPV; family of origin may need parallel work.
- Older adults: medical comorbidity, cognitive change, late-life depression with caregiving strain.
- Pregnancy/lactation: prioritise safety and depression care; couple support is adjunct, not a reason to withhold indicated individual treatment.
- Intellectual disability / autism: adapt communication tools; involve carers carefully without excluding the dyad’s autonomy.
- Cultural/Indigenous contexts: avoid imposing monocultural intimacy scripts; use cultural formulation of roles and help-seeking. [15] [16]
Exam traps (rapid fire)
- Offering conjoint sessions when IPV is active and undisclosed without a safety plan.[15]
- Claiming couple therapy replaces antidepressants for severe melancholic depression or treats acute mania.[8]
- Equating all couple therapy with EFT or with mediation.[14]
- Forgetting BCT for SUD targets both abstinence support and relationship functioning.[10][11]
- Assuming couple therapy is first-line for all depression even when discord is absent.[7]
- Misquoting Christensen as IBCT always dramatically superior at five years — large gains for both, early IBCT edge then convergence.[5]
CASC / viva technique snippets
Plain-language opener: “Couples therapy means we work with both of you as clients. We look at the patterns between you — not who is ‘the problem person’ — and practise safer ways of talking and solving problems, while also treating any depression, trauma, or alcohol problems that are feeding the cycle.”[15][16]
IPV stop line: “I need to see each of you alone first for a private safety check. If either of you is afraid of being hurt, we change the plan so therapy does not make things more dangerous.”[15]
Depression + discord pitch: “Tablets or individual therapy can treat depression; when the relationship is also under severe strain, couple sessions often help mood and the relationship together — if both of you want that and it is safe.”[8][9]
BCT-SUD line: “For alcohol problems, involving a partner in a structured recovery plan can improve sobriety support and reduce fighting about drinking — it is not about blame.”[10][11]
Bottom line for fellowship candidates
Deliver couples therapy as safe dual-client work with private IPV screening, clear model choice (TBCT/IBCT/EFT/disorder-specific), and outcome tracking. Cite Shadish/Baucom for overall efficacy, Christensen for IBCT/TBCT and long follow-up, Barbato/Cochrane for depression, O’Farrell/Powers for SUD, Monson for PTSD conjoint therapy, and Whisman for population comorbidity. Never sacrifice safety or individual medical treatment for modality purity.[2][5][8][11][12][13]
References
- [1]Baucom DH, Shoham V, Mueser KT, Daiuto AD, Stickle TR Empirically supported couple and family interventions for marital distress and adult mental health problems J Consult Clin Psychol, 1998.PMID 9489262
- [2]Shadish WR, Baldwin SA Meta-analysis of MFT interventions J Marital Fam Ther, 2003.PMID 14593694
- [3]Shadish WR, Baldwin SA Effects of behavioral marital therapy: a meta-analysis of randomized controlled trials J Consult Clin Psychol, 2005.PMID 15709827
- [4]Christensen A, Atkins DC, Berns S, et al. Traditional versus integrative behavioral couple therapy for significantly and chronically distressed married couples J Consult Clin Psychol, 2004.PMID 15065953
- [5]Christensen A, Atkins DC, Baucom B, Yi J Marital status and satisfaction five years following a randomized clinical trial comparing traditional versus integrative behavioral couple therapy J Consult Clin Psychol, 2010.PMID 20350033
- [6]Snyder DK, Wills RM, Grady-Fletcher A Long-term effectiveness of behavioral versus insight-oriented marital therapy: a 4-year follow-up study J Consult Clin Psychol, 1991.PMID 2002129
- [7]Barbato A, D'Avanzo B Efficacy of couple therapy as a treatment for depression: a meta-analysis Psychiatr Q, 2008.PMID 18259866
- [8]Barbato A, D'Avanzo B, Parabiaghi A Couple therapy for depression Cochrane Database Syst Rev, 2018.PMID 29882960
- [9]Barbato A, D'Avanzo B The Findings of a Cochrane Meta-Analysis of Couple Therapy in Adult Depression: Implications for Research and Clinical Practice Fam Process, 2020.PMID 32294797
- [10]O'Farrell TJ, Fals-Stewart W Behavioral couples therapy for alcoholism and drug abuse J Subst Abuse Treat, 2000.PMID 10636606
- [11]Powers MB, Vedel E, Emmelkamp PM Behavioral couples therapy (BCT) for alcohol and drug use disorders: a meta-analysis Clin Psychol Rev, 2008.PMID 18374464
- [12]Monson CM, Fredman SJ, Macdonald A, et al. Effect of cognitive-behavioral couple therapy for PTSD: a randomized controlled trial JAMA, 2012.PMID 22893167
- [13]Whisman MA Marital distress and DSM-IV psychiatric disorders in a population-based national survey J Abnorm Psychol, 2007.PMID 17696721
- [14]Wiebe SA, Johnson SM A Review of the Research in Emotionally Focused Therapy for Couples Fam Process, 2016.PMID 27273169
- [15]Lebow J, Snyder DK Couple therapy in the 2020s: Current status and emerging developments Fam Process, 2022.PMID 36175119
- [16]Baucom DH, Belus JM, Adelman CB, Fischer MS, Paprocki C Couple-based interventions for psychopathology: A renewed direction for the field Fam Process, 2014.PMID 24773298