Psych · psychotherapy
Exposure and response prevention
Also known as ERP · EX/RP · Exposure and ritual prevention · Exposure with response prevention · OCD exposure therapy · Behavioural treatment of OCD
Exam-exhaustive fellowship reference on exposure and response prevention (ERP/EX/RP) — OCD maintenance cycle, habituation vs inhibitory learning, hierarchy design, ritual and safety-behaviour prevention, intensive vs outpatient dosing, landmark trials (Foa, Simpson, POTS), medication integration, pitfalls, youth adaptations, and CASC technique. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
ERP (also called exposure and ritual prevention, EX/RP) is a time-limited, structured behavioural treatment derived from learning theory and refined in modern manuals associated with Foa and colleagues.[13] The essential pair is: (1) exposure to internal or external triggers of obsessions, and (2) response prevention — deliberate non-performance of overt and covert rituals. Exposure without ritual prevention is not ERP.[13]
Historical clinical reports (Meyer and subsequent hospital series) established that preventing rituals while confronting feared stimuli could reduce OCD symptoms that had been thought intractable; contemporary RCTs and meta-analyses place ERP among the most efficacious psychological interventions for OCD.[8][9][10][13]
What ERP is not
| Label sometimes confused | Discriminator |
|---|---|
| Supportive counselling | No hierarchy, no ritual prevention, no homework exposures |
| Systematic desensitisation | Relaxation pairing historically; ERP does not require relaxation and prioritises ritual blocking |
| Pure cognitive therapy | May debate appraisals without in-session behavioural tests; modern OCD CBT often includes ERP |
| Prolonged exposure (PTSD) | Trauma memory processing protocol; related exposure science, different targets and manuals |
| "Just stop washing" advice | No graded plan, no expectancy work, high dropout and shame risk |
Epidemiology and access risk
OCD is common enough and disabling enough to justify active case-finding: lifetime prevalence in the National Comorbidity Survey Replication is on the order of about 2 percent, with substantial comorbidity and delayed treatment.[18] The public-health problem for ERP is less "does it work" than access and fidelity: few clinicians deliver true EX/RP; many patients receive medication alone or generic talking therapy; trial dropout and incomplete homework are common; family accommodation undoes gains.[13][15][16]
Mechanisms — from negative reinforcement to inhibitory learning
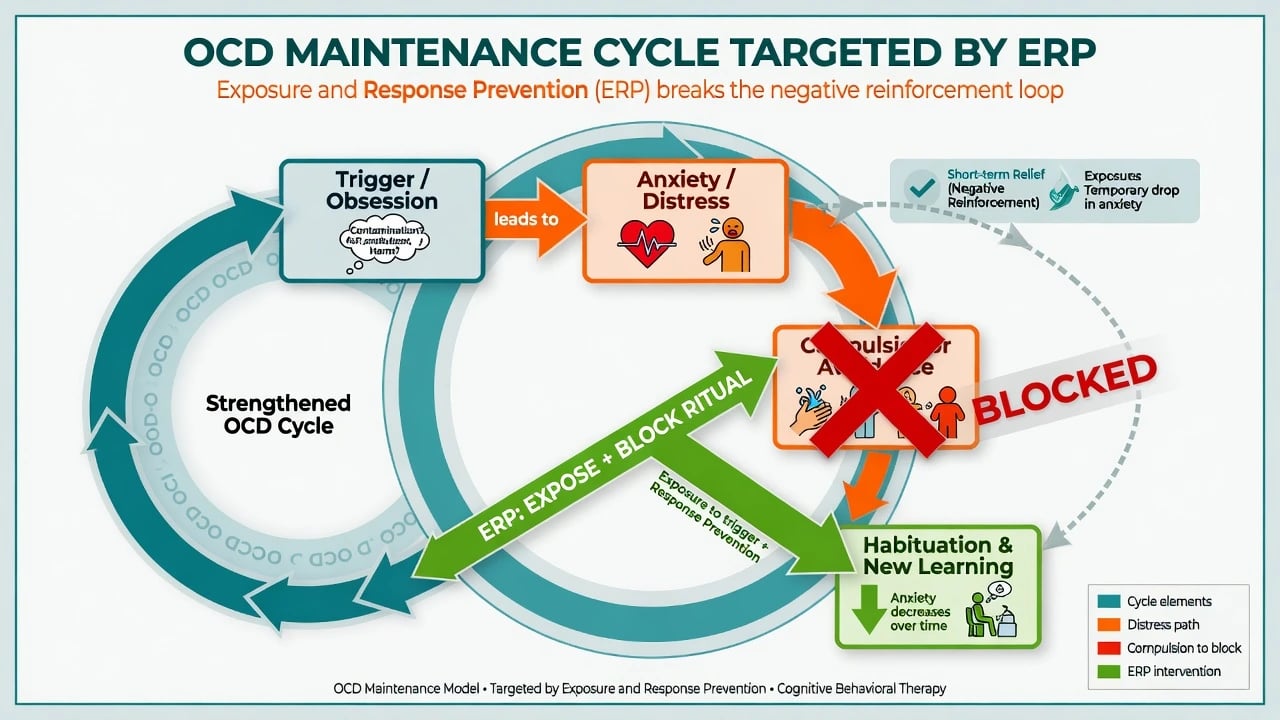
Maintenance cycle
The behavioural core is negative reinforcement. An obsession or trigger elicits distress; the compulsion or avoidance reduces distress short-term; that relief strengthens the ritual, so the next trigger is more likely to recruit the same loop.[13] Covert rituals (mental undoing, silent praying, reviewing) count equally with washing and checking.
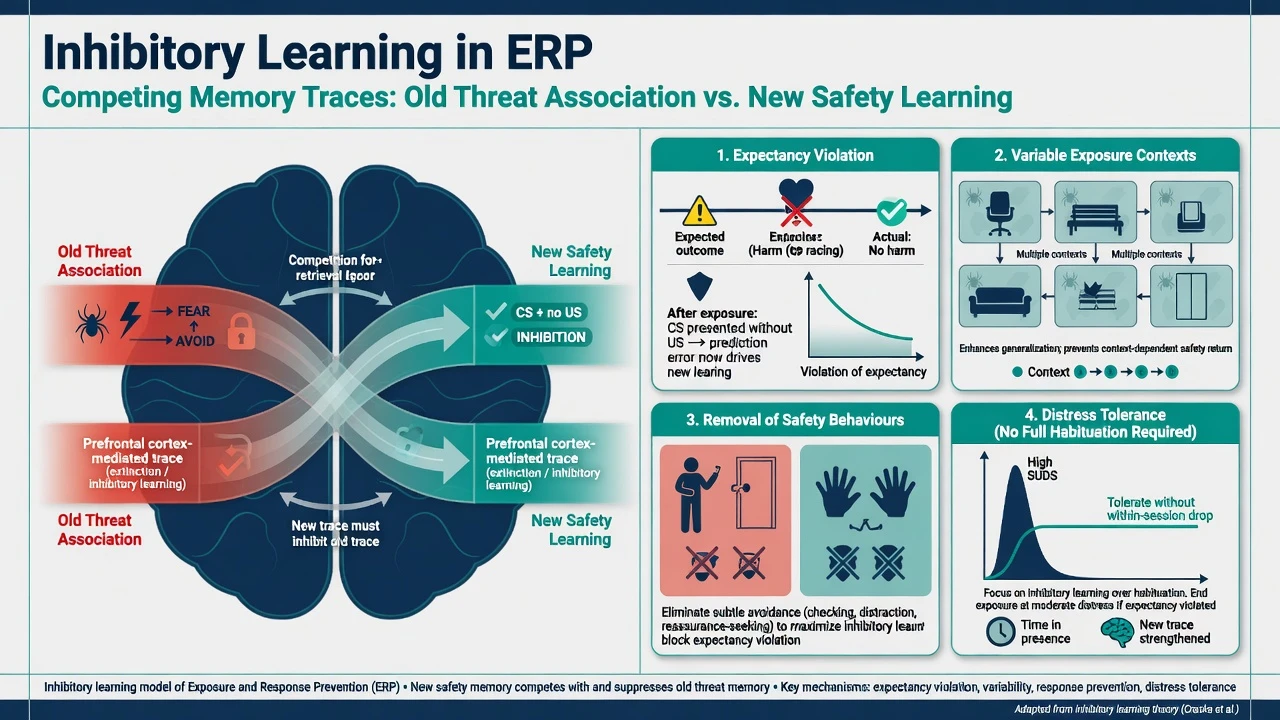
Habituation vs inhibitory learning
Early ERP teaching emphasised within-session and between-session habituation (SUDs falling while remaining in the situation). That remains useful for coaching, but contemporary exposure science emphasises inhibitory learning: new safety associations compete with old threat associations rather than erasing them.[12] Design exposures to maximise expectancy violation, vary contexts, remove safety signals, and tolerate distress without requiring perfect within-session calm as the sole success metric.[12]
Cognitive maintainers (inflated responsibility, thought–action fusion, intolerance of uncertainty) often sit alongside the behavioural loop; many protocols integrate brief cognitive work, but behavioural change with ritual prevention remains the active spine of evidence-based OCD psychotherapy.[8][13]
Clinical presentation relevant to ERP design
Map symptoms into treatable targets for ERP design, then match in-vivo or imaginal exposures with explicit ritual prevention: contamination/washing (delayed or eliminated washing); checking/harm (leave situations unchecked; imaginal scripts for catastrophic harm fears); symmetry/ordering (create asymmetry and resist "evening up"); forbidden thoughts (imaginal exposure; block mental rituals and reassurance); and mental rituals (response prevention of reviewing, counting, praying-as-undoing).[13]
Document time occupied, avoidance map, insight, depression, suicide risk, and family accommodation (who provides reassurance, who cleans, who checks locks "for" the patient).[13][14]
Differential: choosing ERP versus related therapies
[13] [17]Assessment for ERP
- Diagnosis and dimensions — DSM-5-TR/ICD-11 OCD features; rule out psychosis, primary substance, organic differentials when atypical.[17][19]
- Severity — Yale-Brown Obsessive Compulsive Scale (Y-BOCS) remains the standard severity anchor (obsessions and compulsions subscales).[14]
- Ritual inventory — overt and covert; include digital checking, mental reviewing, and reassurance scripts.[13]
- Safety behaviours disguised as coping — gloves, special "clean" zones, phone photos of doors, asking the same question twice.[13]
- Readiness and goals — informed consent for temporary anxiety increase; values-based goals (parenting, work) improve engagement.[13]
- Medical/psychotropic baseline — if combining with SSRI or clomipramine, complete usual prescribing work-up (metabolic, ECG when indicated for TCA/risk factors).[17]
No laboratory test selects ERP candidates; serial outcome measures are the process "investigation."[14][15]
Acute / emergency management interface
ERP is elective. Pause or defer intensive exposures when active high suicide risk lacks a safety plan and appropriate acuity of care; when mania, severe psychosis, delirium, or medical instability is present; when decision-specific incapacity blocks consent to the exposure plan; or when safeguarding crises require immediate protection.[13]
Expected short-lived anxiety rise during exposure is not by itself a reason to abandon ERP if risk is otherwise managed.[13]
Definitive ERP protocol
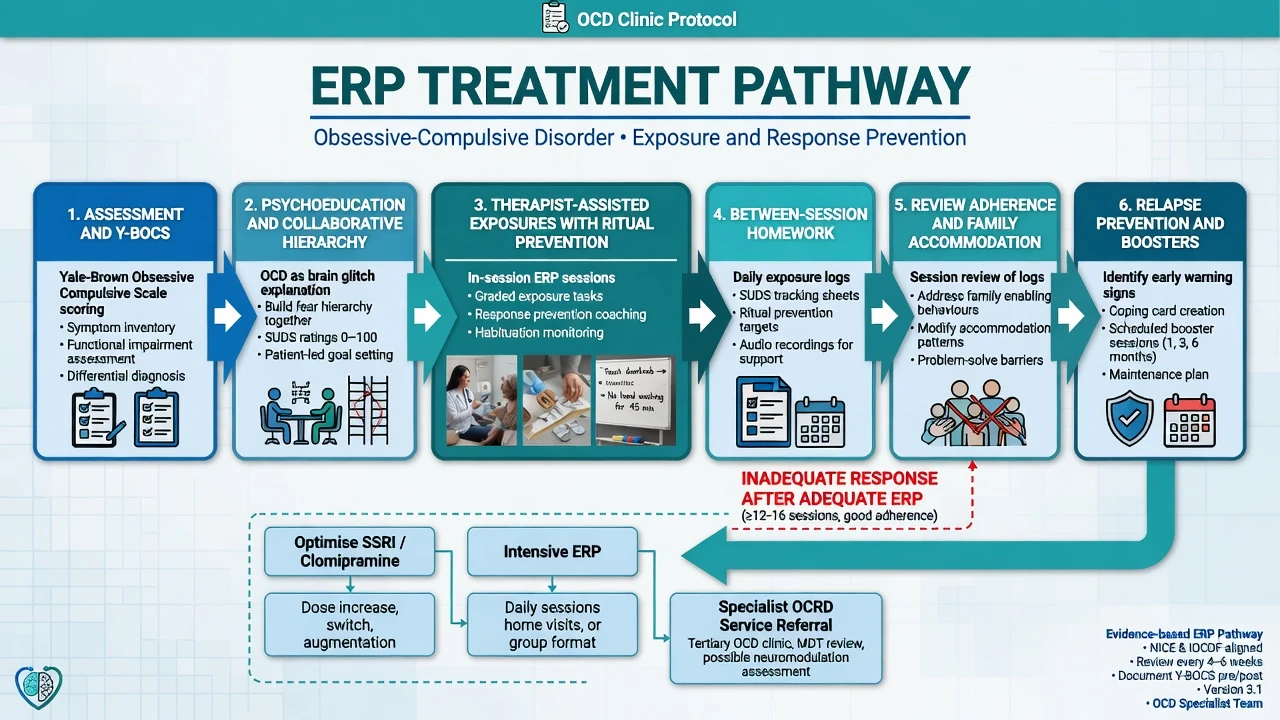
Course structure
Typical outpatient sequence: assessment and psychoeducation → collaborative hierarchy → therapist-assisted exposures with response prevention → generalisation homework → family accommodation work → relapse prevention and boosters.[13][17]
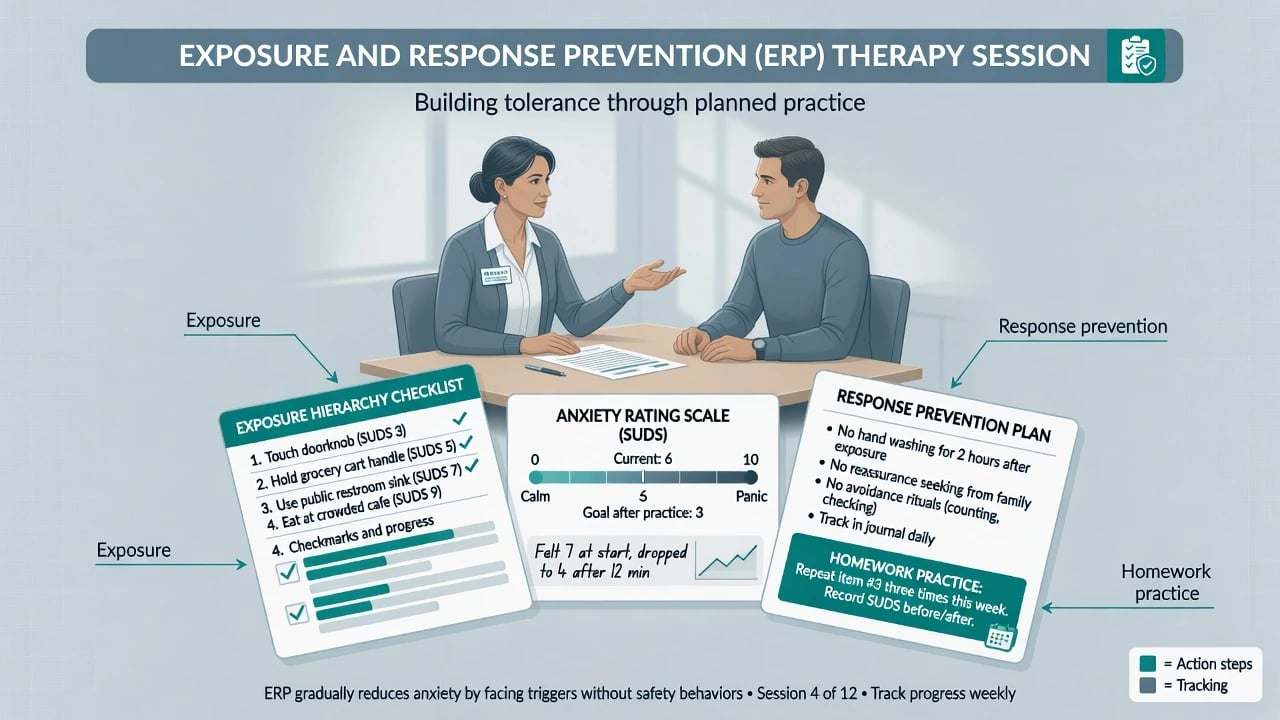
Session technique
- Set agenda; review homework adherence quality (not only "did you try").
- Agree the exposure task and the exact response-prevention rule (e.g. no washing for four hours; no checking more than once; no mental reviewing).
- Elicit predicted outcome / expectancy ("What do you fear will happen? How sure are you?").
- Conduct exposure (in vivo preferred when possible; imaginal when content is internal).
- Block rituals; if a ritual breaks through, re-expose promptly.
- Process learning: "What did you predict? What happened? What does that mean for the OCD rule?"
- Assign between-session practices with the same response-prevention rules.
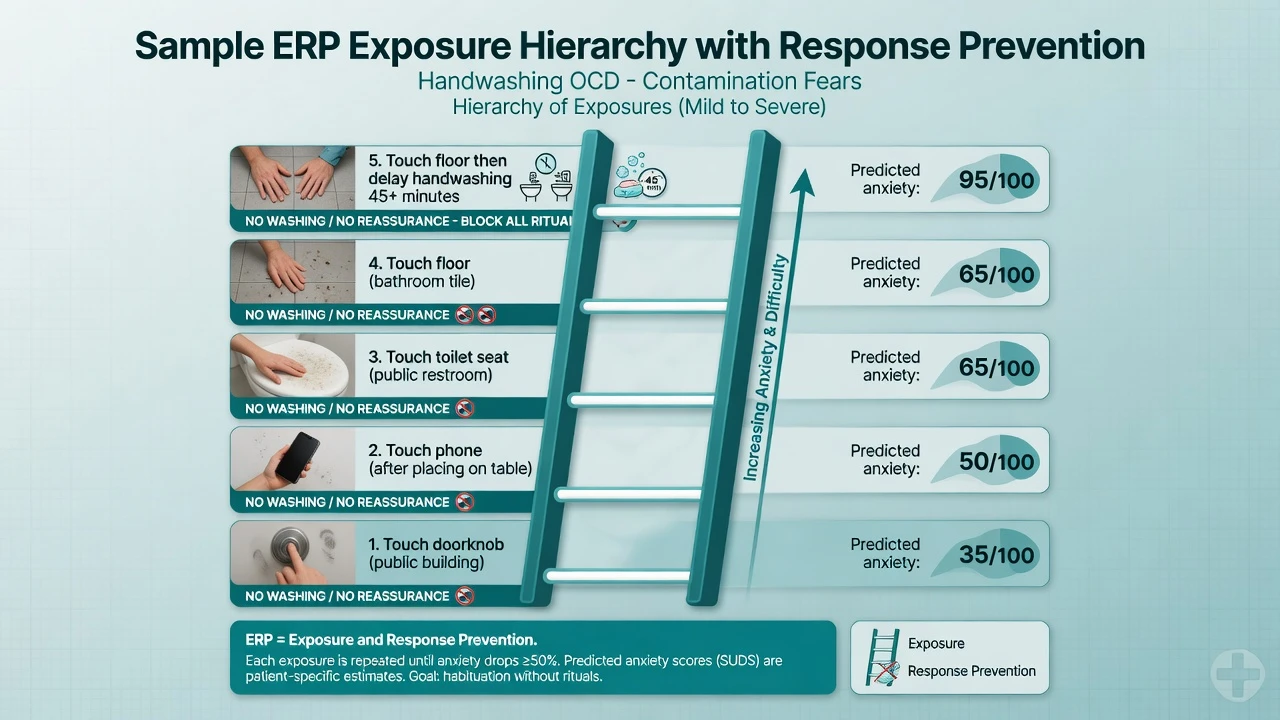
Hierarchy and dosing
Hierarchies rank tasks by predicted distress and meaningfulness. Start with items that are challenging enough to violate expectancies but achievable enough to complete with coaching; climbing forever at trivial levels wastes time, while jumping to intolerable items without skills can drive dropout.[12][13]
Schedule: Classic intensive programmes use daily sessions; Abramowitz and colleagues found twice-weekly EX/RP can achieve outcomes comparable to intensive schedules for many patients over follow-up, improving transportability to ordinary clinics.[5] Weekly sessions can work if total exposure dose and between-session practice are high; sparse sessions with no homework predict failure.[13][15]
Family accommodation
Treat accommodation as part of the disorder system: reduce reassurance, stop family checking/cleaning for the patient, and coach relatives in supportive non-accommodation language. Unaddressed accommodation predicts poorer behavioural outcomes.[13]
Integrating pharmacotherapy
| Strategy | Exam-relevant evidence |
|---|---|
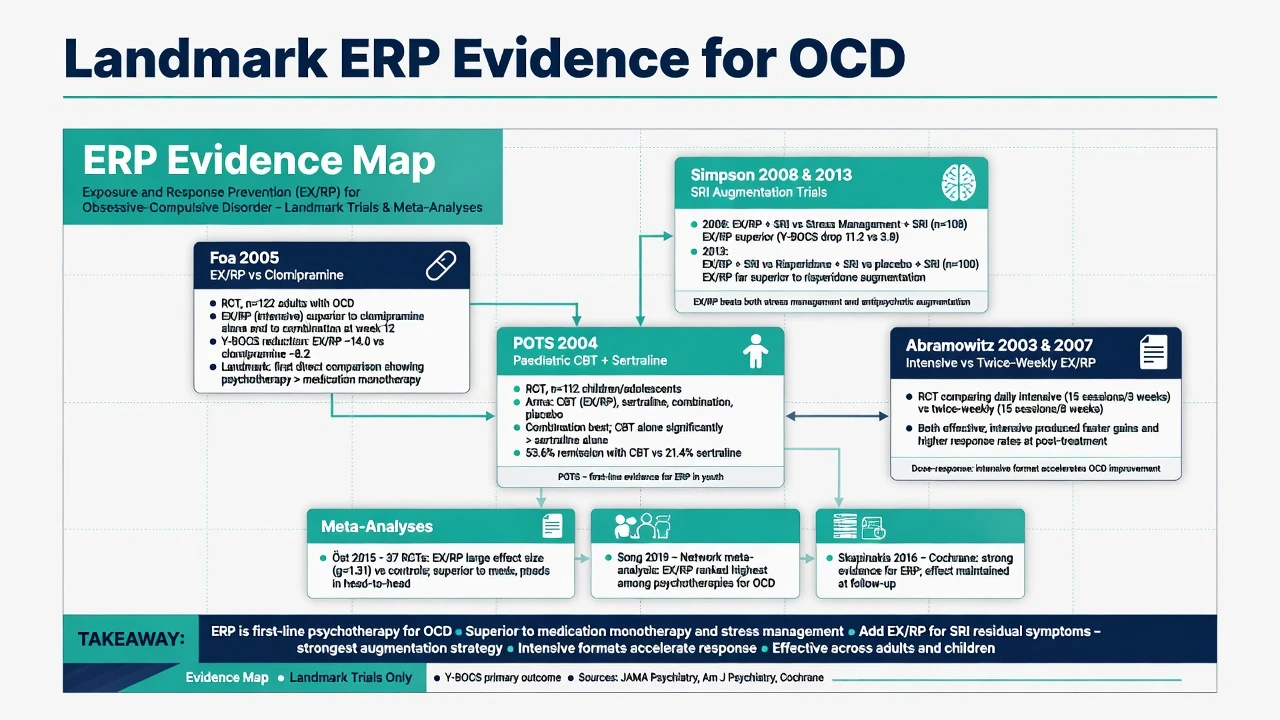
| EX/RP alone vs clomipramine | Foa 2005: EX/RP (with or without CMI) superior to CMI alone; combination not clearly superior to EX/RP alone at 12 weeks in that design.[1] |
| SRI partial response | Simpson 2008: adding EX/RP superior to adding stress management training.[2] |
| SRI residual symptoms | Simpson 2013: EX/RP superior to risperidone and to placebo augmentation; Foa 2015 six-month data support durability of EX/RP advantage.[3][4] |
| First-line meds context | SSRIs (often higher dose bands than depression) and clomipramine remain pharmacological standards; APA guideline frames CBT/ERP and SRIs as core options.[17][19] |
SSRI example framing for combination care (not a substitute for product info): sertraline is commonly titrated toward OCD ranges (e.g. up to 200 mg oral daily as tolerated with monitoring for activation, GI effects, hyponatraemia risk, sexual side effects, and serotonin toxicity with interacting agents); pair with ERP rather than using dose escalation alone as a reason to avoid behavioural work.[6][17]
Network and pairwise meta-analyses support both psychological (ERP-based CBT) and pharmacological efficacy; choice and sequencing depend on severity, preference, access, prior response, and comorbidity.[8][11]
Special populations and subtypes
Children and adolescents
POTS randomised youth to CBT, sertraline, combination, or placebo: combination was strongest overall; CBT and sertraline each beat placebo, with CBT showing particularly strong effects in some site analyses.[6] POTS II showed that CBT augmentation helps children with partial response to SRIs more than medication management alone.[7] Family-based ERP and school accommodation plans are usually required.
Pregnancy and perinatal
Prefer accessible ERP when severity allows; coordinate obstetric care and risk–benefit if SRI continuation or initiation is needed. Do not leave severe OCD untreated because of pregnancy alone.[17]
Older adults, ID, autism, cultural/religious scrupulosity
Slow pacing, medical comorbidity, simplified hierarchies, carer coaching, sensory load, and values-respecting work with scrupulosity (target OCD mechanisms without attacking faith) are examiner-ready adaptations.[13][19]
Related OCRDs
BDD and hoarding share ritualistic behaviours but often need specialised protocols; do not assume a generic contamination hierarchy transfers unchanged.[17][19]
Complications and pitfalls
Other high-yield failures: benzodiazepine blunting of every session; hierarchy never reaching meaningful cues; family undoing practice at home; declaring failure after four unstructured chats; moralising rather than coaching ritual prevention; ignoring depression/suicide that limits engagement.[12][13][16]
Behavioural avoidance and poor adherence components predict worse EX/RP outcomes — monitor process, not only end-of-treatment Y-BOCS.[15][16]
Prognosis and disposition
Meta-analyses show large effects for ERP-based treatments versus inactive controls and robust clinical response among completers, with a non-trivial minority not remitting and relapse risk if rituals return.[8][9][10] Plan booster sessions, a written relapse blueprint (early ritual return → restart exposures), and step-up to intensive/residential ERP or SRI optimisation/augmentation when outpatient fidelity-adequate ERP fails.[4][13][19]
Disposition ladder: specialist outpatient ERP → intensive programmes → CMHT support for comorbidity/risk → inpatient care for risk or medical need (not as coercive "forced ERP"). Neuromodulation pathways for highly refractory OCD sit after adequate ERP and medication trials in specialist pathways.[17][19]
Regional guideline deltas
ANZ / FRANZCP: Expect registrars to understand and prescribe ERP conceptually, refer appropriately, and avoid pseudo-CBT. Local public services often have long waits — document interim ERP-informed homework and SRI care.[17][19]
UK / MRCPsych / NICE framing: NICE-aligned pathways position CBT including ERP as core psychological care for OCD/BDD; stepped care and access standards are examinable in principle even when local delivery lags.[17][19]
US / ABPN / APA: APA OCD guideline supports CBT with ERP and SRIs as foundational; Simpson/Foa trials are classic ABPN-style evidence stems.[1][3][17]
Exam pearls
ERP-CORE coaching checklist
CASC micro-script (contamination example)
"Today we will practise touching the bathroom door handle and then not washing for the next three hours, including no sanitiser and no asking your partner if your hands are clean. Your OCD predicts illness or unbearable dirtiness. We will stay with the urge, rate the distress, and check what actually happened. I will not give reassurance that it is 'safe enough' — that would become a ritual with me. Afterward we will write what you predicted versus what you learned, and set two home practices."[12][13]
Summary table for viva
| Domain | Condensed answer |
|---|---|
| Definition | Exposure + prevention of rituals/safety behaviours |
| Mechanism | Breaks negative reinforcement; builds inhibitory safety learning |
| Measure | Y-BOCS + adherence |
| Landmark adult | Foa 2005; Simpson 2008/2013; Abramowitz 2003 |
| Landmark youth | POTS; POTS II |
| Meds | SSRIs/CMI; EX/RP preferred augmentation over risperidone when available |
| Fail mode | Pseudo-ERP, accommodation, no homework |
References
- [1]Foa EB, Liebowitz MR, Kozak MJ, et al. Randomized, placebo-controlled trial of exposure and ritual prevention, clomipramine, and their combination in the treatment of obsessive-compulsive disorder Am J Psychiatry, 2005.PMID 15625214
- [2]Simpson HB, Foa EB, Liebowitz MR, et al. A randomized, controlled trial of cognitive-behavioral therapy for augmenting pharmacotherapy in obsessive-compulsive disorder Am J Psychiatry, 2008.PMID 18316422
- [3]Simpson HB, Foa EB, Liebowitz MR, et al. Cognitive-behavioral therapy vs risperidone for augmenting serotonin reuptake inhibitors in obsessive-compulsive disorder: a randomized clinical trial JAMA Psychiatry, 2013.PMID 24026523
- [4]Foa EB, Simpson HB, Rosenfield D, et al. Six-month outcomes from a randomized trial augmenting serotonin reuptake inhibitors with exposure and response prevention or risperidone J Clin Psychiatry, 2015.PMID 25375780
- [5]Abramowitz JS, Foa EB, Franklin ME Exposure and ritual prevention for obsessive-compulsive disorder: effects of intensive versus twice-weekly sessions J Consult Clin Psychol, 2003.PMID 12699033
- [6]Pediatric OCD Treatment Study (POTS) Team Cognitive-behavior therapy, sertraline, and their combination for children and adolescents with obsessive-compulsive disorder: the Pediatric OCD Treatment Study (POTS) randomized controlled trial JAMA, 2004.PMID 15507582
- [7]Franklin ME, Sapyta J, Freeman JB, et al. Cognitive behavior therapy augmentation of pharmacotherapy in pediatric obsessive-compulsive disorder: the Pediatric OCD Treatment Study II (POTS II) randomized controlled trial JAMA, 2011.PMID 21934055
- [8]Öst LG, Havnen A, Hansen B, Kvale G Cognitive behavioral treatments of obsessive-compulsive disorder. A systematic review and meta-analysis of studies published 1993-2014 Clin Psychol Rev, 2015.PMID 26117062
- [9]Eddy KT, Dutra L, Bradley R, Westen D A multidimensional meta-analysis of psychotherapy and pharmacotherapy for obsessive-compulsive disorder Clin Psychol Rev, 2004.PMID 15533282
- [10]Song Y, Li D, Zhang S, et al. The effect of exposure and response prevention therapy on obsessive-compulsive disorder: A systematic review and meta-analysis Psychiatry Res, 2022.PMID 36179591
- [11]Skapinakis P, Caldwell DM, Hollingworth W, et al. Pharmacological and psychotherapeutic interventions for management of obsessive-compulsive disorder in adults: a systematic review and network meta-analysis Lancet Psychiatry, 2016.PMID 27318812
- [12]Craske MG, Treanor M, Conway CC, Zbozinek T, Vervliet B Maximizing exposure therapy: an inhibitory learning approach Behav Res Ther, 2014.PMID 24864005
- [13]Hezel DM, Simpson HB Exposure and response prevention for obsessive-compulsive disorder: A review and new directions Indian J Psychiatry, 2019.PMID 30745681
- [14]Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale. I. Development, use, and reliability Arch Gen Psychiatry, 1989.PMID 2684084
- [15]Wheaton MG, Galfalvy H, Steinman SA, et al. Patient adherence and treatment outcome with exposure and response prevention for OCD: Which components of adherence matter and who becomes adherent? Behav Res Ther, 2016.PMID 27497840
- [16]Wheaton MG, Gershkovich M, Gallagher T, Foa EB, Simpson HB Behavioral avoidance predicts treatment outcome with exposure and response prevention for obsessive-compulsive disorder Depress Anxiety, 2018.PMID 29394511
- [17]Koran LM, Hanna GL, Hollander E, Nestadt G, Simpson HB; American Psychiatric Association Practice guideline for the treatment of patients with obsessive-compulsive disorder Am J Psychiatry, 2007.PMID 17849776
- [18]Ruscio AM, Stein DJ, Chiu WT, Kessler RC The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication Mol Psychiatry, 2010.PMID 18725912
- [19]Fineberg NA, Hollander E, Pallanti S, et al. Clinical advances in obsessive-compulsive disorder: a position statement by the International College of Obsessive-Compulsive Spectrum Disorders Int Clin Psychopharmacol, 2020.PMID 32433254